
Abstract
People living with neurological conditions such as multiple sclerosis, Parkinson’s disease and dementia may experience physical impairment, social disengagement, cognitive issues, and emotional disturbances. While qualitative research utilising in-depth interviews can access lived experience perspectives, the use of photovoice has the potential to obtain rich insights that include images and raise community awareness. The purpose of this scoping review was to document salient themes relating to the lived experience of neurological conditions as reported in photovoice studies. Following established scoping review methods of the Joanna Briggs Institute, a comprehensive search of five electronic databases, including MEDLINE, EMBASE, PSYCHINFO, CINAHL, and SCOPUS was conducted, as well as relevant journals and reference lists of retrieved studies. References were sorted, screened, and evaluated for inclusion using Endnote and Rayyan. The search results and the study inclusion process were reported in full in the final scoping review and presented in a PRISMA-ScR flow diagram. Reflexive thematic analysis was managed through NVivo to identify and synthesise findings, as well as identify themes. Following the removal of duplicates, the search identified 109 articles for title and abstract screening. The final dataset consisted of 25 studies published between 2007 and 2021. Two themes were identified: 1) ‘Losses and benefit finding’ focuses on the lived experience of people with neurological conditions including being pushed aside by society, a progressive decline of self and growing as a result of losses; 2) ‘Challenges of using photovoice in neurological research’ covers the confusion of terminology and implementation complexities and adaption. Societal change is needed for greater inclusion of people living with neurological conditions. Future studies using photovoice need to pay attention to methodological issues and include the recommended final step of the photovoice process to hold gallery exhibits to disseminate findings to raise awareness and initiate social change.
Keywords
Introduction
People living with neurological conditions may be challenged with a wide range of sequelae, including physical impairment, social disengagement, cognitive issues, and emotional disturbances (Evans, 2011). The number of people living with neurological conditions is increasing (Feigin et al., 2019), with neurological conditions being among the leading disease groups in Australians aged 75 plus (13% males, 18% females) in 2018 (Australian Institute of Health and Welfare, 2021). Exploring the lived experience of people with a neurological condition has been undertaken within qualitative studies, including the use of photovoice (Wang & Burris, 1997). Photovoice has been referred to as a method of Participatory Action Research (PAR) methodology and as an innovative, artistic, and creative approach purposively connecting researchers and participants to design projects, gathering and interpreting data, and disseminating findings (Fountain et al., 2021; Seitz & Orsini, 2022).
The ‘photo’ of photovoice is the process that turns the camera lens on the experiences of those living with a neurological condition and provides people with the opportunity to record, reflect, and critique personal and community issues in creative ways (Wang & Burris, 1997). The ‘voice’ aspect of photovoice is understood to mean the articulation of lived experience and experiences of oppression, silencing, agency, and control (Liebenberg, 2018). For example, ‘voice’ is recognised as a means of asserting power through more accurate representations of contextual risks and needs, as well as personal and contextual resources and strengths. It provides an opportunity for people with neurological conditions to share experiences and articulate their everyday life through photographic images. To have a voice also implies power – the power to express opinions (Liebenberg, 2018), the power to participate in decisions (Lorenz, 2010) through sharing stories, and it is also empowering and builds strength and resilience (Dantas & Gower, 2021). Therefore, photovoice is directly aimed at creating social change by shaping and forming policies and guidelines that incorporate the strategies, views, or needs of people living with neurological conditions. Photovoice studies generate a level of richness that could potentially influence existing policies that do not align well with those living with neurological conditions.
The Photovoice Method Involves a Series of Nine Steps (Wang, 1999; Wang & Burris, 1997).

The SHOWeD Method in More Detail (Wang, 1999).

The purpose of this scoping review was to document salient themes relating to the lived experience of neurological conditions as reported in photovoice studies.
Methods
The scoping review research question was explored using the framework ‘ • • •
Eligibility Criteria
Eligibility Criteria for the Scoping Review.

Search Strategy
Search Strategy.

Sources of Evidence Selection
The titles and abstracts were imported into Endnote and then into Rayyan’s Systematic Review Screening Software (Ouzzani et al., 2016). Titles and abstracts were initially reviewed in Endnote by two reviewers (JS, LE) against the eligibility criteria. When uncertain, the article moved to a full-text review. Eligible full texts were imported into Rayyan’s Systematic Review Screening Software (Ouzzani et al., 2016) and reviewed in relation to the inclusion and exclusion criteria by the same two team members. A process was established to account for any uncertainty or disagreements whereby the paper/s would be reviewed by a third team member to determine inclusion (there were no studies that were reviewed by the third team member). Attempts to identify articles from hand searches, including references obtained from the reference lists of the selected articles, were successful (n = 1). The search results and the study inclusion process are reported below and presented in a PRISMA-ScR flow diagram (Tricco et al., 2018) (Figure 1). Flow diagram of the study selection process.
