
Abstract
Community-based participatory research (CBPR) and interpretive phenomenology, when merged, can provide insight into the experiences of a homogenous community. The purpose of this manuscript is 2-fold. First, we aim to provide a conceptual view of merging methodological approaches of phenomenology and CBPR. Principles of interpretive phenomenology, the philosophical stance, and the qualitative analysis methodology, as well as how interpretive phenomenology is complementary to CBPR, are reviewed. Second, the utility, rationale, and feasibility of merging these diverse approaches are explored. For illustrative purposes, exemplars from a Parkinson’s disease stakeholder study are used to discuss aims, methods, and results. Focus group data collection strategies and the use of Template Analysis as an analytic tool are also described. Themes that materialized from the data focused on support group experiences for this rural community. In keeping with interpretive phenomenology, the researchers’ interpretation of these themes led to the understanding of an overall essence, or essential theme, of this community’s lived experiences.
Keywords
Interpretive phenomenology and community-based participatory research (CBPR) are often viewed as originating from different paradigms and not suited to be connected in an analytic approach. However, merging interpretive phenomenology and CBPR can provide an in-depth view of a community’s experiences. An exemplar study that will be reviewed herein merged interpretive phenomenology and CBPR approaches using focus group data collection and Template Analysis. This study revealed an unexpected community perspective, resulting from the remarkable consensus of the community members who participated. In addition to thematic analysis, our interpretive phenomenological lens also revealed an essence. First, we discuss the philosophical underpinnings which led to our methodological understandings. Second, the philosophical and methodological understandings are elucidated through explanation of our exemplar study’s elements.
Qualitative researchers use focus groups as a data collection method, allowing the representation of multiple perspectives, while acknowledging that they can derive key information from the consensus or discrepancies between focus group members (Kitzinger, 1994; Leech & Onwuegbuzie, 2007). Focus group data collection is often used in qualitative research, and while many types of qualitative research approaches exist, a phenomenological approach traditionally addresses questions regarding people’s lived experiences. Phenomenology, a philosophical concept as well as a research methodology, seeks to understand and represent the lifeworld of individuals (Tuohy, Cooney, Dowling, Murphy, & Sixsmith, 2013). Participants are bound by a common experience or situation, and the researcher focuses on the meaning of these individuals’ experiences with the phenomenon (Creswell, 2007). The combination of focus group data collection and interpretive phenomenology has utility in many types of studies, such as those aiming to improve patient-centered care (Jones, Ingrahm, Cram, Dean, & Davies, 2013).
Interpretive phenomenological research specifically seeks to describe, understand, and interpret a phenomenon (Tuohy et al., 2013)—seeking the essence of the lived experience (Creswell, 2007). Essence from a phenomenological research perspective is described as the intuitive structure of meaning, whereby, direct examples build a complex understanding of an experience (Merriam & Greiner, 2019). “This form of inquiry is an attempt to deal with inner experience unexamined in everyday life” (Merriam & Greiner, 2019, p. 8).
Some researchers (e.g., Webb & Kevern, 2001) suggest that phenomenology, given its focus on individuals, is a conflicting approach to focus group research. However, group experiences are often examined using CBPR (Israel, Eng, Schultz, & Parker, 2013). CBPR is an approach where focus group data collection elicits the concerns of a specific group, often a community of individuals, joined by a shared trait or experience. CBPR involves community members in the project at various stages. Additionally, we believe phenomenology was particularly a suitable approach for this study because we had a rather singular perspective, despite that it arose from a group. This collective knowledge emerged and led us to the discovery of a community perspective, further explained in the exemplar study Results section.
In a CBPR approach, community members are cocreators of knowledge, along with the lead researchers who are often not part of the community of inquiry. Adding legitimacy to this design, the community members are revered as having expert knowledge about the community as well as their own experiences (Israel et al., 2013). Community members’ involvement and investment in the research allows for a more holistic perspective of research outcomes, as the outcomes reflect how the research is directly relevant to the population/community of inquiry. This same relevance of the research could not be achieved by researchers working without community engagement. Due to the focus on community and community members as researchers, CBPR investigators frequently employ focus group data collection strategies (Kieffer et al., 2013).
Literature Overview
A phenomenological approach, specifically interpretive phenomenology, using focus group data collection is gaining more acceptance (Phillips, Montague, & Archer, 2016) because it can provide richness to experiential data (Palmer, Larkin, de Visser, & Fadden, 2010). The combination of interpretive phenomenology and CBPR with focus groups data collection methods is much less common. However, various combinations of interpretive phenomenology CBPR and focus group methods have been conducted in health-care research with implications for quality improvement and/or a deeper understanding of communities’ experiences with chronic disease. Bragadottir, Halldorsdottir, Ingadottir, and Jonsdottir (2018) explored the diagnosis and experiences of having chronic obstructive pulmonary disease using focus groups as well as family dyad with an interpretive phenomenological approach. They discovered that patients with this chronic disease discussed the stigma of having a self-induced condition and experienced shame. Additionally, they found that more education was needed on the condition by patients, family members, and the general public (Bragadottir, Halldosdottir, Ingadottir, & Jonsdottir, 2018). Similar to our study, these researchers engaged in the hermeneutic circle, common in interpretive studies as well as thematic analysis. Their study did not include a CBPR approach, however.
