
Abstract
Nova Scotia's Supportive Care Program (SCP) is an individualized funding program that provides funds for people living with dementia (PLWD) or acquired brain injuries to purchase basic home care services such as personal care, respite, cleaning and cooking. The SCP has the potential to address the Quintuple Aim of enhancing care experience, improving population health, reducing costs, improving provider experience and improving health equity, yet qualitative evidence is lacking. The aim of this study is to use participatory program evaluation methods to evaluate the SCP and consider how effective it is in addressing the Quintuple Aim. The study objectives and corresponding methods are to (1) Co-develop a SCP logic model to guide the evaluation through consultations with a diverse group of stakeholders including PLWD, caregivers, care providers, researchers, government representatives, and nongovernment organizations, with attention to gender; (2) Evaluate the SCP based on the outcomes and outputs identified in the logic model using focus groups with PLWD, caregivers and home care providers, and interviews with PLWD and their caregivers; and (3) Mobilize knowledge about the ways the SCP addresses the Quintuple Aim through integrated knowledge translation activities with public, policy and research audiences. By focusing on clinically and socially vulnerable populations of PLWD and caregivers, the proposed evaluation of the SCP offers a valuable case in assessing the effectiveness of individually-funded home care in addressing the Quintuple Aim including health equity within the context of dementia care.
Introduction
This study evaluates the Supportive Care Program (SCP), a direct payment program administered by the provincial Department of Health and Wellness in Nova Scotia, Canada, that provides eligible clients who are people living with dementia (PLWD), or people living with acquired brain injuries, and their caregivers with funds to off-set some costs of care in the home (Government of Nova Scotia, 2022). Through the SCP and supported by a caregiver, recipients may obtain up to $1000 a month for home support services including personal care, respite, housekeeping and meal preparation, and up to $495 annually for snow removal services.
The province of Nova Scotia has one of the oldest populations in Canada, high rates of chronic disease and disability, and 40% of the population lives in rural and remote areas, with high unmet care needs (Government of Nova Scotia, 2015). Supporting older people and their caregivers is a government priority in Nova Scotia (Government of Nova Scotia, 2017). Direct payments offer a promising service delivery model relevant to COVID-19 management and recovery efforts in service-poor areas (Kelly, Jamal, et al., 2021). In July 2020, the Government of Nova Scotia expanded the SCP as part of its COVID-19 pandemic response and to support people living with dementia to remain at home rather than in hospital as they waited for home care or long-term care (Government of Nova Scotia, 2020).
A majority of PLWD live at home and want to remain at home for as long as possible (Lepore et al., 2017). In providing people who may be in a vulnerable situation or residing in areas lacking services with funds to hire from the local community, the program offers an innovative approach to improving continuing care service delivery. The relational aspect of the eligibility criteria of the SCP make it distinct in Canada; eligible clients are PLWD and people with acquired brain injuries who have family caregivers with legal health decision making authority who can administer the funding in a supportive capacity (Kelly et al., 2020). By enhancing access to care at home, the SCP has potential to address the Quadruple Aim of enhancing client experience, improving population health, reducing costs, and enhancing provider experience (William Jackson Epperson et al., 2021) and specifically improving health equity for PLWD. Qualitative evidence regarding client and provider experiences with direct payments and health equity for PLWD is a knowledge gap. The goal of this study is to use participatory program evaluation methods to address the gap. This study is timely considering the challenges to providing equitable dementia care and the lack of evaluative evidence of home-based dementia care delivery informed by the Quintuple Aim framework.
Background
Dementia Care in Community
Care in community for people living with dementia is inconsistent and insufficient (Ward-Griffin et al., 2012). Advanced dementia care is often characterized by episodes of acute care, which intensify stress and distress for PLWD, as well as the family and friend caregivers who support them (Afonso-Argilés et al., 2020; Aminzadeh et al., 2012; Arriagada, 2020; Funk, 2019; Keefe, 2011; Liu et al., 2020). Social support offered in the home such as housekeeping, meal preparation and respite can help alleviate the work and stress that PLWD and their caregivers may experience.
Without access to appropriate supports, emergency hospitalization or refusals to accept discharge home may seem the only avenues for PLWD and families in crisis. There are strains on PLWD and caregivers as well as on the health system from the rising numbers of PLWD being hospitalized and categorized as receiving an alternate level of care (medically discharged) in the absence of home and long-term care services (Afonso-Argilés et al., 2020; Aminzadeh et al., 2012; Canadian Institute for Health Information, 2017; Johnson et al., 2018; Toh et al., 2017).