Scoping Review Results
The search identified a total of 225 records. After removing duplicates (n = 117), the remaining 109 records from database searches were screened by title and abstract. The resultant records were assessed for eligibility (n = 26). The final dataset consisted of 25 articles (See Figure 1).
Databases
Each database was searched based on its proprietary search engine interface using Medical Subject Headings (MeSH). The following electronic literature databases were searched without publication date limit - MEDLINE (OVID), EMBASE (OVID), APA PSYCHINFO (OVID), CINAHL (OVID) and Scopus (OVID).
Data Extraction
Data were extracted from included articles utilising a charting table developed and piloted by the two reviewers, adapted from the ‘JBI template source of evidence details, characteristics and results extraction instrument’ (Peters et al., 2020). Data extracted included author(s), year of publication, country of origin, aims, methods, and key findings that relate to the scoping review question (Peters et al., 2020) (See Supplementary material).
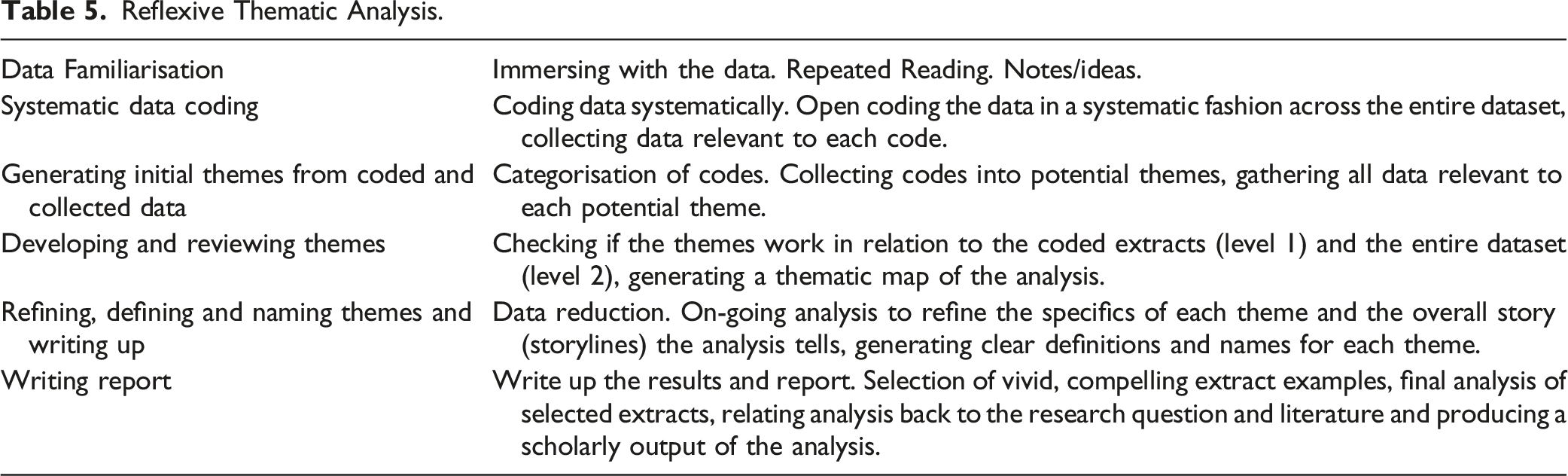
Data Analysis
Reflexive Thematic Analysis.
Positionality
Knowledge generation in reflexive thematic analysis is viewed as inherently subjective and situated, as self-awareness of underlying assumptions is a resource within the analytic process (Braun & Clarke, 2019; Finlay, 2021; Gough & Madill, 2012). The reviewers of this scoping review are from a range of disciplinary backgrounds, including implementation science, critical health psychology, occupational therapy and, importantly, lived experience of stroke. Reviewer reflection focused on the interdisciplinary nature of the team and the resulting diversity in investigator backgrounds and professional training, with each member providing a different perspective on the data analysis within group meetings. Particular attention was paid to discrepant data at several stages of the analysis by proposing alternative explanations or coming to an understanding of existing themes in the context of the literature.
Critical Appraisal of Individual Sources of Evidence
Critical appraisal of individual sources of evidence was not undertaken as it is not a requirement for scoping reviews as per the JBI framework (Peters et al., 2020).
