
Abstract
The voices of people living with dementia are rarely included in primary data collection due to cognitive challenges and the concerns of researchers and others about limitations associated with informed consent. This article presents a successfully implemented, step-by-step process enabling effective participation of aged care residents with dementia using a case study approach. Three methodological and critical steps in data collection were identified that led to the successful participation of residents with dementia in research. The process corresponds with, yet is uniquely different from the common elements in the qualitative research process. These are active participation during data collection, researcher familiarization with participants, and their set interval and time-lapse considerations (timeline). The process of involvement of people with dementia in research should proceed at a pace that is guided by the participants. It is important to consider participant interview pace, pattern, and the conversation time points when interruptions occur, to restart the whole interview process. Researchers need to facilitate active engagement by building and maintaining authentic relationships with the participants.
Keywords
Introduction
There is an increase in the number of people living with dementia, related to population ageing, leading to the need for increased research in relation to matters affecting the wellbeing of older adults who are living with dementia. Dementia is an umbrella term for a neurological syndrome resulting from one of several disorders, with Alzheimer’s disease being the most common. Dementia is “defined as global cognitive impairment that is irreversible and occurs in a clear sensorium” (Blass, 2003, p. 1391). The term “global cognitive impairment” refers to “impairment in memory and at least two other cognitive domains” (Blass, 2003, p. 1391). The impact on the person who has dementia is reduced life expectancy and quality of life. Eventually, they are no longer able to live independently (Alzheimer’s New Zealand, 2017).
The two peak international advocacy organizations, Dementia Action Alliance and Alzheimer’s Disease International, have called for strengthened investment in dementia research with an emphasis not only on finding a cure but identifying innovative models of care. Concurrently, there is increasing recognition of the human rights of people who are living with dementia as people with disabilities (Dementia Alliance International, 2016; World Health Organization, 2016).
The importance of consulting people with dementia on matters concerning them is central to the need for a rights-based approach when researching groups who have the potential to be marginalized. Including people with dementia as participants when the research concerns matters relevant to their lives aligns with an approach that is respectful of their ongoing citizenship (Dementia Alliance International, 2016). However, there are barriers to the inclusion of people who are living with dementia in the research process (Brooks et al., 2017). Human research ethics committees rightly have a focus on ensuring the protection of vulnerable potential participants. Furthermore, the extent of engagement and involvement of people with dementia as participants are challenging to explore due to the progressive nature of the condition and legal implications concerning the decisions to participate. There must be a balance between potential harmful outcomes and the benefits of participation for people with dementia. Safe research practices achieve that balance, while protecting participant wellbeing (Novek and Wilkinson, 2019.
Challenges to participation in research for people who have dementia come from ethics committees, family members and carers, and researchers. Human research ethics committees are concerned with ensuring that research participants can consent to their participation (Ministry of Health, 2014). Gatekeepers such as family members or care staff may decide that particular people are unable to participate in research (Brooks et al., 2017; McKeown et al., 2010). Additionally, sensitive use of data collection methods is required to foster the participation of people with dementia (Brooks et al., 2017; Hellström et al., 2007).
Consequently, challenges in capturing the views of people with dementia and concerns about their ability to contribute to research meaningfully have meant there is limited research that directly involves them as participants. However, this situation is evolving, and researchers are exploring ways of including the voices of people with dementia as an appropriate and valued data source (Beattie et al., 2019; Brooks et al., 2017; Cridland et al., 2016; Rivett, 2017; van Baalen et al., 2011). This article adds to the growing body of knowledge about researching with participants who have dementia.
We aim to report on the methods used to enable the participation of the residents of a traditional Aged Residential Care (ARC) facility in research using case study methodology to explain their move to a new purpose-built village. The new purpose-built village is designed to facilitate resident continuation of lifelong identity by supporting maximization of remaining abilities enabling engagement in valued activities. The study aimed to explain the process and the outcomes of the transition of Whare Aroha CARE residents to The CARE Village Te Manaaki a Tura. Because the desired outcome of the transition was to improve resident subjective quality of life, the explanation would have been incomplete without the views of the residents whose lives were affected
Theoretical Perspective and Methodological Overview
Consistent with the explanatory aim of the research, the study was guided by a critical realist theoretical perspective. Critical realism recognizes a stratified ontology, positioning researchers to identify mechanisms operating below the surface of events, generating phenomena of interest in society (Bhaskar, 1975). Critical realism is therefore a useful perspective for researchers investigating social settings were taken for granted assumptions may hinder beneficial change (Sayer, 2000).