The ethical and practical challenges of providing appropriate dementia care also involves adopting person-centered approaches (Brannelly, 2016; Kitwood, 1997; Novy et al., 2022). Rather than solely understood as a disease, person-centered care requires conceptualizing dementia as a social and relational experience of the self in interaction and interdependence with others, and where environment and social and structural contexts impact care and caregiving (Fazio et al., 2018; Kitwood, 1997). Disablism and ageism shape experiences and responses to dementia; programs and professionals can seek to counteract these forms of discrimination through a person-centered approach (Aubrecht & Keefe, 2017; Brooker, 2004).
Delivering Home Care for PLWD Through Direct Payments
Direct payment funding models for home care are now present in many Canadian provinces, allowing individuals to receive money for eligible supports so they can select their own care workers (Kelly et al., 2020; Kelly, Jamal, et al., 2021). An assumed benefit of directly funded care is that it can increase the flexibility and choice of recipients (Cranford, 2020; Fleming et al., 2019; van Toorn, 2021). Less is known about the experiences of PLWD who participate in these programs, as direct payment programs for older adults and PLWD are relatively new (Dansereau et al., 2022; Fitzgerald Murphy & Kelly, 2019; Kelly, Jamal, et al., 2021). Emerging research provides some evidence that this funding model can enhance choice and flexibility for older people and their caregivers while reducing caregiver strain, with a caution that it can also add administrative burden on the caregiver, who effectively becomes the ‘family care manager’ responsible for finding, hiring, and supervising home care workers (Dansereau et al., 2022; Fitzgerald Murphy & Kelly, 2019). There is also a lack of recognition for home care workers’ choices and preferences compared to recipients, and underexamined tensions between clients’ and workers’ choices in home care provision (Cranford, 2020).
The Quintuple Aim, Health Equity and Intersectionality in Dementia Research
While locating people with dementia at the center of care is crucial to positive social and health outcomes, such outcomes are not always distributed equitably (Aranda et al., 2021). Dementia caregiving may come with significant financial, social and health costs (Duncan et al., 2020; Funk, 2019; Liu et al., 2020), particularly for historically marginalized and excluded people and communities who experience systemic barriers in accessing dementia care and realizing their full health potential (Bradbury et al., 2022; Di Lorito et al., 2021; Pharr et al., 2014; Richardson et al., 2019). There is evidence of gender, class and race-based disparities (Alzheimer Society of Canada, 2022; Sluder, 2020) within and among PLWD and caregiver populations that demonstrates the lack of health equity. Some PLWD have significant care needs (Eales et al., 2020; Keefe, 2011; Schulz et al., 2003), typically provided by family members who identify as female.
Existing qualitative research on dementia and intersectionality identifies social and geographic location as mediating factors in how people experience dementia (Hulko, 2009; O’Connor et al., 2010). In addition to the unequal gender dynamics and impacts of living with dementia as well as caregiving (Arriagada, 2020; Bartlett et al., 2018; Erol et al., 2015), the paid work of personal support and home care for PLWD is largely performed by immigrant, migrant and racialized women in low-paying, low-status roles (Cranford, 2020; Zagrodney et al., 2023). There is also a need to increase research and policy foci on 2SLGBTQQ+ communities’ access to dementia care (di Lorito et al., 2021; McGovern, 2014; Nowaskie & Sewell, 2021). Current evidence suggests that gender and other intersectional barriers, biases and disparities in dementia care have intensified under COVID-19 (Bradbury et al., 2022).
Health inequalities are rarely the result of a single category of exclusion. Intersectionality provides an analytic lens for understanding conditions that lead to and create health inequities (Hulko, 2004; Kelly et al., 2022; O’Connor et al., 2010). Health equity is one aim in the Quintuple Aim framework for health system improvements. To date, there has been limited research addressing dementia care using the Quintuple Aim framework (Sourial et al., 2022).
To address these empirical and conceptual gaps in dementia care research, and meaningfully engage PLWD and caregivers, our team developed a program evaluation study protocol that uses a participatory approach and visual methods in qualitative research on dementia care.
