
Abstract
Māori and Pacific peoples in Aotearoa New Zealand (NZ) face significant inequities in cardiovascular disease (CVD) risk factors, hospitalisations and management rates, compared with non-Māori, non-Pacific peoples. These inequities are intimately linked to factors such as colonisation and the intergenerational impacts of systemic racism. This is the protocol for Manawataki Fatu Fatu for ACCESS (Māori and Pacific hearts in unison for Achieving Cardiovascular Care in Equity StudieS), a mixed-methods programme of research, combining kaupapa Māori and Pacific research methodologies (i.e. incorporating the knowledges, skills and values of Māori and Pacific peoples). In this Māori and Pacific led research programme, we will use qualitative and quantitative methodologies to identify evidence-practice gaps along the healthcare continuum that can be addressed to improve heart health outcomes for Māori and Pacific people in NZ.
The programme is built on three foundation projects: (i) the assessment and management of CVD risk in primary care; (ii) pre-hospital delays in accessing care following an acute cardiac event in the community; and (iii) post-discharge and long-term management of heart failure. There are three phases. Phase 1 aims to systematically document research, completed or underway, about equitable access to evidence-based heart health care. We will establish a national collaboration of equity-focused heart health researchers and providers, and undertake systematic reviews relating to the three foundation projects. In Phase 2, we will undertake qualitative and quantitative research in the three foundational projects, to identify interventions to increase access to heart health care that have most potential to improve Māori and Pacific health outcomes and achieve equity. The quantitative and qualitative studies will be undertaken in parallel and will inform each other. Phase 3 will use findings from Phases 1 and 2 to create a Quality-Improvement-Equity Roadmap to inform interventions to improve Māori and Pacific people’s access to evidence-based CVD care.
Keywords
Background
Heart Health Inequities in Aotearoa New Zealand
Ethnic inequities in heart health outcomes are evident globally (Mazimba & Peterson, 2021; Niakouei et al., 2020). In Aotearoa New Zealand (NZ), ethnic inequities are well documented for Māori (who are indigenous to NZ and make up 17% of the population) and Pacific people (who are indigenous to neighbouring Pacific island countries and make up 8% of the NZ population) (Stats NZ, 2019). Compared to Europeans (who make up the majority, 70%, of NZ’s population), Māori and Pacific people have a significantly higher prevalence of cardiovascular disease (CVD) risk factors (Cameron et al., 2012; Grey et al., 2010; Riddell et al., 2007), experience the onset of CVD at younger ages (Pylypchuk et al., 2018), are four times more likely to be hospitalised with heart failure (Riddell, 2005), and are twice as likely to die from coronary heart disease (CHD) (Grey et al., 2018; Ministry of Health, 2015). CHD is the most important cause of avoidable deaths in Māori and Pacific people, contributing up to 1 year of the approximately 6–7 year difference in life expectancy between Māori and Pacific, compared to non-Māori non-Pacific people in NZ (Walsh & Grey, 2019).
The reasons for these inequities are complex, multifactorial and intimately linked with historical events including colonisation and the intergenerational impacts of discriminatory immigration policies and other forms of systemic racism (Kapeli et al., 2020; Reid & Robson, 2000). These events have contributed to inequities in the distribution of the socioeconomic determinants of health (Craig et al., 2014; Pasifika Futures, 2017), which add to institutional biases in healthcare delivery and adversely impact on opportunities to engage in health-promoting activities and to access good quality health care in a timely fashion.
Within the health system, it is our collective responsibility to ensure that all people, but particularly those who experience inequities, are able to access high quality, timely, responsive and culturally safe (Curtis et al., 2019) healthcare services. Such services must also ensure that patients and their whānau (families) are empowered and supported to manage their own health, CVD risk and (where relevant) chronic conditions with confidence (Grady & Gough, 2014). There is a large body of evidence in NZ that Māori and Pacific people disproportionately experience challenges accessing healthcare, including heart health care (Grey et al., 2018; Health Quality & Safety Commission, 2019; 2021).