The study described in this article sought to explain the transition to an innovative model of care in ARC, a setting where change was required to enable enhancement of resident wellbeing through greater participation in usual daily life than was possible in the traditional facility. In ARC facilities based on the traditional model of care, the physical environment resembles a hospital rather than a home, and resident daily life revolves around facility routines designed to meet their medical and personal care needs (Adams et al., 2017). The new facility is based on a holistic, biopsychosocial model of care, including care for psychological and social needs as well as health care (Ostaszkiewicz et al., 2018). Participating in usual daily life in The CARE Village Te Manaaki a Tura means residents are supported by staff to pursue valued social, hobby, and household activities according to their desires.
Research utilizing a critical realist theoretical perspective is guided by theory, aligning with the need for beginning theoretical propositions in case study research. Case study is a flexible approach, can be used as a methodology or method, and is useful for developing descriptions or explanations of bounded phenomena in context (Luck et al., 2006). Consistent with the recommendation of Yin, (2017), the case study began with two theoretical propositions. The first beginning theoretical proposition, relevant to this article, was that the transition to a facility featuring familiar domestic scale environments would result in respect for the individuality of residents and a fostering of social engagement (Shannon, 2021). The proposition draws from the Hogeweyk care concept, the inspiration for the development of the new facility. De Hogeweyk is an ARC facility in the Netherlands, where residents with dementia live in an environment resembling a Dutch village and are supported by staff and volunteers to continue living life “as usual” (van Amerongen- Heijer, 2015, p. 1).
Background to the Study
In September 2017 residents of Whare Aroha CARE in Rotorua, New Zealand moved to The CARE Village Te Manaaki a Tura. While precipitated by the end of the lease on their existing premises, the purpose of the move was to facilitate supported participation in usual daily life for residents within a secure village where people live in small households in lifestyle groups of six or seven residents. Whare Aroha CARE was contracted by the local District Health Board to provide residential care to older people who required low-level (rest home) care, high level (private hospital) care and specialist (secure) dementia services.
Older people who can no longer live independently may move to ARC following a formal assessment of their care needs. They may require low-level care, encompassing support with health and activities of daily living such as personal hygiene, those with more complex health and mobility needs will require high level care, while specialist dementia services is a subset of low-level care for people who have dementia care needs requiring a secure environment (Ministry of Health, 2019).
Housing residents with differing care needs separately is the norm in New Zealand ARC facilities (Ministry of Health, 2019). In The CARE Village Te Manaaki a Tura, a mixed services model of care has been developed with the support of the District Health Board and the Ministry of Health. In a mixed services model of care, residents who require different levels of service can live in the same part of a facility. For example, in the facility described in this article, residents who require hospital (high) level care, rest home (low) level care and specialist dementia care are all housed together. Therefore, the mixed services delivery model enables people to live in small households with peers who have shared a similar lifestyle, rather than with those who require the same level of care. In The CARE Village Te Manaaki a Tura residents who previously required segregated secure accommodation are integrated into the village community, enabled by technology.
Participants
Demographic Characteristics of the Resident Participants.

Active Participation
There is a tension between enabling ARC residents with dementia to have their voices heard in research and the risk of inadvertent coercion. The power differential between staff, who have the most power, and residents, who have the least power, in institutional settings has been described by Goffman (1968) and others subsequently (Bridges et al., 2020; Johansson et al., 2020). When inviting people with dementia, particularly those who are residing in institutional settings, to participate in research, researchers must be cognizant of that power differential. Deep familiarity with and enculturation in ARC environments through long-term employment in them, as described by Bourdieu (2007), may hinder recognition of institutional power imbalances.
