
Abstract
Chinese scholarship conducting/attempting critical discourse analysis (CDA) on the doctor–patient relationship in China has, to date, predominantly relied on the use of analytical tools from systemic functional linguistics and pragmatics. This methodological orientation, by prioritizing the linguistic structure and functions of the textual data, does not tend to take into consideration the sociocultural contexts, complex power relations, genealogy of discourse, and practice-orientedness of discourse that CDA approaches usually touch on. This protocol article proposes a research design that constructs a systematic-dynamic CDA approach in the context of the doctor–patient relationship in western China in order to incorporate the aforementioned factors that previous Chinese scholarship has ignored. Physicians, cancer patients and their family members, and CDA methodologists are to be recruited to participate in focus groups and interviews to discuss the doctor–patient relationship from their own experience and to inform the construction of an integrated CDA approach. Qualitative context analysis will be adopted to analyze texts transcribed from interviews and focus groups, in order to generate themes and new concepts for the design of a novel systematic-dynamic CDA framework. By establishing an integrated CDA approach tailored to the doctor–patient relationship in western China, we will be able to provide empirical evidence and valuable insights to practitioners and policymakers to ease doctor–patient conflicts, which have intensified in recent years, and facilitate more harmonious relationships.
Keywords
Background
In the last decade, due to increasing doctor–patient conflicts in China (Du et al., 2020; Xiao et al., 2021; Yan, 2018; Zhao & Zhang, 2019), more Chinese researchers have begun to study the doctor–patient relationship, especially through the approach of critical discourse analysis (CDA). CDA, which arose in the 1980s in western scholarship, emphasizes the sociocultural implications of language and the social practice of language application, rather than the intrinsic rules of language itself (Ferguson, 2019). Most of the Chinese researchers using this approach have taken CDA as a fixed theoretical-methodological framework, consequently overlooking the concerns that a critical qualitative approach should be grounded in the research question, the theoretical framework should be adjusted as needed to integrate theoretical choices, and the methodological tools should be constructed in close relation to the contexts and scenarios to be investigated. As CDA represents a category of interdisciplinary theories and methods fundamentally defined by critique, there is no systematic methodological blueprint for CDA that can be followed step-by-step; rather, any so-called CDA framework is ever evolving and led by the specific research question and its relevant context (Wodak & Meyer, 2015).
Three main approaches have been taken to using CDA to examine the doctor–patient relationship in western literature. The first is the dialectical-relational approach brought forward by Fairclough (1993), who examined the dialectical relationships between the text, discourse, and social practices that are observed when doctors and patients interact. Analysis of relevant texts reveals discursive mechanisms which interact with sociocultural contexts to further illuminate the social practices hidden behind the language use of both doctors and patients. The second is the discourse-historical approach proposed by Reisigl and Wodak (2016), which advocated a deeper engagement with Foucault’s discursive theories to explore the social, cultural, and historical factors of discourse and the power relations behind it. Adopting the discourse-historical approach, Reisigl and Wodak examined the aforementioned factors behind the interactions between doctors and patients of different cultures. They argue that cultural and historical backgrounds have notable influences on doctor–patient communication. The third approach, advocated by Van Dijk (2015), is a sociocognitive one. This researcher argued that the cognitive activities of the individual and of groups provide the medium that connects social practice and discursive practice, and that cognitive activities are often multidirectional and do not move unilaterally from social practice towards discursive practice. Taking the sociocognitive approach, Lippa et al. (2017) studied the interactions between doctors and multiple sclerosis patients and their joint construction of disease. Their findings uncovered the cognitive mechanism on both sides and were used to support their argument that medical cognition is bilateral rather than existing only on the side of the doctor.
Literature Review of Chinese Scholarship and Originality of the Study
Mainstream Chinese research on the doctor–patient relationship has mainly used analytic tools from systemic functional linguistics and pragmatics to conduct CDA. Scholars such as Tan (2017), Zhang and Feng (2019), and Luo (2020) have analyzed doctor–patient conversational texts by looking into their linguistic structures and functions to reveal binary power relationships and institutional characteristics. Many of these scholars claimed to have adopted Fairclough’s dialectical-relational approach as their theoretical basis. However, they have predominantly focused on the interpretation of the linguistic meaning of texts while neglecting the non-linguistic content of discourse and the social practice behind discourse, both of which are taken into consideration in Fairclough’s approach.