Study Design and Methods
The study has three objectives and corresponding methods: (1) Co-develop a SCP logic model to guide evaluation with a diverse stakeholder group comprised of PLWD, caregivers, care providers, researchers, and representatives of government, and nongovernment organizations, with attention to gender; (2) Evaluate the SCP based on the outcomes and outputs identified in the logic model; (3) Mobilize knowledge about the ways the SCP addresses the Quintuple Aim. Figure 1 provides an overview of this phased design, including the objectives and methods. Study phases including objectives, methods and participants.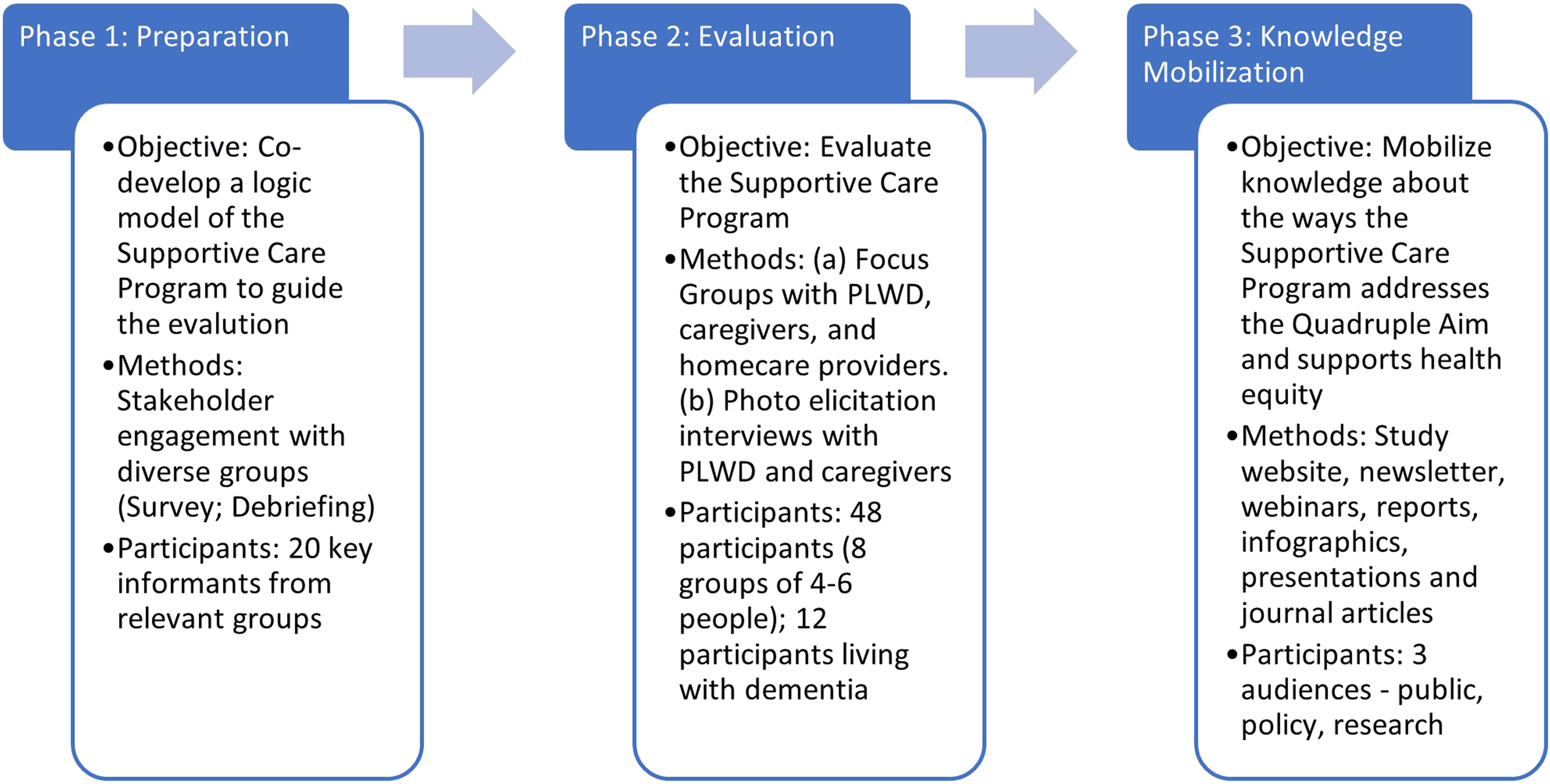
This study will involve conducting a participatory, interactive program evaluation aimed at policy and practice improvement (Owen, 2007). Aligned with a person-and-family-centered approach, the study design is “based on an assumption that those with an individualized vested interest in programmatic interventions within organizations or communities should also control the evaluations of these interventions” (Owen, 2007). We will follow evaluation strategies that begin with developing a program model, to explain how a program “contributes to a chain of intermediate results and finally to the intended or observed outcomes” (Funnell & Rogers, 2011), informed through stakeholder engagement to confirm that the model resonates with those who designed, use, or work with it. The result is a visual logic model that explains key actions, outputs and outcomes, and guides an evaluation of whether a program is working as intended (Mertens & Wilson, 2012).
