
Abstract
Participatory Health Research (PHR) has the potential to result in more equitable health interventions and impactful research outcomes, and is an increasingly used paradigm in migrant health research. In the context of intersecting systems of social disadvantage imposed on migrant and refugee women, PHR could offer an opportunity for researchers to challenge unequal power dynamics in academic research by co-creating knowledge to improve these women’s healthcare access and use. However, there is limited information about how PHR has been conducted with migrant women, including the extent of their involvement throughout the research process. This scoping review aimed to describe and summarize current evidence on the research approaches and methods that have been used in PHR with women of migrant and refugee backgrounds living in high-income countries, and the extent of community engagement in PHR with this population. We searched MEDLINE Ovid, CINHAL, Scopus, and Web of Science databases from 1 January 2012 to 31 December 2021 to identify qualitative, quantitative, and mixed method studies adopting a PHR approach with migrant women as participants. We included 91 studies from 12 countries. Health topics of included studies included: knowledge, screening and prevention of HPV, cervical and breast cancer, mental health, nutrition and physical activity, gender-based violence, and health promotion and education. The most common PHR approaches were Community-Based Participatory Research and participatory action research. Overall, community engagement was commonly reported in most stages of research; however, participatory engagement with migrant women was more often done by proxy through community organisations or agents, rather than women themselves. We argue that more rigorous reporting of community engagement is necessary to demonstrate PHR conducted with migrant women is following the principles of equity and inclusion in community-academic partnerships.
Background
Participatory research is a paradigm and an umbrella term describing different research approaches that centre the inclusion, recognition, active participation and engagement of individuals, social groups, stakeholders, or communities who are intended to benefit from the research (Cargo & Mercer, 2008; Higginbottom & Liamputtong, 2015; International Collaboration for Health Participatory Research (ICPHR), 2013). Compared to non-participatory approaches, participatory research can improve the relevance and interpretation of results by providing cultural validity, congruence, and sensitivity through the collective construction of knowledge alongside participants with lived experience of the issue or topic studied (Cargo & Mercer, 2008; Higginbottom & Liamputtong, 2015). However, the purpose of participatory research goes beyond the generation of knowledge: it also aims to translate research into positive impactful change or action that improves the well-being of the research participants, communities or social groups involved (Higginbottom & Liamputtong, 2015; Vaughn & Jacquez, 2020).
Participatory research ideally acts as an ‘equaliser’ between academic researchers and participants by sharing power and control over the research project and is therefore useful in health research aiming to understand the intersection between social inequity and health outcomes (Higginbottom & Liamputtong, 2015). As a result, it is often advocated for research with groups that are affected by unjust power imbalances and have historically experienced racism or discrimination, including Indigenous and Aboriginal people, people with disabilities, ethnic minorities, and people from refugee, asylum seeker and international migrant backgrounds (Higginbottom & Liamputtong, 2015).
Participatory health research approaches have the common fundamental principles of democracy and active participation, with the focus population at the core of the research, preferably from inception to dissemination (Cargo & Mercer, 2008; International Collaboration for Health Participatory Research (ICPHR), 2013). Therefore, the focus population is not just a source of data, but participants actively engage in the development and implementation of the research project by collaborating with the academic team. This includes involvement throughout: (1) defining the research question, aims and design, (2) collecting data, (3) selecting analysis methods, (4) interpreting the results, and (5) sharing the findings with stakeholders and the larger community (International Collaboration for Health Participatory Research (ICPHR), 2013). In practice, ‘active participation’ throughout participatory health research may be limited for several reasons, such as participant’s time availability and fixed timelines by the academic team, mismatched expectations or conflicts caused by unequal power dynamics amongst community members, and between the community and the academic team, and lack of social accountability from research projects (International Collaboration for Participatory Health Research (ICPHR), 2021bib_icphr_2021)
Participatory Health Research with Women of Migrant and Refugee Backgrounds
International evidence shows that many women from refugee, asylum seeker and international migrant backgrounds (here forth ‘women from migrant backgrounds’) have limited access to health care because of health insurance regulations, language barriers, transport, difficulties navigating a new system, discrimination, and lack of cultural safety or appropriateness (particularly regarding sexual and reproductive health) (Billett et al., 2021; Fair et al., 2020; Jesuthasan et al., 2019; Richter et al., 2020). Participatory health research could offer an opportunity for women from migrant backgrounds and academic researchers to co-create knowledge that could translate to improved healthcare access and services, policies, and regulations. In participatory research, academics and participants are involved in decision-making throughout the research process (Gunella & Rodrigo, 2022). Women from migrant backgrounds often experience gender- and race-based discrimination, and participatory health research could place women on a more equitable position in research where their health and well-being needs are prioritised. For example, recent evidence shows that health interventions for migrant people developed with participatory research approaches were better suited to their target population values and priorities, encouraged a better understanding of the health topic of focus, and increased community determination to make positive change according to their needs (Rustage et al., 2021).
