
Abstract
Background
Historically, the experiences and voices of children and youth living with neurodiversity or rehabilitation needs and their families have not been fully represented in health research. Formative research in this context indicates that families value learning from the experiences of other families as well as from empirical research. However, innovative systems are needed to support this imperative. In response, we co-designed a virtual living lab with families and clinicians to support family-centered knowledge exchange in neurodiversity and rehabilitation research. Living labs are collaborative, user-centered, long-term, and multimethod systems with potential to support the exchange of knowledge of lived experience. This proposal outlines a longitudinal arts-based and qualitative research study that incorporates storytelling as a powerful tool to elicit and exchange stories of lived experience through the virtual living lab, and subsequent usability testing of the platform.
Methods and Analysis
Stage 1- We will conduct an integrated knowledge translation study inclusive of user centered lab design and construction. Stage 2- We will conduct a 6-month longitudinal qualitative storytelling study with 30–40 participants including neurodiverse children and youth ages 5–19 years, their siblings, and parent/guardians, guided by the F-words framework which is based on the International Classification of Functioning, Disability, and Health. Following user-registration within the virtual lab, participants will complete a minimum of 1 story monthly, accompanied by an arts-based component, for 6 months.
Conclusion
Findings will inform the co-development of an arts-based knowledge translation resource to communicate key findings. Stage 3- A subset of families will be sampled to complete usability testing of the living lab platform and storytelling feature using a sequential explanatory mixed methods design. Usability evaluation will inform future platform refinements and provide indications of acceptability and use across subgroups.
Keywords
Introduction
Approximately 12.4% of Canadians live with disability (Lucie & Edith, 2001). In the context of youth disability or neurodiversity research, there continues to be a need for more thorough understandings of family experiences, indicating that much more can be done to understand, include, and support families across the childhood neurodiversity spectrum (Shimmin et al., 2017). Such understandings are critical given that numerous social, environmental and system level barriers exist, impact inclusivity and accessibility for neurodiverse children throughout their lifespan, contribute to familial stress and create social and economic impacts for families and society (Zajicek-Farber et al., 2015). While it is recognized that longitudinal, socially inclusive and strengths-based research with families is needed, research with families is often short-term, deficit based, and characterized by small sample sizes (Archibald et al., 2021c). With sensitivity to this reality, we propose a multistage longitudinal study involving qualitative and arts-based data collection within a living lab platform co-designed with families to encourage knowledge exchange in childhood neurodiversity, as part of an integration knowledge translation applied research program in child health.
Integrated Knowledge Translation and Family-Engagement
Western health care is characterized by a growing emphasis on knowledge translation (KT) and patient-engagement (Greenhalgh et al., 2011). Such engagement is part of a broader Patient and Participant Involvement (PPI) in research movement, catalyzed by recognition that research should be conducted with rather than on participants (Skovlund et al., 2020), participants have a right to this involvement and influence (Greenhalgh et al., 2019), failing to maximizing the use of existing research results in costly research waste (Macleod, et al., 2014), and that engaging stakeholders meaningfully in research improves research uptake (Graham, et al., 2018). Approaches such as integrated knowledge translation (iKT), which emphasize partnership between knowledge users (e.g., families, clinicians) and producers (e.g., researchers), reflect this momentum and seek to improve the relevance and use of research findings in practice and policy (Greenhalgh et al., 2011, 2016). However, there remain critical gaps in how iKT is achieved; new systems that embed and sustain knowledge exchange in clinical environments are lacking yet sorely needed (Archibald et al., 2021c). Such embedded systems could help promote clinical values, such as family centered care, and the meaningful involvement of families in research in sustained, and systematic ways.