That said, a small group of Chinese scholars does deal with the verbal and non-verbal parts of discourse in a more balanced way. For example, Zhu and Huang (2018) applied Fairclough’s dialectical-relational approach to explore how the image of young doctor is constructed by the media. They explained at length the discursive construction that supports the media’s stigmatization of young doctors and its construction of patients as victims, which cannot be expressed by linguistic rules alone. Another group of scholars took this approach further by paying increased attention to the sociocultural features of discourse. For example, Tang and Liao (2016), Liu and Jia (2017), and Tu (2019) based their work on Foucault’s argument that the modern medical system dominates the humanistic orientation of doctors and patients. These researchers concluded that the extreme power inequality between doctors and patients in Chinese society has a significant negative effect on the harmoniousness of the relationship. However, these researchers did not take a genealogical perspective: the way the modern medical system evolves requires a historical analysis of trajectories of medical reform, especially in China where political forces have played a major role in shaping and constructing the medical system and medical practices (Bu, 2017). Moreover, this body of work is unilaterally oriented towards describing power relations in which doctors are favored over patients and thereby inevitably ignores the complex relationship between discourse and power. Power encompasses not only innate traits of discipline and control but also the capability to produce and enable social interactions and structures within the construction of discourse. Existing Chinese studies only focus on doctor–patient communication barriers caused by the power inequality between the two sides (Shen & Zhang, 2013; Tu et al., 2019), and only a few scholars (e.g., Kuang & Liu, 2017), have explored the productive mechanism of the power structure that exists between doctors and patients in China.
Another important feature of non-verbal discourse that has been so far overlooked by Chinese scholars is its practical elements such as actions, practice, and the actors themselves. Language and action are not necessarily consistent with each other, and the observation and recognition of individual behavior that cannot be directly reflected in text are sometimes crucial for understanding discursive construction. Non-Chinese CDA scholars such as Leeuwen (2008) and Willig (2003) have emphasized the non-symbolic element of discursive practice by, for example, revealing from their analyses of doctor–patient conversations, a set of mechanisms that identify the way that specific verbs and the interactivity between words and tones eventually reflect social practice. In China, only a handful of scholars have introduced the concept of practice into the study of the doctor–patient relationship. For example, Wu and Wang (2019) discussed the practical elements of discourse in the application of their trust–repair discourse model, which advocates the use of a top-down approach to diminish the mistrust that currently exists in Chinese society between doctors and patients. Studies such as theirs that involve thoughtful reflections on practice based on conversational texts would perhaps benefit from the collection of data from participatory observation of practices or the undertaking of historical analysis of practical elements of discursive constructions.
To bridge the aforementioned gaps, we endeavor to construct a theoretical-methodological framework of CDA in our research, drawing inspiration from the three established international CDA approaches discussed earlier. Our approach, which we refer to as systematic-dynamic, integrates the dialectical relationship between non-linguistic elements and their sociocultural contexts, the genealogy of discourse, the pluralist view of power, and practice orientedness in discursive construction, all of which are lacking in existing Chinese literature. This integration forms the baseline theoretical framework of our study, in which we attempt to enrich or expand the theories and methods of CDA by analyzing the doctor–patient relationship in public hospitals in western China, so as to provide reflective knowledge for the construction of CDA approaches suitable for Chinese characteristics.
The objectives of this study are as follows: (1) to construct a theoretical-methodological model of CDA which can be verified and modified in the empirical study of the doctor–patient relationship in western China; and (2) to explore the mechanism of the current doctor–patient relationship through the constructed CDA approach and thereby provide a theoretical foundation for resolving doctor–patient conflicts. By presenting empirical evidence to a multidisciplinary team of practitioners (e.g., physicians, nurses, and medical social workers; He, Wu, et al., 2022) and relevant policymakers, we hope to reduce conflicts in practice and formulate supportive policies to improve doctor–patient communications and understanding.
Explanation and Justification of the Method
In this study, a qualitative approach as well as a nascent CDA approach is employed. This methodological choice allows for the construction of a systematic-dynamic approach, and is helpful for fully understanding the discourse that circumscribes the doctor–patient relationship and the social practices behind this discourse. The current CDA in China of the doctor–patient relationship lacks a dynamic, holistic perspective and, instead, rigidly follows one CDA approach that has been established internationally without critical examination. Arguably, the existing approach overlooks the complexity, historicity, and practicality of discourse. Through our CDA of the doctor–patient relationship as conveyed in interviews, focus group transcripts, and conversation texts, we try to construct a set of data collection and analytical methods tailored for Chinese contexts, so as to expand the CDA methodological family in response to a new cultural context of application.
