
Abstract
Background:
Global cases of overdose-related deaths attributed to synthetic opioids are reaching epidemic proportion in many jurisdictions. While the main focus of health agencies and the different levels of government has been to combat the cases linked to injection drug use, the deaths attributed to smoking illegal drugs have not gained the same attention. Moreover, little attention has been given to the role of people with past or current experiences of illegal drug use and how their social networks can mitigate the risk of a highly stigmatized behavior such as smoking illegal drugs.
Methods:
The study concerns the first social network research conducted via a community-based participatory action methodology in two distinct urban (Vancouver) and rural (Abbotsford) centers in British Columbia, Canada. The study will identify the influence of social networks on people who smoke illegal drugs (PWSID) and their adherence to interventions aimed at reducing harm. Through community consultations, members of the Vancouver Area Network of Drug Users and the British Columbia/Yukon Association of Drug War Survivors not only assisted with the design of this research project but also assisted with the data collection, management, protection and entry of demographic, and network information.
Discussion:
Many traditional qualitative and quantitative methods have not effectively engaged people who use drugs as researchers or collaborators due to stigma related to illegal drug use. The aim of this study is to recognize that everyone within the network of PWSID is a few steps away from harm. Therefore, we aim to reduce the harm associated with smoking of illegal drugs, especially for PWSID that are at the highest risk. At the same time, we hope that the social network research via a participatory community-based approach will mobilize PWSID in the process and offer a different method of knowledge construction from the traditional positivist approaches.
Keywords
What Is Already Known?
We know that people who use drug are the health “experts”; therefore, we have taken a community-based participatory action approach to this project. We know that synthetic fentanyl and analogues related fatalities have been reported in literature for people who smoke illegal drugs.
What This Paper Adds?
We are the first study to date to employ the community-based participatory action research using a social network methodology because it both involves community organizations and vulnerable participants and unites the researchers with focused on community action to address the growing synthetic overdose epidemic. Moreover, this is the first research to consider the social network of people who smoke illegal drugs.
Background
The burden of illegal drug use and related cost on the health care and the local communities has never been more acutely felt than the current wave of synthetic opioid overdose fatalities in Australia, Canada, the United Kingdom, and the United States (Ciccarone, 2017). The majority of interventions regarding the use of illegal drugs target injection use, with few resources and little attention given to people who smoke illegal drugs (PWSID). In fact, previous researchers highlighted the need for immediate harm reduction interventions for PWSID even before the introduction of synthetic fentanyl and analogues in the illegal drug markets (Jozaghi, 2014a; Jozaghi, Lampkin, & Andresen, 2016; Voon et al., 2016).
Recent research from Surrey, British Columbia, Canada, identified a cluster of opioid overdoses in people who smoked crack cocaine was due to contamination with synthetic opioids, and previous research from the United States have shown that cocaine, crack cocaine, and methamphetamine could have potential lethal effects even when used through smoking (Klar et al., 2016; McCall Jones, Baldwin, & Compton, 2017). Moreover, there has been research that points to the growing evidence that hepatitis C virus (HCV) and even HIV can be transmitted through contaminated pipes through sharing when PWSID have open wounds or oral lesion in their mouth or lips caused by broken or hot glass pipes (Celentano & Sherman, 2009; Fischer, Powis, Cruz, Rudzinski, & Rehm, 2008; Haydon, & Fischer, 2005). Research has documented that PWSID are at 4.01 and 3.87 odds of acquiring HIV and HCV, respectively (DeBeck et al., 2009; Nurutdinova, Abdallah, Bradford, O’Leary, & Cottler, 2011).
