
Abstract
Interest in studying experiences has grown rapidly; however, little attention has been paid to the applicability of qualitative methods for capturing the service experience in children’s health care. This study examined and compared three data collection methods to capture the multidimensional service experience of child patients and their families: video diaries with child patients, narrative interviews with parents of a child patient, and semistructured interviews with health-care professionals working with child patients. The methods were analyzed with respect to their benefits and limitations and their applicability for capturing the multidimensional service experience presented by service experience co-creation framework, including the temporal, factual, spatial, locus, control, and organizational dimensions. The key findings are as follows: (A) The video diary method has the potential to capture the temporally broad and spatially complex phenomenon of child patients’ service experience and enables researchers to capture service experience created beyond the hospital setting (e.g., through hobbies or in school). (B) Narratives with parents have the potential to capture the temporal, spatial, locus, and organizational dimensions through stories and are well-suited for mapping children’s experiences and the actors influencing them. (C) Semistructured interviews with health-care professionals have the potential to capture a generalized but temporally narrow view of the service experience of child patients, concentrating on experiences within hospital settings. This is beneficial for developing health-care service providers’ actions. Structured analysis and comparison of methods guides researchers to select appropriate methods to take a complementary approach in the understanding of experiences in the context of children’s health care.
Introduction
Recent years have seen increasing interest in and research on experiences. Experiences are particularly pivotal in health care, as patients’ experiences are connected to how patients engage in their own care (McColl-Kennedy, Hogan, Witell, & Snyder, 2017) and, thus, the cost-effectiveness of the health-care system and positive health outcomes for individuals. Due to its extremely personal and sensitive nature, health care has its own unique, context-specific characteristics (Bolton, Gustafsson, McColl-Kennedy, Sirianni, & Tse, 2014; Danaher & Gallan, 2016). These characteristics make health care an interesting field for examining experiences (Berry & Bendanpudi, 2007; Danaher & Gallan, 2016) but also imply that special attention should be paid to methodology: Researchers should simultaneously capture the complexity of the experience and avoid disturbing the sensitivity of patients, who may be undergoing painful experiences that influence their quality of life. In this article, we focus on qualitative data collection methods to capture the multidimensional service experience of child patients (Helkkula, 2011; Jaakkola, Helkkula, & Aarikka-Stenroos, 2015).
To date, little attention has been paid to service experience among children in health care or to the applicability of the variety of qualitative data collection methods (later methods) for capturing these experiences. A search of the academic literature revealed only a handful of studies reporting findings on the experiences of children (see Table 1). Among these, Carney et al. (2003) studied the appropriateness of verbal and visual structured and unstructured questionnaires in hospitalization experiences, and Curtis, Liabo, Roberts, and Barker (2004) utilized different methods to study children’s health-care experiences while examining the data collection process. Some studies have used mixed methods that combine interviews with drawing or play techniques (Curtis, Liabo, Roberts, & Barker, 2004; Sartain, Maxwell, Todd, Haycox, & Bundred, 2001).
Overview of Methods Applied to Study the Health-Care Experiences of Children

Building on existing studies (see Table 1), however, research on the experience of children in health care has been limited and further exploration is needed to elaborate on how different methods capture the multidimensional service experience of child patients. Researchers have approached the experience as an elusive concept, rather than a multidimensional, holistic phenomenon. Hence, more research is needed to yield structured knowledge of how different methods capture the service experience of child patients and with what kind of research designs including methods and informants child patients’ experiences can be captured. Our study seeks to address this gap by empirically comparing a set of studies with different data collection methods on the service experience of child patients.
We conducted three studies with different data collection methods—video diaries, narratives, and semistructured interviews—to study the service experience of child patients in health care. The aim of the study was 2-fold: first, to analyze the benefits and limitations of using each method to study the service experience of child patients and, second, as service experience is conceptually multidimensional and rather elusive, to examine and compare each method’s applicability for capturing different dimensions of the concept.
We examined service experience using Jaakkola, Helkkula, and Aarikka-Stenroos’s (2015) key dimensions of service experience co-creation conceptual framework. Their framework consists of six dimensions, discussed below, that explicitly evoke the different dimensions of the service experience originating from established research streams. To our knowledge, this is the first attempt to utilize the framework in an empirical service experience study.
Background
In this article, we approach the phenomenon of child patients’ experience as a service experience, which we define as a subjective, event-specific, context-specific, and multidimensional phenomenon that is simultaneously individual and social, emerging in various events through imagination or memory (Helkkula, 2011; Jaakkola et al., 2015). The “service” in “service experience” reflects not an output of an intangible product (as indicated by the plural form, “services”), but a process of using one’s resources (e.g., skills or knowledge) for the benefit of another actor (Vargo & Lusch, 2008). From this perspective, an actor (e.g., patient) determines the service experience phenomenologically, not just while using a specific service, but through a wider phenomenological context that extends beyond the specific service and service network to the actor’s everyday life (Gummesson, Mele, & Polese, 2013).