Materials and Methods
Site Selection
There are two main reasons for selecting western China as the field site. First, the authors are based in a university in western China, and therefore it is convenient to collect data in public hospitals there. Second, doctor–patient conflicts are a substantial issue in western China, in part due to lagging economic development in this region and the underdeveloped local health infrastructure (Shen et al., 2017).
Study Period
Schedule of Research.
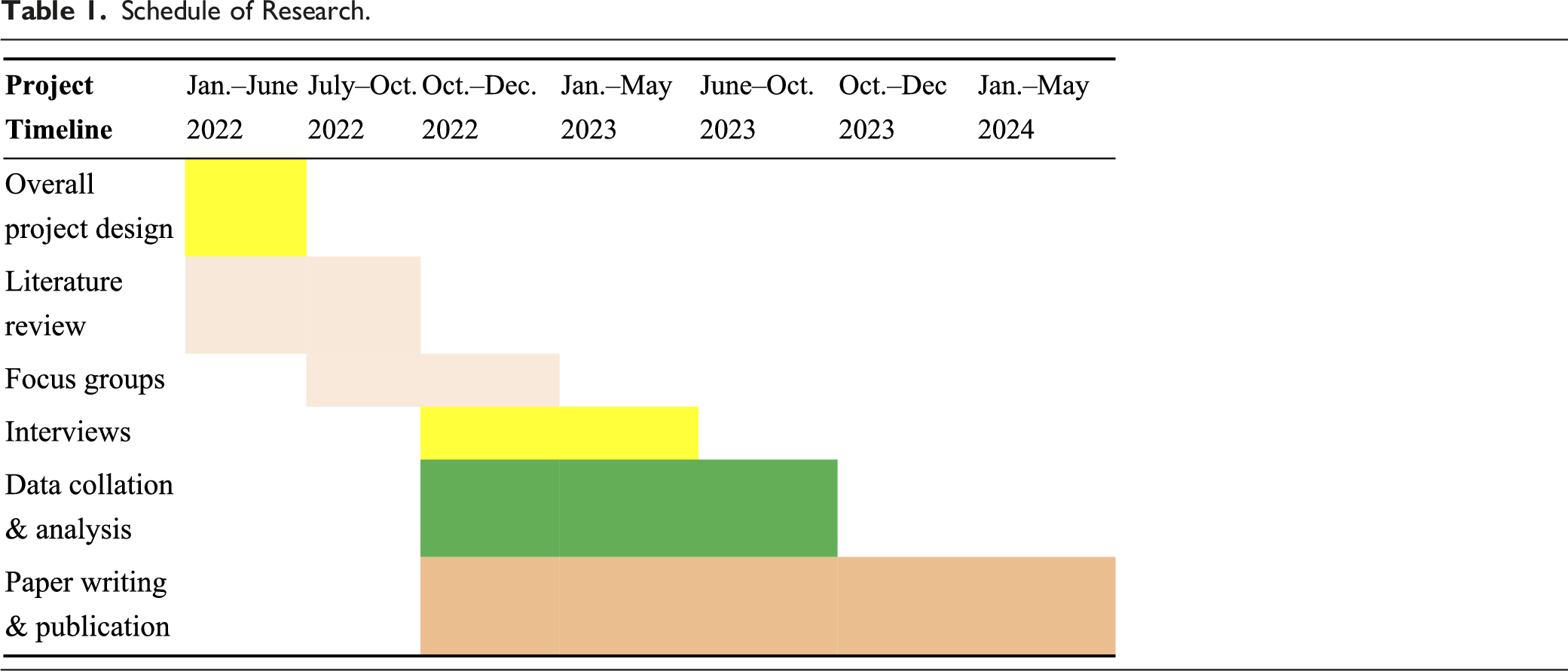

To collect data, two techniques have been adopted. Focus groups led by the main researcher (the first author) will be held among the targeted demographic groups to discuss a series of semi-structured questions (Baden et al., 2022; Moloney, 2011; Yaylacı, 2020), and to yield unexpected findings. In-depth interviews will also be conducted, guided by a set of semi-structured questions in relation to the research objectives, accepting the likelihood that some answers obtained may not be closely related to the interview guide (Cantero-Garlito et al., 2020).