Inequities in healthcare access are important contributors to evidence-practice gaps that in turn lead to poorer heart health outcomes for Māori and Pacific people (Curtis et al., 2010). Evidence-practice gaps are differences in the care we know people should receive (based on the latest evidence) and what happens in real-life practice. A good example of a significant evidence-practice gap in NZ is in the management of CVD risk. Consistent with international evidence-based guidelines, NZ cardiovascular risk assessment and management guidelines recommend anyone assessed as having an estimated 5-year CVD risk of 15% or more be treated with a statin and blood pressure lowering drug (Ministry of Health, 2018). However, studies show that in NZ only about half of people in this high-risk category are currently receiving evidence-based treatment (Mehta et al., 2021) and that Māori and Pacific people are more likely to miss out (Kerr et al., 2014; Muniandy et al., 2021; Selak et al., 2020).
In addition, Māori and Pacific people are significantly more likely than Europeans to die from CHD before reaching hospital (Grey et al., 2016a), are less likely to call an ambulance when experiencing an acute coronary syndrome (ACS) (Garofalo et al., 2012), and are more likely to experience delays to defibrillation (Kerr et al., 2019). Such delays to care are crucially important; definitive medical treatment for ACS should be started as soon as possible to prevent life-threatening complications, and ideally within 1 hour of symptom onset (Chew et al., 2016; Moser et al., 2006; Norris, 2005).
Research Focused on Heart Health Equity in NZ
Research to date investigating reasons for the increased risk of CHD deaths and greater delays to acute care for Māori and Pacific people is woefully inadequate. Differences by ethnicity in severity of disease, prevalence of comorbidities, ease of access to high quality care, awareness of the significance of cardiac symptoms, responsiveness of health providers and a host of other significant, but unknown factors, are likely to be important, but have eluded rigorous enquiry.
While there is a range of published research and possible explanations for ethnic inequities in access to evidence-based heart health interventions in NZ, research to date has been piecemeal and unsystematic. Qualitative and quantitative researchers have almost always worked independently on these issues, investigating the ‘what’, ‘how’ and ‘why’ of heart health equity separately. An integrated approach, incorporating both qualitative and quantitative methods that interrogate available data and capture the stories of consumers, their whānau and wider community, is required.
In addition, the number of Māori and Pacific researchers provided the opportunities to lead, drive and engage in such initiatives has been very limited. Given the heart health inequities experienced by Māori and Pacific people, there is a critical need for Māori and Pacific led research focussed on heart health equity.
Manawataki Fatu Fatu for ACCESS – An Equity-Focused Programme of Research
Manawataki Fatu Fatu for ACCESS (Māori and Pacific hearts in unison for Achieving Cardiovascular Care in Equity StudieS) is a mixed-methods programme of research co-led by Māori and Pacific (Samoan) researchers, combining kaupapa Māori and Pacific research methodologies (research methodologies incorporating the knowledges, skills and values of Māori and Pacific peoples) (Anae, 2019; Pihama, 2011; Smith, 2012). The programme is hosted by The University of Auckland and funded by the Heart Foundation of New Zealand (the major heart health charity in NZ) and Healthier Lives, one of 11 National Science Challenges (a core part of the NZ Government’s investment in science). Governance of the research occurs through: (1) partnerships between the Indigenous Māori and Pacific led research group and funding organisations; (2) accountability and review processes that align with the Indigenous principles which underpin the research and; (3) protection of knowledge arising from the research through partnership agreements and funding contracts.
In this Māori and Pacific led research programme, we bring qualitative and quantitative researchers at various career stages together to systematically examine the importance, and understand the key determinants, of the range of access barriers to evidence-based heart health care and identify interventions that are likely to reduce these barriers.
Aims
The overarching aim of our research programme is to use linked qualitative and quantitative methodologies to identify important evidence-practice gaps along the healthcare continuum (from primary prevention to acute pre-hospital management and post-hospital secondary prevention) that can be practically and rapidly addressed to improve heart health outcomes for Māori and Pacific people in NZ from Māori and Pacific perspectives.