A gender lens frames the overall research design (Bartlett et al., 2018), an intersectionality analytical approach that is crucial to the study’s examination of how the SCP meets the goal of health equity in relation to direct payments for dementia care in community. As such, we will seek to include agency and sole operator home care service providers as well as organizations that exist to provide community-based services to low-income individuals, Black, Indigenous and People of Colour (BIPOC), recent immigrants, minority language, and 2SLGBTQQ+ community members. To produce community informed and relevant knowledge, the study team will work in partnership and consultation with dementia and continuing care organizations with equity mandates.
Participants will receive honoraria to recognize their time and contributions. All data collection activities will be digitally recorded and transcribed to ensure verification of data accuracy. Field notes will be compiled during and immediately following data collection activities to capture observations and impressions. All activities will be conducted by investigators and/or research assistants individually or in pairs. Consultations and focus groups will be a mix of virtual and in-person encounters depending on practicality, safety, travel options and participant preferences and comfort.
Visual Participatory Methods
The selection of participatory visual methods in qualitative research on dementia care is based on evidence of their value and utility in meaningful engagement of participants living with dementia and their caregivers in research, and for supporting communication with people living with dementia (Killick & Allan, 2011; Phillipson & Hammond, 2018). Because semi-structured and structured interviews rely heavily on recall and verbal expression, they are often ill-suited, on their own, for engaging research participants living with dementia (Phillipson & Hammond, 2018). Visual methods involving video, photography and other images center people living with dementia in the research process and create and hold space for expression of their experiences (Killick & Allan, 2011). Beyond dementia research, visual participatory methods are highly effective in studies that seek to center participant voices and pursue co-produced knowledge (Mitchell et al., 2017). Such methods align well with the equity orientation of research guided by an intersectionality lens.
Photo-elicitation is the primary method that will be used in this study; this method is recommended to promote participation of people living with dementia in dementia research. In photo-elicitation, participants reflect on the content of images as part of a semi-structured interview or focus group (Darvell & Bradshaw, 2022; Lim et al., 2022; Parke et al., 2013; Rayment et al., 2019; Smith & Rodham, 2022). Photo-elicitation with ‘auto-driving’ (Shell, 2014), or, or an adapted version of the photo-voice approach in dementia research (Baker & Wang, 2006; see also Genoe & Dupuis, 2013; Wiersma, 2011), involves participants taking photos of their own choosing, images which are then used as interview prompts. Both forms of photo-elicitation will be used. While there are practical and ethical challenges associated with this method that will need to be considered and managed (Shell, 2014; Wiersma, 2011), this method adds validity and depth to dementia care research while providing participants more control over what is discussed.
Phase 1: Co-Developing a Supportive Care Program Logic Model
Consultations will aim at developing evaluation indicators to represent program outputs and outcomes. The team will collect information about stakeholders’ perspectives on the values embedded in the indicators and ensure that there is an accurate and representative set of indicators for all stakeholders that reflect both latent and manifest program goals.
Sampling
The method to co-develop the logic model of the SCP will involve consultations with the following stakeholder groups: PLWD, caregivers, care providers, researchers, representatives of government, and nongovernment organizations. To ensure regional/geographical representation across the province, we will seek representation from organizations and individuals in urban, rural, and suburban areas across the province. We will include system-level and provincial government decision-makers who create SCP policies and administer the SCP and other relevant policies and programs related to direct payments for dementia care in Nova Scotia.
Recruitment
To recruit participants, we will contact existing partners and networks including relevant provincial government departments, non-government associations that represent health and continuing care providers, and non-profit advocacy groups representing people with dementia and caregivers, all at the provincial level. We will also circulate the recruitment call for individuals to participate in stakeholder interviews through ads in print and online news media. There will be approximately 20 participants in the stakeholder consultations. We will seek proportional representation by population from each of the four Nova Scotia health management regions.