Literature
Previous studies in the area of marginalized, stigmatized, criminalized, and at-risk groups have relied on traditional qualitative and quantitative methods to reach these groups and their networks (Phukan et al., 2017). Jacques and Wright’s (2015) qualitative research for example showed how the illegal drug market and the network of producers to traffickers and to consumers operated. A recent quantitative research by Malm, Bouchard, Decorte, Vlaemynck, and Wouters (2017) also demonstrated the link between illegal marijuana growers, their networks, and the risk of apprehension. Moreover, quantitative research by Bouchard, Hashimi, Tsai, Lampkin, and Jozaghi, (2018) has shown the harm reduction network of people who inject drugs and the link between peers and the harm reduction strategies. However, to our knowledge, social network inspired methodologies have not previously been implemented with PWSID, especially in the current climate of synthetic opioid epidemic where drugs adulterated by fentanyl are reported in the illegal markets and are becoming the “new norm” (Ciccarone, 2017; Klar et al., 2016; McCall et al., 2017). In addition, although traditional methods facilitate inferential statistics on the larger population from which the sample is drawn, there are many limitations of the methods that have raised a lot of discussion in the academic community (Broadhead, 2008; Lansky & Mastro, 2008; Ouellet, 2008; Scott, 2008). For example, there have been concerns related to tokenistic involvement of marginalized participants and associated underground economy, risk of violence, coercion, or false reporting (Closson et al., 2016; Logie, James, Tharao, & Loutfy, 2012; Richardson, Wood, & Kerr, 2013; Scott, 2008).
Since the main successive component of the traditional social network methodology’s sampling strategy has been focused on “peers” or “seeds,” mainly based on the notion that such individuals are better able to locate and access the hard-to-reach populations than outreach workers or experienced researchers, we believe that better outcomes can be achieved if peers or people with lived or current experiences of illegal drug use not only act as a referral point but also be invited to partake in the research design, implementations, data collection, data entry, and dissemination of findings in the community (Brizay et al., 2015; Greene, 2013; Jagosh et al., 2012; Wright, 2015). In fact, there is growing interest by health researchers to give greater roles to people affected by the health problems under study (Boyd, 2013; Boyd, Murray, & MacPherson, 2017; Closson et al., 2016; Cropper et al., 2010; Greer et al., 2016; Wright, 2015).
This study aims to examine the implementation of community-based participatory actioned research (CBPAR) in the realm of social network. We are the first study to our knowledge to employ CBPAR using a social network methodology, which involves community organizations and people living in vulnerable situations to address the growing synthetic opioid overdose epidemic. We believe that CBPAR approach has many benefits, as it can influence policy and also educate and mobilize members of the community who are affected (Bush et al., 2017; Damon et al., 2017). In effect, CBPAR suggests that “science is more than adherence to specific epistemological or methodological criteria; it is primarily a means for generating knowledge to improve people’s lives” (International Collaboration for Participatory Health Research, 2013, p. 5). Participatory community-actioned approaches have been utilized in the area of public health previously with positive outcomes (Freifeld et al., 2010; Olsen & Banwell, 2013).
We employ CBPAR approach for the following justifications. First, we believe that the most significant benefits of CBPAR implementation in the realm of social network are enhancement and strengthening of cooperations, colearning, and collective action between researchers and PWSID who live a context of vulnerability (Cornwall, 2008). Second, implementation of CBPAR via social network would improve the quality of the network information’s design, details, and accuracy that fit the local context (Stoecker, 2013) because it is locally situated and it “closes the gap between people’s lived realities, science, and questions of policy” (International Collaboration for Participatory Health Research, 2013, p. 9). In effect, the local knowledge of peer researchers and supervisors about the drug culture and their familiarity with participants will provide rich and detailed network information that would not have been possible via traditional social network research.
Moreover, PWSID may provide more detailed information about their networks and their drug use patterns to peer researchers when compared to staff because they can relate to the peer researchers at a personal level. In fact, drug use patterns have been historically underreported in traditional surveys due to stigma and the illegal nature of the behavior (Harris, Shaw, Lawson, & Sherman, 2016; Hunt et al., 2015). Finally, social network research conducted through the CBPAR could give PWSID a sense of collective ownership over the research project (Stoecker, 2013). PWSID have historically been stigmatized and criminalized for their relapsing chronic medical condition (Jozaghi et al., 2016), but through this research project, they have gained short-term employment, learned new knowledge and skills, and advocated for the members of their community (Israel et al., 2010).