Service Experience in the Health-Care Context
The broad phenomenological service experience concept posits that service experience is created among multiple different actors (Vargo & Lusch, 2011; Verhoef et al., 2009). In health care, the scope of the service experience is particularly broad (Klaus, 2018), as patients may undergo a complex “journey” through different clinical, nonclinical, and social events, all of which influence their total service experience (Ponsignon, Smart, Williams, & Hall, 2015). These journeys include a myriad of interactions with various professionals and patients’ social world actors (e.g., relatives and other patients), all participating in the service experience creation in their own way and in different locations (Frow, McColl-Kennedy, & Payne, 2016). Therefore, the methods used to study this phenomenon must capture a temporally and spatially broad spectrum of events among these actors, which have thus far gone unrecognized in service experience research (Banerjee, 2014). Furthermore, health-care context is highly emotional and may invoke a wide range of thoughts, feelings, sentiments, and physical reactions due to a heightened sense of risk, invasiveness, and personal relevance (Bolton et al., 2014; Danaher & Gallan, 2016), increasing the sensitivity and complexity of the phenomenon.
Zooming Into Service Experience in Children’s Health Care
Accessing the service experience of children should be of great importance and interest in today’s research, especially when focusing on children’s health care. Without access to the content of a child’s experience, we have very limited accounts of what the preferences and needs of children are in the period that may be physically and mentally debilitating for children and may influence their developmental story (Greene & Hogan, 2005). By accessing children’s service experience, we will come to know more about their interpretations of events and their world that may differ from that of adults. This knowledge is pivotal for health-care sector to provide higher quality, safer, and more efficient services for child patients and their families.
When inquiring about the sensitive and complex service experiences of child patients in a health-care context, ethical matters should be considered carefully (Burns & Grove, 2001, p. 166; Phelan & Kinsella, 2013). As participants in research situations, children are more vulnerable and experience stress more readily than adults (Burns & Grove, 2001; Kortesluoma & Nikkonen, 2004). The research process can cause children emotional distress, particularly in situations that ask them to reflect on painful or invasive past experiences (Burns & Grove, 2001). In addition, the power imbalance between children and adult researchers must be considered (Greene & Hogan, 2005). Children may feel intimidated when talking to an unfamiliar researcher (Punch, 2002), and they may try to please the researcher by giving the “right answers” (Punch, 2002; Singh, 2007). Further, compared to adults, children have more difficulty understanding the implications of participating in a study (Kortesluoma & Nikkonen, 2004), including participation rights and study purpose. Finally, some level of cognitive competence, including language skills, thinking, reasoning, and understanding, is needed to fully access service experience (Ponsignon et al., 2015). Some previous studies have utilized visual or mixed methods rather than interviews (see Table 1) to overcome children’s undeveloped storytelling and dialogical skills by making it easier for children, especially younger ones, to present their experiences (Forsner, Jansson, & Sørlie, 2005; Greene & Hogan, 2005).
In pediatric health care, service experiences are evoked among not only patients but also caregivers and relatives (McColl-Kennedy et al., 2017; Michaels, 2018). This makes it difficult to explicitly posit who is the main beneficiary of the experience and the subject for studies concerning experiences in children’s health care: the patient, the parents, or the whole family. Because multiple actors experience the illness in pediatric care, some aspects of the service experience may be accessed through the child’s parents, who are inextricably a part of their children’s lives, or the pediatric health-care professionals responsible for the medical care of the children. However, researchers must remember that children’s subjective service experience may differ, sometimes dramatically, from those of adults (Savage & Callery, 2005). Experiences are always shaped by an individual’s unique values, actions, beliefs, motives, traditions, cultural background, possessions, and aspirations (Bolton et al., 2014; cf. Coyne, 2006); therefore, researchers should pursue methods that allow children of different ages to express themselves (Curtis et al., 2004; Forsner et al., 2005).
Dimensions of Service Experience
A holistic understanding of the service experience requires acknowledging its multiple dimensions. Therefore, in this study, we utilize the key dimensions of the service experience co-creation framework proposed by Jaakkola et al. (2015; see Figure 1).

Dimensions of service experience. Adapted from Jaakkola, Helkkula, and Aarikka-Stenroos (2015).
The framework divides the holistic phenomenon of the service experience into six dimensions to assist in the structuring of service experience studies. Below, each of the dimensions is discussed in detail based on Jaakkola et al. (2015).
The temporal dimension of the service experience reflects its dynamic nature; that is, an individual’s earlier experiences affect his or her valuation of the present service experience and are dynamically updated through new experiences (Heinonen et al., 2010). Interpretations of experience can, therefore, be examined either through the standpoint of isolated moments in the present or through a wider lens incorporating past memories and the foreseen future (Jaakkola et al., 2015).
The factual dimension of the service experience assesses whether the experience is truly lived or imagined by the focal individual. This is especially relevant in the case of expectations, as each individual forms a mental image of the future that may influence the evaluation of a service experience at a particular point in time. In health care, patients assess their experiences based on real-life events, such as current doctor appointments, but also on past appointments and concerns over future operations and illnesses.
The spatial dimension of service experience refers to the location in which the experience is created: in the service setting or beyond the service setting. Parts of the service experience emerge beyond the service setting, in a focal individual’s everyday life across all types of activities related to the phenomenon: ordinary, extraordinary, routine, mundane, and everyday (Heinonen et al., 2010). The other parts take place within the provider’s service setting, such as the hospital setting in health care.