Family Centered Care (FCC) is the gold-standard model of service delivery in child health (Kuo et al., 2012). It is characterized by family provider collaborative partnership to establish trust, effective communication, shared expertise, and culturally sensitive care (Zajicek-Farber et al., 2015). Despite widespread recognition of its merits, shortfalls in implementing FCC persist in part because of a lack of strategies to mobilize knowledge of family lived experience (Kuo et al., 2012). FCC strategies, such as bedside rounds, are often embedded within in-patient care environments. However, ambulatory care settings may have fewer entrenched FCC initiatives (Kuo et al., 2012). Integrating FCC into clinical care and into the healthcare milieu more generally can also be supported through the sharing of experiential knowledge and through a strengths-based approach to communication. To this effect, CanChild, a leading childhood rehabilitation and disability research group in Canada, developed the F-words (or Favorite words) in 2011, to mobilize – in a holistic and useable manner – the domains of the WHO International Classification of Function (ICF) Framework (Rosenbaum & Gorter, 2012). The six “F-words” of fitness, function, family, fun, friends and future have catalyzed international interest and uptake (e.g., >24,000 visits to F-words knowledge hub; use of framework across 26 countries); however, systematic and context specific strategies to embed the F-words in the expression and use of experiential data from families is needed (Soper et al., 2021). This proposal attends to this gap by generating longitudinal story-based data from neurodiverse youth, their siblings and parents/guardians aligned with the F-words, within an accessible and clinically embedded living lab platform for childhood neurodiversity.
Living Labs for Knowledge Exchange in Childhood Rehabilitation and Disability
Living Labs are “collaborative spaces where users create, prototype, and test concepts, innovations, products and system.” (p. 15) (Leminen & Westerlund, 2017) Living labs emerged in the early 2000s as promising user-focused platforms for collaborative problem solving (Archibald et al., 2021c). Within health, living labs are used to support wellbeing and innovations in aged care (Konstantinidis et al., 2017), through the development and testing of technological innovations and through the support of aging in place initiatives. However, living labs represent untapped opportunities to support collaborative research in child health, including the systematic elicitation and sharing of familial experiential data. patient engagement and iKT. The need for such systems was catalyzed by the COVID-19 pandemic, which produced new barriers to patient-engaged research (Archibald & Blines, 2021).
Recognizing the potential for the user-centered living lab approach to support family centered research and care in youth neurodiversity research, we have begun piloting living labs in pediatric populations and are orientated towards the potential of living labs as user-centered models useful for identifying priorities, collecting data, co-designing and evaluating resources and interventions to ultimately improve health care delivery and support behavior change. The sustained nature of living labs enables rich insights of family experiences to be generated through multi-method research approaches in a manner not possible through traditional means. While effective in achieving health and health system objectives in other contexts, (Kim et al., 2020; Phanareth et al., 2017; Vereycken et al., 2019) before our living lab, no living lab platform had been developed to promote iKT, and never for pediatric neurodevelopment and rehabilitation research.
Context of Development
In 2019, we partnered with a large childhood rehabilitation outpatient facility in an urban setting (population in census metropolitan area, 855 310) in central Canada. Our initial partnership was catalyzed by a desire for more family engagement in research and enhanced attention towards knowledge translation. The interdisciplinary rehabilitation center houses approximately 250 staff and provides co-located orthopedic, neurodevelopmental and rehabilitation services to families within a strong family centered orientation.
Our initial engagement and funded research led to a mixed methods investigation involving 9 family focus groups and a survey on the priority functions of a living lab platform, completed by 67 clinicians. Findings indicated a strong orientation towards storytelling and story sharing as a means of knowledge exchange, support for virtual delivery considering COVID-19 restrictions impeding face-to-face information sharing, and the use of creative means (e.g., arts, video) for supporting knowledge exchange. This information was used to engage a youth, sibling and parent advisory group, wherein the features of storytelling, the main functions of the living lab platform, and the living lab name and branding, were delineated. As a result, a scaffolded blueprint of the living lab platform “Collaboration Station” was devised, and next steps for its operationalization were determined. Here, we report on the subsequent stages of operationalization planned for “the platform”, including a longitudinal qualitative and arts-based storytelling study with neurodiverse youth, their siblings, and parents/guardian; the co-design of an arts-based KT resource to mobilize these findings; and an explanatory sequential mixed methods usability study of “the platform” and the associated storytelling application.