Consequently, careful consideration was given to the powerlessness of facility residents in relation to staff members when planning recruitment for the study. A member of the facility management team identified potential resident participants, and the receptionist at Whare Aroha CARE, a staff member with a low level of power in the organization, invited them to participate in the study.
Those participants who had a legally appointed power of attorney for decision-making were deemed to be unable to decide to participate independently. Next-of-kin provided decision-making support for those residents. While people with dementia can be unable to provide informed consent for research participation as their dementia progresses, they retain the ability to appoint a trusted proxy decision-maker such as a family member (Kim et al., 2011). Seven of the resident participants required support with decision-making, and four were able to decide to participate independently. They, or their family member if they required support with decision-making, were initially given an invitation introducing the research and the researcher. If they indicated they would be interested in participating, the receptionist provided them with a Participant Information Sheet.
Consistent with New Zealand legislation, for those who required decision-making support, the first author obtained assent, defined as “affirmative agreement to participate,” from the participant (Health and Disability Ethics Committees, 2020, p. 1). Additionally, written informed consent was obtained from their next-of-kin for their participation in the study. Family member consent was based on their belief that the person’s participation was in their best interests following Right 7 (4) of the Code of Health and Disability Services Consumers’ Rights (Health and Commissioner, 2016). In the case of the current research, best interests were defined as being offered the opportunity to express their views about their living situation.
Each participant was provided with a study information sheet, in a readable format, with simplified language and relevant images. A readable document contains language at a level the reader can comprehend, enabling them to make an informed choice about their participation (Foe & Larson, 2016). The researcher also discussed the project with participants, clarifying their understanding and beginning the relationship-building process. Dewing (2007) recommends building relationships between the researcher and research participants who are living with dementia before collecting interview data. McKillop (2002) stresses the importance of the researcher being genuine with participants, and McKeown et al. (2010) recommend that the researcher has experience in interacting with people who have dementia.
Researcher Familiarization
The first author has extensive experience working with people who have dementia. The first author’s experience has been gained over more than three decades in clinical practice as a nurse in acute and long-term care settings with older adults, including those with dementia. Additionally, her Master of Nursing (Research) project investigated nursing care of people with dementia. During data collection for the current project, she spent approximately 4 days a week for 10 weeks at Whare Aroha CARE and The CARE Village Te Manaaki a Tura during the data collection phases of the project, enabling participants to become very familiar with her presence. Having built a relationship with research participants, the researcher ensured ongoing consent by regularly checking with participants, consistent with process consent as described by Dewing (2007).
The first author collected data with resident participants at two time points. Before residents moved from Whare Aroha CARE data were collected with them, and again at least 4 months after they had moved to the new facility, The CARE Village Te Manaaki a Tura. Data collection with resident participants was via individual audio-recorded interviews that were subsequently transcribed and via observation of daily activities using an observation tool developed by the first author. Participants consented to the recording of the interviews. 10 resident participants were interviewed before the transition; while one declined to participate in an interview at that time but consented to an interview after the transition, having become familiar with the researcher during observation.
To guide observations and ensure consistency, the first author developed an observation protocol (Supplementary Appendix 1), drawing from Dementia Care Mapping. Dementia Care Mapping is a validated tool that is used to evaluate the care of people with dementia (Bradford Dementia Group, 1997). The basic structure of the tool, guiding frequency and duration of observations was used. However, consistent with the purpose of the study, the prompts to observe for care were replaced with prompts to observe for a normalized environment and resident participation in daily life, encouragement to maximize remaining abilities, social and other pleasurable activities.
During the time between the first and second phases of data collection, one resident participant died, and two others transferred to other ARC facilities to be nearer to family members. One participant moved because their family member had relocated to another town, and the other participant moved because they were the widow of the resident participant who had died. Their remaining family lived in another town.
It is recommended that researchers remind participants with dementia what the study is about at the start of each instance of data collection and intervals during the data collection process (Cridland et al., 2016). Reminders were particularly important during the study being reported in this article because data were collected in two different ways at two time points. Additionally, observations of resident daily life took place in four time blocks each day for 2 days, before and after the transition. At the beginning of each interaction, the researcher reminded participants of her identity, affiliation, the purpose of the interaction and the name of the family member who had assisted with consent to participate before checking ongoing consent.