Results
Characteristics of Included Articles
The Extent of Neurological Conditions.

Reflexive Thematic Analysis
Key Themes.

Theme 1: Challenges and Adaption of Photovoice in Neurological Research
This theme explores the confusion of terminology around the use of photovoice as a ‘method’ and ‘methodology.’ It also covers the implementation complexities and adaption, which include a lack of fidelity toward gallery exhibits and using the SHOWeD method (where participants are asked specific questions within focus groups to reflect on the lived experience) and a movement toward the use of adaption (either through the use of camera adaptions or adaption to the SHOWeD questioning route to elicit the lived experience).
Confusion of Terminology
Multiple terms used across the different neurological studies of varying conditions were inconsistently used to describe photovoice, with it being described as either a method (Genoe & Dupuis, 2013; Levin et al., 2007) or methodology (Bishop et al., 2013; Walker et al., 2020). It is also important to note that some authors switch between terms such as methodology and method (Bishop et al., 2013; Walker et al., 2020). Likewise, the term approach has also been used (Pace, 2020). For example, some studies used the term ‘photovoice methodology’, but unlike how ‘photovoice method’ was defined as a method of PAR, the term ‘photovoice methodology’ was not explicitly defined across the majority of studies making it confusing as to what it was actually referring to, leading to confusion between the two terms ‘photovoice method’ and ‘photovoice methodology’. Two studies (Bishop et al., 2013; Walker et al., 2020) did, however, define ‘photovoice methodology’ as a set of procedures, processes, or steps involved in delivering a photovoice study, with the number of steps outlined differing between these two studies (6-9 steps).
Implementation Complexities and Adaption
Implementation complexities were described as the types of implementation challenges existing in photovoice studies across neurological conditions (e.g., cameras and manual dexterity). Implementation complexities often resulted in a lack of faithfulness or fidelity to the original steps outlined in seminal photovoice literature (e.g., missing out on gallery exhibits) (Wang, 1999), and several challenges documented to operating cameras to take photographs. There were also adaptions to specific steps, such as the questioning route (lack of fidelity to the exact questioning route of the SHOWeD method) and adaptions to cameras, which seemed to be common practice across neurological studies to fit the needs of those living with a neurological condition (Levin et al., 2007).
Operation of cameras, such as the need for manual dexterity required to handle a disposable camera, was a difficult task for some of the neurological population (e.g., dementia, post-stroke, and stroke aphasia) (Genoe & Dupuis, 2013, 2014). Beyond implementation challenges due to manual dexterity, small cameras were also challenging with instructions written in small print (Genoe & Dupuis, 2013). When participants with dementia had difficulties operating a camera, their partners took photographs for them, raising the question of whether the photograph represented an independent contribution from a participant (Evans et al., 2016). For some neurological conditions (e.g., post-stroke, aphasia), it was reported that more time was needed to use the camera, delete photographs, and use the features as cameras generally were harder for participants to operate (Levin et al., 2007). Other studies resolved some of these implementation issues in post-stroke participants by tailoring cameras for these participants in their study (Barclay-Goddard et al., 2012). For example, camera adaptions led to one-handed access, larger buttons (Barclay-Goddard et al., 2012), the use of digital cameras with viewfinders (Levin et al., 2007), and the option of using one’s own mobile phone to take photographs (Tornbom et al., 2019).
The SHOWeD method was only implemented within a few studies (Balakrishnan et al., 2017; Brown et al., 2020; Maratos et al., 2016; Walker et al., 2020). Instead, studies adapted questions to suit their study, such as “What do you see in this photo?”, “Can you describe what is in the photo?”, “What is meaningful to you about this photo?”, “What does this photo say about your leisure?”, “What does this photo say about your life now?”, “What does this photo say about how you are?” (Genoe & Dupuis, 2013). Other adaptions present in studies that use the SHOWeD method included adapting the photovoice process from focus groups to one-on-one interviews (Brown et al., 2020) or dyadic interviews where two participants interacted in response to the SHOWeD open-ended questions (Maratos et al., 2016).
Planning a format to share photographs and stories with policymakers or community leaders or disseminate photographs was not always reported or carried out in the studies within a neurological context. For example, only six studies reported the use of exhibits in the mode of gallery-style exhibitions/websites (Balakrishnan et al., 2017; Bishop et al., 2013; Evans et al., 2016; Lorenz, 2010; Pace, 2020; Tornbom et al., 2019). Clarification as to why this important step was omitted could not be found in the remaining studies.