Study Purpose and Objectives
The three aims of this study are to: 1. Operationalize the living lab platform and storytelling feature to understand family’s experiences of neurodiversity or neurodiversity and rehabilitation services framed by the F-words (ICF) framework, based on foundational research 2. Co-design an arts-based KT resource to mobilize evidence of family lived experiences in alignment with a priority F-word category (e.g., novel resource for sharing experience-based data). 3. Conduct usability testing to inform subsequent research and system improvement
Methods
Study Design
This is a multistage mixed methods study inclusive of three stages (Figure 1): 1. Operationalization of “the platform” to support longitudinal qualitative and arts-based data collection; 2. Co-design of an arts-based KT resource to mobilize experience-based data in an F-word category prioritized by participants; and 3. Explanatory sequential mixed methods usability testing of the lab and storytelling feature across user groups to provide needed data to support future scale up and feasibility of research using the living lab platform. Study overview and timeline.
Conceptual Framework
The Canada institutes of Health Research Knowledge (CIHR) Knowledge-to-Action Ethics framework (Figure 2) underpins this research and acknowledges often overlooked ethical considerations in the processes of knowledge creation and translation. Such sensitivity is critical given the ethical nuances of youth research, the necessity of researching with rather than on, and the need to reflect family voices in KT science. Conceptual framework: Knowledge-to-action ethics cycle. Canadian institutes of health research knowledge to action ethics cycle (2018).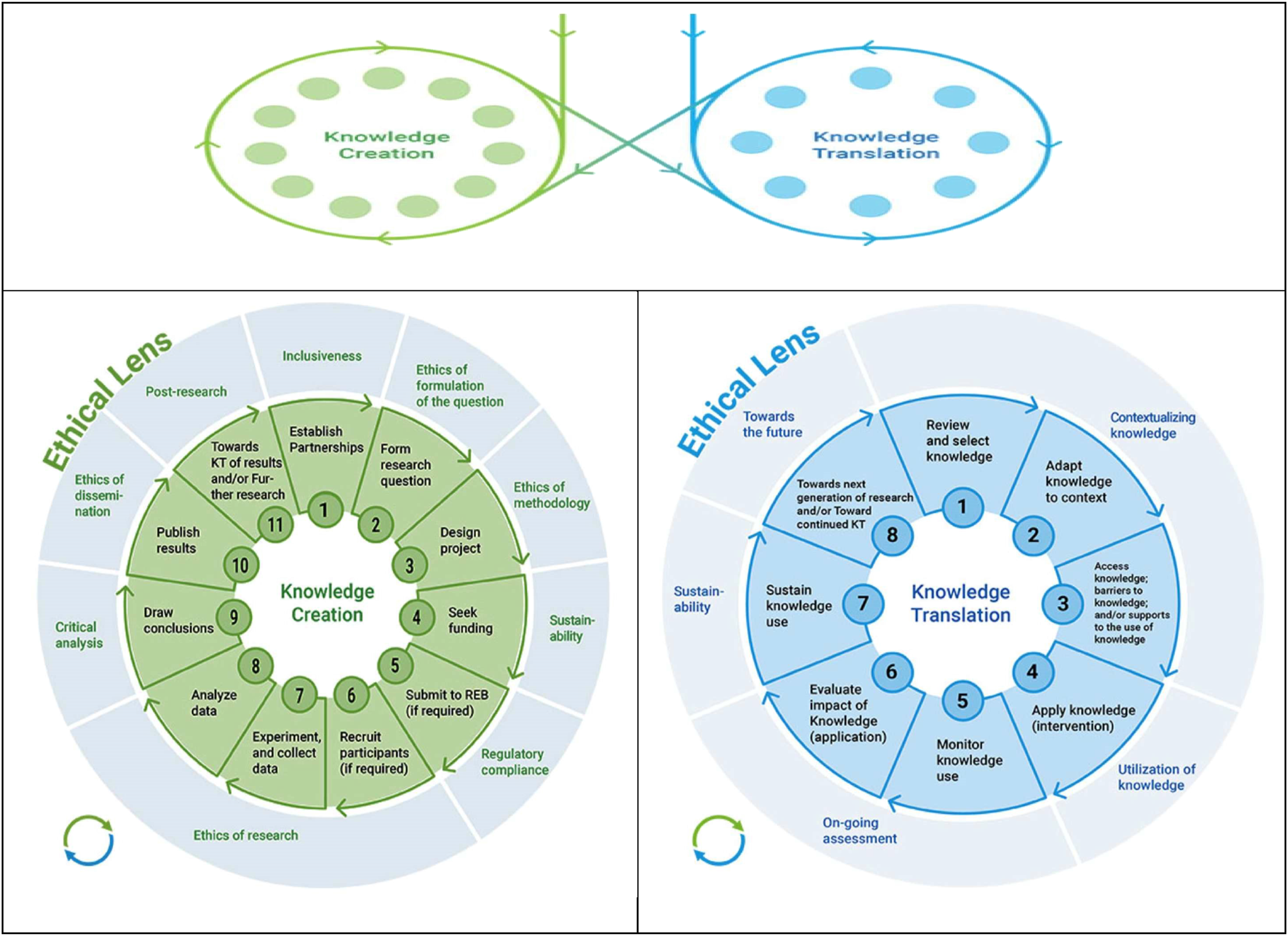
Setting of Study
This study will take place at the previously described partnered child development and rehabilitation services provider in a major urban center in central Canada. Given the web-based nature of the living lab platform, participants can complete data collection at the study site as desired or can participate virtually from any location convenient to them. The center values family involvement to inform health service delivery. This includes the presence of a participant advisory group which informed the development of the platform and associated storytelling study, and a shared vision to embed iKT within the Center to spearhead co-designed innovations and mobilize lived experience data for FCC. Our shared intention is to continue to enhance the living lab platform to support new and applied transdisciplinary research aimed at clinical impact and use of data of familial lived experience.
Participants and Inclusion Criteria
Participants in stage one must be either (1) youth aged 5–19 years who currently or previously accessed services at the partnered rehabilitation center; (2) parents or guardian of youth who has received these services; or (3) siblings of youth who have received services at this facility. Stage three usability testing will include a sub sample of this participant pool as well as clinicians providing services through the facility. The facility provides services to children and families with a range of needs and abilities (e.g., autism, spectrum disorder, global developmental delay, cerebral palsy); there are no inclusion criteria specific to diagnosis.