There are three foundation projects in the programme, which draw on extant research that suggests important access barriers are likely to exist and cause significant inequities for Māori and Pacific patients. These focus on: (i) the assessment and management of CVD risk in primary care; (ii) pre-hospital delays in accessing care following an acute cardiac event in the community; and (iii) post-discharge and long-term management of heart failure. Using systematic research reviews alongside a suite of primary research projects using a mixed methods approach, access barriers to evidence-based care for these conditions will also be investigated.
Explanation and Justification of Method
This research programme is built on kaupapa Māori and Pacific Theory and Research Methodologies (Anae, 2019; Naepi, 2019; Pihama, 2011; Ponton, 2018; Smith, 2012). It is Māori and Pacific led; the two principal investigators are Māori (MH) and Samoan (CG), with extensive experience in kaupapa Māori and Pacific research methodologies and the majority of the research team are of Māori and/or Pacific ethnicities. Māori and Pacific whānau are at the centre of the research, which investigates issues that are considered essential by Māori and Pacific partners and stakeholder groups. The research uses Māori and Pacific practices, refuses ‘victim-blame’ and deficit analyses, avoids essentialising concepts of indigeneity, recognises the heterogeneity and uniqueness of Pacific communities, develops the Māori and Pacific health research workforce and works towards eliminating ethnic inequities (Reid et al., 2017).
Guiding Principles of the Manawataki Fatu Fatu Research Programme.

Research design, including methods, sampling and recruitment
Our research programme has three phases.
Phase One
In the first phase, we will establish a national collaboration of equity-focused heart health researchers and health providers. The timing of this research programme is aligned with the establishment of a national centre of research excellence, also focused on heart health, Pūtahi Manawa | Healthy Hearts for Aotearoa New Zealand, and another research programme many of our researchers are also involved in, the Vascular Equity for Aotearoa New Zealand (VAREANZ) group. We also have strong linkages with the Heart Foundation of NZ, Hato Hone St John (which provides ambulance services to nearly 90% of the people in NZ), the NZ Branch of the Cardiac Society of Australia and NZ (the professional body for cardiologists and those working in cardiology), and the four NZ regional clinical cardiac networks of providers of heart health across community and hospital-based settings.
Our goal in this first phase is to systematically document research, completed or underway, about equitable access to evidence-based heart health care. Phase 1 includes: i) A national hui (gathering) of NZ researchers and health providers with expertise in heart health equity to identify knowledge gaps and areas of focus for access-related research.
This hui, held in July 2021, was designed to make visible the landscape of research and services on heart health equity in NZ; draw out aspirations of ideal Māori and Pacific heart health outcomes; and formulate concrete steps in growing and supporting our rōpu (group) of researchers and health providers.
The hui facilitated the coming together of providers and researchers alike to agree on some key areas of focus, which included supporting Māori and Pacific people in the heart health workforce, establishing an equity-focused discharge planning project, launching a communications platform to improve visibility of relevant research and evaluations, and an undertaking to widely share findings of our research.
ii) Systematic literature reviews relating to the three foundation projects.
These reviews will examine: 1. Gaps in cardiovascular risk assessment and management in primary care for Māori and Pacific people in NZ. 2. What is known about factors related to ethnic and gender differences in time to care for out-of-hospital cardiac events. 3. What is known about all aspects of heart failure for Māori and Pacific people in NZ (scoping review).
Phase Two
In the second phase, we will undertake qualitative and quantitative research in the three foundational projects, with a focus on identifying interventions to increase access to heart health care that have most potential to improve Māori and Pacific health outcomes and achieve equity. The quantitative and qualitative studies will be undertaken in parallel and will inform each other. Both the quantitative and qualitative research will draw on kaupapa Māori and Pacific research methodologies.
The quantitative research arm asks, for each of the areas of CVD risk assessment and management in primary care, pre-hospital care for acute cardiac events, and long-term management of heart failure: a. What is the evidence-practice gap for Māori and Pacific patients? b. How does this gap compare to Europeans? c. How much of this gap is due to access barriers? What are the main causes of access barriers?
The qualitative research arm asks, for each of these areas: what are the experiences of heart health care for Māori and Pacific peoples and what are their ideas for improving care?