Women play an important role in the holistic improvement of their families and communities, and can provide with valuable insights to address health issues (Decker et al., 2010). However, in the past, feminist academics noted that in participatory research and development projects, women were not included as community representatives, or in group settings where women were present, their participation was minimised (Decker et al., 2010). Therefore, it is important to examine if current participatory research with this population is fostering active participation of women through the research stages and the research decision making process.
Scoping Review Aims and Review Questions
Scoping reviews are useful to examine the ways in which research has been conducted on a specific area, to identify gaps in knowledge, and identifying the main characteristics of a concept or existing literature (Munn et al., 2018; Tricco et al., 2018). To our knowledge, there are no scoping reviews summarizing the types of participatory health research approaches and methods used specifically with women from migrant backgrounds. Importantly, the extent of participatory engagement in research with this population is similarly under-reported. The aim of this scoping review is to provide a descriptive overview of which participatory approaches and methodologies have been used in health research with women from migrant backgrounds living in high-income countries. This scoping review aimed to answer the following review questions: (1) What participatory health research approaches have been used with women from migrant backgrounds living in high-income countries? (2) What is the extent of community engagement of women from migrant backgrounds in participatory health research? and (3) Which research methods have been used in participatory health research with women from migrant backgrounds living in high-income countries?
Methods
This review is reported using the Preferred Reporting Items for Systematic Reviews and Meta-analysis extension for scoping reviews (PRISMA-ScR) (Tricco et al., 2018). (Appendix 1) and the protocol was registered with Open Science Foundation (DOI: osf.io/5afmv).
Eligibility Criteria
Characteristics of Included Studies.

aFor studies with >1 papers, we recorded date of first paper publication.
bThe multicounty studies were conducted in Italy, Portugal, and Spain, (Alhassan et al., 2016) and Belgium and Netherlands (Keygnaert et al., 2012).
Search Strategy for Identification of Studies
We searched MEDLINE Ovid, CINHAL, Scopus, and Web of Science databases using a search strategy that we created for this review (Appendix 2), including key terms for the population and research approaches related to the broad concepts of “women,” “refugee,” “asylum seeker,” “migrant,” “participatory research,” “community engagement” and “health.” There was no limitation in geographic location, or language. Date was limited from the inception of databases to 31 December 2021. We decided not to extend the search strategy into grey literature databases as we considered the large number of included peer-reviewed papers during full text assessment sufficient to represent participatory health research practice. During eligibility assessment of full text papers resulting from the database search, in the case of implementation and evaluation studies, we searched in the full text papers for formative research references and assessed the resulting full text papers for eligibility.
Selection of Studies
Results of the database search were imported into Covidence (Veritas Health Innovation, 2022) for reviewing. Two reviewers (MVC, AH) independently screened all publications in two stages: (1) Title and abstract screening for preliminary selection according to our inclusion and exclusion criteria; (2) Full text screening of the selected articles in the previous stage for final inclusion in the review. All disagreements between the two reviewers were resolved through discussion with at least another reviewer (MAB, KB, CV).