Other research groups (Jones et al., 2013; Palacios & Kennedy, 2010) have combined CBPR approaches and interpretive phenomenology but collected data through individual interviews or family dyads rather than focus groups. Palacios and Kennedy (2010) identified key themes regarding the reflections of Native American teen mothers, such as chaotic and diminished childhood experiences prior to their pregnancy through individual interviews.
Jones, Ingrahm, Cram, Dean, and Davies (2013) conducted a community-based study with Maori—indigenous people of New Zealand. While this was not specifically a CBPR study, culturally appropriate community-based methodology (Kaupapa Māori research) was implemented along with an interpretive phenomenological lens. Family focus group interviews were a portion of the data collection. These researchers provide an example of a well-conducted community-based study evidenced by a 100% retention rate of participants. The authors attributed this high retention rate to the respectful conduct of the research and the collaborative and culturally appropriate strategies used. The outcomes have implications for improving the treatment of asthma among the indigenous Maori people and reducing health disparities. Unlike our study, the latter two (Jones et al., 2013; Palacios & Kennedy, 2010) did not use focus group data collection.
Amendola (2013) also sought to gain essential knowledge and understanding of Hispanic and Latino community leaders’ experiences. Focus groups were used in Amendola’s (2013) CBPR study that employed van Manen’s (2016) interpretive phenomenology analysis method. Results regarding culturally sensitive research practices are surmised to ameliorate the lack of health-seeking behaviors in communities with limited health-care services. Most of these studies (Bragadottir et al., 2018; Jones et al., 2013; Palacios & Kennedy, 2010) pertained to individual (or individual family) experiences, unlike our study which examined a collective experience through focus group discussions, leading to a community perspective. None of the aforementioned studies (Amendola, 2013; Bragadottir et al., 2018; Jones et al., 2013; Palacios & Kennedy, 2010) incorporated Template Analysis, nor did they report an overall essence, distinguishing them from the exemplar study that is explained herein. Regardless of certain aspects of methodology, all of the aforementioned studies demonstrate that merging of interpretive phenomenology and CBPR is possible and beneficial for both individuals and groups in a health-care context.
Our exemplar study was unique in that we used Template Analysis in conjunction with focus group data collection using a phenomenological lens and a CBPR approach. Template Analysis, in particular, was fitting with our research paradigm because it allows recognition of multiple epistemological positions (Brooks, McCluskey, Turley, & King, 2015; King, 2004), that is, it was flexible enough to fit our merged approaches but is also applicable to health-care research (Brooks et al., 2015; King, Carroll, Newton, & Dornan, 2002; McCluskey, Brooks, King, & Burton, 2011). We sought perspectives from individuals with diverse levels of involvement with Parkinson’s disease (PD, e.g., people with PD, their caregivers, and professionals who regularly treat with people with PD). Finally, our innovative research methodology revealed an overall interpretive essence or overarching (essential) theme. Our research is the only study we know of to merge a CBPR approach with interpretive phenomenological methodology using focus group data collection and derive thematic results that led us to an overall essence.
The purpose of this article is to describe the merging of interpretive phenomenology and a CBPR approach using focus group data collection. First, this merging will be considered conceptually and then illustrated through an exemplar study. An interpretive phenomenological lens and analysis methods can help enhance the authenticity of findings from a CBPR study by seeking in-depth understanding of the experiences of the community of inquiry. In the following sections, we initially present an overview of known methodological aspects: (1) the methodological foundations of phenomenology, highlighting interpretive phenomenology; (2) interpretive phenomenological methods in combination with focus group data collection; and (3) interpretive phenomenology merged with CBPR.
Finally, we will illustrate our methodological innovation by exploring exemplars from our study that helped develop a deeper understanding of the experiences of a rural PD community (see Figure 1).