Sample Size and Recruitment
Stage 1
User-Centered Design & Build
Over 5 months, foundational information from our initial engagement and funded research was shared with a technological application designer (Sept 2022 – January 2023) to create the build plan for the living lab platform. From March through July 2023, the design plan was operationalized with the technology company to create a useable, secure and functional living lab platform to support the data collection and KT design of subsequent research stages proposed here. At various time points, the build was shared with the participant advisory and clinical/research partners for feedback; public engagement talks and an information sharing event at the facility enabled additional feedback to be elicited on the living lab platform, thereby improving the user-centered nature of the design.
Story and Arts-Based Data Collection
Sample size estimates in qualitative research are common; iterative data collection and analysis is a hallmark of rigorous qualitative research and enables data-driven decisions regarding sample size (Archibald et al., 2015; Thorne, 2008). We aim to recruit between 30-40 participants across the 3 subgroups (i.e., approximately 10 children or youth, 10 siblings and 10 parents/guardians). 30-40 participants are robust size for longitudinal qualitative research to enable deep analysis and subgroup comparisons (e.g., gender, intersectional considerations) (Collins et al., 2007; Sandelowski, 1995). While we hope to attain comparative sample sizes across the subgroups, our previous research with this population suggests that we may have higher representation from the parental subgroup (Archibald et al., 2020a); this will be examined as a component of usability in stage 3. We will leverage the networks and established communication in convenience and purposive recruitment strategies successfully used in our previous research (Archibald et al., 2021c). Interested participants will contact the study team to discuss eligibility, study information, and possible enrollment. Research staff will be at the facility during busy clinic times to raise awareness of and discuss the study with interested participants; an engaging 45 second short, animated film with QR code to a study information page will be playing in the clinic spaces to encourage awareness and study participation. Once it has been confirmed that participants have a clear understanding of the study process and their involvement, an electronic consent/assent form with a socio-demographic information questionnaire will be shared with participants. Parents or guardians will complete consent for participants unable to provide their own consent or who are not considered mature minors (e.g., under 16 years of age).