A focus group guide (Appendix 1) and an interview guide (Appendix 2) have been designed, partly inspired by relevant literature, to initiate the discussion about the research objectives. Some of the questions in these guides will be modified on the spot during sessions, according to participant responses. The first author is conducting the focus groups and interviews (already begun), which are taking place in the selected field hospitals and are expected to be completed between November 2022 and January 2023. Audio recording is being used to collect the qualitative data generated from the process. We will stop conducting interviews once the data reaches theoretical saturation. However, as the focus groups are to be used for preliminary construction of the theoretical-methodological framework of an integrated CDA approach, the data collected does not need to reach theoretical saturation.
Sampling/Recruitment
Participant selection is to take place between September 2022 and January 2023, using a purposive sampling technique. Even though the project has gained support at the hospital management level, the researchers understand the barriers in recruiting participants in the context of end-of-life. We acknowledge the difficulty in encouraging participants to discuss topics in relation to the death of their family members, due to Chinese familism, filial piety, and the taboo against talking about death in Chinese culture (He & van Heugten, 2020).
Participants: Focus Groups
The focus groups will include three groups of participants recruited from the selected hospitals in city A, Sichuan Province, China: a group of oncology specialists or doctors in charge of cancer patients (8–12 persons), a group of cancer patients and their families (10–15 persons), and a group of methodologists (5–eight persons) familiar with critical discourse analysis. The discussion will focus on the views and perspectives of participants of the doctor–patient relationship, in their own experience, and on how to construct a preliminary framework for integrated critical discourse analysis.
Participants: In-Depth Interviews
Participant recruitment for the in-depth interviews has been completed in three local hospitals in City A, Sichuan Province; City B, Gansu Province (in northwest China); and City C, Yunan Province. Interview participants include cancer patients and their family members and physicians. Within the hospitals, 15–24 participant units have been recruited (5–8 per hospital), with each unit including one cancer patient, one or two family members (usually the spouse or adult children), and the attending physician (who could also be part of other units). Interviews are expected to last between a half hour and 3 hours as appropriate.
Recruitment Strategy
For the focus group stage, with the help of the head of public affairs in the participating hospital in City A (Sichuan), we have distributed pamphlets to potential doctors and patients (including family members) and successfully recruited ten doctors, 12 patients, and 12 family members. The first author has also begun contacting potential methodologists specialized in critical discourse analysis in China, aiming to recruit five to eight people to join an online focus group to discuss developing an integrated critical discourse analysis approach for analyzing the doctor–patient relationship in western China.
For the interview stage, we have already contacted 4 wards or management level at the participating hospitals to help with participant recruitment. Pamphlets detailing the study will be sent to the liaison at each hospital to distribute to potential participants. Phone calls will be made to those showing interest in participating to confirm their participation; for those agreeing to participate, appropriate interview time slots will be arranged at their convenience (due to the COVID-19 travel constraints, it is expected that most interviews will take place via video chat or telephone; He, Mu, et al., 2022). The recruitment strategy will be based on data saturation (where new concepts no longer arise from the texts) rather than on a preplanned number of participating units.
Before any focus group or interview begins, explanation will be given regarding the study rationale, the guarantee of participant anonymity, and the rights of participants (such as the rights to drop out of the study at any time and avoid any form of harm).
Data Handling/Analysis
Transcription and Translation
At the start of focus group or interview sessions, consent for recording each session will be obtained from the participants. With permission obtained, the entire session will be recorded using recording pens, and the interviewers may also take field notes. After the session, the interviewer will connect the recording pens to the computer for electronic transcription, and then check transcriptions against the recordings and manually correct any mistakes. The interviewers will also type up the field notes and insert them into the transcribed texts as appropriate.
Data Analysis
In this study, a data analysis method of qualitative content analysis is to be used. For the focus group data, the authors will read the transcribed texts repeatedly to familiarize themselves with the qualitative data. A preliminary CDA framework will be constructed based on the relevant literature and the analysis of the focus group data. For the interview data, the authors will first carry out several intensive readings of the transcriptions, take reflective notes, and conduct critical discourse analysis to extract major themes, adopting the preliminary CDA approach devised after the focus group stage. The authors will meet regularly to exchange notes and ideas about emerging themes. An external auditor, who is an expert in CDA in the field of doctor–patient relationships, will also be invited to examine the themes and concepts generated as well as the entire analytical process. The authors will then begin to convert these themes, concepts, and reflections into a manuscript draft.