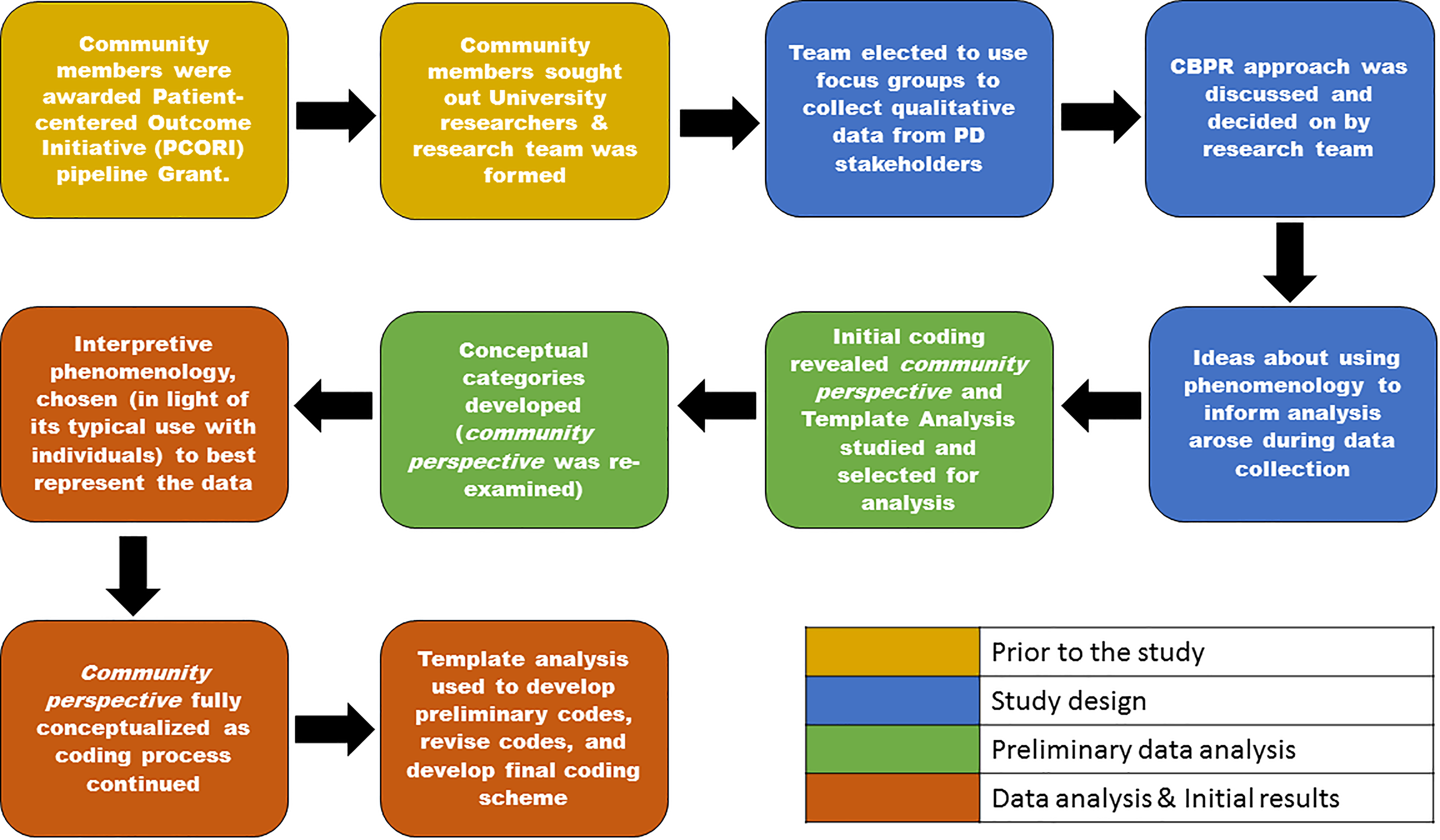
Methodological decision-making.
Phenomenology: Methodological Foundations
Historically, a phenomenological research approach started as descriptive in nature. It sought to provide representations of people’s experiences through an unbiased perspective (Matua & Van Der Wal, 2015; Sloan & Bowe, 2014). This form of phenomenology, termed descriptive or transcendental, can be contrasted with interpretive phenomenology, sometimes further classified as either existential or hermeneutic. Interpretive phenomenology suggests that researchers cannot remove themselves from the phenomena that they are studying (Sloan & Bowe, 2014) and that there is more than one meaningful representation of human experiences (Kafle, 2011). In the remainder of this section, we will describe the unique elements of interpretive phenomenology, specifically, aspects of interpretation, and a brief review of essence.
Interpretive phenomenology examines human experience, and thus, interpretation is critical (e.g., Langdridge, 2007; Laverty, 2003; Tuohy et al., 2013). That is, the search for understanding in interpretive phenomenology can only be communicated through the researcher’s explanation of the participants’ experiences. Critical aspects of the researcher’s interpretation include the researcher’s bias, background, and position within the research topic and process, requiring one to be diligently reflective. Relatedly, two other key concepts of interpretive phenomenology are that researchers cannot remove themselves from the phenomena that they are studying (Sloan & Bowe, 2014) and that multiple representations of human experience exist (Kafle, 2011).
Interpretive phenomenology distinctively seeks to discover the essence, or essential meaning, of the phenomenon under inquiry. The process of uncovering the essence of lived experiences may be described as a qualitative researcher identifying the phenomenon of a human experience and then deriving a description that represents the very nature of the experience (Kafle, 2011; Sloan & Bowe, 2014). The essence should not be viewed as a mysterious idea but rather the ability to identify the meaning embodied in the lived experience (Merleau-Ponty, 1962; van Manen, 2016).
This idea of essence is central to an interpretive phenomenological study. van Manen (2016) described a necessity for the researcher to capture the interpreted essence rather than simply convey the experience. Describing the experience cannot occur without interpretation. van Manen (2016) acknowledges that while the use of language is inadequate to describe the full essence of a phenomenon, it is the only way to disseminate the experience.
Interpretive Phenomenology and Focus Groups
Focus groups are a special type of group in terms of purpose, size, composition, and procedure, with participants often selected because they share certain characteristics pertinent to the topic of interest (Krueger & Casey, 2009). Focus groups are an economical way for people to share openly about problems or delicate subject matter and provide researchers with a way to collect data from a group unit versus individual or family interviews (Cyr, 2019). An interpretive phenomenological approach is used less frequently with focus group data, as it is generally applied to the inquiries of individuals. In fact, some health-care researchers believe that interpretive phenomenology cannot be applied to the use of focus groups (Webb & Kevern, 2001), while other health-care researchers (e.g., Cote-Arsenault, & Morrison-Beedy, 2001; Kooken, Haase, & Russell, 2007) have demonstrated the congruence of interpretive phenomenology and focus group data collection.
The value of an interpretive phenomenological approach to focus group data is to elicit more experiential insight and reflection than may be achieved in an interview. The focus group is ideally a naturally occurring one, when group membership is, in fact, also the topic of inquiry (Palmer et al., 2010). Smith’s Interpretative phenomenological analysis (IPA), a popular hermeneutic analysis method, has also been used with focus group inquiry (Palmer et al., 2010). Smith (2004) claims that using focus group data collection with an interpretive phenomenological lens is an endeavor that should be explored further. Whether conducted with groups or individuals, research using an interpretive phenomenological lens has largely the same objective—to enhance knowledge and understanding of human experiences.