Our quantitative analyses will utilise national health datasets (hospitalisation, mortality, pharmaceutical dispensing, laboratory testing and ambulance attendances), and the regional TestSafe dataset of all laboratory tests for Auckland and Northland (Wells et al., 2017). These datasets can be linked at the individual level using encrypted identifiers (see Data Handling Section below for more detail). They will allow us to examine the frequency of blood testing and dispensing of medications for people in primary care, as well as those hospitalised with heart conditions, including heart failure. In addition we will examine access to pre-hospital care for acute cardiac events in the community. These linked health datasets will be complemented and their completeness assessed using Statistics New Zealand’s Integrated Data Infrastructure (IDI), which captures people from multiple other health as well as non-health national datasets such as the NZ Census (Zhao et al., 2018).
While it will quantify the evidence-practice gaps and inequities impacting Māori and Pacific peoples, quantitative research cannot explain why these gaps and inequities exist. Therefore, in-depth comprehensive qualitative studies with cross-cutting themes relevant to the three foundation projects will explore important causes of evidence-practice gaps in heart health care, and possible solutions, through the stories and experiences of Māori and Pacific patients and their whānau, support networks, service providers and policy makers.
The qualitative studies will include in-depth semi-structured interviews with approximately 65 Māori and Pacific patients and/or whānau members who have received care or were eligible to receive heart health care for: CVD risk assessment and management in primary care, paramedic care following an acute cardiac event in the community, long-term medical management of heart failure or other relevant heart conditions. The interviews will be conducted by researchers fluent in the preferred languages of participants including te reo Māori and Pacific languages. The patient/whānau interviews will be complemented by focus groups and key informant interviews with approximately 10 health service providers and healthcare managers in primary, secondary, and paramedic care to understand organisational barriers and influences underlying inequities in access and outcomes. Key informants will comprise health providers, including people who are Māori, Pacific and non-Māori/non-Pacific, people working for Māori/Pacific organisations and people working for non-Māori/non-Pacific organisations. Valuing the contribution of the patient and whānau participants and using this as a learning experience for the providers, the provider interviews will be in two parts. First the participant will be asked to share their experiences of caring for Māori and Pacific patients with CVD and their aspirations in this regard. Then the researcher will present the findings of the patient and whānau interviews and ask the provider to respond.
As experienced clinicians and researchers, and valued community members, the research team has an extensive network of colleagues, professional and personal contacts. We will draw on this network when recruiting for the qualitative studies. Key contacts (including primary care doctors and practice nurses, cardiologists, and cardiac nurses) will connect with potential participants for patient/whānau interviews, provide them with information about the study, and ask them to contact the researchers if they would like to participate or obtain more information. Recruitment of providers will take place through the wider networks of colleagues and professional contacts in primary care, paramedicine, specialists (secondary and primary care) and managers, planners and funders. Participants from throughout NZ will be included, ensuring representation from smaller towns and rural areas. For recruitment of patients, whānau and providers we will use snowballing, whereby participants are asked to encourage their eligible colleagues, friends and whānau to participate. Participants may also self-identify in response to an advertisement.
Phase Three
The third and final phase of our research programme will involve the creation of a Quality-Improvement-Equity Roadmap to inform action plans for interventions to eliminate inequities in Māori and Pacific people’s access to evidence-based CVD care. This Quality-Improvement-Equity Roadmap will be developed by integrating, and where relevant, triangulating, findings from Phases 1 and 2. Current NZ health system reforms, with an increasing focus on equity, mean the timing is right for the Quality-Improvement-Equity Roadmap. In July 2022 a new statutory entity, Te Aka Whai Ora - Māori Health Authority, was established and given responsibility for ensuring the health system is effective for Māori. These changes in the NZ health system indicate desire to change but this research project is ideally placed to inform how the system needs to change to meet its stated equity objectives.
Interventions are likely to be needed at macro- (central agency), meso- (health organisational and community) and micro- (frontline and personal health) systems of care. At these different levels, examples may include health policy changes (e.g. affordability of prescribed medications), workforce development, addressing health literacy needs at systemic levels (including service and organisational barriers) (Grey et al., 2016b), data sharing across health providers, changing service delivery models such as enhanced care co-ordination across health and social services, monitoring and feedback approaches specifically for equity and addressing specific barriers to care such as engaging adequately resourced and appropriately trained health coaches or navigators, cultural support workers, interpreters and the availability of shared medical appointments.