Data Extraction and Synthesis
Two reviewers (MVC and AH) extracted all relevant data using a charting form designed and tested for this review, including information on study characteristics, aims, design and setting, methods of data collection, analysis and dissemination, health topic studied, participants and participant place of origin. The extracted data by the first reviewer (MVC) was then double reviewed against the journal articles by the second reviewer (AH) to ensure data relevancy and completeness. Disagreements in extraction were resolved through discussion with at least another reviewer (MAB, KB, CV).
Participatory engagement in the following stages of research was recorded (yes/not reported): inception and/or development of study aims, designing the study, data collection, data analysis and/or interpretation of findings, and non-academic dissemination of findings with the broader community and public. For recording engagement in data extraction, if it was not clearly stated the people doing data collection were part of the community of interest, we recorded it as “not reported” even if they spoke the community’s language. We do not report on community engaged academic dissemination of findings (i.e. where community members were listed as co-authors in papers) since reporting was not consistently clear throughout studies to accurately identify those cases.
In studies where authors reported participatory engagement in a research stage but did not provide further details on how the community was engaged, we recorded it as “not specified”. We do not report on research methods that were not participatory (e.g., if interviews were designed and conducted with peer researchers but the same study used surveys where the community was not engaged, we only report on the interviews). We synthesised extracted data into tables and used descriptive statistics to allow comparison across categories.
Results
We identified 2122 records from the database searches. Ninety-nine papers met the eligibility criteria, and one paper was identified from reference search during full text screening. The 100 eligible papers were then merged by study (e.g. where more than one paper was included from a single study), resulting in 91 included studies published between 2012 and 2021, all in English (Figure 1. PRISMA flowchart). PRISMA flowchart.
Characteristics of all Included Studies
Table 1 reports the main characteristics of included studies. In summary, the 91 included studies were conducted in 12 high-income countries: 66 studies in North America, 13 studies in Australia, 7 studies in Europe, 4 studies in the United Kingdom, and 1 study in Asia. The most common health topic in the included studies was knowledge, screening and prevention of HPV (Human papillomavirus), cervical and breast cancer (18/91, 19.8%), followed by mental health (13/91, 14.3%), nutrition and physical activity (11/91, 12.1%), gender based violence (10/91, 11.0%), health promotion and education (10/91, 11.0%), child health and nutrition (8/91, 8.8%). Less common health topics in the included studies were primary health care access and utilisation (6/91, 6.6%), sexual health (5/91, 5.5%), maternal health (4/91, 4.4%), health inequalities (2/91, 2.2%), occupational health and safety (2/91, 2.2%) and oral health (2/91, 2.2%).
Participatory Health Research Approaches Used with Women of Migrant Backgrounds Living in High Income Countries
Most studies described their participatory health research approach as community based participatory research (CBPR) (52/91, 57.1%), or as participatory action research (PAR) (13/91, 14.3%). A subgroup of studies descried their participatory approach with broader terms such as participatory research, methods, design, or approach (6/91, 6.6%), community-engaged or community-based research (6/91, 6.6%), or community-academic partnership (3/91, 3.3%). The remaining studies were described as either Photovoice (5/91,5.5%), community-based collaborative action research (2/91, 2.2%), participatory concept mapping (2/91, 2.2%), community asset mapping (1/91, 1.1%), and appreciative inquiry (1/91, 1.1%) (Appendix 3(a)). Five studies did not report engagement with the community of research interest beyond an initial community consultation or advisory group and were not included further in the data synthesis of this review (Appendix 3(b)).
Additional Characteristics of Included Studies
Additional Characteristics of Studies With Some Community Engagement Beyond an Initial Consultation or Advisory Group.

aincluding 1 study with (trans)women as participants. (Rhodes et al., 2015).
Participatory Engagement by Research Stage
Table 3 presents participatory engagement by research stage and type of community engagement. For the purpose of this review, we categorised community participatory engagement into three mutually exclusive types: 1. Engagement with community agents: community organisations, community leaders, community health workers and educators, and community members trained as peer researchers, that were involved in any research stage but were not considered participants of the study. 2. Engagement with participants: members of the community who were involved in any research stage but also provided data as research participants during the data collection stage that was later analysed in the study. 3. Engagement with community agents and participants: both community agents and participants were involved in a research stage. Participatory Engagement by Type and Research Stage Used in Participatory Health Research With Women of Migrant Backgrounds.
