
Abstract
COVID-19 restrictions necessitated innovative online adaptations to conventional qualitative methods; however, virtual interviews do not permit capturing visual data from participants’ environments. Traditional mobile interviews conducted in situ provide contextual, relational, and situational knowledge. Virtual adaptations of mobile interviews have been theorized but not fully tested. This paper compares experiences with an online interview and a virtual adaptation of a mobile interview, the Participant-Directed Mobile Interview (PDMI), during a pilot study examining the design elements of private dental office waiting rooms as symbolic presentations of a dentist’s and dental clinic’s identity. Participants (n = 4), who worked in private dental clinics and had participated in the planning and designing the waiting room, were selected using a purposive and convenience sample design. Participants were required to have access to a mobile device, the internet, and the Zoom cloud-based video conferencing platform. A semi-structured interview preceded PDMI, and both were recorded on Zoom. Unlike the online semi-structured interview, PDMI revealed the participant’s relationship to the space, produced more nuanced and contextual data and clarified the meaning of subjective statements and terms. Mobile devices used by the participant (iPad/mobile phone) provided the researcher with a view of the space and access to visual and relational data that would not be possible if the camera focused on the participants alone. Participants could freely explore, interact with, and reflect on the space in real-time, enhancing the depth and breadth of responses. PDMI was limited by participants’ access to and choice of equipment and internet services and their technical skill level. This technique could be applied to circumstances beyond the COVID-19 pandemic. PDMI could increase access, reduce research costs in distant or remote communities, and provide valuable insights within various methodologies and disciplines.
Keywords
Introduction
During the COVID-19 pandemic, qualitative methods were largely restricted or eliminated due to public health restrictions, generally limiting ethnographic field studies (Teti et al., 2020). Social distancing requirements diminished researchers’ ability to interact with participants, experience locations and mobilize local and contextual knowledge. The ethics and practicality of conducting in-situ face-to-face interviews under these conditions are questionable (Shareck et al., 2021). As a result, interest in methods for conducting qualitative research at a distance increased. Many researchers began considering ways of adapting traditional qualitative methods to an online or virtual environment (Newman et al., 2021).
Qualitative methods adapted to online environments included focus groups, photovoice, and virtual group interviews (Dodds & Hess, 2020). These methods fail to provide contextual and environmental data. Literature on online adaptations for in-situ methods is limited. Therefore, innovative and adapted methods were required to collect contextual data from the participant’s environment.
Related Works
Walking interviews are a mobile data collection method used successfully in qualitative studies to capture environmental context and meaning (Flick et al., 2019; Kinney, 2017). Variations of walking interview methods exist (Kinney, 2017), but each involves the researcher being in-situ, walking with, observing, and interviewing the participant in a selected location. This method allows the researcher to participate in the participants’ lived experiences, daily interactions, and the environment providing valuable contextual data beyond what a face-to-face interview in a remote office may provide (Flick et al., 2019; Kinney, 2017; Shareck et al., 2021). Walking interviews reduce power imbalances between the participant and researcher because the participant takes the lead in driving the topic, conversation, location, and walking route (Kinney, 2017). Further, the method changes the character of the interview into a more open-ended, spontaneous dialogue (Kinney, 2017) and facilitates the mobilization of intersubjective, contextual ways of knowing (Brown & Durrheim, 2009). The environment and the objects encountered within it can elicit memories, stories and experiences that may not be available to participants sitting in an interview separate from their environment (Kinney, 2017). Further, the walking interview can be considered a triangulation of methods between field observation and interviews (Flick et al., 2019).
Of interest to this study, Shareck et al. (2021) theorize several adaptations to walking interviews, one being a virtual walkaround of a place of interest. The walking interview occurs, synchronously or asynchronously, in the participant’s chosen location and path. Using a headcam, the participant provides the researcher with a view of the environment and objects. This method preserves the participant-led, real-time, contextual nature of a traditional, in-situ walking interview. Further, this method may provide a partial sensory and contextual understanding of the participant’s environment and interactions. These benefits would allow one to explore material culture in a remote location, such as a dental clinic waiting room that largely had restricted access at the time and how objects in the space hold meaning for participants.
Using mobile phone footage as a data collection method is not new. In urban ethnography, researchers have used a similar method to map experiences of the New York cityscape during the COVID-19 pandemic (Yavo-Ayalon et al., 2022). However, the application of the walkie-talkie method described by Yavo-Ayalon et al. (2022) has yet to be tested as a data collection method for critical ethnography to examine material culture in smaller settings.