Ethical challenges were also documented surrounding the ability of the person with a neurological condition to get others to consent to be photographed. For example, consent was shown at times to be problematic (Genoe & Dupuis, 2013) or missed altogether (Balakrishnan et al., 2017). Other ethical challenges reported included challenges in understanding that consent was required from those photographed (e.g., dementia) (Genoe & Dupuis, 2013) and difficulty asking consent of people in photographs (e.g., post-stroke, aphasia and dementia) (Evans et al., 2016; Genoe & Dupuis, 2013, 2014; Levin et al., 2007; Wiersma, 2011). Some neurological conditions make it more difficult to ask permission or to understand the consent process (e.g., dementia and post-stroke aphasia), thus making it harder to adhere to ethical procedures. To overcome such challenges, some studies adapted the process to suit the needs of the neurological population by providing a wallet sized card to participants explaining aphasia with a sentence asking permission for the participant to take someone’s photograph (Levin et al., 2007). Other more difficult ethical challenges to overcome were those issues that included capacity and impaired memory to match people in photographs to the consent form.
Theme 2: Losses and Benefit Finding
This theme highlights the challenges faced by those with a neurological condition, the complexity surrounding living with a condition (interpersonal and intrapersonal types of experience), and how savouring was used as a strategy to overcome challenges. Adaptive strategies included living in the moment, savouring one’s connection to others, and fostering positivity and hope for the future despite challenges.
Pushed Aside from Society
Insufficiencies in healthcare and rehabilitation issues were most apparent in terms of rehabilitation, treatment, and care challenges. These system-level (healthcare system) challenges highlighted a need for more support and timely care for people living with a neurological condition (e.g., Amyotrophic Lateral Sclerosis, myotonic dystrophy, stroke, Parkinson’s disease, cerebral palsy) (Gunton et al., 2021; LaDonna et al., 2015; Maratos et al., 2016; Roger et al., 2018; Tornbom et al., 2019; van Heijningen et al., 2021): “You get help for six months after the stroke, and then you get no more help. The speech therapy stuff, I have had to sort out myself. Same thing with physiotherapy and other exercise” Stroke (Tornbom et al., 2019). “In addition, participants felt this lack of awareness of most neurological conditions extended to the health-care system, leading to incorrect and prolonged diagnoses, as well as other barriers to available treatment and care. For example, while technology and tests are heavily relied upon today, they make both patients and clinicians vulnerable to quick answers. It requires a leap of faith by a professional to stay with a patient’s experience in order to provide the best possible symptom management, otherwise, clinicians may inadvertently exacerbate the negative experiences of their patients with the health-care system” Parkinson’s disease (Roger et al., 2018).
A lack of understanding and consideration with paternalistic actions directed toward the persons living with a neurological condition exemplifies being treated and perceived differently because of one’s neurological condition, and this resulted in feeling being pushed aside by society (Balakrishnan et al., 2017; Barclay-Goddard et al., 2012; Evans et al., 2016; Genoe & Dupuis, 2011; Gunton et al., 2021; LaDonna & Venance, 2015; Maratos et al., 2016; Roger et al., 2018; van Heijningen et al., 2021). It was reported that this different treatment directly resulted in the person living with the neurological condition questioning their capabilities and competence, resulting in the individual feeling negative towards such actions taken by others towards them (Genoe & Dupuis, 2011).
Physical environmental challenges were also illuminated and were presented in the photographs and accompanying narrative by documented obstructions and other obstacles that caused problems to the individual living with a neurological condition (Balakrishnan et al., 2017; Barclay-Goddard et al., 2012; Bishop et al., 2013; Evans et al., 2016; Genoe & Dupuis, 2013; Gunton et al., 2021; Maratos et al., 2016; Seetharaman et al., 2021; Tornbom et al., 2019; van Heijningen et al., 2021; Walker et al., 2020).
The Progressive Decline of Self
Intrapersonal challenges were marked by emotional barriers causing mood swings signified by the frustration felt and challenges of dealing with the physical, mental, and emotional changes of living with a neurological condition resulting in a progressive decline of self. Emotional challenges (e.g., shame, disappointment, sadness), mental challenges (muddled thinking and decline), physical deterioration (reductions in capacities) and the constant intrapersonal battles faced by people living with a neurological condition were demonstrated to progressively decline and corrode a former self: “So yeah, there are many, many, many, many days that I get frustrated, I get down, I cry …” [refers to when skills were lost]. Dementia (Genoe & Dupuis, 2014).
The above quote emphasises the struggles of a ‘lost previous self’ through the repetition of ‘many’ and the frustrations and emotions that accompany living with dementia.
