
Abstract
We propose an original method of analysis within a hermeneutic-dialectic framework theoretically supported by the work of Hans-Georg Gadamer, Bertell Ollman, and Maria Cecilia Minayo. We draw a unique means of analysis to guide an understanding of the labor realities for health workers who care for older adults. This method of analysis proposes a way to create consensual opinions, question this consensus and then put these aspects in a dialogical encounter with the qualitative researcher and interpreter. We illustrate the application of this methodological process using dialogical conversations and narrative interviews with 12 health workers from the Brazilian Unified Health System (SUS). The hermeneutic-dialectic process of interpretation involves us in movements of comprehension, which allows us to understand realities including the actual sad situation of some territories, creating possibilities for home health care, the integrality of attention as a tool for providing home assistance in the primary care field, and the necessity of a set of services to provide an organizational routine for home visits to older people. This methodological analysis has the potentiality to help develop other research on similar topics. The results illustrate that good home care for older adults requires effective articulation between compassionate workers and public health agencies.
Introduction
What does it mean to understand the experiences of health professionals who take care of older adults inside their homes? How can we understand these realities from health workers in a public health system? What does it mean to understand the perspectives of professionals from the Brazilian public health system? Do the professionals’ traditions and personal agencies reflect the realities of this work? Can we understand these realities by questioning the consensus of the professionals’ narratives? In any case, some situations beyond these questions require an analysis supported by different theoretical perspectives to construct a scientific understanding. These situations guide the development of this paper.
Health workers who perform home visits and in-home health care for dependent older adults face difficulties and stressful situation during their daily work. The situations these workers face must be analyzed to comprehend the realities of their work. Personal agency, territories of work, nature of agency-based caregiving, witnessing the sad environment and older individuals’ vulnerability, and the economic costs of mobility are some examples of these situations (Jackson et al., 2019; Marques & Bulgarelli, 2020; Ohta et al., 2020; Zoeckler, 2018). Thus, it is important to understand these workers’ realties to construct data and scientific knowledge that can guide new polices, new public agency strategies, and new attitudes to make this work less stressful. Because understanding and comprehending are relational processes (Schwandt, 1999), we were encouraged and motivated to present this paper.
Such understanding takes place in a relational dialogue reached through dialogical conversations surrounded by dialectical questioning (Gadamer, 1999; Schwandt, 1999). From an ontological perspective, Gergen (2009) highlighted that understanding is a process constructed together in our “relatedness” and affection with the “object/phenomenon.” Therefore, it is possible for researchers who are affected by this phenomenon to create an understanding of the health workers’ realities. Thus, we create and propose a unique way to analyze data within a hermeneutic-dialectic method to understand these realities. To create this possibility of analysis, we appropriate several concepts and assumptions related to Brazilian population aging, realities and traditions of public health agencies, and policies toward family health care. This analysis may be applied worldwide in other research with similar aims, approaches, participants, and phenomenon. We frame this work in terms of gathering hermeneutical, social, and dialectical perspectives.
This paper proposes our original inductive analysis that combines the researchers’ interpretations and insights with the theoretical perspective of philosophers Hans-Georg Gadamer and Bertell Ollman and the methodological support of sociologist Maria Cecilia Minayo. We collect these epistemological concepts and theoretical supports, within a hermeneutic-dialectical method, to propose a methodological way of analysis articulating the narratives, speeches, and emotions of health workers during their daily labor.
The aim of this paper is to share our unique scientific method of data analysis to understand specific realities within a hermeneutic-dialectical method. We aim to share the application of this method analysis by illustrating our research object and results.
Epistemological Background, Concepts, and Assumptions
In Brazil, the growth in the older population is characterized by high speed (Veras & Oliveira, 2016). The contingent of older people has increased from 4% in 1940 to 9% in 2000, and it is estimated that in 2050, 18% of the population will consist of aged people (IBGE, 2015). Such data corroborate projections by the World Health Organization (WHO), which estimates that in 2025, Brazil will be in the sixth position worldwide in the total number of senior citizens. In response, home health care for this population has received investments from a public health agency named the Unified Health System (the Portuguese acronym is SUS) to promote public health actions and services to provide care for this portion of the Brazilian population.