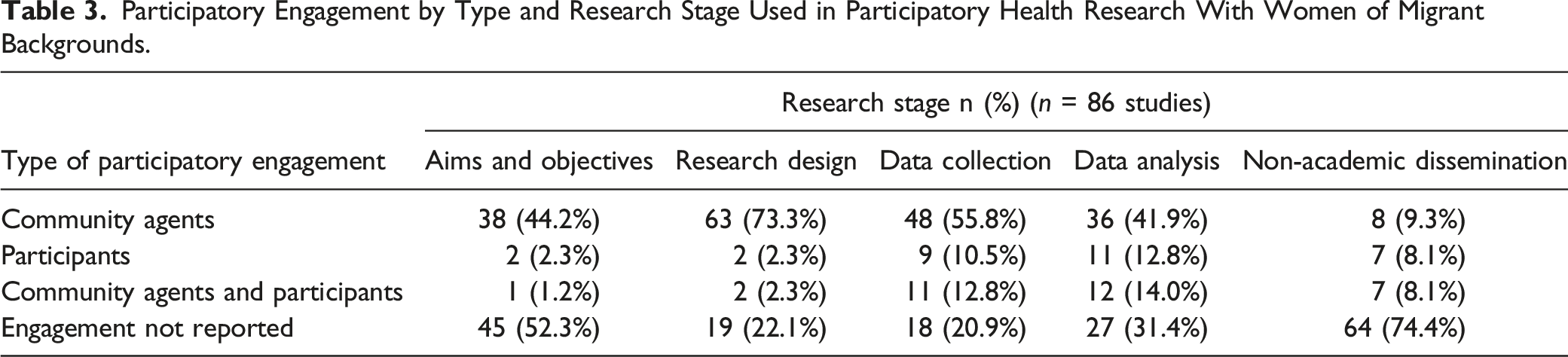
There was variable reporting of participatory engagement of any type across the research stages: Data collection (68/86 studies, 79.1%), research design (67/86 studies, 77.9%), data analysis and/or interpretation of findings (59/86 studies, 68.6%), development of aims and objectives (41/86 studies, 47.7%) and non-academic dissemination of research findings (22/86 studies, 25.6%). Only ten studies reported community engagement in all stages of research. Interestingly, the most common type of participatory engagement reported throughout all stages of research was engagement with community agents, and it was the highest in the research design stage (63/86 studies, 73.3%). For comparison, only two studies (2.3%) had engagement with participants in the research design stage.
Engagement with participants was equally low in the development of research aims and objectives (2/86 studies, 2.3%), compared to engagement with community agents (38/86 studies, 44.2%). Data collection and analysis were the research stages where engagement with participants and engagement with participants and community agents was more common, yet it was only reported in between 10 to 14% of studies in each of those stages. Participatory engagement in non-academic dissemination of research findings with the broader community was commonly under reported, with only 22/86 studies reporting some type of engagement. Engagement with participants only was more prevalent in the data analysis stage (11 studies, 12.8%) and data collection stage (9 studies, 10.5%) compared to other research stages. Engagement with both community agents and participants followed a similar frequency pattern as engagement with participants only.
Participatory Research Methods
Research Methods With a Participatory Approach Used in Participatory Health Research With Women of Migrant Backgrounds.
aPercentages >100%, categories are not mutually exclusive.
bFocus groups, survey discussions, conversation café, workshops.
cPhoto-elicitation interviews, participant generated photographs and discussions.