Data Collection
Steps in the consultation process will involve holding meetings with stakeholders to introduce the study, share the draft logic model, disseminate a survey and gather feedback from the survey. The survey will be online and gather information from the stakeholder about: • Contextual background about why they think the program is needed and what issues of power, discrimination and oppression exist in relation to the program; • Program activities and resources: what they think the key principles, beliefs or ideas guiding the program are; what resources are needed for the program; and • Intended program results: program outputs and outcomes, and what they think the main impact of the program is on users, home care providers and the overall health system.
Phase 2: Evaluating the SCP
Methods to evaluate the SCP based on the outcomes and outputs identified in the logic model will be focus groups and photo elicitation interviews with PLWD, caregivers and home care providers.
Sampling
Participants will be PLWD and their family/friend caregivers in Nova Scotia, as well as home care providers, both regulated and unregulated (or private) providers. 1 To be eligible to participate, PLWD and caregivers will have accessed the SCP at any point since April 1, 2017 (5 years from project funding date), for 3+ months. Efforts will be made to ensure diversity in terms of geography (minimum 1–2 per region), gender, ethno-racial, cultural, and rural/urban representation. Home care providers will include both senior level staff (management and direction) and frontline workers who are employed as home care providers or by agencies providing home care. We will aim to include employees from both regulated home care providers and non-agency workers (not recruited through an agency).
Recruitment
Participants will be recruited using purposive sampling. Recruitment posters will be circulated via project team networks, local media through paid ads (e.g., radio, print, online) and social media (Facebook, Twitter, LinkedIn, etc.).
Data Collection – Focus Groups
Focus groups will be with PLWD and their caregivers, and home care providers. We will conduct eight focus groups, composed of four to six participants per group, with one to two focus groups per Nova Scotia Health Management Zone. There will be a total of 32–48 participants total in eight focus groups.
Focus groups for home care providers and PLWD/caregivers will be in separate focus groups. We will ask participants in focus groups about manifest and latent (known but not publicly stated) program goals; program implementation; whether and how goals are achieved for people on the waitlist for publicly funded home or residential long-term care (e.g., by addressing some social/non-medical care needs), and how the program affects their lives and health (e.g., by providing clients and caregivers with funds to purchase services and supports that can enhance their quality of life, such as respite); and conditions of work among home care workers.
Data Collection - Interviews
Interviews with photo elicitation and photo voice will be with PLWD and caregivers. We will conduct 12 interviews with PLWD and their caregivers. Participants in focus groups and interviews will be offered the equivalent of $50 per hour in the form of gift cards as an honorarium.
Both photo-elicitation and photo-voice will be used as part of semi-structured interviews. In photo-elicitation, the interviewers will use images and photos to elicit responses and generate discussion. The images and photos will correspond to aspects of dementia care that the direct payments program could be impacting. In photo-voice, participants will be given a camera and be asked to take photographs about what they are able to do or acquire for their care through the direct payments they have received. They will independently take photographs and/or, where appropriate, be supported by a caregiver to take notes about the photos they have taken. The researchers will seek to conduct the photovoice interviews as soon as possible after the participant has taken the images to facilitate better recall given challenges with memory.
Phase 3: Knowledge Mobilization
This project uses an integrated-knowledge translation approach that meaningfully engages diverse stakeholder communities and includes PLWD, caregivers, home care providers and health system decision makers as research partners and project advisors (Keefe et al., 2020; Kothari et al., 2017). The key audiences for the study include PLWD and caregivers, policy-makers, and researchers and research outputs will focus on these key audiences.
Ethics
Potential ethical issues involve a possible risk to reputation or status for service providers, such as home care agencies, who may fear losing funding or contracts if there are perceived concerns about service quality. Similarly, people living with or providing care to someone with dementia may believe that access to care or the quality of the care they will receive is contingent on providing positive feedback on the type and level of services or programming available to them. To counteract these risks, the study team will ensure the confidentiality of information about participant identities.
Second, dementia-related cognitive impairment can impact capacity to consent to participate in research. The researchers will involve participants living with dementia in deciding on participating in the study but will adapt the research design and adjust consent and communication with PLWD as needed (Webb et al., 2020). This flexible and responsive approach includes drawing on leading knowledge about best practices in communication and relying on trusted family/friend caregivers (as authorized third parties) who can provide supported decision-making in accordance with the PLWD. The team will monitor consent including signs of dissent throughout the interview process. We will also ensure caregivers can share their own strategies for supporting communication with PLWD.