Preliminary Results and Discussion
This study aims to develop an integrated CDA approach in western China. As shown in Figure 1, based on existing international and domestic Chinese literature, the theoretical framework and specific methods of a preliminary CDA approach suitable for the context of the doctor–patient relationship in China will be constructed and then analyzed and improved to best suit that context. Research process and the preliminary theoretico-methodological framework.
Preliminary Theoretical Framework Construction: Systematic-Dynamic Critical Discourse Analysis
Based on the key ideas of the three important schools of CDA and the gaps in the Chinese scholarship identified in the introduction section, this study endeavors to identify a suitable theoretical and methodological approach to examine and understand the doctor–patient relationship in China. As shown in Figure 1, this preliminary theoretical framework primarily consists of four aspects: the dialectical relationship with sociocultural factors, multidimensional power relations, genealogical analysis, and practice orientedness.
The dialectical relationship with sociocultural factors is to be incorporated into the framework because the literature in which CDA has been used to investigate the doctor–patient relationship in China arguably places too great a weight on textual structure and other linguistic functions: the strategy of organizing words and sentences may result in the objectification of an ideological structure and reinforce a form of power relations. In overlooking or assigning too little importance to the non-linguistic elements of discourse, the dialectical relationship between wider sociocultural factors and the meaning of discourse has been neglected.
Multidimensional power relations and genealogical analysis are included because Chinese studies have also focused solely on the negative effects of the power relationship between doctors and patients, without recognizing the potential productive function of power relations where the doctor, as the professional, is in the dominant position in diagnosis and disease treatment. For example, in the early stage of China’s economic reform, initiated in 1978, in order to establish the authority of modern medicine over Chinese traditional medicine and folk medicine, the authoritative status of doctors was promoted and strengthened in official and public discourse (Blumenthal & Hsiao, 2015). Power and its discursive mechanisms are subject to constant change. We incorporate the theoretical-methodological element of genealogical historical discourse analysis to highlight the diachronic and historical features of the discursive construction of power relations, especially in a rapidly changing context such as China.
Practice orientedness also belongs in this framework because this element of discourse plays an important role in revealing the complex relationship that a text fails to convey. The elements of practice and non-practice mutually influence each other, temporally and spatially, and are constantly evolving, resisting, and reproducing each other, while at the same time they are being manipulated by various discourses.
To summarise, we adopt a complex, historical, and practical perspective to construct a preliminary framework for an integrated systematic-dynamic CDA approach.
Methodological Framework for Data Collection and Analysis
On the methodological level of the development of this theoretical-methodological approach, we blend the standpoint of the importance of practice and action with the tradition, found in most ancient Chinese philosophies, of valuing practice. We, in turn, reframe the research methods to capture the spirit of practice-orientedness: that of discourse in practice. As such, during data collection and analysis, emphasis is placed on developing a reflexivity that connects practice and discourse, and the revelation of the practical elements of discourse (such as through the practical text-transcribing method) is embedded into the discourse analysis process (He et al., 2021).
Verification and Reconstruction of the Integrated CDA Approach in the Context of the Doctor–Patient Relationship
The theoretical-methodological framework that has been designed for this study is tested and modified, the discursive mechanisms in relation to the framework are enriched and expanded, and the preliminary framework is reshaped, in the context of the doctor–patient relationship in western China, so as to develop a CDA approach that is more suitable in the Chinese context.
Ethics
This research has been approved by the Ethics Committee of XX university and will be registered with the Chinese Clinical Trial Registry. Before potential participants were enrolled, they were informed of the purpose and process of the study, their right to end their participation at any time, and the measures in place to protect their safety and identity throughout. Potential participants were and are required to provide a signed consent form (either electronically or in person) prior to the focus group or interview session. The personal information of participants will be stored separately from the transcriptions and will be accessed only by the researchers conducting the data analysis. To ensure anonymity, any characteristics that might reveal the identity of the participants will be removed from any published documents. The audio files will be destroyed once the verbatim transcription is completed.