Phase 3 will include interactive participatory co-design workshops involving patients, whānau and providers, facilitated to enable the development and/or refinement of promising interventions that can address the barriers and enablers identified in this research programme. This approach is designed to provide insights regarding the influences and drivers of access barriers and inform a process by which communities are empowered to explicitly inform service delivery that can meet their expectations, needs and aspirations for CVD health and wellbeing.
Opportunities
The findings of this research programme are likely to be applicable to other conditions beyond CVD, and the way this programme is structured has implications for future research projects. Rather than having tokenistic inclusion of Māori and Pacific researchers, or even co-leadership with Pākehā, this programme intentionally moves towards Māori- and Pacific-led research to ensure that research is helping and supporting the aspirations of Māori and Pacific peoples.
Workforce Development
In line with the workforce development aims of Manawataki Fatu Fatu, this research programme has: • intentionally recruited Māori and Pacific emerging and mid-career researchers undertaking focused streams of research activity • provided scholarships and research funding for qualification pathways for Masters, PhD and postdoctoral levels. All postgraduate students identify as Māori or Pacific peoples and receive scholarships funded through the programme • developed a student-led mentoring and coaching program supporting research skills and career development • assisted these researchers in networking across the sector, building connections to clinicians, administrators, government, and non-government organisations • supported upskilling of dissemination experience via presentations at local hui and national and international conferences, and • enabled opportunities for researchers to seek supplementary research funding to extend and advance their research interests beyond the current programme of research.
Data Handling/Analysis
The significance of the Manawataki Fatu Fatu programme comes from the integration of Māori and Pacific research methods and the mixed methods approach. True to Māori and Pacific research methodologies, and following our guiding principles, all data analysis will be decolonising and transformative (Pihama, 2011). Pihama (2011, p. 51) described decolonisation as “how we look at interrupting colonisation; how we question; how we reflect; how we question and challenge some fundamentals that we may hold that may not be ours, that may have derived from a colonial context or from colonial Western understandings and views”. In this context, decolonisation means that we will be alert for the ways that colonisation, migration and racism have affected the patients’ stories and interpretations of their own experiences, and the ways the discipline of Western medicine shapes expectations of provider and patient. Transformative means that our analysis will look to the strengths of Māori and Pacific patients and whānau and will not just create theory but contribute to making positive change.
We will apply the principles of Māori data sovereignty at all times, namely: Rangatiratanga (authority); Whakapapa (relationships); Whanaungatanga (obligations); Kotahitanga (collective benefit); Manaakitanga (reciprocity); and Kaitiakitanga (guardianship) (Te Mana Raraunga, 2018). Quantitative data will be linked using an encrypted national health index number, which allows de-identified linkage of individuals across multiple datasets. The qualitative interviews will yield data in the form of recordings, observations and field notes. The recordings of all interviews will be transcribed by a transcriber who has signed a confidentiality agreement. We will translate interviews conducted in languages other than English, and the final repository of data will all be in English. All data will be securely stored as per data access protocols.