Brazil invests in the structuring of primary health care (PHC) services through the National Policy for Basic Care (NPBC), which brings paths for home care health assistance by means of the Family Health Strategy (FHS). This strategic work process is characterized by developing health care in health centers and at the homes of vulnerable people, such as dependent and bedridden older people. Brazilian policies regarding SUS traditionally and historically envision home care as a set of health services provided to individuals allowing them to live with dignity within the comfort of their homes (Yakerson, 2019). This is seen as a facility of SUS, which has domiciliary visits and in-home care as strategies to access vulnerable older adults (Heidemann et al., 2018). Regarding these strategies, teamwork articulation is important, and a team needs to move in the same direction toward a shared goal. This articulation happens among different professionals who discuss and collectively propose clinical treatments, preventive care, palliation, and home healing care (Heidemann et al., 2018).
The SUS in-home health services are organized by health professionals (physicians, nurses, dentists, and health technicians) who work together as an integrated team in a specify territory. Traditionally (Gadamer, 1999), this professional team develops monthly domiciliary visits to identify vulnerable older adults’ needs in a specific territory. The health assistance is developed inside the older person’s home by any kind of health treatment possible depending on technical limitation (Heidemann et al., 2018). The health professionals’ perspective regarding home health assistance can be understood through their discourses and practices. We wish to convey that the current practices and situations that a health professional develops and faces during their work, while visiting a vulnerable old person, can be expressed by speech and daily narratives. Their narratives bring up consensus that can be questioned to create divergencies that, when analyzed together as Minayo (2014) proposes, can create a rich comprehension of a research object.
There are different interfaces of home care in primary health care, which qualitatively and quantitatively address the perceptions of workers involved in this care, the network of services, and the social support. Discussion in the literature, from family health professionals’ perspectives, considers the importance of communication with the family and the service organization (Ohta et al., 2020). There are significant factors that influence this communication (Nieuwboer et al., 2018), including communication with the palliative care team. Professionals consider communication as an indispensable tool of patient care to promote palliative care for older people who are naturally getting close to the ends of their lives (C. G. D. Andrade et al., 2017). For the methodological analysis that we propose with this paper, the communication between researchers and workers is vital.
In addition to these aspects, home care is an instrument of the ontological organizational network of services, particularly for the older population, because it encompasses the use of different care technologies (Souza et al., 2018). However, there are gaps in the literature regarding methodologies that highlight the importance of views from professionals who develop domiciliary care for older people. What does it mean to work in this model of care from the workers’ viewpoint? How can we analyze this phenomenon? We believe that contemporary hermeneutics and dialectical perspectives can be used together to potentially answer these questions. We seek to analyze this viewpoint to support the comprehension of a worldwide phenomenon and its experience of truth (Abettan, 2017; Gadamer, 1999; Minayo, 2014). We believe that by encountering different perspectives from workers, we can respond to these questions and guide the construction of knowledge on methodological possibilities to fill this literature gaps.
Theoretical Perspectives to Support a Unique Way of Qualitative Data Analysis Within a Hermeneutics-Dialectical Method
The hermeneutics-dialectical method is a perfect scenario for creating different perspectives of analysis. It is possible because the flexibility of constructing consensus and at the same time discuss the consensus using dialectical questioning, reached in the participant narratives, is something that can enrich different kinds of qualitative data analysis (Minayo, 2002). The hermeneutics-dialectical method has guided several studies on research objects/phenomena including transformative thinking, harm reduction strategies, workers’ mental health, and male health (Khasri, 2020; Miranda et al., 2020; Tristão & Avellar, 2019). This method is the contemporary art of interpretation (Nava et al., 2018).
The scope for new way of analysis is possible from a hermeneutics-dialectical perspective. Therefore, we proposed a unique analysis combining philosophical orientations of Hans-Georg Gadamer, Bertell Ollman, and Maria Cecilia Minayo (Gadamer, 2018; Minayo, 2002; Ollman, 2003; Ollman & Smith, 2008). These viewpoints led us to construct an original way to analyze qualitative data within a hermeneutics-dialectical framework (Figure 1). This led us to design research using an inductive method based on these sociologists’ theoretical support, the participant’s narratives, and our insights (Freeman, 2007). We created this analysis orientation through different approaches such as those Minayo (2002) highlighted with the epistemological and teleological hermeneutics-dialectical process to design a methodological way to understand realities regarding health workers in the current world.

Analysis framework to understand the realities of home health care to older adults within a hermeneutic-dialectical method. Brazil, 2019.