Growing As A Result of Losses
Studies highlighted that while many people with neurological conditions experience a myriad of losses, they also grow as a result of these losses (Balakrishnan et al., 2017; Barclay-Goddard et al., 2012; Genoe & Dupuis, 2011, 2014; Greer et al., 2015; Hebblethwaite & Curley, 2015; LaDonna & Venance, 2015; Maratos et al., 2016; Roger et al., 2018; Tornbom et al., 2019). While reconciling the reality of their diagnosis, or as physical and mental capacities deteriorated with the neurological disease progressing, a positive attitude and a new look on newfound capacities and ability to savour the present mental and physical functions provided a sense of hope by being optimistic and maintaining positive attitudes towards the present and future. Greer et al. (2015) detailed that one participant took a photograph of a butterfly which was a powerful metaphor to represent their growth as the butterfly exemplified their positive attitude and transformation as a result of their losses: “Well, the butterfly itself is a symbol of renewal, of coming out of a tomb. And in doing this, I just felt I could just fly out of this body that I’ve used up. Well, it’s a symbol of new life and it’s a symbol of resurrection and it’s… butterfly is just a symbol to me of living. I think that’s what we have to do” Parkinson’s disease (Greer et al., 2015).
The above quote highlights despite physical deterioration occurring, the person living with Parkinson’s disease can still take a positive attitude toward life.
Savouring through positive reflection and hope by the use of photographs and the process of photovoice was apparent in the findings. Specifically, positive reflection demonstrated the savouring strategy used by people living with a neurological condition (Balakrishnan et al., 2017; Barclay-Goddard et al., 2012; Genoe & Dupuis, 2011, 2014; Greer et al., 2015; Gunton et al., 2021; LaDonna & Venance, 2015; Lai et al., 2019; van Heijningen et al., 2021) and a sense of hope (Genoe & Dupuis, 2014; Greer et al., 2015; Gunton et al., 2021; Hebblethwaite & Curley, 2015; LaDonna & Venance, 2015; Tornbom et al., 2019). Photovoice facilitated this technique of positive reflection with photographs allowing the experience to be savoured (Balakrishnan et al., 2017; Barclay-Goddard et al., 2012; Genoe & Dupuis, 2011, 2013, 2014; Hebblethwaite & Curley, 2015; van Heijningen et al., 2021).
In one study, a participant discussed the connection between a photograph and reinforcing the bond to those that appear within the photograph because the photograph acted as a reminder that they were not alone (Genoe & Dupuis, 2014). For example, savouring by appreciating the moment and connection is exemplified in the following quote: “… it’s a combination of peers being together, friends being together, with a purpose … it gave us time to talk about what we each found difficult at that period of time, with our journey. So there again [the photo] reinforces the bond and for me it gives me a purpose to continue because I know I’m not alone.” Dementia (Genoe & Dupuis, 2014)
Relationships were important to people living with neurological conditions (Balakrishnan et al., 2017; Barclay-Goddard et al., 2012; Genoe & Dupuis, 2011, 2013, 2014; Hebblethwaite & Curley, 2015; van Heijningen et al., 2021). Support networks were savoured by being cherished and, although primarily reported to focus on significant others, the sense of connection and relationships also extended to appreciating relationships with pets. “To cuddle with pets is an excellent way to recover … cuddling with my cat has been lifesaving to me! And also, that pets don´t speak! So nice”. Stroke (Tornbom et al., 2019) “Both being among other people and sharing experiences and joy, but also being able to help and support others in their lives, were the main reasons for volunteering… I do the phone circle helpline on Wednesday mornings, and it takes three-quarters of an hour, which usually works out. And it’s nice work.” Cerebral Palsy (van Heijningen et al., 2021)
Discussion
Overall, this scoping review provides a synthesis of the extent, range, and nature of how photovoice has been applied to date in neurological research. The reflexive thematic qualitative synthesis of the articles was useful for depth of engagement over the challenges encountered when attempting to implement photovoice yet at the same time also providing an articulation of the lived experience across a broad range of neurological conditions.