The plan for qualitative data collection and analysis is depicted in Figure 1. In keeping with our guiding principles, data collection and analysis will be carefully timed and managed to ensure that the research is truly whānau-centred and values Māori and Pacific voices. We will begin with interviews with patients and whānau members. Qualitative data analysis will employ template analysis (King, 2012), an analysis technique that “may be used within a range of epistemological positions” (King, 2012, p. 454). As a method, rather than a methodology, it does not have its own epistemology or ontology, so is suitable for use within Māori and Pacific paradigms. In template analysis, researchers develop themes based on a subset of the data and use these to create a template that is then used to code the whole dataset, “through an iterative process of applying, modifying and re-applying the initial template” (King, 2012, p. 458). A small number of a priori themes can be used. Plan for qualitative data collection and analysis.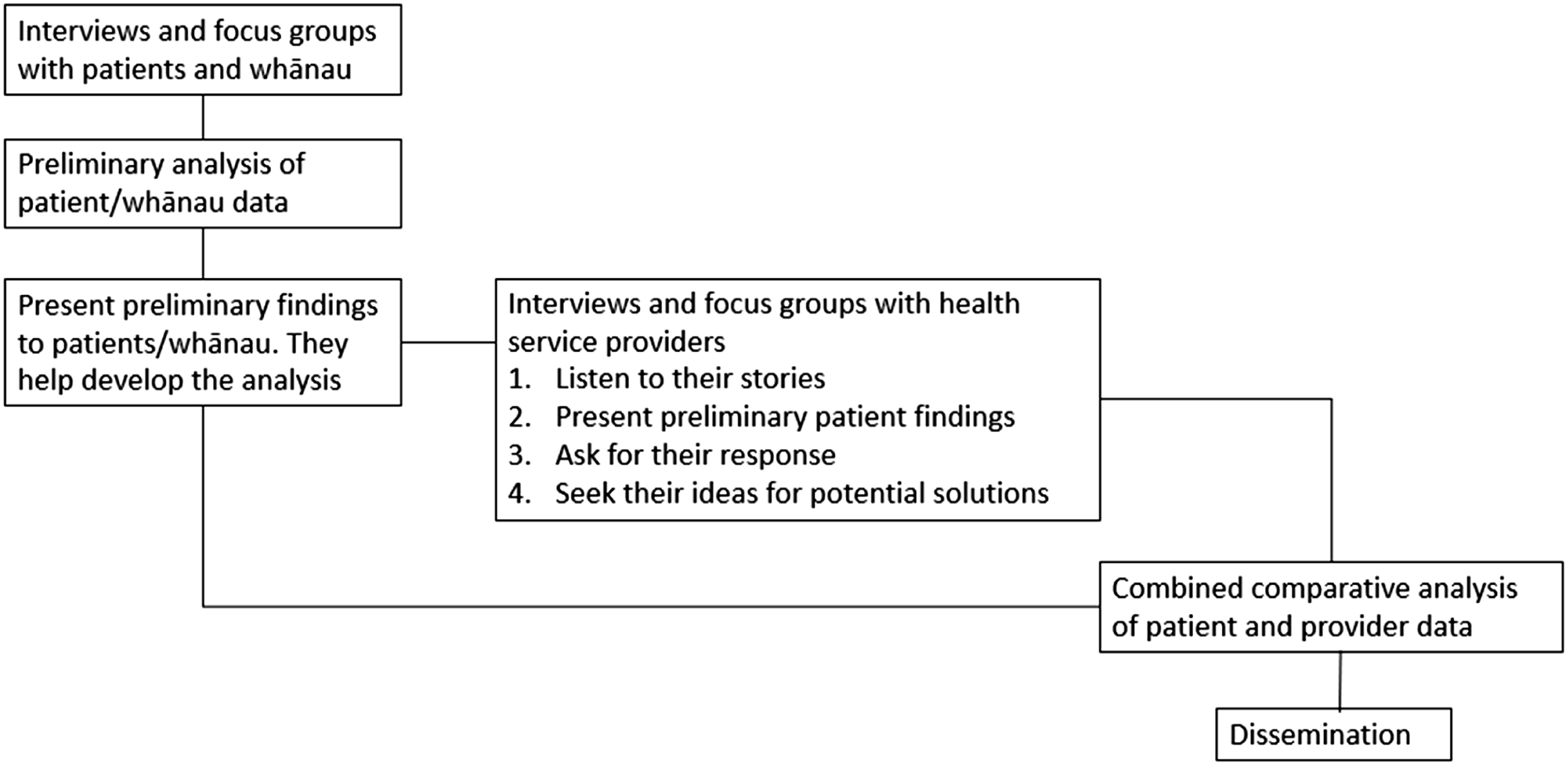
When beginning analysis of the patient and whānau interviews, the research team will work with a subset of interview transcripts to develop a template. This subset will include Māori and Pacific participants, covering the three foundation projects. To ensure both Māori and Pacific stories are properly understood and represented in the analysis, the research team will divide into a Māori group and a Pacific group to undertake the initial coding. This will be followed by a whole-team discussion to develop a preliminary template. Following an iterative process, we will apply the template to transcripts individually, and as a group, until the template is satisfactory. When the template has been developed, we will host hui with patient and whānau participants, in which we present the preliminary findings and seek feedback. This will ensure that the guiding principles of valuing Māori and Pacific knowledge and being whānau-centred are upheld. Following this, two Māori and two Pacific team members will use the template to code all the transcripts, using NVivo software, making small changes to the template as required. We will maintain an audit trail to demonstrate the development of the themes. To ensure consistency between coders, the first two transcripts will be coded as a group, with discussion and agreement on each theme.