Interpretive Phenomenology and CBPR
A natural synergy exists among CBPR and an interpretive phenomenological philosophical assumption. Constructivist (or social constructivist) and interpretivist paradigms both grew out of hermeneutic philosophy (Mertens, 2015) and are, therefore, clearly linked. Interpretive phenomenology seeks to elicit perspectives and experiences to construct shared meaning, and social constructivism contends that meaning is made in a social context, and that to understand the phenomenon of interest one must gain the perspective of those who lived it (Mertens, 2015). CBPR asserts that the social context is a place to create meaning and states that understanding of a community’s (or community members’) experiences should come from the community itself (Israel et al., 2013).
Another important similarity between interpretive phenomenology and CBPR approaches is the embedding of reflection in the methodology. The general purpose of these two types of studies is similar: co-constructing knowledge. That is, the purpose of an interpretive phenomenological approach to research is to gain a deeper understanding of a phenomenon by systematically uncovering meaning through lived experiences. “Qualitative approaches to research such as phenomenology seek to include knowledge as co-constructed” (Sloan & Bowe, 2014, p. 1298), relying on interpretation from the researchers combined with the experiences shared from the participants. The idea of co-constructing knowledge is also a key principle in CBPR studies because CBPR recognizes a community as both a social and cultural group and involves community partners in multiple aspects of the research as well as in cocreating knowledge and change from research findings (Johnson, 2017). CBPR employs individuals not only as research participants but also as researchers.
The focus of this article is to discuss the similarities in their overarching purpose as opposed to a detailed review of each type of research design. That is, these two methodological approaches are synergistic because of their shared similar research aims focused on the development of competent and caring practitioners and, to this end, can incite institutional improvement (Quigley, 1997). The development of informed practitioners, rooted in the best interests of their communities, may be achieved using CBPR principles. In fact, the central tenet of CBPR research is to achieve practices that best suit a community and its needs. Interpretive phenomenology aims to understand lived experiences and when applied to health care, aims to gain a more in-depth understanding of patients and their health-care experiences.
Additionally, the essence of a group or collective experience is a valuable outcome for qualitative researchers seeking a deeper understanding of the community’s experiences. An essence can be obtained through interpretive phenomenology and community-based approaches. Moreover, focus group data, particularly when the groups are naturally occurring may be the ideal data collection method.
Reflection is another point of linkage between interpretive phenomenology and CBPR. Focus groups, when conducted in the context of CBPR, are inclusive and empowering, viewing community members as the experts, the ones who can interpret their own experience as well as equally participate with researchers and health-care professionals throughout the process (Kieffer et al., 2013). Reflection, commonly referred to as reflexivity, should not only pertain to the research process but also to the researcher’s own understanding of the phenomenon, in conjunction with a surrender of control and certainty about what the research will reveal (Kafle, 2011).
Reflection is key to conducting CBPR studies because this type of research offers a path to transform teaching, research, and service. Engaging the community through CBPR is essential for researchers external to the community to understand transformative change. Researchers directly from the community are also transformed through their reflection of the experience (Jacoby, 2015). Thus, CBPR adds to the concept van Manen (2016) previously described: Interpretive phenomenology posits that one learns mainly from reflecting on experience.
The literature reviewed herein suggests that merging CBPR and interpretive phenomenology can potentially discover culturally sensitive research practices that could reduce health disparities. The aforementioned studies (Amendola, 2013; Bragadottir et al., 2018; Jones and colleagues, 2013; Palacios & Kennedy, 2010) all had implications for discovering culturally sensitive research practices that could reduce health disparities.
Exemplar Study
This section will demonstrate the merged research approach by describing an exemplar study about support group experiences of a rural PD stakeholder community (e.g., people with PD and their caregivers as well as various health-care professionals who treat individuals with PD). The study was conducted in a rural state in the western United States. The state, considered overall rural (communities with less than 50,000 people), has 69% of its population living rurally (Rural Health Information Hub [RHIhub], n.d. a). In fact, 78% of the counties are also considered frontier (the most remote and sparsely populated places in the United States; RHIhub, n.d. b).
Particularly, we describe the study’s aims, specific design and methodological elements, and study results to illustrate this novel merging of approaches and its utility. The researchers of this exemplar study included two of the three authors of this manuscript (Bush and Singh), and therefore the exemplar study researchers will be referred to as “we” and the study as “ours.”
The exemplar study description demonstrates researcher engagement and collaboration with a community, combined with a subsequent reflection on the lived experiences of that community. Our intended purpose was to (a) gain a deeper understanding of the PD stakeholders’ (i.e., people with PD, their caregivers, and professionals who treat individuals with PD) support group experiences, (b) obtain meaningful results in the form of representative themes, and (c) pursue an overall essence from the derived themes as well as the researchers’ reflection and interpretation of the themes. The appropriate university’s Institutional Review Board (IRB) approved this project, and the researchers complied with all IRB requirements and policies on the protection of human subjects.