Stage 3 Usablity Testing
Data Collection
Stage 1
We will collect participants’ socio-demographic information. Age, gender, diagnostic and family composition data will be collected within the secure user-profile registration feature of the living lab platform. Registered users will use their generated system passwords to complete their user profiles (e.g., avatar, username) and within the living lab platform, enter semi-structured stories and associated artistic entries (e.g., photographs, drawings) guided by the parameters we established with youth and parent co-researchers in our previous work. Each subgroup of youth, sibling, and parent/guardians’ participants will be encouraged to complete story entries a minimum of once per month for 6-month. Non-entries or incomplete entries will not be included in across-case thematic analysis and require no additional analytic provision as missing data. Frequency of data entry, durations between entries, and frequency (and effectiveness) of follow up reminders will be documented to provide insight into use and platform sustainability. Arts-based data methods are a developmentally appropriate approach to inclusion data collection with youth and have been a rich source of complementary data across the lifespan in our previous work (Archibald et al., 2014a, 2020a).
Participants will be able to enter free text stories and tag those stories in accordance with the 6 F-word and content tags (e.g., school, bullying, sleep) at any time of story entry and with no maximum frequency. Definitions of each F-word and information on “what makes a good story” as identified through our mixed methods research (e.g., diagnosis, communicating with friends, transitions in school) (Archibald, 2022) will be available to serve as guidance to participants. Participants may elect to submit one or more stories on singular or multiple topics, depending on life experiences, life changes, current needs, and reflections. Participants will be encouraged to submit their associated artistic entry if not received at the time of story submission, using a personalized reminder email. Similarly, personalized reminders will be sent to participants who have not yet completed their diary entries in the third week of each month (monitored through a date of last entry progress notation within the lab administration section). Following the entry of each story, the research team (i.e., principal investigator and research coordinator) will be notified using the living lab platform specific notification email; stories will be reviewed for sensitive and identifying information. Participants will receive a $20 gift-card in recognition of each month completed. A subset of families will be contacted for usability follow up immediately after data collection concludes.
Stage 2
We will build off thematic analysis of participant stories and prioritization of the F-word tags utilized in stage 1 to develop an arts-based KT resource to communicate an important aspect of the findings (e.g., key messages for a subgroup of participants). We will work with a subset of participant advisors to inform the co-design of this resource over a 6-month period. We expect that different F-words will be prioritized across youth, sibling, and parent/categories; as such, we will utilize an inverted rank ordering method used successfully in our previous work (Archibald et al., 2020b) and consultation with participant advisors to determine priority selection for KT resource development. Using Zoom video-conferencing software, (Archibald and Blines, 2021; Archibald et al., 2019) we will engage the participants in a series of 4 co-design sessions involving 6 asynchronous steps to develop the arts-based KT resource, guided by our previous work (Archibald et al., 2021a). $25/hour honorariums will be provided to each participant advisor in alignment with best practice standards (CIHR, 2022). Draft KT resources will be shared on the living lab platform to encourage narrative feedback from all stage 1 participants over two 2-week cycles of feedback and iterative revision. The KT resource will then be hosted on the living lab platform and a link to its access provided to all staff at the partnered facility.
Stage 3
Fifteen youth, sibling, and parent/guardian participants from stage 1 – aiming for 5 per subgroup – will be purposively sampled with considerations for diversity in sex, gender, age, ethnicity and with consideration to level of system use (e.g., low to high engagement) and with consideration of the intersection of these categories, to complete a brief usability questionnaire and semi-structured usability interviews immediately following the stage 1 data collection period. The System Usability Scale (SUS) will be used and will be administered using a secure and user-friendly online platform (e.g., SurveyMonkey™, Qualtrics™). The SUS is a 10-item reliable and validated instrument that measures users’ subjective perceptions of system usability using a 5-point Likert scale (Hyzy et al., 2022). As close to scale completion as possible, a semi-structured follow up interview will be conducted to expand upon and explain the SUS ratings, and to provide supplemental data into platform utility, motivations for use, perceived benefits and challenges including areas for future platform improvement. Interviews will be conducted over the secure Zoom videoconferencing platform – which we have used successfully in previous research (e.g., Archibald et al., 2019) or over the telephone, based on participant preference.