Participants were offered the option of a standard interview or a walking interview, where the researcher accompanied the participant during their usual activities. One participant who liked to walk chose this option. Collecting data in different ways supported participation for people who found it challenging to fully express themselves verbally, as illustrated by the quote, below from participant 25. I can’t think of anything when I want to say something, that’s the problem, you know what I mean. Participant 25.
An additional benefit was that an interview could take place after the participant had become comfortable with the researcher due to the extended amount of time spent together during the observation of daily life. Because some resident participants took several minutes to formulate their answers before speaking, the researcher learnt to wait for the answers, rather than assuming the person did not have anything to say. While the participant was engaged in thinking during that time, the researcher was waiting and initially found it challenging to adapt to waiting what seemed like a long time. Reflecting on the difference between a social conversation and a conversation for the purpose of research, and the extra challenge that poses for a person who has dementia facilitated the researcher’s adaptation.
Additionally, the familiarity between participants and the researcher contributed to the ability of residents to guide data collection in ways that suited them. For example, in addition to choosing not to be interviewed until they were comfortable with the researcher, as one participant did, participants chose to discuss their preferred activities such as craft, creative writing and household tasks such as cooking and laundering clothes, while the researcher was observing them. Of those activities, craft and creative writing occurred in both settings, while participating in household tasks, was only observed in the new small-scale, inclusive facility.
In line with other research, feedback to participants was an integral part of the study. Participants were provided with regular informal feedback about the impact of their participation, for example, regarding the progress of the study and study outputs, such as conference contributions. Consistent with the experiences of previous authors, participants valued the opportunity to continue to contribute to the society that their participation afforded, including knowing that their experiences would be shared with others (Cridland et al., 2016). Study participants have been provided with a summary of the study results, written in an accessible format, using language that is easily readable.
The summary was sent individually to participants, and the contents of the summary were discussed at a presentation given by the first author that participants were invited to. Resident participants who did not attend the presentation were individually visited by the first author who discussed the results of the study with them. All participants appreciated being provided choice and confirmed that the results presented to them resonated with their experiences. The process of enabling research participation for people with dementia is illustrated in Figure 1, below. The process of enabling research participation for people with dementia.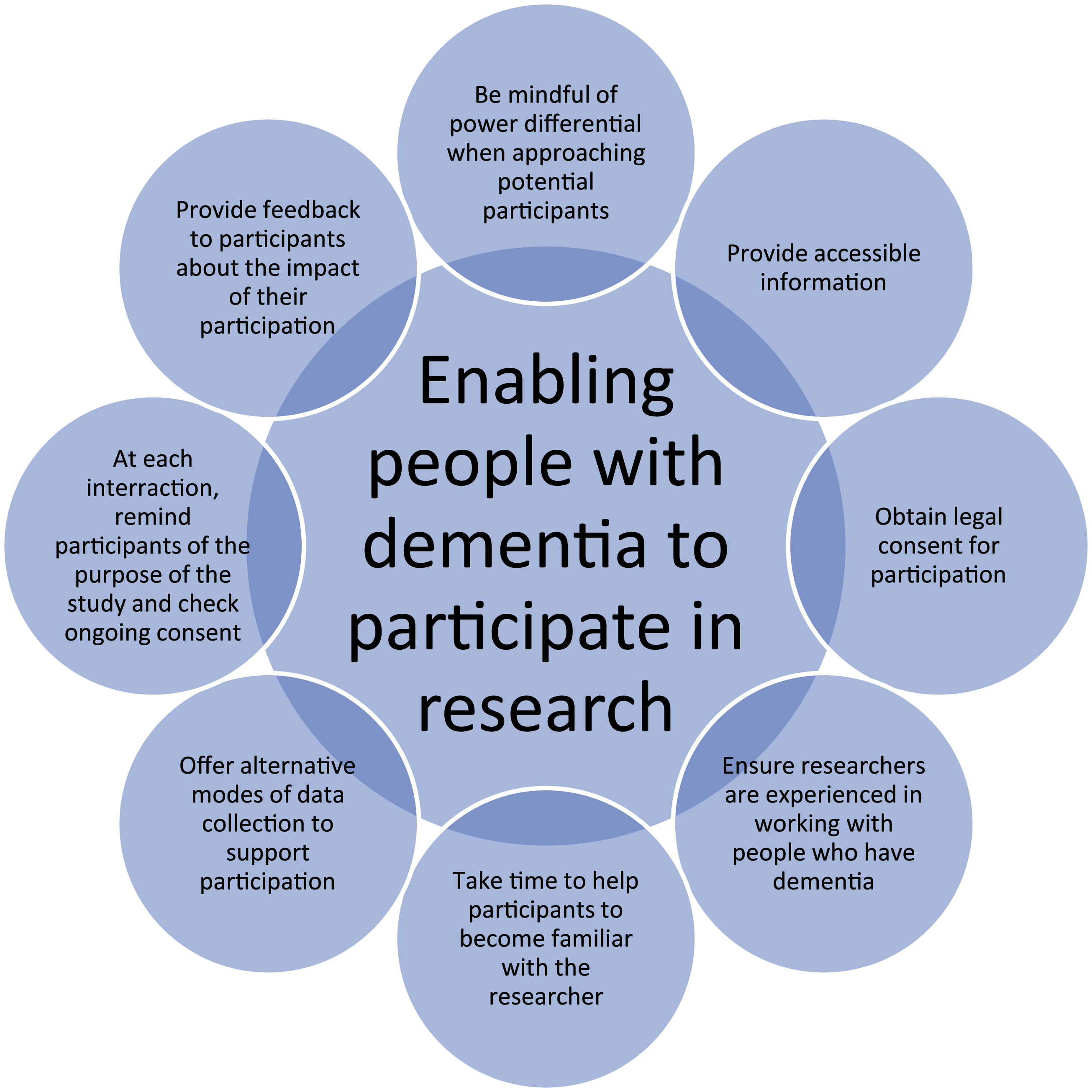