Description of Innovative Methods
To describe the research process utilized for the exemplar study, we first refer to Crotty’s (1998) four elements of research (epistemology, theoretical perspective, methodology, and methods). Our epistemological view, social constructivism, is reflected by the researchers’ collective point of view that meaning for our participants would be constructed over time (e.g., as they had additional support group interactions, changes in their feelings of group membership, and/or more experience with the disease process or with those who have PD). We believed participants’ knowledge and meaning regarding support group experiences were inextricable from their personal relationships and human interactions (Gergen & Gergen, 2008).
Our theoretical perspective/paradigm was that of interpretivism, in accordance with our interpretive phenomenological methodology. Our focus was on discovering the meaning of PD stakeholders’ contextualized, subjective experiences with PD support groups. We also sought to derive a representative interpretation of the experiences. Our methods included focus group data collection and Template Analysis as concrete techniques (Crotty, 1998) along with additional techniques and procedures described in the following sections.
Procedures
Initially, we collected focus group data for a CBPR study to examine the experiences of PD stakeholders with rural support groups (see Figure 1). This CBPR project involved multiple groups of researchers including community, university, and student researchers. Community researchers refers to individuals from the community of inquiry that had a significant role in the research throughout the study. University researchers refers to formally trained researchers who helped lead or conduct all aspects of the research and oversaw that the study was conducted in accordance with the IRB protocol for the protection of human subjects. Student researchers were bachelor’s or master’s degree-seeking students who opted to participate in the research under the supervision of the university researchers. The university researchers utilized several of Israel, Eng, Schultz, and Parker’s (2013) nine community engagement principles/methods throughout the research design including principles such as CBPR acknowledges the community as a unit of identity, that CBPR builds capacity, and fosters co-learning among all partners (Israel et al., 2013).
Both university researchers and PD stakeholder community members were involved throughout our research study. The CBPR research approach, utilizing members of the community of inquiry, was deemed an appropriate, natural, and meaningful way to approach our search for understanding the experiences of this community (Wallerstein & Duran, 2006).
Participants and sampling
Five focus groups consisting of 30 PD adult stakeholders participated in the study in their rural state. Stakeholders included persons with PD, caregivers, and professionals who work with individuals with PD regularly (e.g., physical therapists, occupational therapists, speech-language pathologists, pharmacists). Each focus group consisted of —four to nine stakeholders who volunteered to participate by responding to a call for participation in a statewide network newsletter.
To those who had expressed interest in the meeting, but were unable to attend, a video chat option was offered. Because the nature of the study is identifying rural needs, we did not want to exclude a group simply because they could not travel to participate in person. Thus, one of the five focus groups (with four individuals) was conducted via video conference rather than in person and the rest in hotel conference rooms. Participants self-selected where and with whom they sat. We implemented self-selection to groups intentionally to foster a more open setting for sharing personal experiences, opinions, and beliefs as well as to address and potentially reduce unequal power relationships. During the moderation of focus groups, the stakeholders with PD emerged as the experts of their group, which appeared to help align power relationships appropriately for this study. We revisit the concept of power relationships in the following section.
Design
Aspects of the CBPR approach were integral to the design of the study because we sought to understand support group experiences for people with diverse PD stakeholder backgrounds. Therefore, the common CBPR data collection strategy of focus groups was used (Tapp, DeHernandez, & Smith, 2017). Additionally, focus groups for this study reflected “mini-communities,” and consisted of various types of PD stakeholders in each focus group.
A CBPR approach was also chosen for its focus on equalizing power relationships. Notably, in our study, stakeholders who had PD surfaced as the experts in their focus groups, and this occurred across groups. This is an important distinction, especially in a CBPR study, because in other types of more traditional scenarios, health-care practitioners would be viewed as the experts. We observed that the majority of rich data, shared by people living with PD, were regarding their support group experiences. Such expertise was considered appropriate to the university researchers and was in fact our goal. This expertise was only achieved through a CBPR approach because possibly being a researcher as opposed to being researched was empowering to community researchers. The professionals who attended our focus groups seemed to naturally fall into the role of consultant, providing information about their areas of expertise such as medication issues that arose or payer source issues (e.g., Medicare reimbursement).
We achieved diversity in stakeholders’ attendance by sending the invitations to the luncheon, via the newsletter, to all parties interested in PD in any capacity in the state. However, we did not orchestrate the diversity of the stakeholder groups in any way. We sought to maximize participants’ comfort, so participants self-selected where they sat and with whom they interacted, much like a natural-occurring community.
Finally, we chose a CBPR approach because it was the most authentic way to study the inner workings of a community, to whom we were outsiders (Propst, McDonough, Vogt, & Pynnonen, 2008; Schneider, 2012). It added authenticity to the study by including community members as researchers at multiple levels of the project. The study’s aim was phenomenological at its core because we sought to understand, at an in-depth level, how people with PD and those who cared for them described their support group experiences while living in rural communities. Our presumption, based on discussions with community partners through the statewide Parkinson’s network, was that everything about PD and PD health care was more challenging in a rural community because of the sparsity of providers, the lack of specialty clinics and hospitals, and the small numbers of individuals living with similar neurological conditions.
Data collection
Focus group questions were designed and presented collaboratively by the academic researchers and the community members. Each moderator also asked follow-up, context-dependent questions. The informal, semistructured focus group interviews were the primary source of data collection, along with field notes. Co-moderators were either community members or student researchers. The focus group discussion guide included issues previously identified by PD community partners (PD patients and caregivers) such as current health-care barriers and resources as well as needs and possibilities regarding future PD health care. Focus group discussions were audiotaped and transcribed verbatim by student researchers. The university faculty researchers reviewed and analyzed the transcriptions as well as field notes, first, through immersion in the data corpus and hand-coding. Later, the data were further organized using NVIVO 10® software.