Adaption was shown to be useful to help overcome a range of complexities of implementing photovoice steps (e.g., issues around manual dexterity) when using digital or disposable cameras (Genoe & Dupuis, 2013, 2014), mobile phones, polaroids, or tablets, since many of the participants were found to be struggling with camera equipment. For specific neurological populations, adaption to cameras was necessary (Barclay-Goddard et al., 2012; Evans et al., 2016; Genoe & Dupuis, 2013, 2014; Tornbom et al., 2019). Adaption due to implementation complexities regarding cameras was recommended in studies, such as providing better camera equipment, more careful instructions for using cameras and directly adapting camera equipment to match the needs of the neurological condition. Or, even in proposing strategies to better fit the needs of the neurological population under study (e.g., stroke with aphasia, which included motor challenges that make coordination for camera use difficult, use of aphasia-friendly instructions, graphic instructions, story booklets – notecards to gain consent, or augmentative and alternative communication devices, etc.) (Levin et al., 2007). Likewise, implementation complexity was highlighted when attempts were made to implement informed consent (Wang, 1999). Participants with a neurological condition giving their consent to participate in the research and also obtaining consent from people that appeared in their photographs (essentially acting as co-researchers) were shown to be more difficult for specific neurological populations (e.g., dementia and post-stroke aphasia) (Genoe & Dupuis, 2013; Levin et al., 2007). Therefore, some of the neurological research focused on the implementation issues of taking pictures without permission, or photographs that risked the portrayal of others without permission, which was of particular concern for some stroke survivors with long-term impairments such as aphasia (Levin et al., 2007) and those with dementia conditions (Genoe & Dupuis, 2013; Levin et al., 2007). Moreover, studies also reported that it was helpful to adapt photovoice steps, with options including having a companion or family member present to obtain consent, and/or helping to set up and take the photographs on behalf of the person with the neurological condition (Evans et al., 2016). A recommendation, therefore, would be for future research on photovoice within neurological conditions to adapt the processes around obtaining informed consent (step 4), adapting cameras (step 6) and the SHOWeD method (step 8), but not to miss the core step of galley exhibits, whereby findings can be disseminated, and social change created (step 9) (Wang, 1999).
The theme of losses and benefit finding highlights the common challenges and strategies used by people living with a neurological condition. This included issues faced, such as insufficiencies in healthcare and access to rehabilitation services, indicating a view that people with neurological conditions may be treated differently. In a number of papers, the complicated health system left people living with a neurological condition confused as to why care stopped suddenly and no more services were available (Gunton et al., 2021; LaDonna et al., 2015; Maratos et al., 2016; Roger et al., 2018; Tornbom et al., 2019; van Heijningen et al., 2021). Tornbom et al. (2019) also found that many years after a stroke, participants still experienced improvements through persistent rehabilitation, and wished for more interactive rehabilitation training, including collaborative forms of rehabilitation being suggested in the long-term phase of stroke. In addition, there seemed to be a lack of understanding and consideration toward people living with a neurological condition by the public, family, and the medical profession (Balakrishnan et al., 2017; Barclay-Goddard et al., 2012; Evans et al., 2016; Genoe & Dupuis, 2011; Gunton et al., 2021; LaDonna & Venance, 2015; Maratos et al., 2016; Roger et al., 2018; van Heijningen et al., 2021). Multiple misunderstandings were highlighted by a person with a neurological condition missing an appointment with the stroke team because of their problem remembering to turn up for the appointment, and this person living with stroke thereafter incurred bills for this missed visit (Tornbom et al., 2019). This dismissive and negative behaviour shown toward people living with a neurological condition was also exhibited by family members in the form of paternalistic actions whereby daily chores, roles, and responsibilities were directly taken away from the individual with a neurological condition. Although this was often intended for good, it led the person living with a neurological condition to feel as if they were being undermined in terms of their capabilities, thus negatively impacting their confidence.
Obstacles and obstructions that posed threats to physical safety (e.g., narrow aisles, sidewalks in poor condition, lack of outdoor lighting, or lack of accessible entrances) also presented challenges. Without change around these issues, people living with neurological conditions could be hindered from living successfully due to the negative impact on their confidence and independence (Balakrishnan et al., 2017; Barclay-Goddard et al., 2012; Bishop et al., 2013; Evans et al., 2016; Genoe & Dupuis, 2013; Gunton et al., 2021; Maratos et al., 2016; Seetharaman et al., 2021; Tornbom et al., 2019; van Heijningen et al., 2021; Walker et al., 2020). By not addressing the social needs required for change, concerns around physical environmental barriers could likely prevent activities such as going to shops or restaurants and further isolate people living with neurological conditions from society, resulting in a person feeling ignored and not important enough for society to address such issues, and leaving a sense of disappointment with how people living with a neurological condition are being treated by society. A similar argument exists directed at the Australian Government’s National Disability Insurance Scheme (NDIS), which was reviewed, as previously it discriminated against people living with a neurological condition aged over 65 years old who, unless already in the government scheme, were pronounced ineligible for NDIS funding, leaving older people who experience neurological conditions later on in life totally and utterly stranded and ignored by this disability service (Matthews et al., 2021).