Material culture refers to the everyday objects and artifacts in an environment (Buse et al., 2018). These objects symbolically hold personal, cultural and social meaning (Buse et al., 2018). Further, these objects are repositories of individual and shared cultural stories, memories and histories (Hurdley, 2006). The placement of objects in waiting rooms can evoke an atmosphere or mood, influence the movement and agency of individuals, and reinforce inequitable power relations and hierarchical tensions (Bell, 2018). Much of the literature on material culture focuses on private residences (Hurdley, 2006) and public healthcare facilities, hospitals, and medical clinics (Bell, 2018; Belle, 2017; Street, 2012). Privately run dental clinic waiting room designs may be more influenced by the personal identity of the dentist/owner and a need to appeal to a critical consumer. In a competitive market, dental offices compete for new customers and design a welcoming, comfortable atmosphere to maintain the loyalty of existing clientele.
Displays of material culture can also be representations of self. These displays involve a performance that negotiates between the public and private self, social norms and expectations, and an individual’s unique qualities (Goffman, 1959). This impression management is enacted symbolically through clothing alterations and the work environment’s material culture (Goffman, 1959; Parker & Warren, 2017). The symbolic nature of the material objects simultaneously reflects social expectations, resists undesirable stereotypes, and distinguishes the individual from others in the profession (Parker & Warren, 2017).
Dentists must negotiate multiple perceptions about themselves and their profession that are both public and private. Professional regulatory bodies, education, and ethical and moral obligations may inform a dentist’s perception of self. Further, dentists must negotiate broader social discourses about dentists and the negative perceptions of dental treatment (Nettleton, 1989). Impression management may be a marketing strategy in a competitive market where dentistry is increasingly commercialized (Moeller & Quinoñez, 2020). How dentists and dental clinics manage patient impressions and social discourses about dentists and their services through material objects in their waiting rooms has not been explored.
Entering the waiting room, patients get a first impression of the dentist and an indication of the dentist’s professionalism, level of care, and cost of care (Unthank & True, 1999). Patients interpret the symbolic meaning of the waiting room’s aesthetics and decor. Diversity amongst waiting room designs in private dental clinics suggests that the choices of material elements and design aesthetics have purpose and meanings unique to each dentist and dental clinic. Interior design in dental clinics is also articulated with stress reduction, safety, and competitive marketing (Panda et al., 2015; Unthank & True, 1999). In an entrepreneurial environment, the patient is positioned as a critical consumer shopping for the dentist and dental clinic that best match their preferences and needs (Moeller & Quinoñez, 2020).
Methods
This pilot study received institutional ethics approval (#PRO 00094014).
This pilot study used a synchronous virtual mobile technique for a virtual walkaround theorized by Shareck et al. (2021) and demonstrated by Yavo-Ayalon et al. (2022). The study aims to explore the material culture displayed in the dental office waiting rooms as symbolic representations of the dentist and the dental clinic as a means of impression management.
This paper focuses on the researcher’s experiences using a semi-structured online interview and a virtual walking interview called the Participant Directed Mobile Interview (PDMI). The aim is to provide a comparison of the methods and a foundation for further uses of this innovative method for conducting qualitative research at a distance.
Critical ethnographic theory and methodology informed the pilot study (Creswell & Poth, 2016). An ethnographic methodology has been used to explore professional identities and the presentation of self among other professions (Belle, 2017; Parker & Warren, 2017). Ethnographers are interested in the meaning of behaviours, language, interactions, and artifacts and must immerse themselves in a participant’s environment and experiences. Interview and observation methods give voice to the emic perspective (Creswell & Poth, 2016). The in-situ nature of ethnography provides context to what participants are saying and a more nuanced, first-hand understanding of what is occurring (Creswell & Poth, 2016).
Critical ethnography acknowledges the inherent bias of the lead researcher. The researcher’s situatedness and subjectivity impact their perceptions and interpretations of data. In this case, the researcher’s previous experiences in the dental offices studied and established relationships with participants limited the researcher’s objectivity. Further, critical approaches aim to reveal everyday objects' symbolic and often implicit meanings and the social discourses underpinning these understandings.