Data analysis
Template Analysis was chosen as a data analysis method due to its flexibility and applicability to many types of worldviews and philosophical lenses (Brooks et al., 2015) and particularly its use in health-care research (King et al., 2013; McCluskey et al., 2011). This flexibility was advantageous as we merged research approaches not commonly combined. Template Analysis fits well with research paradigms, such as interpretivism, that recognize multiple perspectives and allow for diverse interpretations of a given phenomenon (King, 2004).
Additionally, Template Analysis was chosen because of its compatibility with the use of a priori codes, its general use of hierarchical thematic coding, its focus on maintaining a balance between structure and adaptability, and the priority given to the richest data and a broad view of the data (Brooks et al., 2015). To clarify the latter point, Template Analysis promotes more of a cross-case approach to data, as opposed to a within-case approach, as seen in other types of interpretive phenomenological data analyses such as Smith’s (1996) IPA (Brooks et al., 2015). The aspect of a broader view was specifically applicable to our study as we gained a community perspective and did not take a case-by-case approach. Template Analysis was also well suited to our study as we had two a priori concepts represented in our interview protocol. We acknowledged that these concepts may emerge from the data and would therefore be predetermined themes. Like all other themes in Template Analysis, a priori themes are “subject to redefinition or removal…should they prove ineffective at characterizing the data” (Brooks et al., 2015; Krueger & Casey, 2009, p. 218). The specific a priori–conceived themes are addressed and illustrated further in our exemplar study Results section.
We followed the general guidelines of Template Analysis as presented by King and colleagues (2013) as well as other basic coding strategies and principles (e.g., constant comparison, open coding, axial coding). Figure 2 displays an overview of the processes/steps of our Template Analysis.
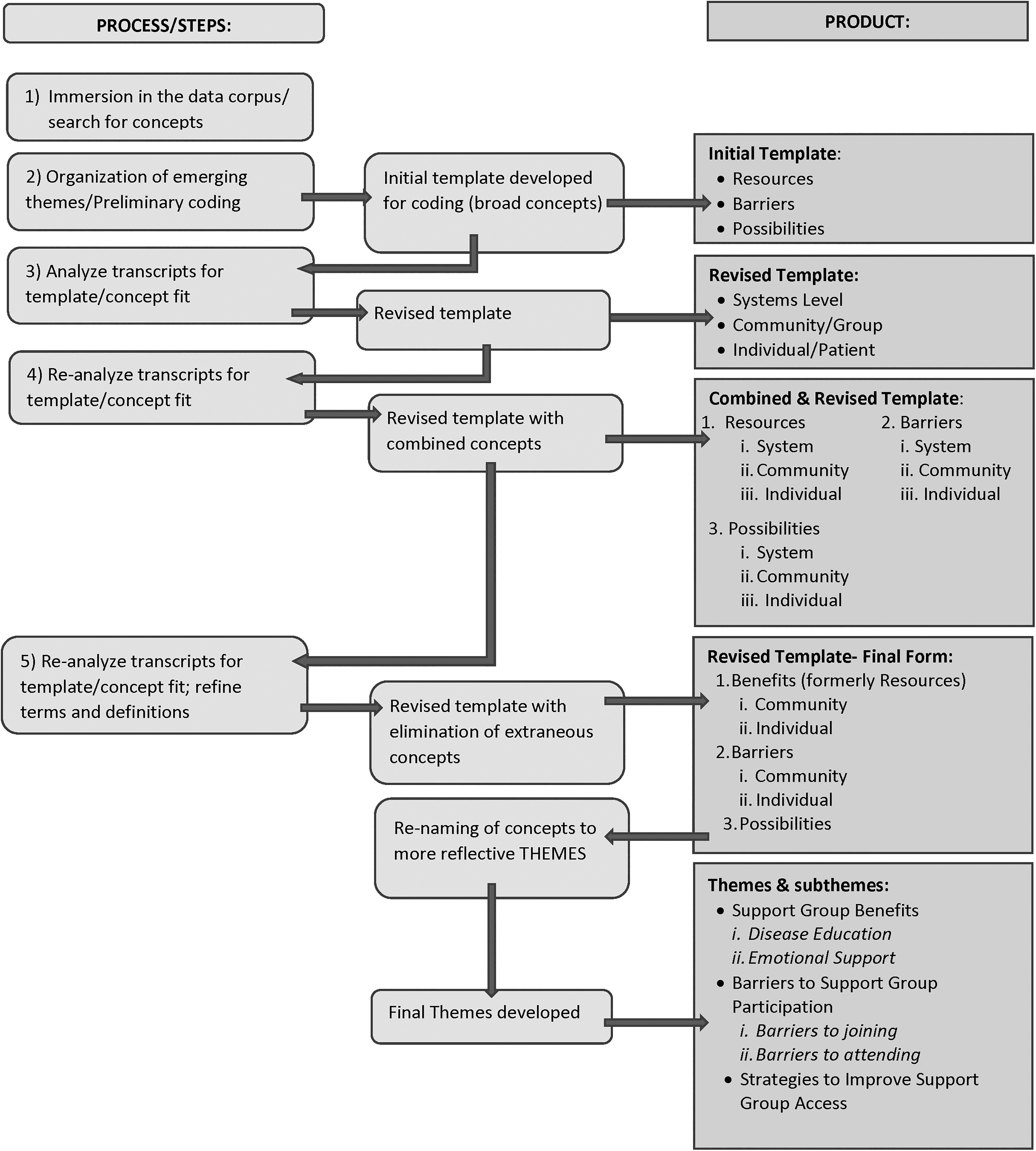
Template analysis diagram.