Rationale and Focus
While morbidity and mortality as a consequence of illegal drug smoking is a serious public health issue, little information is available regarding the profile of PWSID who are at the greatest risk. By establishing that everyone within the “connected region,” that is, within the network of PWSID is a few steps away from harm, we aimed to reduce the risk of overdose and other drug-related harms to those who are at the highest risk. At the same time, we are hoping to understand how the structure of the harm reduction network for PWSID is associated with the local context in which harm reduction services are delivered. The harm reduction networks depend on harnessing the power of peer harm reduction connections through mobilizing, educating, and disseminating knowledge which is tailored to the local needs of PWSID. However, it is important to emphasize that the illegal drug use stigmatization is linked to situations of vulnerability that is associated with a broader social determination rather than individual choices alone. Therefore, this study has engaged and provided employment to people with lived or current experiences of illegal drug use as researchers in their communities. The community organizations that provide peer-based models of health care to at-risk individuals and who suffer social exclusion processes have been involved in consultations, design, and implementation of this research project. Our main objective, as with any participatory research, was to mobilize, transform, and strive for evidence-based harm reduction solutions that would be generalizable to other jurisdictions with similar challenges. More specifically, the research is exploring the following questions:
Description of the Method
Recruitment
The study consultation with community groups in Abbotsford and Vancouver began in 2016. The British Columbia/Yukon Association of Drug War Survivors and Vancouver Area Network of Drug Users board members approved the research proposal and provided input to improve the questionnaire and the oral consent. The peer researchers were selected through community advertisements in Abbotsford and Vancouver via posters that were distributed by members of the drug-using community. The recruitment process was focused on providing low-barrier hiring opportunities to PWSID who have historically been excluded from paid initiatives in the research area (Coupland, & Maher, 2005). Ten peer researchers were selected in Abbotsford and seven peer researchers from VANDU. The peer supervisor at Abbotsford was appointed based on her extensive experience and deep connections to the neighborhood. Two peers were selected to share the peer-supervisor role at VANDU following an application process and interviews.
Ethics
The University of British Columbia’s Behavioural Research Ethics Board approved this research project (study #: H16-01580). This research is funded through the Canadian Institute of Health Research postdoctoral fellowship (201511MFE-358449-223266). Since social network research requires both respondents and their contacts be named, we have established procedures to protect the participants’ confidentiality and data analysis that can ensure research participants’ information are protected (Kadushin, 2005). Incentives for the peer researchers to complete the training included changing the top-down paternalistic approach to research, to a more participatory and respectful approach where “people who use (or have used) drugs should have a voice in shaping polices and interventions that affect their lives” (Peer Engagement and Evaluation Project, 2018, p. 3).
Sampling and Training
First, the peer researchers received 10 hr of paid training (Can$10 per hr) by a postdoctoral fellow related to confidentiality, anonymity, obtaining informed oral consent, and the right to withdraw. They were also presented with real-life scenarios to examine their learned knowledge. The peer researchers then received training on collecting demographic information and administering the social network questionnaire.
In line with previous research in this realm (Bouchard et al., 2018), peer researchers were trained to read the quote: I would now like to ask you some things about your contacts or friends with which you may practice harm reduction when you smoke illicit drugs. Please note that any information you provide about your contacts or friends such as their medical condition, years of drug use or the drug they use is based on your perception. This information may not be based on the actual fact. This information will be destroyed after the names and other information have been turned into numbers
Peer researchers were instructed to remind the participants that they can use someone’s street name or the handle they use to identify themselves in their social networks. Peer researchers were encouraged to practice administering the consent and questionnaire with another peer researcher until they felt comfortable distinguishing an informed oral consent, the right of refusal, and what coercion looks like. Each paid training sessions included printed copies of lectures, refreshments, fruits, and vegetables. The overall goal of training was to rely on the lived experiences of peer researchers while providing equitable, respectful, and low-barrier training (Closson et al., 2016).