Sampling and Recruitment
Purposive and convenience sampling guided participant selection. Initial inclusion criteria were dentists who were clinic owners and had actively participated in the design and decorating decisions for the dental clinic’s waiting room. Given the pilot nature of this study, we aimed to conduct three (3) to five (5) interviews. The lead researcher phoned seven dental clinics of dentists and clinics known to the researcher and invited the dentist/owner to participate. Due to time and scheduling limitations of some of the dentist owners, the researcher expanded inclusion criteria to clinic staff members who were actively involved in the design and decorating decisions for the dental clinic’s waiting room.
The researcher advised participants that due to COVID-19 restrictions on face-to-face interactions, the interview would be conducted and recorded using Zoom, an online platform. Information and consent forms were sent by email to each participant. After signed consent forms were returned to the researcher, participants were contacted by phone to schedule a time for the Zoom meeting. An invitation and link to their scheduled Zoom meeting were sent by email.
Data collection
Before the scheduled Zoom meeting, the researcher asked participants to ensure they had access to Zoom and either a portable cell phone, iPad or laptop because part of the interview would involve the participant providing a virtual tour of the waiting room. The researcher also informed participants that their mobile device camera would need to be able to provide the researcher with a view of the setting.
The participant’s physical location during the online meeting, the dental office waiting room, was predetermined by the researcher to capture visual data of material objects in respective waiting rooms.
Interview sessions
Interview sessions for this study consisted of two (2) data collection methods: a virtual semi-structured interview and a Participant Directed Mobile Interview (PDMI). Respectively, these methods served as a proxy for in-person interviews and field observation because COVID-19 restrictions prevented in-situ or face-to-face methods at the time of the study.
Semi-Structured Interview
Semi-structured interviews using an interview guide were designed to elicit the participant’s perspectives about, and descriptions of, the dental clinic, the dentist, the clinic’s/dentist’s reputation, and the clinic’s patient population. Participants were asked to indicate other individuals who had input in design choices, as the presence of other perspectives may have impacted design choices. The researcher inquired about factors considered in the design and decoration of the waiting room, such as professional or building code requirements, who would use the room and how it would be used. Also, participants were asked to discuss materials they felt were essential to the space and identify objects they did not include in the room and reasons why. Each participant was asked what made their waiting room unique or special.
Participant-Directed Mobile Interview
At the end of the semi-structured interview, participants were instructed to perform the video tour of the room-PDMI. PDMI is an online adaptation of a traditional mobile or walking interview (Brown & Durrheim, 2009). This method was intended to provide visual data about the waiting room and participants' relationship to the space as the participant walked and talked. The method enabled the researcher to analyze the visual data from a participant-observer standpoint (Brown & Durrheim, 2009).
Participants were asked to change the camera direction on their mobile devices to face the room to provide the researcher with a view of the environment. The researcher left the tour’s starting point and the path to the participant. Then, the researcher asked the participant to conduct a step-by-step tour of the clinic’s waiting room and reflect on choices of decorations, objects, furniture, colours, materials, aesthetics, and their purpose and meaning. Participants were encouraged to talk about areas and objects in the room as they encountered them, to be as detailed as possible and to share any stories or feelings surrounding them.
Following each interview, the researcher manually transcribed dialogue from the interview and walkaround verbatim into a Word document.
Analysis
Participant statements and visual data underwent critical discourse analysis. As the literature suggests, dental professionals draw on social and professional discourses (Nettleton, 1989). The assumption that these discourses are often implicit in participant responses requires attention to latent and manifest data (Feighery, 2011). This analytical method is subjective, interpretive, and iterative and relies on contextual knowledge (Feighery, 2011). Analysis was informed by and interpreted through the researcher’s experience in dental offices as a registered dental hygienist.
Transcripts of interviews and visual data from PDMIs underwent multiple levels of analysis. Initial open coding of manifest data provided descriptive codes of the dentist/dental clinic and design features. Latent data regarding the dentist’s/clinic’s presented self was drawn from participant statements and the researcher’s interpretation of statements. Open coding revealed three (3) broader themes: 1) mood/atmosphere, 2) identities, and 3) activities. A coding matrix for each theme facilitated the organization of codes and categories (Gibbs, 2007). Data and themes drawn from each transcript were compared internally and externally to those from the other two interviews.