After the patient and whānau hui we will begin interviews and focus groups with health care providers. These interviews will include presenting the findings of the patient/whānau interviews and seeking providers’ response to this information. Analysis of provider interviews/focus groups will follow a similar process, using a subset of interview transcripts to develop a new template, which is then applied to the full set of provider interviews/focus groups. Finally, we will undertake a comparative analysis of the combined patient and provider data. This will involve critical comparison of the two final templates (patients/whānau and providers), looking for similarities and differences.
Quantitative analyses will predominately be descriptive and focused on comparing data between ethnic groups. Ethnicity will be self-identified and classified using prioritised and/or total ethnicity output methods, as defined in NZ ethnicity data protocols (Health Information Standards Organisation (HISO), 2017).
Ethics
As is appropriate for kaupapa Māori and Pacific research methodologies, our guiding principles are fundamental to this research and provide the foundational ethical guidance.
The qualitative study has received approval from the Auckland Health Regional Ethics Committee (AHREC), reference AH22609. Informed consent will be sought from all qualitative study participants. Participants may withdraw consent for taking part in this research prior to the interviews and focus groups. Participants may withdraw consent for the collection of data at any time, without providing a reason. Participants will be provided koha (a gift in acknowledgement of the time and commitments they make, including travel costs) for attendance at interviews and focus groups. This will be in the form of a petrol or supermarket voucher to the value of NZ$50 per person up to a maximum of NZ$100 per family.
There are a number of ethical issues to consider for the qualitative study.
Participants will be asked to speak about their experiences of receiving or providing heart health care. This will potentially involve reliving difficult experiences such as a cardiac arrest or a difficult experience with a healthcare provider, colleague or patient. Most of the research team are clinicians with experience in responding to patients or colleagues in difficult situations. All researchers will know when and how to refer a participant for external professional assistance.
Participants might fear that information they provide will impact their employment or any future healthcare they receive. Interviewers will assure participants that all efforts will be made to protect their identity and ensure that no individual or whānau can be identified in the research findings. Participant data will be collected on a confidential basis, and no identifying information relating to study participants will be linked to the presentation of analyses. Source documents will be held securely at the main study site, with identifiable data stored separate to all de-identified data. Interview transcripts and field notes will not include identifying information. De-identified data will carry the participant’s unique study code and pseudonyn assigned in discussion with study participants.
Ethics approval for the quantitative components of the research is covered by a pre-existing approval through the VIEW research programme, which receives annual ethical re-approvals from the Northern Region Ethics Committee Y (original approval in 2003 [AKY/03/12/314]) and the Multi- Region Ethics Committee (original approvals in 2007 [MEC/01/19/EXP] and 2011 [MEC/11/EXP/078]). Because all data are de-identified, individual patient consent is not required for the quantitative analyses.
We also recognise the importance of Indigenous Māori and Pacific data sovereignty, recognising that data (qualitative and quantitative) is a taonga (treasure), has been gifted to us by participants, and therefore requires careful consideration and interpretation that is aligned with indigenous Māori and Pacific cultural values.
No biological tissue will be collected in this research.
Rigour
For Indigenous research the requirements for ethics and rigor go beyond standard research practice. To ensure rigor in our research, and reporting of that research, we will follow the “CONSolIDated critERtia for strengthening the reporting of health research involving Indigenous Peoples” (CONSIDER statement) (Huria et al., 2019). In addition, we will monitor against our guiding principles and our own Indigenous standards.