The organization dimension assesses how service experience creation may actualize in dyadic or more systemic interactions among multiple actors. For example, patients with chronic illnesses usually embark on long medical journeys during which they potentially encounter systematically several different health-care professionals.
The locus dimension indicates that the service experience can be examined at the individual or collective level. For example, in pediatric health care, collectiveness can refer to a situation in which a child’s experience is created collectively through everyday interactions with his or her parents. Such a situation is also linked to the control dimension, which indicates that the service experience can be provider led or can emerge organically among patients and their relatives.
Method
Our study drew from three studies with different data collection methods conducted to examine experiences in children’s health care. The studies were part of a larger research project, LAPSUS, which aims to study the experiences of child patients and their families in the context of a children’s hospital. The research project and studies were approved by the ethical committee of the Hospital District of Helsinki and Uusimaa and are closely linked to the development and construction of a New Children’s Hospital (n.d.) in Helsinki, the Finnish capital.
In this article, we follow the interpretivist/constructivist approach, rather than the positivist research approach, to understand the world of human experiences and rely on participants’ views of the studied phenomenon (Creswell, 2003, pp. 7, 8). We conducted the qualitative research as a collective, instrumental case study with a phenomenological method, where the unit of analysis is the different data collection methods (Creswell, Hanson, Clark Plano, & Morales, 2007; Yin, 2003). We utilized an extreme case strategy with maximum variation sampling to select three different qualitative data collection methods for exploration (Patton, 1980, p. 105). We chose this approach to obtain broad data on different methods to analyze the benefits and limitations of each method and to compare their applicability to capture dimensions of the service experience. Furthermore, our approach enabled us to examine the topic from a research design level as our studies, in addition to utilizing different data collection methods, approached the service experience from different perspectives. The three selected studies were video diaries with child patients (Study 1), narrative interviews with parent(s) of a child patient (Study 2), and semistructured interviews with pediatric health-care professionals (Study 3; see Table 2). Method selection was based on the variability of data inquiry format and structure, perspective on the phenomenon, and temporal scope. Selected methods, therefore, were either structured or not, pure interview or a story, or comprised a mix of verbal, visual, and physical elements.
Overview of Three Studies for Exploring the Service Experience of Child Patients in Health Care.
aNumber of participating families from which one or two parents participated.
The studies were conducted from 2015 to 2016. The study participants were comprised of child patients, parents of child patients, and employees of two public university hospitals in Finland: the Children’s Hospital in Helsinki and the Department of Pediatrics and Adolescence at Oulu University Hospital (see Table 2). Eight of the participating children in Study 1 belonged to the same family as a parent participant in Study 2; the rest of the participating children, parents, or health-care professionals had no family or professional connection to each other. Having family and professional connections were not seen as important in this study as socially constructed experiences were examined in a higher dimensional level rather than examining one’s experience in-depth.
Study 1: Video Diaries With Child Patients
Video diaries were used to study the experiences of the child patients. The aim of the study was to determine how child patients express themselves and what they say about their experiences in their own words. When choosing this method, particular attention was paid to inspiring the child patients and acknowledging their vulnerability as participants (Gaver, Dunne, & Pacenti, 1999). To help the children express their feelings and experiences, the method was designed to allow the children to respond verbally, visually, and physically (Curtis et al., 2004; Sanders & Dandavate, 1999; Sartain et al., 2001; Wensveen, 1999). It was also hypothesized that the method’s playful approach would enhance motivation to participate (Mattelmäki & Battarbee, 2002) and reveal otherwise hidden knowledge (Buchwald, Schantz-Laursen, & Delmar, 2009; Noyes, 2004; Rich & Patashnick, 2002) about chronically ill children. In this study, the classic diary was modernized into a video diary, since contemporary children are accustomed to watching and producing video clips on web-video platforms like YouTube. To ensure that the participants would express their own thoughts and feelings, the sample was chosen from an older age-group (10–16 years old).
At the beginning of the data collection process, nurses at the children’s hospital contacted outpatients with chronic illnesses (rheumatism, diabetes, or inflammatory bowel disease). Patients and their parents were informed of the study and asked to participate. If they agreed, they were asked to complete a written consent form. A total of 34 families were contacted and 20 declined to participate (rejection rate: 59%). Children who were interested received a probe package, including a tablet for video diaries, a binder with tasks and instructions, three story cubes (with different pictures on each side to prompt storytelling), and a marker pen. The probe tasks were constructed to include playfulness (e.g., drawing and hobby crafting) and to prompt sensual, emotional, compositional, spatiotemporal, and social aspects of the children’s experiences. The probe task themes varied daily and included drawing a patient path, explaining daily routines related to the illness, and creating a collage demonstrating “[a] dream vacation in the hospital” (for detailed information, see Karisalmi, 2016; Karisalmi, Stenhammar & Kaipio, 2018). The 14 participants were asked to record daily video clips on the given themes or tasks for 9 or 10 days. Within 2 weeks of returning the probe packages, they also participated in face-to-face interviews to clarify and elaborate on their responses. The method and probe package were pilot-tested, and minor changes were made to elucidate the instructions and task descriptions and improve the order of the tasks (so that easy and more demanding tasks varied on consecutive days).