Data Management and Analysis
Consistent with the critical realist theoretical perspective that guided the study, the procedures recommended by Miles et al., (2014) and Danermark et al., (2019) were utilized to analyze the study data. Additionally, NVivo 11 (QSR, 2016) computer-assisted qualitative data analysis system (CAQDAS) enabled management of the large amount of study data and facilitated the development of codes and subsequently themes. Initially deductively derived codes were developed from the beginning theoretical propositions for the study, as recommended by Danermark et al., 2019, progressing to the development of inductively derived codes, including in-vivo coding that included the words of the study participants, and process coding, codes named with gerunds, indicating actions, as recommended by Miles et al., (2014). Codes were operationally defined, to ensure consistency of coding. During second-cycle coding, themes were developed by grouping similar codes together. An event listing matrix was used to display data relevant to events in the transition in chronological order, assisting clear understanding of the events occurring in the transition, consistent with Miles et al., (2014).
Extant theory was used during the retroductive process described by Danermark et al., (2019) to identify the unseen mechanisms, acting to generate the phenomena of interest relevant to the study. Therefore, an explanation of the process and outcomes of the transition was developed, consistent with the aim of the study. This article is concerned with the research participation of ARC facility residents who have dementia, the study results will be reported elsewhere.
Ethical Considerations
Approval to conduct the study was obtained from the national Health and Disability Ethics Committee (approval number 16/NTA/133) and from the Auckland University of Technology Ethics Committee (approval number 16/424). In addition, a locality agreement was signed between the study sites for the research and the researcher, ensuring site specific matters relevant to research governance were addressed.
Insights Gained
Article 19 of the United Nations General Assembly (1948) universal declaration of human rights enshrines the human right to hold opinions and have freedom of expression. The increasing prevalence of dementia, together with the growing demands of people with dementia to be consulted about things that concern them highlight the growing importance of respecting the human rights of people who have dementia. Researchers must be cognizant of the means of promoting inclusivity in research for people who have dementia.
The use of different methods of data collection with resident participants has facilitated their inclusion in the research described in this article. In particular, spending time with residents during the observation of their daily lives has positively contributed to building the relationships that enable people with dementia to feel comfortable during research interviews. For example, one participant did not consent to an interview before the transition but was comfortable with the researcher after the transition and agreed to be interviewed. This was a result of the researcher and the participant spending time together building familiarity and trust.