Findings
Participants (n = 4) represented three dental offices. Two participants were dentists/owners, and two were dental office managers. One interview involved the dentist and the office manager at the dental clinic. Three participants were female, and one was male. The locations of the dental offices varied: one was in a downtown business district, and two were in suburban areas. The choice of participant mobile device used during the session varied. Two sessions saw participants use a mobile phone while the other chose an iPad. Each recorded session combined the semi-structured interview with the PDMI and lasted approximately 45 minutes. The length of time for each segment of the interview was similar.
What follows are findings from the pilot study based on the aims and objectives of that study. The author has separated data collected during semi-structured interviews from PDMI data to highlight the differences in the data captured from each method.
Findings from online semi-structured interviews
Discussions included the number of dentists and staff providing care in the clinic, the number of operatories, the type of services provided, and the clinic’s location. Participants' descriptions of their clinics were often limited to quantifiable terms. For example, two participants described themselves as “solo” practitioners while a third described their clinic as “a large, multi-dentist…6 dentists…12 operatory…” The latter explained that this was a “family practice” providing “general dentistry.”
Similarly, the patient population for the clinic was described demographically. Participants referred to their patients as being of “all ages,” “from first visits to seniors,” or “multigenerational family members.” One participant explained that their office typically saw “predominantly…… blue-collar workers” and identified jobs such as “service workers……government…workers…[and] self-employed.” Participants described the neighbourhood or catchment area of the patient population, such as “the university or downtown business area.” Patient populations were also defined by whether or not they had access to insurance. Interestingly, one participant reported that some of their patient population “valued dentistry enough to pay out of pocket” despite not having insurance, introducing a qualitative description.
Participants’ discussions about the waiting room were often pragmatic, focussing on the design process and the functionality of the space, such as choosing a designer or contractor, building codes, wheelchair accessibility and the flow of bodies through the space. However, participants provided subjective descriptions of the design of the waiting room, the dentist and the patient population. One participant described the feel of their waiting room as “fresh, bright, lots of light, clean.” Additionally, participants chose to explain their waiting rooms using similes, metaphors or comparisons to other clinics or healthcare spaces. Two participants described their offices metaphorically as “home,” and one interviewee described their patients as “family.” Other terms used to describe the desired “feel” of the room were “zen,” “calm,” and “fun.” Participants also drew on their experiences in other dental clinics and healthcare.