Study 2: Narrative Interviews With Parents of a Child Patient
The narrative interviewing method was used to study experiences in children’s health care and service experience dimensions of children from the perspective of child patients’ parents. Narrative interviewing was chosen as a method because narrative interviews reveal the storyteller’s experiences in story form, conveying meaningful events actualized in different locations and at different times (Helkkula & Kelleher, 2010). Therefore, this method enabled us to examine child patients’ service experience holistically and dynamically. It was hypothesized that, as parents are inextricably part of child patients’ care and social life, they could be used to study children’s service experience.
The narrative interviews with the child patients’ parents were carried out at the interviewees’ homes or workplaces (see Mannonen, Kaipio, & Nieminen, 2017). Participants provided informed written consent. The participants were comprised of 24 families, including both families with young children with congenital disorders and families with teenage children suffering from chronic illnesses (from which eight teenagers were participants in Study 1). These illness groups were selected because young children (younger than 2 years old) were the hospital’s largest patient group in terms of both resources and head count, and teenagers enabled comparisons between the experiences of the parents and the children in later phases of the research project. Participating families were selected in collaboration with the partner hospital, and families were first approached by the hospital. The rate of the rejections was not recorded. Interviews were conducted between winter 2015 and spring 2016, and each interview lasted 1–2 hr. In most families (14), only 1 parent was present, and in the remaining 10, both parents were present. The interviews were audio-taped and later transcribed verbatim. The interview structure was based on a modified version of the critical decision-making method (Klein, Calderwood, & Macgregor, 1989; Mannonen, Aikala, Koskinen, & Savioja, 2014; Mannonen et al., 2017). The four main themes covered were as follows: (1) a description of the incident or illness, (2) the construction of a time line for the incident, (3) an identification of related experiences and emotions, and (4) an identification of the communication tools used and partners and information sources consulted.
Study 3: Semistructured Interviews With Health-Care Professionals
The semistructured interview method was utilized with health-care professionals because it allowed us to focus on a particular theme and add depth to the interviewees’ answers (see Carney et al., 2003). Semistructured interviews were conducted with doctors (n = 11), head nurses (n = 4), and other nurses (n = 8) working at the Pediatrics and Adolescent Medicine Department at Helsinki University Hospital and the Department of Pediatrics and Adolescence at Oulu University Hospital. All approached hospital professionals agreed to participate and provided verbal consent for participation. Interviews were conducted between September and December 2015, and each lasted for about 1 hr. The interviews were audio-taped and later transcribed verbatim. Participants were selected to represent a range of professional groups and specializations (e.g., rheumatics, neurology, cancer ward, and pediatric surgery).
The interviews covered six themes: (1) participant background, (2) patient experience, (3) patient journey, (4) patient experience quality measurement, (5) organizational culture, and (6) “New Children Hospital.” The first three themes were designed to understand the health-care professionals’ views concerning the experiences of children and their families, and the last three themes were used later in the project. The patient experience theme included six questions: (a) define patient experience, (b) describe things that influence experience, (c) describe a good experience using three adjectives, (d) describe how health-care professionals can influence patients’ experiences, (e) describe how health-care professionals can influence parents’ experiences, and (f) describe things that are important for patients’ and parents’ experiences. The patient journey theme included seven questions: (a) interaction points in the patient’s journey, (b) emotional states at these points, (c) challenges in journey points, (d) things influencing flow, (e) memorable encounters with patients, (f) information-sharing during the journey, and (g) strengths and weaknesses of current way of operating.
Analysis of the Studies
Our analysis of the studies comprises two phases. First, we conducted a within-study content analysis for each of the conducted studies. Analyzed data included the filled binder, the video clips, interview transcripts from the video diary method, transcripts of narrative interviews, and transcripts of semistructured interviews. Our first-round analysis followed deductive approach and explored how the applied methods generated information on the dimensions of service experience. Each individual interview or personal data set was analyzed based on a predetermined framework and coding (Jaakkola et al., 2015; McCarthy & Wright, 2004) using a qualitative data analysis software. In addition, we analyzed each method’s applicability for studying service experience in children’s health care, including benefits and limitations. The applicability of each method was analyzed with respect to the method’s ability to capture the dimensions of service experience and the appropriateness of using the method with the selected sample through discussions among the participating researchers.
Second, we conducted a cross-study analysis of the three studies. The cross-case analysis process drew on discussion within the research team and was based on experiences and interpretations from the first round of analysis. The aim of the cross-study analysis was to identify differences and similarities among the studies concerning capturing the six dimensions of the model. Therefore, units of the cross-study analysis were dimensions of service experience and two factors within each dimension (e.g., broad–narrow time frame in the temporal dimension). Each dimension and its factors were analyzed independently through discussion to compare the studies.
Results
The studies revealed that the methods varied in the broadness and depth with which they captured the dimensions of the service experience of child patients. The following sections present the results of the studies, concentrating on the benefits and limitations of each method and how each method captured the dimensions of child patients’ service experience.