Data Collection with a Participatory Approach
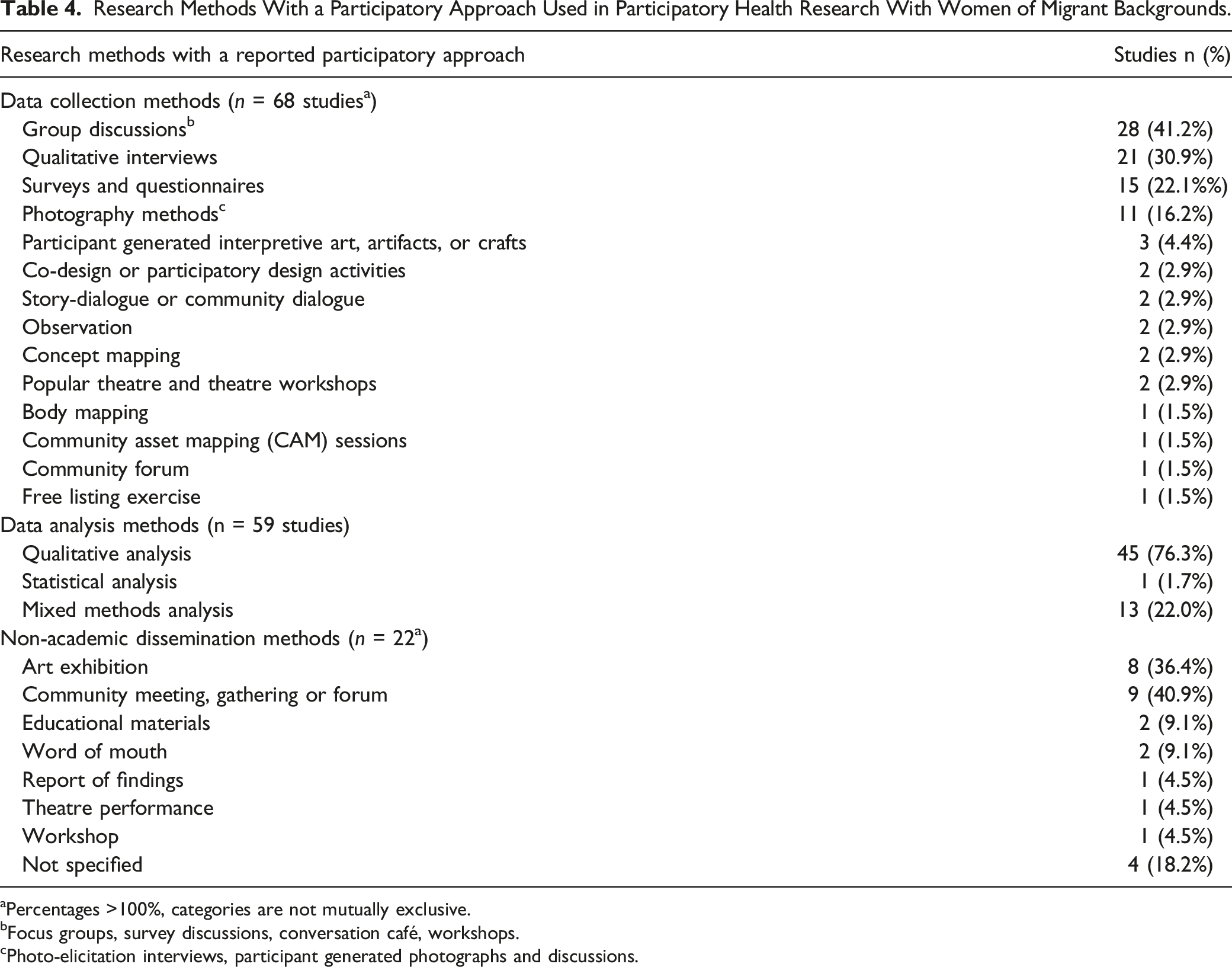
Out of the 68 studies that reported participatory engagement in data collection, 21 studies reported two or more methods of data collection. In total there were 14 data collection methods reported, and two studies did not specify how their data was collected (Table 4). The most common method of data collection was group discussion, including focus groups, survey discussions, workshops, and conversation café (28/68 studies, 41.2%), followed by qualitative interviews (21/68 studies, 30.9%), and surveys and questionnaires (15/68 studies, 22.1%). Arts-based methods of data collection were also common: 11/68 studies (16.2%) used photography methods including photo-elicitation interviews, and participant generated photographs and discussions, 3/68 studies (4.4%) collected data through participant generated interpretative art, artifacts, or crafts, and 2 studies (2.9%) through popular theatre and theatre workshops. Less common methods of data collection that reported participatory engagement were co-design or participatory design activities, story-dialogue or community dialogue, observation, concept mapping, body mapping, community asset mapping sessions, a community forum, and free listing.