Hans-Georg Gadamer was a modern German philosopher who brought the perspective of hermeneutics as one way to understand realities within the language in use. This hermeneutic philosophy is an art of interpretation grounded in the current language in use, while we are talking about health issues. This language exists in our societies surrounded by diverse traditions, dialogue, preconceptions, and social construction of consensus (Gadamer, 2018). Currently, the hermeneutics brought by Gadamer is considered a contemporary philosophical school in which a reality is always the result of an interpretation (Nava et al., 2018). Interpretation can be accomplished with the interaction between different voices, languages, preconceptions, and personal agencies articulating themselves to create a consensual opinion about something. This is the hermeneutical movement based on Gadamer’s dialogical model of interpretation. This means that comprehension of the consensus emerges from dialogue and conversation (Gadamer, 1999). This process was encompassed by the fusion of horizons regarding participants’ discourses of practices, emotions, and ways to cope with empirical work problems (Gadamer, 1999). This philosophical background teaches us how to understand consensus by listening to participants’ voices, identifying their preconceptions, and positioning ourselves as interpreters (Gadamer, 2018).
To enrich the possibility of analyzing health workers’ narratives and understanding their realities in depth, we considered the discursive perspective of Bertel Ollman, a North American contemporary sociologist who fosters understanding how social classes struggle to work in modern societies. His discursive dialectical perspective led us to comprehend the fact that an individual’s work makes the world have a sense and representation of classes have their social relevance. According to Ollman (2003), dialectics is a method of thinking about world reality in its scope of interactions. The concepts of representations of classes, in a Marxist perspective, led us to consider Ollman’s dialectic perspective to understand health worker labor in modern societies. This guided our analysis to question some consensuses that were first created by means of the hermeneutical philosophy once followed. Bertell Ollmann brings the complex Marxist theory into a dialectical way of understanding work as something that affects us internally in the process of constructing its social results (Ollman & Smith, 2008).
With these two different approaches, we followed Maria Cecilia Minayo’s framework. This Brazilian contemporary sociologist proposes a way to put hermeneutics and dialectics together to create a comprehension of the world with dialogical encounters. This sociologist states that there is a connection between consensus, dialectical questions, researchers’ insights, and interpretations regarding social class speeches (Minayo, 2014). These dialogical encounters happen between the researchers and theories while approaching the chosen theories to construct their interpretations, and between the researchers and the participants while developing interviews with them. The current literature presents the applicability of Minayo’s perspective to analyze phenomenon regarding SUS workers. Several issues are studied using this perspective, such as workers’ medication to avoid mental suffering, training of professionals to identify situations of violence, stigmatizing, and community health workers’ mental health (Campos et al., 2018; Egry et al., 2018; Fernandes et al., 2020). According to such theoretical orientations, we can create a way to analyze data grounded in methodological steps as follows.
We started the construction of our analytical process by means of a conversational perspective of analysis. Conversation about in-home heath care is a topic that spoke to us. Methodologically, such conversations emerged through qualitative interviews, which led us to identify similar and consensual opinions and point-of-views regarding the workers labor realities. This means that our interpreter’s voices suspended our prejudices and traditions and we created, initially, a hermeneutical agreement with the participants’ voices reflected in consensus/themes (Figure 1) (Gadamer, 1999; Vlăduţescu, 2018). While looking to the health workers’ speeches, we had in mind that they were representing their work class. In other words, the consensual themes emerged bringing the health worker classes’ speeches. In a second dialectical movement, we—the researchers—identified contradictions throughout questioning the professionals’ speeches, to identify the actual meaning of the consensuses. We created dialectical themes (Figure 1). This was a dialectical movement of comprehension as suggested by Minayo (2002). This dialectics perspective, represented in the movement of making questions regarding the consensus, allowed us to go beyond the speeches and understand how it relates to the labor context (Ollman, 2003).
The dialectical questions, presented in our analysis, were developed through intriguing situations identified during the dialogue regarding the research object. We identified questions/dialectical matters regarding work practices and coping with emotions and affections during the development of their daily work. It is important to point out that our participants were health workers from SUS, and they represent one class of Brazilian health workers. In this case, our participants represented the class of workers from a public health agency. In a final movement, we connected, by means of our insights and interpretation, the hermeneutical consensuses, and the dialectical themes to understand health workers’ realities. This means that we brought the dialogical encounter between our interpreter voices and the participant voices in a constructionist analysis (Minayo, 2014).