Third, there are inherent power differences between PLWD and caregivers and it is possible for caregivers to ‘take over’ interviews and speak for the PLWD. The study team will take steps to address this concern by emphasizing with caregivers the importance of ensuring that PLWD have a voice through written guidance and supporting caregivers with tips and strategies for allowing PLWD to communicate verbally and non-verbally.
Fourth, there are limits to anonymity and confidentiality in focus groups. Participants will be made aware that there are limits to their confidentiality and anonymity in the information letter they receive and in the consent process (including the consent form). Participants will be asked to keep the identities and content as well as data from the focus groups confidential by refraining from sharing any content from the focus groups publicly.
Fifth, participants engaged in photo-voice interviews may take pictures of other people (members of the public or family/friends) which requires consent. To use these photos, individuals will consent to having their picture taken and used in the study. To avoid participants having to disclose that the project is about dementia (and that they are living with dementia), the researchers will give the participant a study brochure that will be used to ask the person for consent and will also minimize the participant having to explain what the study is about. The researchers will not use any photovoice data in the study where there is no reliable record of consent.
An ethics protocol has been reviewed and approved by the University Research Ethics Board at the home institution (St. Francis Xavier University). Review by the provincial health authority research ethics board, and the institutional and organizational review approvals of co-investigators and project partners, are in progress.
Analysis
Data collected will be recorded and transcribed for analysis using NVivo software. The study will use thematic analysis whereby study personnel examine the data for patterns using open and concept-driven coding (Braun & Clarke, 2006). The concepts used to analyze the data will include person-and-family centered care, health equity, gender, and intersectionality. Themes we will analyze will correspond to the Quintuple Aim framework. Given the phased approach to the overall evaluation, open coding will involve attending to themes arising from the logic model (outputs and outcomes of the SCP) to examine outcomes for recipients and home care providers, as described in interviews and focus groups. The analysis will be iterative; themes arising from research activities in the early stages of the study will inform subsequent phases of data collection and analysis. For example, new knowledge and insights about equity-related barriers to accessing the program generated in the stakeholder consultations will be used to refine research questions on equity that will be posed in interviews and focus groups.
Rigor
Overall, the study relies on a robust sample that aims to gather information from a diverse set of stakeholders to highlight the heterogeneity of perspectives in dementia care. The systematic marginalization and exclusion of the perspectives of people with complex and/or advanced dementia in dementia care services research and quality improvement initiatives reflect a structural inequity. This study will use the visual methods of photo voice and photo elicitation to support PLWD engagement. Home care providers and home care workers will also be included in the participant sample. The study team involves a multi-disciplinary group of emerging and established academic and health system researchers with advanced expertise in qualitative methods, health equity research and health services and policy evaluation. The team will compile field notes on data collection activities and hold regular team debriefing to record emerging findings which will help confirm research results. Detailed records on data collection and analysis practices will enhance the dependability of the study. The multi-phased and varied engagement with program recipients, service providers, advocates and administrations is a triangulation strategy that supports confirmability of study findings.
Conclusion
While there is a strong desire by many older people with dementia to remain at home, there remains limited understanding in research and policy about how to appropriately support equitable, sustainable and population health-promoting person-and-family centered dementia care in community. In evaluating Nova Scotia's model of direct payments for dementia care, the study will contribute to emerging research on the direct payments model in dementia care (Fitzgerald Murphy & Kelly, 2019; Kelly, Hande, et al., 2021; Kelly, Jamal, et al., 2021) by engaging those most closely impacted by and familiar with the SCP, notably the recipients of direct payments, caregivers and home care providers, as well as those who provide information and administer the program. The study will contribute to research on dementia care, intersectionality and gender (Bartlett et al., 2018; Hulko, 2004), linking findings to health equity and implementation science research to advance knowledge about health systems and health care improvement.
Footnotes
Acknowledgements
The authors gratefully acknowledge Trudy Flynn, Bernadette Lake, Glenda Keenan and Kim Silver for providing input on early versions of the study protocol from patient/caregiver, care provider and health system perspectives.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the financial support Canadian Institutes of Health Research (CIHR) Institute of Health Services and Policy Research Catalyst Grant: Quadruple Aim and Equity. Research personnel, space and equipment was accessed through the Spatializing Care Lab at St. Francis Xavier University with support from the Canadian Foundation for Innovation and Canada Research Chairs Program research stipend.