Benefits and Limitations of the Studied Methods
Video diaries with child patients
The data collected through the video diaries were verbally and visually rich, as the children reflected thoroughly upon their thoughts, feelings, and dreams through multiple pictures, screenshots, drawings, and daily video clips. The children mostly reported on school, family and friends, hobbies, and leisure time in their daily routines, suggesting that the child patients defined their experience through everyday events rather than through their illness. Such latent information might not have been revealed with more conventional and spontaneous methods (e.g., interviews).
Video diaries also captured the temporal dimension, as all informants described their past journeys and their encounters with different health-care professionals and other actors related to their illness. However, most of the children lived in the moment and worried about concrete, timely issues, such as food restrictions.
Some of the older children also described some imaginary experiences concerning the near future, such as how their illness would affect their high school studies and possible career options: topics more typical of adult interviews. These expressions of actual encounters with health-care professionals and future imaginary experiences imply that the video diary method can be used to capture the factual dimension of the service experience in children’s health care.
The rich data gathered through the video diaries included several different experience locations within hospitals and children’s everyday lives (e.g., home or hobbies). Therefore, the method captured the full spectrum of the spatial dimension of service experience. Related to the hospital locations, children recalled positive experiences with entertainment devices, board games, canteen snacks, and windows and negative experiences with the lack of privacy and medical equipment.
The children highlighted the importance of maintaining social relationships with hospital personnel and members of their everyday social environment, including family members, relatives, friends, and peers. This implies that the organization and locus dimensions can be captured using the video diary method with child patients. Concerning the control dimension, children expressed feeling that they had little control over service creation, including hospital visits, clinical procedures, and transfers among hospital units. Patient-led experiences were captured through children’s expressions of experiences in home settings and other locations outside the hospital setting, beyond the health-care service provider’s control.
Researchers utilizing this method may face challenges with their samples. The rejection rate in the video diary study was high, with 20 of the 34 contacted children declining to participate due to, for example, a lack of time, strength, or motivation. Teenage boys were especially unmotivated to participate. We believe that the sensitivity of the context, the lack of incentives, and the lack of familiarity with the video diary format as a research method and its laborious nature may have influenced children’s willingness to participate (see Karisalmi & Nieminen, 2017). Participants’ feedback on the method was contradictory; some participants appreciated the short daily time investment, while others would have preferred larger investments over fewer days. Because of these individual preferences, it is unclear whether a shorter time commitment would have improved the participation rate.
The high rejection rate in the video diary study may have yielded biased data, as all participants who did agree to participate were highly motivated to complete the study. Therefore, it is unclear whether unmotivated children with more severe illnesses, such as cancer, experience their illness and treatment differently. A few technical difficulties, such as noise, dim light, and the accidental deletion of some video clips, occurred during the study period but caused only minor issues in analyzing the data.
Narrative interviews with parents of a child patient
Narrative interviews with parents of a child patient captured the dynamic journeys of families with ill children through cumulative stories. Parents explicated family’s navigation through myriads of clinical and nonclinical care encounters and the effects of the illness on their everyday lives beyond the hospital setting. Their stories also revealed the service experience of the child patients, as parents expressed their estimations of their children’s experiences or reflected their children’s own testimonies. This implies that, to some extent, parents may serve as experts on their children’s experiences, at least for younger children. However, parents’ estimations may also be incomplete and/or biased. Children, especially teenagers, may hide feelings and thoughts from their parents that may limit parents’ views of their child’s experience. Furthermore, parents’ own emotions and their experiences related to the care may cloud their interpretations of their child’s experiences.
The narrative method fully captured the temporal dimension of the service experience. The parents’ cumulative stories both narrowly concentrated on meaningful events and broadly expressed how past and future experiences and scenarios influenced their own and their children’s experiences. The events the parents described included hearing the diagnosis, being excited to return to the hospital, and the medicines and care beginning to work. Concerning past experiences, parents described past unsuccessful encounters, but also how past experiences influenced their children by, for example, familiarizing them with operations or injections. Future experiences included uncertainty and concerns about future operations and life with the illness. The breadth of the information shared about meaningful events suggests that parents’ narratives are well-suited for capturing the factual dimensions of child patients’ service experience, as they included both lived and imaginary experiences.
The narrative interviews captured the full range of the spatial dimension through the parents’ stories, which included events in multiple locations, such as the hospital, school, social welfare sites, peer support sites, and families’ everyday life surroundings. Parents also reflected on the influence of a wide variety of actors, including hospital personnel, patient associations, other patients and families, relatives, and school personnel. These insights enabled access to the organizational dimension from the parents’ perspective and yielded useful data to examine different actors’ capacities to influence service experience creation beyond the hospital setting in children’s and their families’ everyday lives.
The parents’ narratives also captured the locus dimension of the service experience, as they described their children’s individual experiences from their own perspective, but also shared collective experiences within the family. This suggests that narratives are well-suited for revealing and examining both individual and collective levels of service experience in children’s health care.
With regard to the control dimension, the narratives revealed multiple events in which the control of service creation was in the hands of the service provider (e.g., surgery) but also events in which the control shifted to the patients and families (e.g., self-care, peer support). Thus, the control dimension was fully captured by the parent interviews.