As we were developing our template, we made multiple revisions and reflected the significant changes in Figure 2. We incorporated other interpretive phenomenological principles not listed on the figure as they occurred throughout the process and not in one discrete step. These included multiple discussions between the researchers, ongoing self-reflexivity, and the process of moving reciprocally between the community’s experiences (data) and the perception of the researchers (interpretation) using the hermeneutic circle (Halling, 2008).
The hermeneutic circle is a process by which reciprocal and circular questioning along with continual examination and reexamination of data and the researcher’s interpretation of the data takes place. This was used as a complementary process to our use of Template Analysis. These processes occur repeatedly, uncovering new insights and expanding upon already-attained insights (McConnell-Henry, Chapman, & Francis, 2009). The circle is carried out (and potentially never finished) with an aim to uncover the genuine meaning, thereby gaining an in-depth understanding of the experience of inquiry.
We continually brought our focus back to the lived experiences of our participants situated within our purpose of understanding the meaning of support group experiences of a rural PD community by returning to our data and considering our aim of developing a representation of the experiences that resonated with stakeholders. After determining and titling our themes, we returned to the transcripts to examine the themes and their meanings again. After further reflection, our interpretive lens guided us toward the overall essence and interpreted meanings of rural PD stakeholders’ support group experiences. Credibility of our analysis procedures was ensured by continual discussion between the two qualitative expert authors, cross-check of emergent themes by the other researchers including community researchers involved in the study, and member checking. We conducted member checking at a follow-up luncheon where the research team presented the main findings to the rural PD community and asked for additional input and necessary changes. No significant changes were needed, only subtle word changes of themes that were largely due to the group’s preferences.
Description of Exemplar Results
Discovery of the community perspective
When we initially designed the study, as well as when we began data analysis, we envisioned analyzing opinions and experiences. We first noted significant statements through individual descriptions; however, it became apparent early in our preliminary analysis that our stakeholders were reporting the same benefits and resources across participants within groups as well as across focus groups. We were surprised by the obvious consensus of our focus group participants. We began reanalysis within the context of a community perspective (which are the analyses process what we have described herein). We searched for disparate perspectives and opinions, but even in the personal experiences relayed, commonalities rather than differences were conveyed by stakeholders regarding the lived experiences with PD support groups. This is further described in a pertaining paper regarding our results (Bush, Singh, Hidecker, & Carrico, 2018). The strong consensus about resources and barriers may be partially due to the individuals with PD being revered as experts about living with the disease. This equalization of power relationships, addressed previously, is key to a CBPR approach. That is, the providers and caregivers in the focus groups may have been less likely to communicate their opinions, deeming them as less relevant or less important. Also, people who do not have PD, even if they had attended groups, may not have strong opinions either way because they do not rely on support groups in the same way that people with PD do.
Once this consensus emerged, we began conceptualizing our results as a community perspective during our preliminary data analysis and explored its suitability. Throughout our analysis, we explored the data using this community concept.
Thematic results
First, through Template Analysis, representative themes emerged and their descriptions were continually refined (see Figure 2) PD stakeholders in rural communities discussed the benefits and barriers they experienced. The two a priori categories, Barriers and Resources, did in fact emerge as significant in the data, given their richness of description. These a priori themes were imperative to include, as they were deemed important by our community-based researchers who were also members of the community of inquiry.
Illustrating our use of Template Analysis, broad categories were further developed as themes and eventually given different names (Support Group Benefits and Barriers to Support Group Participation) as well as assigned subthemes. The subthemes represented significant statements about support groups’ benefits and barriers at a group or community level as well as at an individual level. Further data analysis revealed an unanticipated theme as well, which we initially categorized as Possibilities and later named the theme Strategies to Improve Support Group Access, which was more reflective. Three main themes and four subthemes are explained in detail in a previously published manuscript (Bush et al., 2018) and are listed in Table 1.
Themes and Subthemes Derived From Template Analysis With Illustrative Quotes.

The essence
Following Template Analysis, an overall essence was derived as we reflected on our entire analytic process and reflected on the resulting themes. We sought a cohesive statement that was reflective of the community experience and one that seemed evident as we returned to each theme and subtheme.
In examining and reexamining our results, it was clear that Strategies to Improve Support Group Access was notably different from our other two main themes. As we reflected on this, we examined it from its genesis, the concept of Possibilities. The participants’ mission partly seemed to be providing recommendations to us to change (and improve) support group access. Possibilities implied future, and the fact that they were worded as recommendations furthered their futuristic implications. Strategies to Improve Support Group Access was chosen as the theme name, using “strategies” to convey that this content had been stated as action items in a directive manner. We began to realize that this theme was not about how to improve the participants’ own support group access, even though they had admittedly experienced barriers to joining/attending support groups. Perhaps most importantly, this theme pertained to how to improve access, in the future, for others—recommendations from the people who had PD and their closest caregivers.