Peer researchers were provided with official ID tags with the University of British Columbia’s logo, back packs to carry the questionnaires, notebook, pens, chocolate bars, bottles of water, a receipt booklet to administer the signatures for participants’ reimbursement, and “mental health cards” containing emergency mental health and free mental health drop-in centers contact information for participants who may feel overwhelmed. Each peer researcher’s note book was used to write the time, date, first name, the location, and a statement that oral consent was obtained. Eight of the original 10 peer researchers at Abbotsford successfully completed the 10 hr of the ethics training for the data collection. Six of the seven peer researchers at VANDU successfully completed the ethics training in Vancouver. The peer supervisors were trained on data management, data entry, and data protection. Peer researchers were provided with Can$10 cash to pay and reimburse each participant for their time after the participants signed the receipt booklet. Peer researchers were provided with Can$20 for returning each completed survey to the administration offices. In addition, one-time reimbursements of Can$25 were provided to peer researchers for their cell phone cost to ensure their safety. One of the peer supervisor in Vancouver was also provided with a personal laptop. Data collections in Abbotsford and Vancouver have been completed, but data entry is still ongoing by peer supervisors in both areas.
Application/Process of the Method
The peer researchers in both Abbotsford and Vancouver were instructed to approach people they knew in their established network, who use illegal drugs mainly via smoking, were 19 years or older, and who the peer researchers feel comfortable interviewing. In addition, the peer researchers in both Vancouver and Abbotsford were encouraged to discuss between themselves what locations they will target for the survey and who already have been interviewed in their networks so that the same people would not be interviewed for the second time.
The study procedures, payments, and recruitment were amended based on the recommendations of the peer-research supervisors. The questionnaire involved three components: demographic information and medical history; drug use and criminalized behavior; and social networks. The demographic part involved the anonymized information on the self-reported characteristics of participants such as their age, gender, relationship status, and ethnicity or race. Respondents were asked about their medical history, their drug use habits involving smoking and risky behavior. Drug use and criminalized behavior were related to their drug of choice, whether they ever overdosed, number of years that they have smoked illegal drugs, money spent on drugs, training on naloxone and CPR, use of naloxone, sharing, lending or borrowing pipes, and illegal drug use in public places. In addition, questions related to criminalized behavior such as receiving tickets by police, being victimized by other people who use drugs (PWUD), drug dealers, or police were asked. The complete lists of questions are shown on Table 1.
Itemized Question for the Demographic Section of the Questionnaire.

The social network component of the survey measured three network criteria: a respondent’s list of contacts and their basic attributes, the harm reduction-specific attributes of a respondent’s close contacts, and the connections between a respondent’s contacts. Table 2 provides the list of the demographic, drug use, medical condition, and the length of relationship as it pertains to the personal network of each respondent. For example, respondents were asked to provide information about their contacts’ perceived behaviors. These include years of drug use, drug of choice and if they still use drugs, whether the respondent considered the contact as a mentor, and the building where their contact resided.
A Respondent’s List of Contacts and Their Basic Attributes.

Table 3 demonstrates how a respondent identified their closest contacts with whom they share harm reduction knowledge and practice harm reduction behaviors. This could include harm reduction supplies, harm reduction locations, detox centers, and other harm reduction interventions in last 12 months.
The Harm Reduction-Specific Attributes of a Respondent’s Close Contacts.

Table 4 demonstrates how a respondent showed the connections between each of their contacts by providing information regarding which of their contacts in their personal network knew each other.
The Connections between a Respondent’s Contacts.