Limitations concerning the narrative interviewing method include the inherent unverifiability of secondhand accounts and observations of actual encounters. Further, some parents found it difficult to review their experiences. This finding underscores the sensitivity of the studied context and the need to give particular attention to ethical considerations in these kinds of studies.
Semistructured interviews with health-care professionals
The semistructured interviews with the health-care professionals captured a generalized view of child patients’ service experience. The interviewed health-care professionals had several years’ experience in pediatric health care; therefore, they were able to provide an overall picture of children’s experiences. Health-care professionals reflected on the service experience of child patients through their professional perspective by describing service experience creation in doctor–patient and nurse–patient encounters in the hospital. The professionals’ lack of knowledge about the service experience of children and their families beyond the hospital setting limited the breadth of information captured by this method and sample.
Concerning the temporal dimension, the health-care professionals primarily described children’s service experiences through snapshots of encounters with patients and their families. The health-care professionals stated that some patients go through multiple wards and meet various health-care professionals during their care. The health-care professionals’ concentration on the hospital setting yielded rich data on the organization dimension.
Concerning the factual dimension of the service experience, the health-care professionals primarily described the patients’ and families’ actual lived experiences, including encounter situations, experiences of pain or painlessness, and waiting for appointments. The health-care professionals also gave examples of child patients’ imaginary future experiences, such as fears of dying and concerns about future operations.
The spatial dimension was captured only partially, as the health-care professionals concentrated on describing service experience within the hospital. The health-care professionals emphasized the importance of the hospital environment, including personnel’s clothing, technical devices, noises, colors, and playing areas, in providing a good service experience for children.
With regard to the locus dimension, the health-care professionals described the service experience as collective: a characteristic they considered specific to children’s health care. The health-care professionals expressed that, although clinical and nonclinical processes focus on the child patient, they are experienced by the whole family due to the family’s shared feelings and continuous participation. However, although the health-care professionals regarded the service experience as collective, they also emphasized the importance of seeing children as individuals and meeting their individual needs and concerns. Therefore, while the semistructured interviews captured both the individual and collective levels of the locus dimension, they concentrated purely on the hospitalization period, leaving a gap concerning the service experience beyond the hospital setting. This also applies to the information gained about the control dimension of the service experience, as the interviews with the health-care professionals yielded one-sided but detailed information on processes led by hospital personnel.
It is worth noting is that health-care professionals may give biased views of the service experience in children’s health care. Interviews were held in the workplaces of the health-care professionals, and participants may have felt the need to be a representative of the health-care organization that they worked for. This may have influenced participants’ will to answer questions in a socially desirable manner, causing bias. Health-care professionals may also be biased to answer in a manner that makes them look better. For example, data included little information about health-care professionals’ own errors that could have influenced the service experience. However, the interviewees did share some errors made by other health-care professionals. To minimize bias, we suggest conducting interviews with health-care professionals outside work.
Analysis: Summarizing and Comparing Methods
Our studies with different methods and sources imply that it may be extremely difficult to obtain a complementary view on the service experience of child patients by using just a single method or source, although each method has strengths. The video diary method provided rich data on the subjective service experience of the child patients on their everyday life and surroundings and provided insights into chronically ill child’s minds (see Table 3). The narrative method with the parents yielded data on the collective experience, providing insights into family dynamics in families with an ill child. Semistructured interviews with health-care professionals yielded data that provided an in-depth understanding of hospital processes that construct the patient experience.