Based on the experience gained during the study, we recommend including the use of observational methods during data collection with people who have dementia, to positively augment other traditional data collection methods such as interviews. The time spent with participants during observations enables them to be familiar with researchers and to feel at ease during subsequent interviews. In the study described in this article, the participants with dementia have contributed to the knowledge base about the process and outcomes of moving from a traditional to an innovative model of care in ARC. Additionally, they have contributed valuable knowledge about how to enable people with dementia to participate in research meaningfully. The first author reminded them of their contributions at the times data were collected and during meetings to inform them of the study results.
The step-by-step process utilized in the data collection and recruitment of residents with dementia as research participants includes the fundamental elements of collecting data in any research project. However, what is unique in this experience is the strengthened approach to data collection methods, which enables individuals living with dementia to guide the process. The researcher had to consider the context of participation in the light of being able to observe participants during and after interviews. Interviews and observations of daily life are resident-guided, with consideration of their own space and time, and providing the opportunity to stop and resume the interview. Researcher familiarity with the residents with dementia within their environment, which in some studies described as the “insider” or the “emic” (Hoare et al., 2013; Simmons, 2007), were reflected in this process. The processes described in this paper reflect the understanding that the researcher’s knowledge about the resident is limited, variable and will take time to consolidate.
Strengths and Limitations
The current data collection method, which enabled successful research participation of residents with dementia is possible in traditional ARC settings and care settings based on a clustered domestic model of care such as The CARE Village Te Manaaki a Tura. In care settings, using a clustered domestic model of care, the physical environment is small-scale, home-like, and staff and residents contribute to the running of the household (Afendulis et al., 2016). The step-by-step process utilized in this study offered residents greater opportunity to guide data collection in such settings. Moreover, the data collection process supports the efforts of enabling participation of people living with dementia in research, where appropriate language use and avoiding participant distress are considered key principles (Novek & Wilkinson, 2019). The model allowed people living with dementia the opportunities to participate in valued activities in that setting and facilitated research participation. Contrastingly, when participants were living in the traditional ARC setting, their opportunity to participate in valued activities was limited, impacting on their ability to guide data collection in that setting. Despite this limitation, it should be noted that the method has a unique strength, being resident-guided, distinguishing it from researcher-led traditional research methods in data collection.
Conclusion
The process undertaken in this study is illustrative of the slogan “Nihil de nobis, sine nobis” [“nothing about us without us”], where inclusive and active participation of stakeholders and participants in research is needed, particularly on topics that have policy and health service delivery implications. This article reported the methods used to include people who have dementia and who live in an ARC facility in research about the transition to a new purpose-built facility inspired by de Hogeweyk village. The study offered insights into the process and outcome of the transition from Whare Aroha CARE to The CARE Village Te Manaaki a Tura that would not have been complete without the views of the residents, who were affected by the transition. The research processes aimed at the active participation of people who have dementia, who guided data collection in terms of the extent of participation, familiarization, and timeliness. These processes were proven to be doable as utilized in this study. The researcher’s role is to facilitate these steps in any research with people who have dementia. While this paper reports on a study that was conducted in New Zealand, the methods used to seek the views of ARC facility residents who have dementia will be of interest to an international audience of researchers.
Supplemental Material
sj-pdf-1-ijq-10.1177_16094069211055938 – Supplemental Material for Nothing About us Without us: Research Methods Enabling Participation for Aged Care Residents Who Have Dementia
Supplemental Material, sj-pdf-1-ijq-10.1177_16094069211055938 for Nothing About us Without us: Research Methods Enabling Participation for Aged Care Residents Who Have Dementia by Kay Shannon, Jed Montayre and Stephen Neville in International Journal of Qualitative Methods
Footnotes
Acknowledgments
The research was supervised by the third author and Professor Valerie Wright-St Clair.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research for this article: This work was supported by the Hope Foundation for Research on Ageing scholarship awarded to Dr Kay Shannon in 2017, 2018, and 2019.
Supplementary Material
Supplementary material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.