In summary, we believe this method of analysis within a hermeneutical-dialectical method can be applied to other research because worldwide health workers’ narratives are socially and collectively constructed though their daily work speeches. Talking to the health workers and analyzing their narratives under Gadamer, Olmann and Minayo’s theoretical support may be a possible methodological process to reach an understanding about their realities. Toward this, we focus on health workers from the Brazilian public health system, which is a very challenging scenario consisting of professionals engaged in developing good healthcare and assistance. We encourage the use of this analysis to understand any kind of health workers’ realities in their scenarios of practices.
Presenting the Applicability and the Findings in Terms of Illustrating This Unique Way of Analysis
We believe our method of analysis is unique, original and different from other qualitative analyses. It enables us to put together three different philosophers’ perspectives to analyze the realities of health workers. There is no methodology in the literature that presents a way to use dialogical encounters to reach a specific working-class consensus and at the same time question it under Bertell Ollman’s support. It is important to highlight that this method of analysis has some limitations. For example, it may be used to understand realities reported only by health workers. Even when it has a relational perspective, this method of analysis does not require participation from home health care patients. We understand that realities are “objects of the world” that can be understood with many discourses and traditions brought from a unique class, such as the worker class. Further studies with other methodology can examine other discourses such as the ways home health care patients understand home health care.
Even with some limitations, we believe that other scholars can engage with and use this method to analyze their data regarding workers’ narratives. There is no other perspective in the literature that puts together different philosophers’ perspectives to embrace comprehension of health worker classes within a hermeneutical-dialectical method. Scholars can use this method of analysis to understand other realities form different classes of health workers, seeking their contexts, personal agencies, and preconceptions and constructing a dialogical encounter with their own interpretation. This method of analysis can be applied to research studying health workers from hospitals, nursing homes, hospices and primary health care centers from public or private agencies.
The development of our analysis happened simultaneously with data production for research aiming to analyze home care for vulnerable older adults from the health workers’ perspectives. During the process of data production and the approach to the thoughts of the specific sociologists, we constructed trigger questions to develop narrative interviews, participant selection, dialogical encounters/interviews, data analysis, and data interpretation. Toward this, we collected/produced data through 12 semistructured narrative interviews with health professionals (physicians, dentists, and nurses) who worked in the SUS of Porto Alegre (RS). No worker refused to participate or dropped out of the interview. The interviewees’ schooling ranged from eight to twelve years of study, and their time spent working with PHC at SUS ranged from two and a half to six years. The average age was 29 years, and 16 (73%) were female. A female graduate student, the author of the present paper, interviewed the workers personally at health centers. We believe that a narrative is a hermeneutical and dialectical device to reach reality in terms of consensus and contradictions (Abettan, 2017; Gadamer, 1999; Ollman & Smith, 2008). The interviews, which were performed in private offices at the professionals’ workplace, were previously scheduled by phone with each professional according to their availability. This research was part of the interviewer’s thesis, and she has expertise with home oral health assistance and family practices. This means that the researcher is internally affected and has her own perspective about this kind of work, which is fundamental to the creation and development of an analysis within a hermeneutical-dialectical qualitative research (Gadamer, 1999; Ollman & Smith, 2008). We had an interest in giving voices to the health professionals and workers from SUS because we are advocates and enthusiasts of this service, and we identify ourselves with the importance of investigating this reality. None of the interviewees had prior information about the interview, which ensured no bias.
During the interviews, we followed a guiding script. This interview guide was created to include trigger questions to generate debates and discussion regarding the daily work routine, realities of in-home care practices, and questions to stimulate conversations about emotions and feelings. Some examples of trigger questions are as follows: “Do you consider home assistance something inserted in the municipality public health system network?” “Do you feel prepared as a physician, dentist, or nurse to provide home health assistance to vulnerable older adults?” and “What are the advantages and potentialities of home health services to older patients?” These questions had a hermeneutic and dialectic nature intended to seek consensual situations and possibilities of raising dissent. Reaching consensus, or dissensus in a discourse analysis, comprises hermeneutical and dialogical knowledge (Abettan, 2017; Gadamer, 1999; Minayo, 2014). The interviews’ audios were transcribed according to Atkinson and Heritage (1999), transcription norms, and all transcripts were returned to participants for comment and agreement during the analysis process. The results were returned to participants after the analysis process to validate and confirm the participants’ opinions. The duration average for each interview was 35 minutes.