Settings to explain what they tried to avoid. For example, one participant found the idea of a “spa” distasteful, while another wanted to avoid “marketing.” Many of the participants listed crowded seating as undesirable. One participant associated crowded waiting rooms with industrial farming and production lines, stating, “People are people, not cattle.” Participants did not expand on subjective terms or comparisons, leaving them up to interpretation.
Of interest to this study, only one participant statement points to a relationship between the material culture of the waiting room and impression management.
“...the first impression, so the waiting room, front entry, couldn’t be opulent in any way. It had to …..feel like it’s comfortable, you’ve made me a really nice…you’ve made an office that reflects who you are, it’s friendly, it’s casual enough, it’s still beautiful, but it’s not too precious, or too…breakable, or the elements are too expensive and …just too extravagant. We really had to walk the line of…we wanted it to be nice but we didn’t want it to come across as …that it was just dripping with …you know, we’ve overspent……we didn’t want people to walk in the door and say “Wow! Am I paying for this.” (Interviewee A)
Findings from PDMI
The starting point and path of the PDMI varied according to the participant’s role in the dental office (Figure 1). Office managers always began the video tour at the dental office’s entrance. The office managers mimicked the patient’s path upon entering the building. The tour proceeded from the entrance to the seating area and the front desk. Dentists, however, took on a provider’s perspective of the space and always began the tour standing at the entrance to the treatment area. Their tour would proceed to the seating area and the front desk. Sketches of Waiting Rooms Indicating Participant Positions, the Path of PDMI, and Locations of Material Objects Encountered During the Video Tour.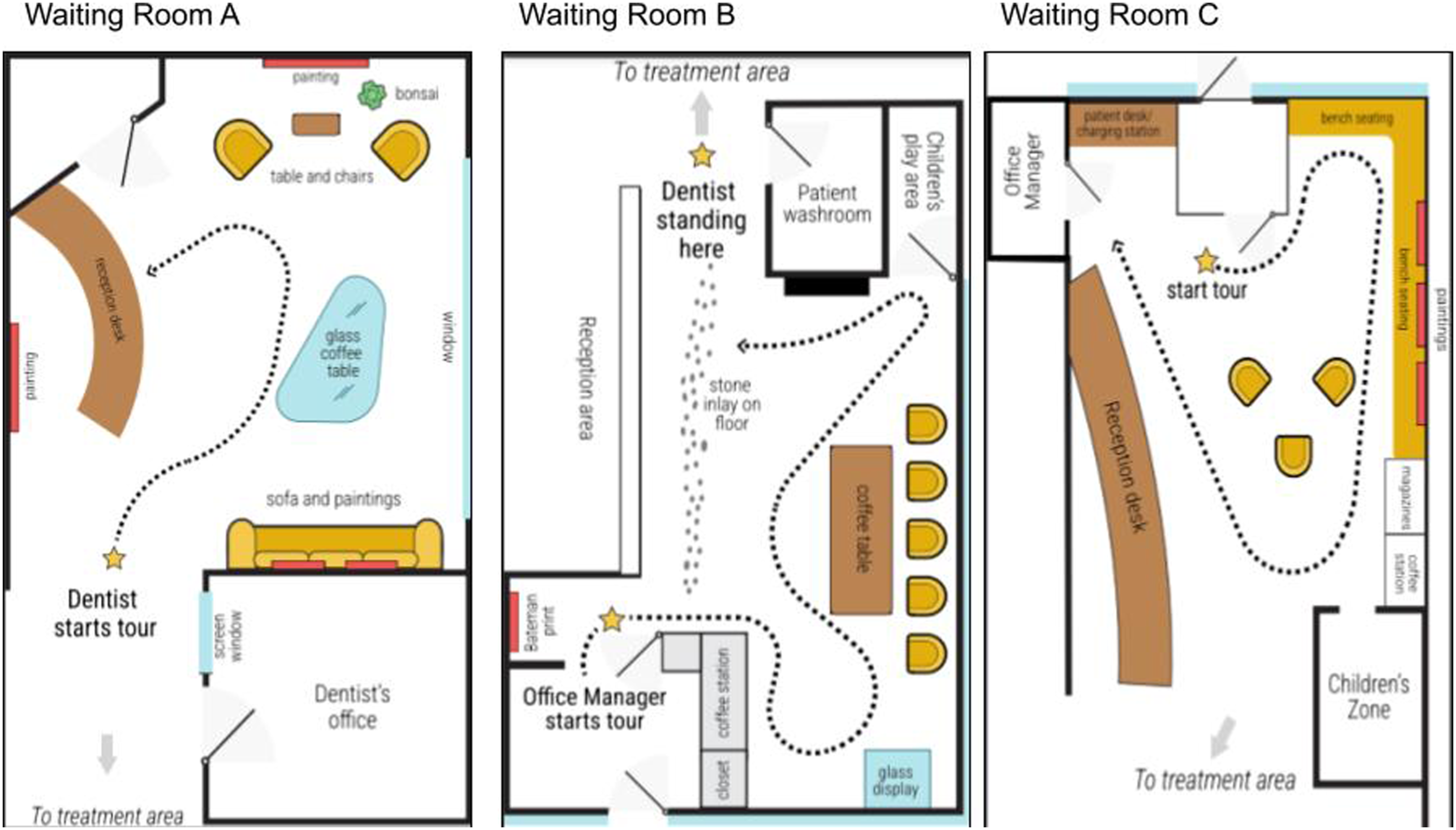
Participants discussed the room’s appearance before COVID-19 restrictions when entering the waiting room. Often they discussed how chairs and objects had been removed from the space to facilitate social distancing, decrease touchpoints in the room and ensure surfaces could be disinfected. Of interest to this study, one dentist began discussing how, before COVID-19 restrictions, some material objects that reflected their personal aesthetic needed to be reconsidered because of patients’ needs.
“when we had our old chairs.. um.. we had a very low profile sectional here and I would never go back to that again. Because I forget, that patients that are elderly, or patients that are older or need assistance with their.. with their.. you know.. with getting up or sitting down..” Interview B
Encountering material objects in the room during PDMI prompted participants to recall and share stories about their personal histories. Unlike family photographs, these material objects hint at the dentist’s self but limit how much personal information is revealed in the space (Figure 2). A dentist recalled a childhood memory of life in northern Canada while discussing a print portraying a wolf in the shadows of a poplar forest. Another dentist pointed to material objects such as a bonsai tree, teak accents and Asian-inspired decor representing the dentist’s family, culture and childhood home. Material Objects Hint at the Dentist’s Identity.