The lived experience of both encountering losses but interestingly seeking out benefits shows that despite the physical and mental decline, people can live successfully with a neurological condition by remaining hopeful and optimistic and savouring their current physical as well as mental status despite the inevitable continued losses experienced. Since it was shown that benefit finding and support networks helped people grow as a result of losses (Balakrishnan et al., 2017; Barclay-Goddard et al., 2012; Genoe & Dupuis, 2011, 2014; Greer et al., 2015; Hebblethwaite & Curley, 2015; LaDonna & Venance, 2015; Maratos et al., 2016; Roger et al., 2018; Tornbom et al., 2019).
Savouring is linked to positive psychology (Bryant & Veroff, 2007) and also included positive affectivity and optimism. For those with neurological conditions, savouring was a strategy with both cognitive and behavioural strategies deployed to positively reflect and provide a sense of hope to accept new capacities and to find a renewed purpose in life. Experience of positive support, which included those in one’s social network, was shown through strong social ties and maintaining those relationships shown within photographs with photographs acting as conduits of moments shared, representing their relationships with others and signifying how important maintaining relationships are for those with a neurological condition (Balakrishnan et al., 2017; Barclay-Goddard et al., 2012; Genoe & Dupuis, 2011, 2013, 2014; Hebblethwaite & Curley, 2015; van Heijningen et al., 2021). The positivity and optimism shown in savouring (whether encountering one’s own emotions or external events) enables people to deconstruct, reflect and re-evaluate sensory experiences that took place at the time of the photograph and appreciate the different emotions experienced thereafter in the form of the photograph. The savouring experience (Bryant, 2003), as applied to photovoice, can cover a combination of reminiscence (temporal focus on the past), present awareness, and the future (anticipation – remembering how much they looked forward to it earlier, which is recalled anticipation or reminiscing about it later which is called anticipated recall). This could relate to a past positive experience depicted in a photograph. A present positive experience evoked taking the photograph or discussing it in the focus-group or interview discussion, for which a photograph has served as a prompt, or a future positive experience a participant expresses hope to come to fruition. In short, there appears to be a combination of reminiscence, present awareness, and anticipation. To emphasise this point for future studies, savouring complements photovoice methodology whereby people are required to take a photograph, present a narrative that accompanies the photograph delivered to a broader group to highlight the meaning behind the photograph and verbalise, share and communicate those sensory experiences to others. This experience in itself may contribute to fostering reminiscence, present awareness, anticipation, and may act to intensify and prolong feelings of positivity and hope (Evans, 2011; Smith & Bryant, 2016).
On the topic of terminology, it is worth noting that photovoice is presented in the seminal paper by Wang and Burris (1997) as a method (set of steps) with its own methodology (theoretical underpinnings, rationale, justification for that method), but later Wang (1999) describes photovoice as a method of PAR and a series of steps to follow which include a final step outlining the action component (social change) of PAR, that requires the delivery of a photovoice exhibit step. Likewise, some studies using photovoice within the context of neurological conditions used the term ‘photovoice method’, and this clearly defined photovoice as a method of PAR, with photovoice shining a light on the roles of ‘
The confusion over terminology may run even deeper in its potential influence since it may explain some of the variation found in implementation between the various studies. In the context of neurological conditions, there is considerable variation in the implementation of a photovoice study and the use of the photovoice methodology steps outlined by Wang (1999) in their seminal photovoice literature. Only a few studies showed that they were implementing the last step (Step 9) as photovoice was originally intended to be delivered with the presentation of findings to key stakeholder groups through gallery exhibits (Balakrishnan et al., 2017; Bishop et al., 2013; Evans et al., 2016; Pace, 2020; Tornbom et al., 2019). Missing this step can result in a lost opportunity for raising awareness with policymakers or for any collaborative endpoint changes, which can reduce the social change aspect of photovoice and limit the potential influence of those with lived experience on people with the power to make endpoint changes. Without this final step, the photovoice goal of social change becomes less attainable. There was a lack of clarity over why this step was omitted. Some potential reasons for this omission could be that this final step may be hard to achieve with resource implications and is perhaps reflective of the lack of clarity and consistency within the epistemological positioning. To explore the idea of resource implications in more detail, technological development and the use of social media may afford new ways of engaging policymakers in final gallery exhibits (see for example, Aboulkacem et al., 2021) and could potentially overcome such fiscal issues, but only if some of the risks can be mitigated. Therefore, several things to be considered when using social media technology for gallery exhibits, including ethical procedures and rigourous safeguarding procedures required due to the importance of dissemination of imagery. Since the movement from a controlled environment of a face-to-face gallery exhibit (where control of who is attending and invited to view photographs) to a less controlled environment of social media platforms highlights the differences in how photographs can be used and where they may end up, which may have potentially negative repercussions in the long term for those photographed (e.g., the photograph used differently then what the person taking the photograph intended). Alternatively, reflecting on the photovoice method and photovoice methodology debate presented earlier, the final gallery exhibit step is the action step within PAR to initiate social change. However, perhaps some authors viewed photovoice as its method (i.e. a set of steps) with its methodology (theoretical underpinnings, rationale, justification for that method) and this could be an equally valid explanation of why some studies chose not to include the final exhibit step. Thus, providing another potential explanation that is also feasible.