Thus, the essence of this research had to encapsulate that (1) there were both barriers to and benefits of support groups in rural areas (2) that the benefits outweighed the barriers, and (3) that this community sought to improve access to support groups for individuals like themselves in the future, not for themselves. That is, the legacy these individuals wanted to leave was for future patients with PD. Many aspects within the data corpus communicated what we interpreted as hope. Hope that the disease process is made easier in the future. Hope for a cause, and of course, the agonizing hope for a cure that will most definitely come too late for this rural PD community. We believe we have captured the community’s experience with PD support groups through this essence: Experiencing support group benefits, despite barriers…leaving a legacy.
Discussion
Our exemplar study demonstrates methodological innovation by merging an interpretive phenomenology lens with a CBPR approach. This merging was achieved through focus group data collection and a two-step data analysis that resulted in thematic results as well as an overall essence of a community’s experience. A combination of methods and design elements enabled the researchers to gain a deeper understanding of a rural community of PD stakeholders and their experiences with support groups.
Other studies such as Bragadottir and colleagues (2018) sought a deeper understanding of patients’ and caregivers’ experiences with a chronic disease. These researchers also found that patients’ health-care education about their condition was lacking (Bragadottir et al., 2018), as did our exemplar study.
Uniquely, our study examined a collective experience through focus group discussions with a community. Additionally, our use of Template Analysis was innovative because it revealed an overall interpretive essence, along with thematic findings. Our research is the only study we know of to merge a CBPR approach with interpretive phenomenology using focus group data collection and Template Analysis to derive hierarchical thematic results as well as an overall essential theme.
Our original intent for this project was to conduct a CBPR, qualitative inquiry to determine what PD stakeholders believed were barriers and resources to PD health care in their rural community. Focus group data collection was selected by our community researchers as the best representation of multiple perspectives as well as the PD community. Interpretive phenomenology, specifically, emerged as the most fitting way to represent the community of stakeholders (see Figure 1).
We are aware that when merging methods, the debate is less often about the merging of design elements, and more so with the merging or congruence of the theoretical underpinnings of the approaches being merged. CBPR research often uses a critical approach theory or a constructivist theory (Caine & Mill, 2016). A social constructivist approach corresponds with interpretivism, in that it takes the stance that the process of knowing is contingent upon human interaction with the world in a social context (Crotty, 1998). The interpretive paradigm purports that reality is constructed in social contexts as well and that shared meaning is created through eliciting human perspectives and experiences (Mertens, 2015). Interpretivism and social constructionism both value the human perspective and aim to understand the process of making meaning. Further, the worldviews of interpretivism and social constructivism are congruent with a CBPR approach in our study because we solicited responses from a community about their health-care experiences. We then sought to interpret those experiences after engaging with, deferring to, and collaborating on this research with the community of interest.
Despite the design elements being less of a debate than the theoretical underpinnings, their consideration and explanation is necessary to provide a holistic, transparent view of our methodological decisions. Our community perspective would not have emerged without the use of both focus groups and a community-based approach. Focus groups were the best way to talk to and learn from as many community members/stakeholders as possible (Cyr, 2019), and our search for an in-depth perspective about a community was best achieved by including community members, as researchers, who experienced the phenomena (Israel et al., 2013).
The representation of the perspectives of this community could not have been gained without a phenomenological approach, and using an interpretive approach enabled us to find a representative essence. Template Analysis allowed the inclusion of a priori themes which best represented the community of stakeholders, as the a priori concepts were critical to the development of the interview protocol and developed by the community researchers. Template Analysis also allowed us to represent our changes and modifications to the themes in a meaningful way, demonstrating that they were based on our iterative process, use of the hermeneutic circle, and reflected constant comparison.
Recommendations for Merging Interpretive Phenomenology and CBPR
A perceived limitation may be our use of a priori concepts, which were later deemed themes through the analysis process. A superficial view of this may raise concern or seem inconsistent with our interpretivist lens, further consideration of how they were determined, as well as our use of a CBPR approach, should address these concerns. When used carefully and thoughtfully, a priori themes, like the ones in our study, permit researchers to convey concepts that inform the study or assist in determining the study’s aims (Brooks et al., 2015).
Finally, the overarching aspect of this study may be problematic for some because we used focus group data collection methods and used an interpretive phenomenological lens to view and analyze our data. We have contemplated this aspect and still feel that our methodological choices best represent the data. Some studies may describe diverse themes rather than focusing on one central essence like our study did with community lived experiences. As with all qualitative studies, the researcher’s worldview should guide the research aim, and the aim should inform the data collection and analysis process. The individual design elements of our exemplar study may not be the most suitable ones for other researchers who combine CBPR and interpretive phenomenology. The inductive nature of all qualitative studies should guide the researcher as she or he makes the inevitable changes and modifications in a search for meaning—especially when seeking in-depth understanding of a community.
Conclusion
This article adds to the methodological literature base and may also inform health-care practice. We explored merging two approaches, CBPR and interpretive phenomenology, as well as their congruence. The similarities in the overall aim of both CBPR and interpretive phenomenology are to represent people’s perspectives and experiences with a phenomenon. Community-based research may lend itself to an interpretive phenomenological approach, using focus group data collection, when there is a collective perspective from a homogenous community. The exemplar study described illustrates how and, ultimately, why we merged these approaches. For clinicians working in rural areas and with patients, caregivers, and stakeholders, both the exemplar study results and our methodological decisions discussed herein, have implications for practice—to view living with a chronic disease as a communal experience is potentially transformative to many clinicians. Some of the methodological understandings such as stakeholder engagement and viewing the chronic illness experience as an essence clearly can be informative of patient- or client-centered clinical practices.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.