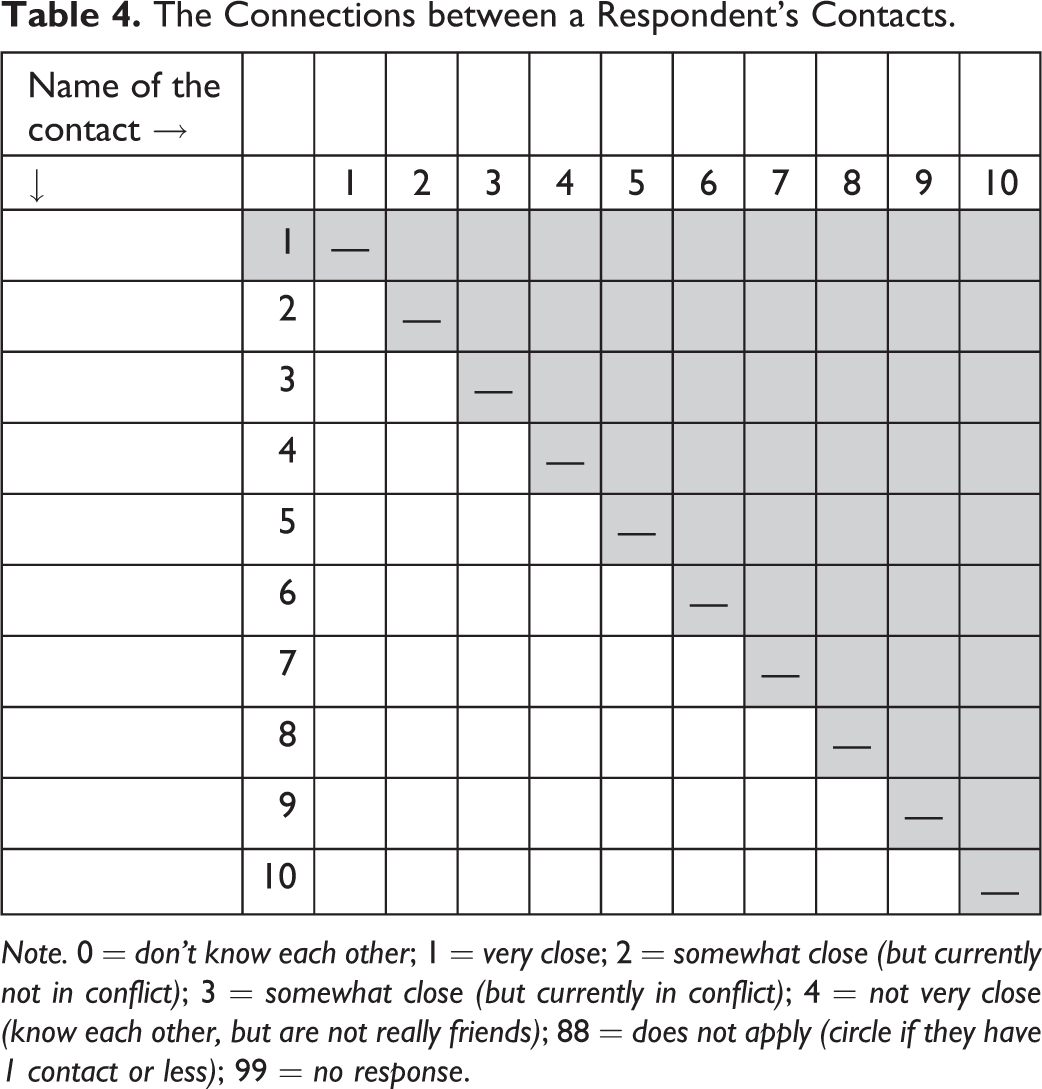
Note. 0 = don’t know each other; 1 = very close; 2 = somewhat close (but currently not in conflict); 3 = somewhat close (but currently in conflict); 4 = not very close (know each other, but are not really friends); 88 = does not apply (circle if they have 1 contact or less); 99 = no response.
Data Analysis
The data entry for demographic and network information provided on Tables 1 through 4 is in progress by the peer supervisors in Abbotsford and Vancouver. One of the primary objectives of this research project was to link the name and systematically verify the connected individuals with the network members. The easiest way to match names would be where the full names and demographic attributes match perfectly. In cases where network members identified by respondents have the same, or similar names, we have employed mixed substitutes and confirm with peer researchers and peer supervisors who know many of PWSID in their communities to orderly distinguish between each respondents and their contact they name in the surveys.