Among the professionals who work in PHC developing domiciliary care, we chose participants who effectively performed primary care actions. The professionals had degrees in medicine, dentistry, or nursing and were not trainees. We used the snow-ball sample technique to form reference chains and perform saturation of participants and meaning saturation (Hennink et al., 2017; Marshall, 1996). During the process of interviewing, transcribing, and analyzing, the object of the study was always in our thoughts (Davidson, 2009). These sampling and meaning saturation procedures in qualitative research are grounded in studies by the World Health Organization and Maria Cecilia Minayo (Minayo, 2017; WHO, 1994).
We systematized the data according to content analysis from a thematic analysis perspective (Bardin, 2008), creating the aforementioned consensual themes. The interpretation and our inferences sought to approximate the hermeneutic-dialectic method (Gadamer, 1999; Minayo, 2014) and were also based on the literature regarding home assistance practices and PHC. Thus, the hermeneutic-dialectic approach is relevant for researching health professional practices (Collet & Wetzel, 1996; De Campos et al., 2012; Minayo, 2002).
After that, we started questioning the consensus that generated the trigger discussion in a dialectical movement of interpretation. Therefore, the analysis of the data was an articulation between our inferences within the support of hermeneutics and dialectics (Gadamer, 1999; Ollman & Smith, 2008). All of that composed our hermeneutical-dialectical method of analysis (Minayo, 2014) (Figure 1). This proposed analysis encompasses the fact that comprehending, in an ontological and epistemological perspective, is existential and happens between different voices and the interpreter/researcher’s efforts to make sense through the research object (Gadamer, 1999; Schwandt, 1999). In other words, the comprehending process can be constructed with the analysis regarding familiarity and strangeness, consensus and dissensus, dialogical and dialectical situations (Gadamer, 1999; Ollman & Smith, 2008; Schwandt, 1999; Minayo, 2014). This ontological process happens using actual dialogical encounters (Freeman, 2007; Gergen, 2009).
In summary, we constructed a hermeneutical consensus and then dialectically questioned it with our perspectives as health qualitative researchers. All these hermeneutic and dialectic movements, which we named referred to as a dialogical encounter, occurred through our insights regarding the health-workers-class narratives.
Even in a local basis and regional scenario, the present study brings a Brazilian social construction that is translated into signs to comprehend the meanings of in-home health services to older people from the perspectives of health professionals who work to the Brazilian public health system. We understand home care as any kind of health assistance and services that creates health promotion strategies, prevention and treatment of disease inside a person’s home. The interviewer for the present research is a health worker who developed home care; thus, the conversations happened with a common language, which means a dialogue in a mutual recognition of the aspects of home health care and assistance (Gadamer, 1999; Vlăduţescu, 2018).
We believe that there was no distinction among the three different health professionals interviewed (physician, nurse, and dentist) because we assume that all these professionals account for home assistance and are part of the Brazilian multiprofessional work team used to carry out activities in the territory under the care of a primary health care center. This means that they are immersed in the traditional practices of SUS and comprehend health care as a human right that is universal to all Brazilian people. This leads the workers to be responsible for the health of older individuals, and this fact internally affects their labor process. The workers need to be emotionally stronger to develop a good job to heal diseases and negotiate the best treatments along with the older person’s caregivers.
We created a possible comprehension of the research object, keeping in mind that these workers have their own accounts full of history, experiences, narratives, and opinions that are in the same language that Gadamer (1999) portrays as a dialogue. We believe that while performing the narrative interviews, we created a conversation with these professionals to bring a new sense to our topic of interest (Freeman, 2007; Gadamer, 1999). This “new sense” has a discordance of opinions and perceptions that are fundamental to our understanding (Minayo, 2014). The dialectic concept used to comprehend their realities is assigned as a positive value (Ollman & Smith, 2008). It helps the team to discuss and construct good praxis regarding taking care of an older adult.
We created themes, which we named as “thematic movements of comprehension,” regarding hermeneutical dialogical encounters and dialectical questioning. This means that we used content analysis to create them by regarding our state of being and the acting and diverse perspectives from the research participants. Ideologies and critiques of the health system, as well as the process of working with resource constraints in SUS, appear in the narratives and are perceptible as dialectical questioning processes to express opinions. All these manifestations pervade the interpretative movements.