Participants also related stories about the artist, the scene portrayed, and the local art gallery where they purchased an art piece. One participant referred to the use of “relatable art” (Figure 3). Two participants noted that the artwork featured local landscapes and landmarks familiar to the dentist and the patients. The participants pointed to scenes from a local park and a topographic city map as examples. Another dentist took the time to relate a story about the craftsman that laid the decorative stonework on the waiting room floor. Material objects prompted these discussions, and the findings suggest that dental clinics use design elements to suggest a commonality with the patients, such as shared experiences, community membership or support for local businesses and products. “Relatable Art”.
Material objects and design features in the room prompted further explanations of how the physical features reflected the mood or atmosphere the offices were attempting to create. PDMI allowed one participant to demonstrate how the use of “bright green fabric” and “clean white and grey walls” was chosen to create a “fun, fresh” feel in the room. The visual data also clarified the emic perspective of the participant. Although two participants used “home” as a metaphor for the mood of the room they had created, the PDMI revealed that this term was used very differently (Figure 4). One waiting room included a coffee center, padded chairs, a fireplace and a television, while the other opted for a comfortable sofa; club chairs sat next to a large picture window. The latter participant explained that the office was their “second home” and wanted to include objects they enjoyed. The former participant went on to describe the patients as “family” and had attempted to create a more literal interpretation of a living room in a home. Interpretations of “Home”.
Methodological Takeaways
Many advantages of using PDMI in this pilot study align with those discovered in the literature for other online adaptations of qualitative methods, notably the ease of use and setup for the researcher and participants (Dodds & Hess, 2020). However, this pilot study provided a unique opportunity to compare an online interview method with a virtual walkaround method. Unlike the online semi-structured interview, PDMI revealed the participant’s relationship to the space, produced more nuanced and contextual data, and clarified the meaning of subjective statements and terms.
As in Yavo-Ayalon et al. (2022), the rear-facing camera on the participant’s mobile device allowed the researcher to see objects within the space the participant was describing and relating. The view of the space gave the researcher access to visual and relational data that would not be possible if the camera had focused on the participants alone. Additionally, the researcher felt more engaged with the conversation and the environment during PDMI. The virtual engagement with the environment dealt with some challenges in gathering field data noted by other researchers (Dodds & Hess, 2020; Shareck et al., 2021).
The conversation between the researcher and participant during PDMI was more casual and flowed easier than during the semi-structured interview. The unstructured nature of PDMI resembled real-life interactions rather than a formal interview. During PDMI, participants explored, interacted with and reflected on their environment and objects in real-time, facilitating meaningful dialogue and reflection. Objects in the waiting room elicited memories, stories about patients and the community, comparisons to other environments, and reflections on the room’s past, present and future. Discussions about material objects in the room added contextual understanding and emic perspectives to the subjective data collected during the online interview.
A shift in power and control was evident when comparing the transcripts of semi-structured online interviews and the PDMI. During PDMI, participants had the freedom and power to orchestrate the tour and discussion. The reversal of control and power reduced research bias and power imbalances and elevated the participants’ situated and contextual knowledge. This finding aligns with previous research utilizing traditional walking interviews (Brown & Durrheim, 2009). The researcher and the interview guide steered the questioning and conversation during the semi-structured interview. The conversation was more of a dialogue. Alternatively, during PDMI, the participant determined the tour’s starting point and what to discuss. The exchange became more casual and conversational. Simple probing questions arose in response to what the participant was doing and discussing rather than following a formal guide.
Unique to this study, PDMI also provided insight into how participants situated themselves in the environment not previously reported in the literature reviewed. The contrast between how dentists and office managers positioned themselves when viewing the room was fascinating. Participants’ positioning and pathway choice reflected their day-to-day reality and roles in the dental clinic and implied their relationship with the patients. It is interesting to consider how the mobile interview process reflected Goffman's (1959) understanding of identity as a performance. All the participants in the interview were actively presenting themselves in specific ways to maintain the social situation and our established identities and relationships. It is important to note that participants did not discuss their roles in the office during PDMI but bodily assumed these positions. The online interview did not reveal this finding.