Clinicians: Following a 2-month KT resource review period, 15–20 clinicians will be recruited to complete semi-structured interviews to investigate the usability and acceptability of the living lab platform. Central usability constructs of system effectiveness, efficiency, user attitudes and acceptability of system use will be assessed, as will reasons for non-engagement, to inform future platform refinements and expansion.
While the foundation of the usability framework originates from the realm of human-computer interaction in the late 1970s, Dr Nielson introduced the concept of usability engineering, which has since become pivotal in assessing and enhancing user experiences (Liew et al., 2019). The components of the usability framework encompass several vital elements, commencing with user analysis and delving into the needs, goals, and behaviors exhibited by individuals engaged with a product (Liew et al., 2019). Mixed methods evaluation will provide insight into pertinent usability domains while enabling investigation into specific platform attributes.
Data Management and Analysis
Stage 1
Longitudinal qualitative research using interpretive description is ideal for generating robust understandings of dynamic family experiences and to informing iKT given its emphasis on clinical application of research data, the ability to move beyond mere description of findings, and because the approach is amendable to integrating arts-based data sources (Thorne, 2008). Using the mixed methods data management and analysis software MAXQDA, the story entries for each subgroup will be read repeatedly to gain a sense of the whole, prior to conducting line-by-line coding. Codes from the first 3 transcripts will inform a coding framework to apply to remaining entries within and between each dominant F-word grouping. New data from within-category story entries (e.g., in the “function” category) will refine the coding (Charmaz, 2014). Codes will be grouped into themes to facilitate sub-group comparisons enabled by heterogeneous sampling (e.g., age and gender-based comparisons); themes will be clustered in the dataset and subgroups, and thematic labels modified as needed (Braun & Clarke, 2006). Data will be examined within subgroups and then compared across subgroups to identify patterns and distinctions. Arts-based data will be analyzed by form (e.g., photography, drawing), key content, constituent elements, and tone using a framework successfully applied in our previous work (Archibald et al., 2014a), and handled holistically with narrative data. F-word categorization will be tallied and descriptively analyzed to suggest prioritization and guide selection for KT resource development. Recognized qualitative trustworthiness criteria will be used to assure research quality (Tobin & Begley, 2004). Using this approach, incomplete monthly entries will have no analytic impact as entries are analyzed thematically across categories. System use data (frequency of story provision, frequency and number of reminders required, effectiveness of reminders) will be descriptively analyzed using the SPSS function in MAXQDA management software and considered in relation to stage 3 usability data.
Stage 2
Feedback provided through the iterative feedback-revision cycles will be categorically collated and content analyzed to enable clear identification of suggested improvements (e.g., categories of imagery feedback, format feedback, key message feedback etc.). Data analysis will occur immediately following the first 2-week feedback cycle, be used to modify the draft KT resource (e.g., storyboard), and a summary of modifications communicated along with the revised draft to participants on the platform. Following a 2-week analytic and revision window, the revised resource will again be shared, a second round of feedback attained, and content analysis will be used to inform penultimate modifications to the draft resource as required.
Stage 3
Following the sequential explanatory mixed methods design procedures, quantitative data from the SUS will be inputted into MAXQDA, descriptively analyzed, and then further explored through semi-structured interviews to provide a more comprehensive understanding of the platform usability and acceptability (Creswell & Plano Clark, 2018). Numerical data will be cleaned and while missing data is not expected due to opportunities to follow up with research participants in the qualitative data collection phase, missing data will be handled with imputation methods (i.e., based on mean value for variable), as required (Polit & Beck, 2021).