The thematic movements of comprehension permeate situations such as the actual sad situation of some territories, creating possibilities of home health care, the integrality of attention as a perspective for providing home assistance in the primary care field, and the necessity of a net of services to provide an organizational routine of home visits to older people (Figure 2).
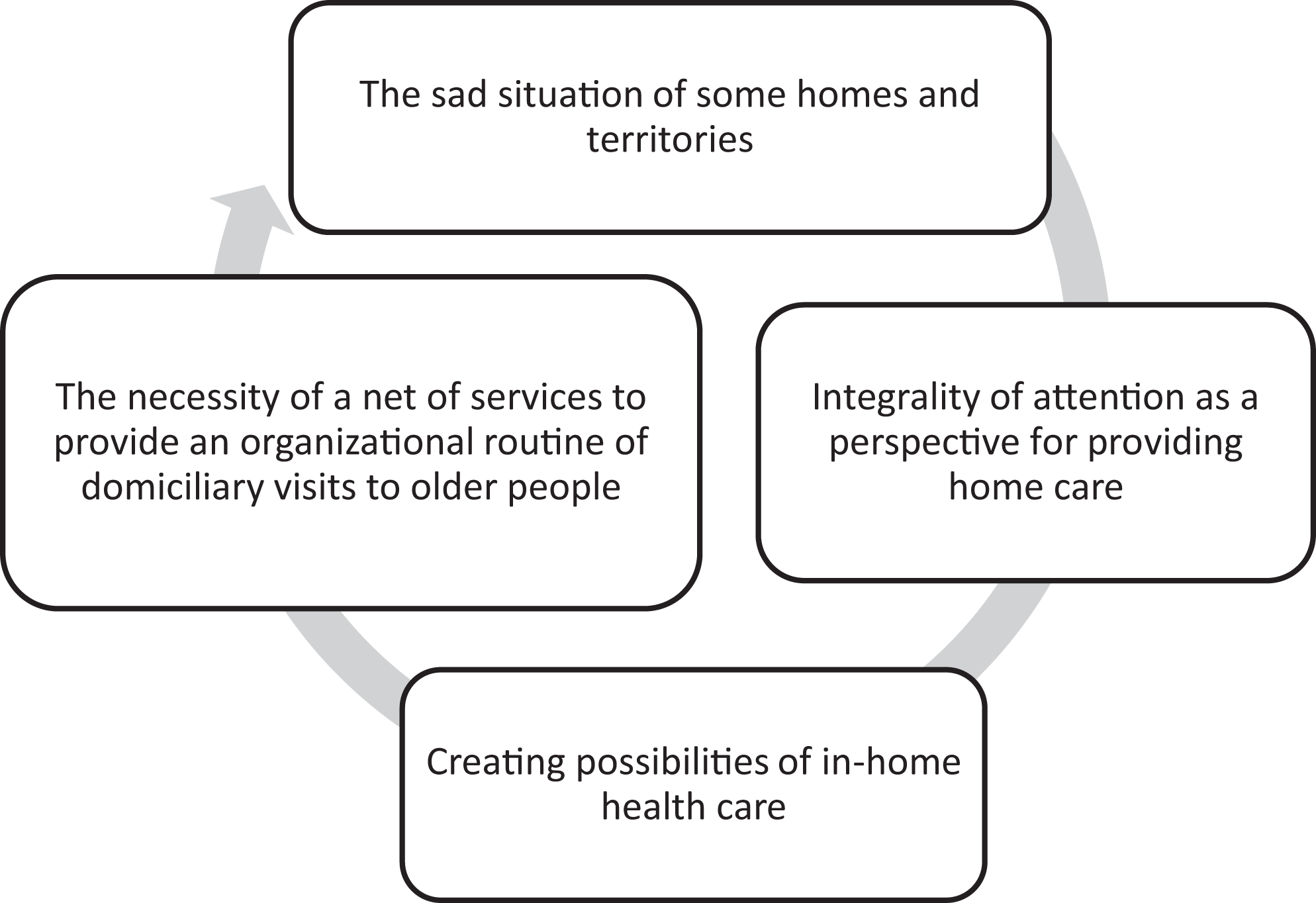
Thematic movements of comprehension to understand the realities of home health care to older adults within a hermeneutic-dialectical method. Brazil, 2019.