Data Analysis Methods
We were not able to extract the specific analysis method most studies used due to inconsistent or lack of reporting, therefore we report on data analysis according to their study design. Of the 59 studies that reported participatory engagement in the analysis of data or interpretation of findings, 45 studies (76.3%) used qualitative data analysis methods, 13 studies (22.2%) used mixed-methods analysis, and only one study (1.7%) used a quantitative analysis method.
Dissemination Methods
Out of the 22 studies that reported participatory engagement during the non-academic dissemination of findings, six studies used more than one dissemination method and four studies did not specify how the dissemination was conducted (Table 4). The most common method of dissemination was art exhibition (8/22 studies, 36.4%), followed by community meetings, gatherings, or forums (9/22 studies, 40.9%), educational materials (2/22 studies, 9.1%), and word of mouth (2/22 studies, 9.1%). The least common forms of dissemination were report of findings, theatre performance, and a workshop.
Discussion
We identified the different approaches and methodologies used in participatory health research with women from migrant backgrounds living in high-income countries. Over half of included studies were conducted in the United States of America, around 30% were conducted in Australia and the United Kingdom, with the remaining studies conducted in Europe, and one study in Asia. Our findings show participatory health research with women of migrant backgrounds in high income countries is used to study a broad range of health areas covering non-communicable and communicable disease, health promotion, education and prevention, and health equity. Over 70% of included studies described as either CBPR or PAR, while the remaining used broader terminology such as participatory or community-engaged research, suggesting researchers chose a more flexible approach to research methodologies than the more strictly defined CBPR and PAR methods.
Community engagement was commonly reported in most stages of research across all studies. However, participatory engagement with women from migrant backgrounds was most commonly done by proxy through community organisations, community health workers and health educators, than direct engagement with the women as research participants. This was particularly true for engagement in the development of research aims and objectives, and research design stages. Limiting the engagement of participants in the early stages of research might happen for varied pragmatic or ethical reasons. Prioritisation of community engagement should be discussed with study participants and community organisations according to their time and engagement capacity. However, these reasons should be stated clearly by authors in academic publications. For example, in one of the included studies conducted in Simonsen and Ryom (2021) considered it inappropriate to involve the refugee women participants in their study in the development of research aims and design since their recent arrival to the country already placed pressure on them to fulfill different administrative and educational tasks. Therefore, the authors decided instead to prioritise the women’s participation in later stages of the research process (Simonsen & Ryom, 2021).
Most studies did not provide explanation on why participants or community agents were not engaged in some of the research stages. Additionally, while it is recommended to share the benefits of the research locally with diverse stakeholders to enable action (International Collaboration for Participatory Research (ICPHR), 2021), about three-quarters of studies did not report whether they had shared the findings with the broader community. This is an important finding of our review as engaging the community of interest in the research dissemination strategy shows commitment from academic teams to the transformative principles of participatory health research. Sharing results findings locally could provide an opportunity for community members to suggest and enact solutions to health issues, increase community members knowledge and change societal attitudes towards a specific health topic (George et al., 2023).
Strengths and Limitations
This is the first scoping review synthesizing the types of participatory health research approaches and methods used specifically with women from migrant backgrounds throughout the different stages of research in high incomes countries. We used robust and rigorous review methods, and our broad inclusion criteria allowed us to explore a large number of studies focused on diverse health areas. While we did not exclude any languages in our inclusion criteria, our search terms were only in English, and we did not have any search results in other languages. Additionally, community organisations with a focus on advocacy conducting independent participatory health research might not report their findings in academic journals and therefore would not have been captured by our search strategy. Lastly, community participation in the included studies was rarely reported in detail by authors, therefore while our findings show community participation was commonly reported across the different research stages, the true extent of how much or how little the community participated in the research process could not be determined by this review.