An advantage of Braun and Clarke’s (2019) reflexive thematic analysis is that researchers reflect on their experiences, values and how this shapes the meanings and gives life to the research conducted. AN's collaboration with the decision-making process in the construction of themes was an integral part of the analytic process. AN reflected on his experience being involved in this research and is a person with lived experience of a neurological condition involved throughout the development of this paper, from conceptualising the review to reviewing findings and preparing recommendations. To summarise AN’s reflection on being part of this research is highlighted by the following: It is a strong desire to help benefit research through lived experience, to use research to make change for people living with neurological conditions, and to lobby for those over 65 years old to be included in the NDIS [National Disability Insurance Scheme in Australia] and to help people to live their best lives despite their neurological condition (with the NDIS policy viewed as age discrimination and subsequently being reconsidered by NDIS). AN’s knowledge and lived experience added rigor to recommendations and ensured the research remained focused on improving the lives of people living with a neurological condition and raising awareness about the lived experience.
A final area for further investigation is the adaption of photovoice steps, as this practice makes photovoice more relevant and appropriate to the neurological population. In addition, as new research becomes available, further exploration of strategies to help people living with different neurological conditions is a worthwhile endeavour. It is a topic recently addressed in a commentary paper on photovoice within neurological research (Lorenz & Bush, 2022).
A recommendation from the scoping review findings would be for future research to explore the link between savouring and photovoice since savouring events and sharing stories about past events, or future plans has been shown to enhance and amplify positive emotions (Bryant et al., 2011). For example, in sharing photographs in group work, others in the photovoice group may also point out relevant positive details in the photograph that the person may have missed from an event that further heightens the secondary experience of the affective response. Watching another person and their emotional reaction to a photograph can also increase one’s positive emotions (Bryant & Veroff, 2007). For example, in the extant savouring literature, a study documented the use of expressive-based interventions using photographs with open-ended prompts in persons with dementia, reporting improvement in positive affect and interpersonal communication skills immediately at post-intervention and at 2-month follow-up (Pereira et al., 2021). This is a promising finding as it parallels the current study findings of savouring as a potential strategy and provides an understanding for future research to link photovoice and savouring together (Ando et al., 2020; Dlugonski et al., 2012; Lai et al., 2019).
Conclusion
PAR methods, such as photovoice, are intent on understanding lived experience. In this scoping review, it provided a voice for those living with neurological conditions. In addition, the scoping review identifies some challenges both in terms of implementation of the photovoice steps in neurological research and challenges living with a neurological condition. Examples of the lived experience included feeling pushed aside by society, particularly focusing on insufficient healthcare and rehabilitation and the strategies (savouring) to deal with such challenges. Implementation complexities require adaptions to steps within photovoice to better fit the needs of the neurological population, and we encourage such adaptions and call for a further adaption to include savouring type questions within the SHOWeD method for future research in photovoice. Finally, adaptions to core steps should be avoided, such as missing out on gallery exhibits, since the goal of photovoice is to initiate social change, and by missing this core step, social change is less attainable.
Supplemental Material
Supplemental Material - Exploring the Use of Photovoice in Understanding the Lived Experience of Neurological Conditions: A Scoping Review and Reflexive Thematic Analysis
Supplemental Material for Exploring the Use of Photovoice in Understanding the Lived Experience of Neurological Conditions: A Scoping Review and Reflective Thematic Analysis by James Smith Andre Nels, Laura Emery, and Mandy Stanley in International Journal of Qualitative Methods
Footnotes
Acknowledgments
We would like to acknowledge colleagues Professor Joanne Dickson, Dr James Kelly and Ms Manja Laws for their continued support and advice.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Multiple Sclerosis Society of Western Australia (MSWA).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.