To illustrate our findings, we present these consensual and dialectical themes and discuss them by means of a narrative text, with some excerpts from the narratives articulating them with regard to our interpretation in order to construct an environment of hermeneutical-dialectical reading to comprise the study’s aim. We considered the workers’ backgrounds through their reports of practices, knowledge, professional experiences, and personal agency. We had a perception of dedication and valuation of home care practices and services in their territory of agency. For Gadamer (1999), histories and experiences are important in the process of understanding something that we experience and provide consensus. Thus, health professionals daily face the reality of their territory, which requires accurate knowledge of the service assignments and their management, in addition to linking their actions to housing conditions and the population’s dignity (Brasil, 1994; Ward et al., 2018).
The worker who provides home health assistance, who circulates in a specific territory, and who has an academic background in public health, seeks to interconnect information brought by Brazilian public health system user while also keeping a critical eye on the situation of the older person who needs health care and assistance at his/her home. These workers are empowered with this capacity to look critically and negotiate actions within the reality of the vulnerable person such as a care person-nurse interaction (Spiers, 2012). During the domiciliary visit, the workers will inevitably judge the elements that can make their work difficult or promote health inside the residence. This judgment is full of preconceptions (Gadamer, 1999) regarding their private values on what is a good ambiance to promote health. This private judgment needs to be negotiated with their actual possibilities of care. We can see that professionals will narrate based on his/her awareness that some aspects, such as observation and critical observation, should be considered as a work strategy in the context of health care for older people. At the same time, some workers do not even try to negotiate or construct a good home ambiance to promote health for the older person. Why does this happen? Dialectally, it seems that the position that they occupy at the SUS is perceived as an ordinary job. They do not recognize the potentiality of their actions and there is no recognition of his or her workforce. We observe the house, the family, how they relate to each other, the hygiene conditions, the housing conditions, the type of care, whether there is anything that indicates violence, mistreatment. If the person is living a worthy life, you know…So…you can see everything…You can have a good notion…Because we are also trained to take a look, you know(.). We don’t go there only for the sake of the patient; so many times we want to know how he lives, who is living with him, people’s behavior, interpersonal relations, all the conditions. (interviewee 3, female, nurse) Hum…To take a bath…Ok…In this case, you go to that patient’s house and there is no shower head, they don’t have it, you know…So, you must promote health according to that reality, you know…and we bought a shower with the community’s support…(Interviewee 12, female, Dentist) Because of some difficulties we can’t see, because:…we don’t know the person’s environment without stepping inside their home…But I do not change anything. I do my job. (Interviewee 01, female, Nurse)
Healthcare should be understood in a multifactorial context, requiring adaptation to different realities. The optimization of resources inside a vulnerable older person’s residence should be negotiated with the caregiver. It is distressful, but we observed that optimized situations are often developed. This is based on the residence reality that one can address the main way of providing care to the older person within his social environment. The contexts of developing home health care generate distressful conditions for these professionals. In this aspect, consensual anguish is perceived by these professionals’ perspectives while they dialogue with themselves about it and use a plural language showing their social agency and the sad situations that they face. I think that, potentially, this thing of really knowing the older adult surroundings and daily routines…we have a lot of older people here, in our small area/territory of responsibility…older people who are restricted to their residence, not because they can’t walk or have a caregiver, but due to the geographic barriers to leaving their home. So, we have to work on the potential of that environment, their houses…to bring satisfaction to their lives. (Interviewee 10, male, physician).
Do these workers comprehend what the integrality of care is? Historically, the professionals participating in the present research experienced a public health system whose doctrinal principle was the integrality of attention, that is, the integration of services and different health professionals working together to take care of a single case. Therefore, this historically and traditionally constructed integrality is part of these professionals’ agency, which is rooted in preconceived (Gadamer, 1999) positive perceptions of domiciliary care. This integrality of health care services, including the domiciliary visits to home care, is based on a political democracy that leads these professionals to participate in the dialectical thinking of their working process (Ollman & Smith, 2008). This means that teamwork, as a workforce tool used to deliver home care, was dialectically constructed during decades of struggle by Brazilian health professionals and politicians.