Lessons Learned From Studies on the Service Experience of Child Patients.
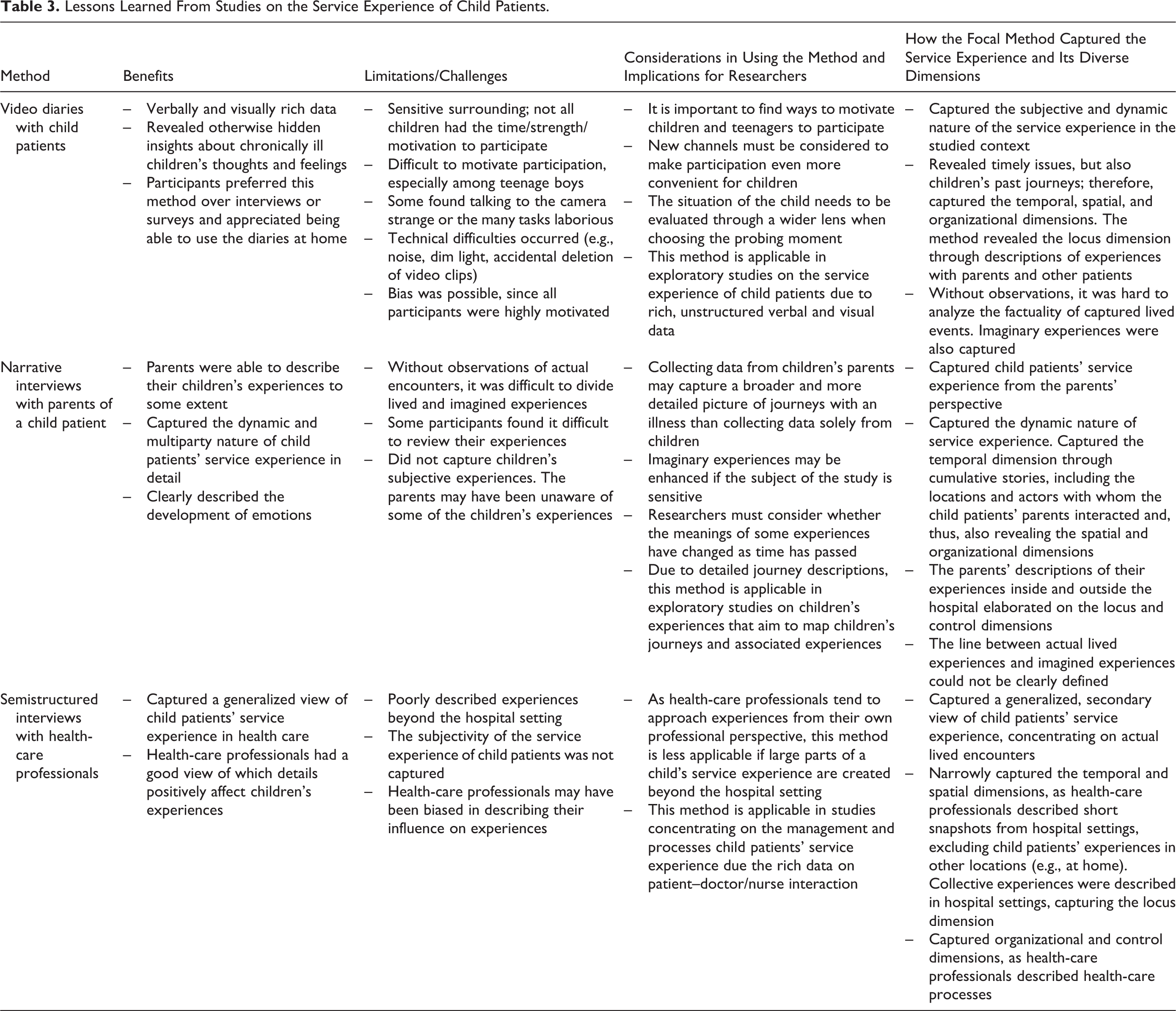
The video diary method with the child patients and the narrative interviews with parents of a child patient were both useful for capturing the dynamic nature of service experience and the broad temporal dimension. Patients and their parents both described their care and life with an illness from a temporally broad perspective and elaborated on how some previous experiences influenced later experiences. Comparing to these two methods, the semistructured interviews with the health-care professionals yielded more temporally narrow information, focusing primarily on hospitalization periods and overlooking information on self-care and other experiences in patients’ everyday life surroundings. Therefore, researchers using only semistructured interviews with health-care professionals can only partially capture the service experience of child patients. Video diaries and narratives, by comparison, can each capture the full spectrum of the temporal dimension.
Concerning the factual dimension, the narratives and the video diaries captured future imaginary experiences, such as concerns about future life with an illness. However, the parents’ interviews yielded much deeper information, as the children tended to concentrate on present issues. Compared to these methods, the semistructured interviews with the health-care professionals concentrated more on lived actual encounters, such as appointments and clinical procedures. However, analyzing methods’ applicability for capturing the factual dimension of child patients’ service experience in health care is problematic as, without observation, it is hard to clearly show which experiences were actually based on past lived encounters and which were imagined by the informant.
Both the narrative interviews and the video diaries captured the spatial dimension of child patients’ service experience beyond the hospital setting. The narrative interviews with the child patients’ parents yielded comparatively deeper and broader data on the spatial complexity and multiparty nature of the service experience of child patients in health care. Video diaries completed at home, however, encouraged children to describe their experiences beyond the hospital settings, including events in school and through hobbies.
All methods captured both levels of the organizational dimension of the service experience in children’s health care. Service experience evaluation through systemic interactions was emphasized across all collected datasets. The locus and control dimensions were also captured in all studies. However, data collected through semistructured interviews with health-care professionals concentrated mainly on the hospitalization periods, providing little information on patient-led experiences. Table 4 presents which dimensions of service experience were captured (marked as x in the table) in each of the study.
Service Experience Dimensions That Were Captured in Each Study.

We acknowledge that our study has limitations. Our research design enabled us to examine the capability of different methods to capture the dimensions of service experience and to examine how a child patient’s service experience can be captured through different informants, two factors that influence the ability to capture the multidimensional service experience. Hence, this study went beyond simple method comparison to the higher research design level, and it may be expected that some of the results were more related to the informants, but rather the method. For example, we expect that the detailed data from the narrative interviews on spatial complexity and the multiparty nature of service experience might have been related to the use of parents as informants rather than the narrative method. Therefore, having constant participant type in all three studies may have provided different results. The generalizability of our findings may be limited due to cultural and societal differences. All our study participants were Finnish citizens; therefore, we cannot conclude whether willingness to participate and share sensitive experiences differ based on cultural background. Early childhood education in Finland relies on playful learning methods, which may have facilitated our ability to implement playful video diary tasks. We also acknowledge that Finland’s public tax-funded health-care system may have influenced the patients’ experiences, potentially limiting our findings’ applicability to countries with strong private health-care sectors. The possible influence of public versus private health care could be investigated in future studies.