Regarding participant safety, a research assistant specialized in counseling will regularly monitor for any possible risks. If any participant tries to hurt themselves in the process of data collection, the researcher will immediately report this to the Ethics Committee of XX university and the ethics audit group at the China Clinical Trial Registration Center. The researcher will then assist the participant to seek help from the mental health department of the nearest hospital. Due to the severity of the issues investigated, information for counseling services will be prepared, and, if needed, help will be provided in the form of a certified counselor to ensure the emotional and mental health of each participant is supported. A list of websites offering mental health, trauma, and counseling services is to be distributed to participants prior to their focus group or interview session (see Appendixes 1 and 2).
Rigor
We will follow the consolidated criteria for reporting qualitative research (COREQ) guidelines (Tong et al., 2007) throughout the study.
The credibility of this study is to be ensured through the triangulation of data sources, investigators, and data collection methods. Data sources will come from different groups of people, including CDA methodologists, doctors, cancer patients, and family members. The themes and concepts emerging from the study will be confirmed by participants selected from each group (one CDA methodologist, two doctors, three cancer patients, and three family members). Two authors will extract themes and concepts separately and then pool and synthesize their findings. A third auditor will also be invited to cross-check all emerging themes and concepts.
Data dependability, in the case of a qualitative study like this that investigates human experiences, refers to the extent to which the data collected from participants are true to their actual experiences (Aspers & Corte, 2019). We will be vigilant about reflecting on the ways our subjective positioning interacts with our interpretation of the textual data, in order to reach a high degree of neutrality and impartiality. Most interpretations will be reviewed by willing participants after the verbatim transcription. Any misinterpretations will be discussed and modified until the satisfaction of the participants is achieved.
Transferability is to be enabled through a thick description of the research findings in relation to the sociopolitical and cultural contexts as well as the characteristics of the participants, so that other researchers may draw inspiration from the results and transfer the study process to other settings and scenarios in future endeavors.
Limitation
Our study involves three cities in three separate provinces in western China (two in southwestern China and one in northwestern China) that feature significant regional and cultural differences. It is to some extent problematic to categorize them together as “western China”, even though this term is frequently used in Chinese scholarship to refer to this geographic area. Although we will work to pinpoint the commonalities between these three cities in terms of the doctor–patient relationship during the analysis stage as well as recognize the provincial differences in the final discussion, it would be useful to consider these three provinces separately in terms of future adoption of our CDA approach.
The hospitals selected as study sites are all in provincial capital cities at the third-tier level. (There are three tiers of public hospitals in China: the third-tier hospitals are often the best equipped; the first-tier ones are the least-resourced community hospitals; and the second tier are the ones in between.) This means that these study sites do not represent the hospital experience of the whole province. It would be relevant to compare the doctor–patient relationship in hospitals in different cities, between urban and rural areas, or at different tier levels within the same city.
Another limitation arises from the fact that this study will not include conversational data between doctors and patients. Power relations are arguably most transparently revealed through such direct conversation. However, this form of qualitative data has already been examined extensively in the literature, and, more importantly, hidden power relations and discursive constructions, which are often undetectable in direct conversations, can be revealed through participants’ own narratives expressed in a safe environment rather than in confronting scenarios such as diagnosis sessions. Nonetheless, our approach could and should be used in the future to analyze conversational data to gain a more comprehensive understanding of the doctor–patient relationship in western China and to verify its suitability for examining conversational data.
Conclusion
In the investigation of ever-increasing doctor–patient conflicts in China, it is vital to develop tailored theories and methodologies to understand the relationship between these two parties. Considering the complexity of developing an integrated CDA methodology in the Chinese context, we have adopted and will undertake multiple strategies to enhance the rigor and trustworthiness of this study. Study results will be sent to practitioners, hospital managers, and health policymakers in order to enhance their understanding of the doctor–patient relationship in western China and identify measures they can take to improve it.
Footnotes
Acknowledgments
This work is a product of joint effort from multiple quarters. We wish to thank all our study participants, including patients, their family members, and their doctors, as well as our project assistants and volunteers, for their participation in and support for the study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Chinese Ministry of Education (2020 Youth Foundation for Humanities and Social Science Research, Project No. 20XJC840001), a fellowship from the China Postdoctoral Science Foundation (Project No. 2021M691521), the 2020 Young Teacher Development Project from the Chinese Universities Scientific Fund (Project No. 230600001002020030), and as a Major Project of the Academic Innovation Team Building from the Research Institute of Social Development, SWUFE (Project No. 2021110087).