Following the quantitative analysis, recorded interview data will be professionally transcribed verbatim. Audio recordings will be listened to repeatedly to gain a sense of the whole and to assist with data cleaning. Qualitative data will be analyzed using direct content analysis (DCA) –a common approach in healthcare research that involves categorizing and coding data based on predetermined concepts (e.g., usability constructs) (Assarroudi et al., 2018).
Qualitative data patterns will be categorized according to domain (e.g., feature), usability construct (e.g., aesthetic, efficiency) and subgroup (e.g., type of user, population), and integrated with descriptively analyzed numerical data using a joint display (Guetterman et al., 2015). A joint display is a visual representation used to facilitate integration of data sources and types, capture comprehensive data from both modes of inquiry, and promote transparency, rigor, and ease of communicative reporting (Creswell & Plano Clark, 2018; Guetterman et al., 2015; Richards et al., 2019). Data will be further integrated with system generated data on the length and frequency of system use within the joint display, to provide a comprehensive picture of system usability and to guide future improvements.
Patient and Public Involvement
This study is part of a patient and family engaged research program which at various stages has involved a participant advisory group, and systematically builds upon the research and knowledge exchange needs of youth and families identified in our previous work (Archibald et al., 2021c). It reflects engagement and alignment with family experiences, preferences as well as the priorities of a pediatric rehabilitation services facility. The co-design of the KT resource with interested participants will encourage additional involvement.
Ethics and Dissemination
The Research Ethics Board at the lead authors institution approved this study (HE2022-0397). Site access approval was obtained from the partnered rehabilitation center. Study participants will receive non-technical summaries of the research findings through email, along with a link to or attachment with the KT resource, depending on its format. The KT resource will be hosted on the living lab platform once the KT resource feature of the living lab platform has been operationalized. The KT resource, depending on its format, will also be hosted on the lead authors website and YouTube channel, and promoted through the respective channels of our collaborators and partners. Academic findings will be published in open-access journals to promote family and partner accessibility; presentations at local and international conferences will extend reach. Opportunities for co-presentation of findings will be offered to participant advisory members as appropriate.
Rigor
The trustworthiness (qualitative rigor) of the proposed research will be upheld using a range of strategies, as informed by Tobin and Begley (2004). First, our commitment to aligning the ethical and methodological tenets of the study by way of internal consistency and through attention to the CIHR-Knowledge to Action Ethics framework (2018) in relation to accessible and inclusive research practices, upholds study credibility. The longitudinal design and triangulated usability findings will provide insight into the nature of participants experience, and factors influencing the sharing of these experiences within the platform, thereby upholding credibility. Use of interpretive description and the orientation towards KT resource development speaks to values around transferability, wherein the core aspects of experiential findings are made available for assessment, resonance, and use by other families. The iterative process of data collection, management, and analysis is consistent with rigorous qualitative research practices (Thorne, 2008). Integrating arts-based data has the potential to enhance data depth and richness, and with debriefing with participant advisors, contributes to confirmability.
A high degree of participant involvement throughout this programmatic work, including the co-design of the arts-based KT resource and the participant advisory group, further strengthens trustworthiness by encouraging the integration of participant perspectives and preferences into the research process, thereby upholding credibility and transferability.
Discussion
There is much progress to be made in understanding and using the experiences of families to improve care (Greenhalgh et al., 2011). The global movement towards participant and patient involvement in healthcare research and practice reflects knowledge that research is best situated within the experiences and priorities of families tasked at realizing its relevance in the context of their everyday lives. In this study, we draw upon our foundational research on living labs (Archibald et al., 2021c; Archibald, Wiebe, et al., 2021b) and their potential as integrated knowledge translation systems, as well as artistic and story-based methodologies employed for effectively communicating intricate health information (e.g., Archibald et al., 2018; Archibald & Blines, 2021; Archibald & Gerber, 2018). Our aim is to generate a repository of stories of lived experience to encourage knowledge exchange and familial connection in relation to neurodiversity, along with a more thorough understanding of the priorities, strengths, and areas for improvement in care, by leveraging storytelling as a crucial strategy for advancing family-centered care.