Dissemination
As is the nature of kaupapa Māori and Pacific research, dissemination of findings to participants is incorporated throughout the programme. Patient and whānau participants in the qualitative study will be invited to a hui to discuss the developing findings, and the results of the patient and whānau interviews will be taken to the interviews and focus groups with health care providers. Interactive participatory co-design workshops, involving patients, whānau and providers, will be held to enable the development and refinement of promising interventions that can address the barriers and enablers identified in this research programme. National hui to be held with NZ researchers and practitioners with expertise in CVD inequities will provide an opportunity for reciprocal exchange of information.
All research studies will be written up and submitted for publication in local and (where appropriate) international peer-reviewed journals. Important findings, particularly in Phase 3, will be communicated with the health sector via presentations at primary care, nursing, public health, cardiology, and Māori and Pacific health conferences and/or workshops, as well as to relevant decision-making bodies.
Students will be encouraged to present their findings at various fora, which will provide valuable opportunities for academic growth. Both principal investigators work at the interface of research and health service delivery and will use opportunities in their non-academic roles to promote important findings and encourage their translation into improvements in health care provision. Many of the named researchers, as well as supportive colleagues at The University of Auckland, are also actively involved in teaching, including within the medical, nursing and pharmacy programme, and key findings will be integrated into health professional teaching curricula where appropriate.
Conclusion
Manawataki Fatu Fatu is a 3-year programme of research focused on achieving equity in heart health care for Māori and Pacific people in NZ. It represents a unique model of research, being both Māori and Pacific led and using Māori and Pacific methodologies and mixed methods. Other important aspects of the research programme include Māori and Pacific student and workforce development, community and stakeholder involvement, and a transformative approach, with the aim of producing a roadmap of practical solutions for equity in heart health.
Full Copies of Interview Schedules/Focus Group Schedules/Fieldwork Plans
Interview Schedules for Qualitative Study
Patient/whānau interviews/focus groups will explore the participants’ experiences accessing care and navigating transitions between primary, community and secondary care; and views and aspirations relating to health care service engagement. Specific questions may include: • Tell me about your/your whānau’s experience of heart health/heart disease/ambulance for chest pain • Tell me about the care that you/your whānau have received, from the first ‘episode’ until now • Views about relationship with professionals/service. Of the services you or your whānau have had contact with regarding your heart health/heart disease/ambulance for chest pain, what made you feel comfortable and/or uncomfortable? • What is important for you when it comes to heart health? • Have you ever been concerned about the access to or quality of a service provided for your/your whānau’s heart health/heart disease/ambulance for chest pain: please describe. • If you were the Prime Minister, what would you do to improve current heart health/heart disease/ambulance for chest pain services?
Health service provider interviews/focus groups will explore the participants’ experiences planning, funding and providing care at primary, community and secondary levels; and views and aspirations for Māori and Pacific CVD care. Specific questions may include:
Part one individual interviews: • Tell us about a particularly memorable experience you have had with a Māori or Pacific patient with CVRA/ACS/HF o Why was it memorable? o What did you learn from the experience? o What do you think others could learn from the experience? • If you were the Prime Minister, what would you do to improve current heart health/heart disease/ambulance for chest pain services?
Part one focus groups: • What are some of the things within our health system that stop it from being able to address equity? • What do you think are some of the barriers are for your patients in accessing timely CVD care? • What is working well and should be scaled up or strengthened? • If you were the Prime Minister, what would you do to improve current heart health/heart disease/ambulance for chest pain services?
Part two (interviews and focus groups):
Having shared your story, we’d now like to share some of the themes from interviews with Māori and Pacific people about their heart care. These are not specific to your service but have been collated from interviews with people from all over Aotearoa. On presenting each theme and the data I’d like you to think again about what stands out for you and why; any learnings; and any ideas on potential solutions?
Appendix
Glossary

Footnotes
Authors’ Contributions
All authors have contributed to drafting and approving the study protocol.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by a grant jointly awarded by The Heart Foundation of New Zealand and Healthier Lives National Science Challenge, grant number 1819.