Conclusions
Theoretical Contributions
The study was conducted to increase our understanding of the qualitative methods used to study the multidimensional service experience in children’s health care, which is considered a complex research topic due to its subjective, unique, and dynamic nature (Zomerdijk & Voss, 2011).
First, the study contributes to qualitative method research by conducting three studies with different data collection methods and comparing how each captured a contemporary phenomenon: service experience. We extend knowledge from previous studies by showing that children are able to express their experiences through the playful, unstructured video diary method. These results reflect those of Curtis et al. (2004), who also found that playfulness and flexibility in research methods supports child patients’ ability to describe their experiences. Our finding that child patients are capable of expressing their experiences in their everyday life surroundings, however, contradicts the findings of Sartain, Maxwell, Todd, Haycox, and Bundred (2001), who found that children had difficulties expressing their experiences in home settings. Hence, it could be hypothesized that playful, temporally and spatially flexible methods may help children express themselves and yield a deeper understanding of children’s experiences, particularly in sensitive and invasive services (see Lovelock, 1983).
Second, the study contributes to experience research by providing novel structured knowledge on experiences in the setting of children’s health care. The methods can be implemented in other contexts to gain broad, in-depth information on experiences created beyond the service settings and among the different actors (Banerjee, 2014). Our study went beyond simple method comparison and examined three different informant groups that may provide experience data on the service experience of child patients. Moreover, this study appears to be the first to apply and empirically examine the service experience dimensions presented by Jaakkola et al. (2015). Our study contributes to the service experience research (Danaher & Gallan, 2016; Frow et al., 2016) and suggests that the dimensions of the service experience in health care elaborate: a broad temporal dimension, a spatial dimension including both the service setting (hospitals) and far beyond (home, school), a systematic organizational dimension, strong imaginary experiences in the factual dimension, a collective locus dimension, and a control dimension including both provider-led to patient/family-led services.
Implications for Researchers and Practitioners
Video diaries seem to suit studies aiming to explore children’s service experience. When choosing probing and video diaries as a method, the method’s appropriateness for the participants must be considered. Children’s situations must be evaluated through a wider lens, since the video diary method can be time-consuming to complete. Children, especially high schoolers and children with many hobbies, may not have time to complete the requisite tasks; therefore, the method may not always be suitable. To address this issue, researchers may consider increasing the method’s time flexibility.
Through narrative interviews, the patients’ parents were able to describe the entire span of interactions and encounters better than their children. This helps researchers map temporally prolonged experiences in detail but may also imply that parents’ assessments of their children’s experiences differ from the children’s own assessments (see Savage & Callery, 2005). However, narrative interviews with children’s parents may be useful for studies aiming to map children’s experiences and influencing actors, as well as for exploratory studies concentrating on the experiences of children in sensitive contexts, as they may be more convenient to implement than methods involving collecting data from children. We encourage researchers to complement their understanding of service experience in health care using data collected from both child patients and their parents. Although this does not triangulate the validity of subjective experience, it may increase researchers’ understanding of the collective nature of the phenomenon, which is hard to achieve using a singular perspective.
Interviews with health-care professionals seem well-suited for studies concentrating on developing health-care service providers’ actions to shape patients’ service experience. This method should be used cautiously, however, if a large part of the patient’s experience is created beyond the provider’s service setting (e.g., in illnesses in which self-care plays a major role). In these contexts, provider-side professionals may provide only partial information, resulting in a narrow picture of the phenomenon. The use of video diary or narrative methods with individuals, children, or adults can help address this issue by providing patient perspectives and information beyond the service setting. In addition, the use of multiple methods and samples may enable researchers to zoom in and out on the phenomenon, depending on whether the study focuses on isolated moments or a broader temporal perspective.
Future Research Agenda
Future research concerning methodological insights into children’s experiences could test how different technologies, gamification, and interactivity can be used to solve problems collecting the experiences of younger children, especially children at a low developmental stage with undeveloped language skills, through reading and supporting children’s storytelling ability. The video diary method study revealed problems motivating children to participate. Further studies are needed to learn how to motivate children to participate in research. Papers that tackle these issues could assess new methods and channels to make it easier and more convenient for children to participate (see Karisalmi & Nieminen, 2017). Furthermore, our study examined a limited set of three purposefully chosen methods. The methods and our findings can be adopted into research and practice to improve the holistic service experience of child patients, not only within the hospital setting but also beyond it. However, we strongly encourage researchers from different disciplines to investigate the service experience of child patients using varying methods to advance this field of science even further. Finally, our three methods involved participants with little connection to one another (i.e., links existed only between some of the children participating in the video diary method and their interviewed parents). It would be interesting to study the experiences of children, their parents, and even their nurses to determine whether their experiences are cohesive or different.
Footnotes
Declaration of Conflicting Interests
The author(s) declares no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) discloses receipt of the following financial support for the research, authorship, and/or publication of this article: LAPSUS—Renewing Hospital for Children and their Families is a research project funded by Business Finland (former Tekes; grant numbers 40298/14 and 40297/14).