Within the health sciences, storytelling has gained traction for its capacity to communicate complex health information (e.g., Scott et al., 2009), as a way of individual and collective sense-making, and also in recognition of its longstanding and rich history as an Indigenous way of knowing and methodology (Absolon, 2022; Brooks et al., 2022). Story is often how we make sense of our experiences of the world and through reading the stories of others, locate our own experience and gain access to opportunities to acknowledge and understand the behaviors of others. Incorporating artistic responses alongside story-based responses will enable a holistic perspective of participant experiences, and a visual context for interpretation and analysis (Archibald et al., 2017), and visual anchors to incorporate into future KT resource development. The possibilities for creating a story repository based on the information exchange needs of contributing participants are plentiful; we anticipate that this work will open new avenues for iKT involving resource co-design, broad mobilization of lived experience data, and scale-up of a story-based repository of lived experience data.
Research highlights a disconnect between family and care providers perspectives regarding family centered care (Kuo et al., 2012), and a critical need for innovative systems that help mobilized knowledge of familial lived experience (Archibald et al., 2021c). iKT can help move towards shared understandings, illuminating the perspectives of various knowledge users for whom research evidence is intended (Archibald et al., 2021a; Kitson et al., 2013). Our research has demonstrated the power of iKT in identifying critical participant experiences, developing arts-based KT resources for communicating findings (e.g., communicating complex research evidence using storytelling, with the storyline based on family experiences), including communicating diverse perspectives (Archibald & Blines, 2021; Archibald et al., 2014b, 2018; Archibald & Scott, 2019). We previously developed a rigorous approach to creating arts-based KT tools that are based on a comprehensive understanding of lived experience and knowledge needs, and that integrate these findings with gold standard research evidence (Archibald et al., 2018; Archibald & Scott, 2019). In the context of childhood neurodiversity, the provision of resources to support wellbeing and family centered care is well supported (Kuhlthau et al., 2011), yet further attention to the development of such resources is warranted and reflects a marked opportunity to co-create meaningful evidence-based resources reflective of family experiences. The living lab platform will provide the needed infrastructure for this user-centered co-design, enabling feedback cycles with multiple participants in an engaging and cost-effective manner, and providing a mechanism for future implementation and evaluation of the system and accompanying resources.
Limitations
This study is designed to simultaneously gather data on lived experience across three subgroups and elicit understanding of the usability of the platform. Participant attrition may result from the longevity of the data collection period and asynchronous mode of data collection; however, insights into these occurrences will be gained through usability testing. Variability in the quality and length of stories produced is likely and will also be assessed in usability testing to inform the need for future refinements, such as more storytelling parameters. Unequal numbers across the subgroups may also occur and will provide important insight into propensity of platform use.
Footnotes
Acknowledgements
We gratefully acknowledge the support from the rehabilitation service center and associated foundation, including that of Barb Borton, Director of Rehabilitation and Clinical Services at the partnered rehabilitation centre. We acknowledge the contributions of parent partner Carrie Costello, engineer Shea Hunt, in relation to earlier stages of this project, and the consultation of Peter Rosenbaum, Rachel Tiplicky, and Andrea Cross in relation to the F-words for the current initiative. RLW is supported by a Tier 1 Canadian Research Chair (CRC) in Child and Family Engagement in Health Research and Healthcare (CIHR – Canadian Research Chair – 950–231845). KW is supported by the Dr. John M Bowman Chair in Pediatrics and Child Health (Endowed Chair, Rh Institute Foundation and University of Manitoba).
Author Contributions
MA conceptualized the study, wrote and finalized the protocol. OA drafted the manuscript and is involved in study coordination. EH, RW and KW contributed to study conceptualization, reviewed the manuscript and approved the final version. AM contributed to drafting stage 3 of the manuscript, and approved the final version.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: KW is a clinician and Research Director, BB is Director of Rehabilitation and Clinical Services, and EH is a Research Associate at the partnered rehabilitation center. None are directly involved with participant recruitment.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by a Research Manitoba New Investigator Award.
Ethics Statement
Data Availability Statement
Data sharing not applicable to this article as no datasets were generated or analyzed during the current study.