Limitations of PDMI were encountered. The camera lens and the participant’s focus limited the researcher’s view of the environment. Even with the camera turned towards the environment, the researcher’s view is limited by the camera lens and the participant’s control. Therefore, the camera lens could only provide a partial experience of the space. It is possible that the participant consciously or unconsciously excluded environmental data. This problem could have been avoided by asking the participant to turn the camera toward areas the researcher wanted to see (Yavo-Ayalon et al., 2022). The researcher could have asked the participant to provide a pan of the room before initiating PDMI. Alternatively, the participant’s control of the camera and the shared view of the environment were beneficial as they elevated the participant’s perspective and filtered out visual data external to the participant’s focus. Future research using PDMI should consider having the participant start the video by panning the entire room or space before beginning. This comprehensive view of the environment could provide additional insights not found in this pilot study.
Issues with participants’ access to and choice of equipment occurred. One participant’s iPad was not as amenable to the video tour as the mobile phones were. Mobile phones had front and rear-facing cameras, which allowed the researcher and participant to view the environment and each other simultaneously. Participants using mobile phones found it easy to reverse the camera without turning the screen away from themselves. The participant using the iPad discovered that the device did not have a way of reversing the camera direction. They needed to turn the iPad screen away from them to show the researcher areas of the room and required directions on aiming the camera to put the object or place discussed in the camera frame. This technical issue resulted in delays and increased participant anxiety. To avoid participant discomfort, the researcher occasionally asked the participant if they preferred to move on to another area which may have resulted in missed data and skewed the pilot study results.
The variety of mobile devices used among participants may have resulted in a lack of uniform data collection during PDMI. Also, this study would have benefitted from ensuring that all mobile devices have a camera lens that reverses to view the environment but allows the participant to view what the interviewer is observing. Had it been known that iPads did not have a rear-facing camera, an iPad would not have been an option. Yavo-Ayalon et al., 2022, also reported issues with mobile devices. This pilot study may have benefitted from having more consistent equipment used across interviews. However, PDMI worked best when participants used a mobile device they were familiar with and one that allowed them to view their screen and the face of the researcher.
In contrast to the researcher-led semi-structured interview, some participants were uncomfortable taking the lead during PDMI. However, participants quickly overcame discomfort as they progressed through the mobile interview. Most participants found the online interview process comfortable. Participants could join the interview from the comfort of their own offices. Unlike previous studies (Dodds & Hess, 2020; Rania et al., 2021), participants reported that using the Zoom online platform for the first time caused anxiety. Participants unfamiliar with the Zoom online platform or mobile device also needed assistance during the tour. At the time of the pilot study, the use of Zoom video conferencing was becoming more common in educational spaces but not in clinical domains. Studies have reported that familiarizing the participants with technology and reminding them of tasks they must perform before the session begins is helpful (Yavo-Ayalon et al., 2022). Future studies using PDMI should pre-interview instructions on using the Zoom online platform, outlining the process of the online semi-structured interview and PDMI, and the use of the rear-facing camera on their devices. Finally, the researcher acknowledges that the findings in this article drew from a pilot study with a small sample. Further testing of PDMI among larger samples and settings is required.
PDMI shows promise for uses for qualitative research beyond the COVID-19 pandemic. As this pilot study demonstrates, PDMI was effective at researching from a distance and could be helpful for researchers with limited access to remote or distant communities or settings. This data collection was free of additional expenditure or effort. This method would allow researchers to expand the sample frame and size without incurring additional costs. PDMI could also allow researchers to conduct multiple case studies in several locations without travelling. Other methodologies could benefit from PDMI as well. Most notably, PDMI could be an effective tool for community-engaged participatory research.
Conclusion
PDMI is an online data collection tool that is an effective proxy for in-situ field study. Compared to online interview methods, PDMI demonstrated several advantages. Participants were free to move about and relate to objects in the room. PDMI allowed participants to orchestrate the discussion and movement path through the space, effectively reducing power imbalances inherent in the researcher/participant relationship. Viewing the environment provided contextual and local data that would have been unavailable in a face-to-face interview alone. Today, mobile devices are commonplace, so researchers using this tool are unlikely to encounter populations that need access to them. However, modern technology is in a perpetual state of evolution, and the equipment available for online methods such as PDMI may improve.
Additional testing of mobile interviewing techniques, specifically the PDMI designed for this study, would be of value.
Footnotes
Author’s Note
The authors would like to express their appreciation to Patrick von Hauff, academic technology specialist, for assisting us with the waiting room sketches. We also thank Dr. Ken Caine, professor of Sociology at the University of Alberta for his mentorship.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The Edmonton District Dental Society and the Oral Health Community Engagement Fund of the University of Alberta School of Dentistry.