We identified situations where the performance of integrality of care occurred with the protagonism of some professionals, who, while being questioned about their actions in someone’s home care, were eager to report successful cases involving the older adult care at home. As explained by Gadamer (1999), motivation is essential, and it was reported in some speeches: We even had a moment to discuss the case inside the health center, which made me go to the protective service in person for them to take measures, you know…because it was no longer a health issue, but rather a principle of social assistance; so, we…there is a good partnership with a good level of case solution. (Interviewee 7, women, Nurse)
Thus, understanding care integrality and worker interaction is intricately linked to the daily challenges to performing home assistance in the territory (Minayo, 2014; Peduzzi, 2001). Protagonism by some health professionals is necessary to effectively act within the residence. Moreover, the dialectic nature is observed in reports in the different demands of care provided in this environment, which needs effective flow through the net of services in health care. Such flow originates from a perspective of teamwork, specifically combined with theoretical and political assumptions that guide practices of teamwork (Ollman & Smith, 2008).
Teamwork in in-home health care can be understood from the perspective of integration, compliance, and reciprocal communication between specialized works (J. F. Dias et al., 2017; Peduzzi, 2001; Savassi, 2016; Vivian & Wilcox, 2000) and requires an established service flow to make workers’ actions effective. The consensus emerges that home care, from these workers’ viewpoints, does not effectively occur as it could and should: I think that we could be much more involved than we are, you know…we end up staying too long inside the office due to the high demand. Currently, in this territory we don’t provide services to this office alone; so, in addition to this health center, we have other health centers to support…it is too much work. (Interviewee 6, male, Nurse)
Aligned with the understanding that home assistance occurs in a context where different social actors interact, we can observe that the potentials of this type of care can be understood as including more than biomedical service (Merhy, 2020). Approaching the hermeneutic-dialectic perspective (Gadamer, 1999; Minayo, 2014), we can observe the report of a professional awareness that it is possible to understand parts of the older person’s life from a home visit. That is close to what Floriani and Schramm (2004) described, thereby also evidencing the possibilities that may arise in actions to promote health based on older adults’ groups. Moreover, there are situations of professional development, chiefly involving overload of tasks in this flow of services, and societal underestimations. The workers need to be supported through their agencies (Tsui et al., 2018) or public health systems. There is a consensus, and some dissensus, because they make it explicit that it is not possible to fully comply with PHC protocols and manuals because life is shaped according to the demand and population characteristics of each territory. The professionals work hard to develop good home care, and the public health systems should improve support for them. This support is a dynamic human process with different opinions regarding their occurrence.
Final Considerations
The possibility of associating the philosophical hermeneutics, pointing out the understanding of the social consensus from a class of health workers, and at the same time associating this with dialectical perspective regarding questioning the reality, dissension and contradictions enabled us to understand different perspectives from health workers and their practices. We believe that the methodological approach that we brought to this qualitative and interpretive possibility was something sustainable that reached the proposed aim of understanding something socially and collectively constructed. We believe that questioning consensus regarding health work issues in modern societies provides more revealing results than traditional thematic analysis. This happens because consensus/themes can show only “pictured and immutable reality,” whereas by using a dialectic approach to question this reality, we can still create dissensus interpretations regarding a reality that is constantly in movement.
Illustrating the use of our analysis uncovered different realities regarding home assistance and care to older people faced in the daily routine of the Brazilian public health service. This revealed contexts that generate distress for the studied working class. Within the consensus and few dissents from the professionals’ perceptions and our interpretation, we can conclude that articulation between the territory reality and the real possibilities of care in a residence are essential to be acquainted. Furthermore, the integrality of care to a vulnerable older adult is fundamental to make in-home care effective in primary care, as well as the need for a “flowing service” that permits the organizational routine of home visits. The process of constructing health care includes, among other aspects, compassionate care. We understand that compassionate care is essential to the professional working for SUS. Considering these assumptions as strategic actions of care, the methodological analysis and the results of this unique analysis will probably contribute to create a perspective directed to the difficulties and potentials faced by public health practitioners.
Finally, this paper shares a description and an understanding of the original method of analysis that we created. We believe that others can engage in the same analysis when studying other “socially and collectively constructed” objects regarding health workers’ perspectives.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
The present research protocol was approved by the Committee for Ethics in Research (CEP) of Universidade Federal do Rio Grande do Sul/UFRGS (Federal University of Rio Grande do Sul) (Protocol number 1.990.925). Each participant had signed the informed consent before participation in the semi structured narrative interview.
Any underlying research materials related to this paper can be accessed contacting the corresponding author by email.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was funded and financially supported by Fundação de Amparo à Pesquisa do Estado do Rio Grande do Sul/FAPERGS (Foundation for Research Support of the State of Rio Grande do Sul), under protocol Alexandre Favero Bulgarelli: ![]() .
.