Implications for Future Participatory Health Research
Through the data synthesis of this review, we identified the following gaps in (1) participatory research approaches, (2) health areas of study, and (3) Participatory health research reporting. First, studies conducting participatory health research with women of migrant backgrounds across all health areas in high income countries typically reported following either CBPR or PAR approaches. However, very few of the included studies engaged women who were research participants in the research decision making or planning. Limited inclusion of participants in research decision-making could signify a higher risk of replicating oppressive societal dynamics in which the autonomy of women of migrant backgrounds is either ignored or suppressed. Therefore, we propose that more radical participatory approaches that give participants more control over the research process could be useful for the advancement of health equity of women in this population, such as feminist action research, defined by Reid (2004) as a framework “that enables a critical understanding of women's multiple perspectives and works toward inclusion, participation, action, and social change while confronting the underlying assumptions the researcher brings into the research process”.
Second, our review identified few participatory research studies whose aim was specific to maternal, sexual or reproductive health and rights of women from migrant backgrounds. Given that recent evidence shows migrant and refugee women have difficulties accessing and utilising sexual and reproductive health services (Billett et al., 2021; Davidson et al., 2022), we identify this as an important area of future study for participatory health research. Additionally, most included studies took place in urban settings, therefore we encourage future participatory health research to explore the health of migrant women living in rural and regional settings in high income countries.
Third, we identified clear opportunities for improvement on research reporting in participatory health research. In the context of intersecting systems of oppression affecting the social determinants of health of migrant women, more rigorous and transparent reporting of their involvement and decision making in the participatory health research stages is needed to demonstrate whether the principles of democracy, equality, and inclusion are being practiced. Ideally, participatory health research with women of migrant backgrounds should also take it into consideration gender dynamics while designing research projects and report their impact throughout the stages of research. More detailed reporting on the practicalities of methodological approaches for analysis, data collection, and non-academic dissemination of findings being used on participatory health research is also needed to guide future research. This is particularly relevant for those aiming to use innovative methods in participatory research to facilitate engagement with women of migrant backgrounds and their community. This could include art-based methods, which can be less reliant on written expression, making them more accessible to people of all languages and educational levels.
As other considerations for participatory health research, participants in the included studies were often recruited broadly by geographical region of birth such as Latin America, the Caribbean or Africa (Appendix 3(a)). We note that shared ethnicity or geographical region of birth do not necessary equate to “community”. Migrant communities are heterogenous and therefore so are their health needs and priorities, and as such, researchers should be mindful of biases around concepts of identity and community. Furthermore, researchers working on participatory health research via community agents must recognise that these agents might not always represent the interests of the communities they aim to serve (International Collaboration for Participatory Research (ICPHR), 2021).
Conclusion
We used scoping review methods to explore how participatory health research is conducted with migrant women in high-income countries. Through the synthesis, we identified three key gaps in participatory research with migrant women: (1) approaches to participatory research that may disempower women, (2) expanding participatory health research with migrant women to extend into maternal, sexual and reproductive health and rights, and (3) the need for more rigorous research reporting about engagement with communities. Addressing these gaps will help to ensure that the participatory health research principles of equity and inclusion are being followed in future research practice with migrant women.
Supplemental Material
Supplemental Material - Participatory Health Research With Women From Refugee, Asylum-Seeker, and Migrant Backgrounds Living in High-Income Countries: A Scoping Review
Supplemental Material for Participatory Health Research With Women From Refugee, Asylum-Seeker, and Migrant Backgrounds Living in High-Income Countries: A Scoping Review by Martha Vazquez Corona, Alya Hazfiarini, Cathy Vaughan, Karen Block, and Meghan A. Bohren in International Journal of Qualitative Methods
Footnotes
Acknowledgement
We thank Patrick Condron for his feedback and support in the development of the search strategy for this review.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study is supported by an Australian Research Council Discovery Early Career Award (DE200100264, awarded to MAB). MVC’s time is supported by the Melbourne Research Scholarship and Human Rights Scholarship (University of Melbourne). MAB is also supported by a Dame Kate Campbell Fellowship. The funders had no role in the study design, data collection, analysis, decision to publish or preparation of the manuscript.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.