The data analysis for the network characteristics will be determined using specific social network analysis software (e.g., organizational risk analyzer [Borgatti, & Everett, 2000] for visualization of the network and UCINET, version 6. [Carley, Pfeffer, Reminga, Storrick, & Columbus, 2013] for the primary network analysis). For the demographic data, once all the data entry has been completed, we will use descriptive statistics and bivariate comparisons for respondents across the sites, taking into account the rural versus the urban centers. In line with the previous network research, we will analyze the network density and periphery and the actual size of the core-based minimum residual method algorithms (Carley et al., 2013). Finally, the nodes or the articulation points that hold the connected components of the network together will be determined via the algorithm that performs across all the articulation points in the graph.
Discussion
Through the first community-based participatory collection of detailed network information from PWSID, this study examines social support through informal harm reduction peer social networks and whether the network encourages PWSID to partake in activities that reduce the risk of illegal drug-related harm. Being the first social network research to examine the risks of PWSID, this study is likely to make a significant contribution to applying the knowledge from social capital literature to implement or offer an intervention that will saves lives and prevent diseases in the affected communities. Moreover, considering the nature of rural versus urban settings in this research will offer a wide range of possibilities that can provide us a better understanding of how to remove PWSID from harmful and risky behaviors. The result of this study could allow health policy makers to identify the people who are isolated, those lacking close support networks and those further from the core of the harm reduction networks. Thereby, this study has the potential to offer practical solutions to design ways to bring at-risk drug users and disfranchised PWSID closer to harm reduction and support networks, where opportunities for harm reduction and preventative measures can be made possible through peers and health professionals.
This methodological approach to social network research utilized in this study is pioneering. For example, in this research, we offer a more pragmatic approach to social network data collection that also considers community mobilization rather than traditional tokenistic approach to research within the social network data collection that reinforces the stigmatization of PWUD. In addition, by relying on the Social Exclusion Knowledge Network (2008), where exclusion/inclusion is “characterized by unequal access to resources, capabilities and rights which leads to health inequalities” (p. 3), we offer opportunities for future researchers to better engage and provide more capacity-building opportunities.
We believe that capacity building through CBPAR and network research will enhance the facilitation of the alliances between the harm reduction community services, health-care education through peers, and other broader social movements. Ultimately, research that engages the community has the potential to orient the tackling of the vulnerability for PWSID who are “steps away from harm” in their connected regions of social network through promoting the peer health that will become an essential component of sanctioned public health model. But like any new methodological approach, this study has a number of limitations. First, similar to all CBPAR, we attempted to maximize consultations with community organizations and PWSID in the design of the study, the research instruments, and the study implementation; however, financial and administrative costs were limited to those described above. Second, the remuneration design and the procedure do not fit well with the participatory research since a true CBPAR involves “the recognition that co-creative, collective process of knowledge generation requires facilitation” and it is usually implemented from bottom-up approach” (International Collaboration for Participatory Health Research, 2013, p. 16). However, despite the remuneration design being a limiting factor, we believe the procedures implemented in this research follows Collins et al. (2017) recommendations related to compensations and it fits well with the vulnerability, sensitivity, and the marginalization of PWSID (Closson et al., 2016). Finally, the issue of mobilization and engagement has been well described by people with lived or current experiences of drug use (Peer Engagement and Evaluation Project, 2018; Peer Engagement Principles and Best Practices, 2017); however, due to the nature of social network research and the request by the ethics board for data reduction policy of top-down approach, the community empowerment of PWSID may be difficult to achieve.
Despite the shortcomings noted above, the participation of PWSID in the data analysis, although limited, has not reduced the potential of the work of researchers in implementing CBPAR. At this stage, the steps taken to reduce the top-down approach, such as recruitment and training of peer researchers and their community supervisors, was part of the process and the products generated in the research is a testament of the success of social inclusion of PWSID. For future research in this field, we recommend the possibility of increasing the participation of the community researchers such as PWSID to validate the findings and assist in knowledge dissemination while at the same time enhancing the internal validity of the research findings. At the end of the data collection and analysis phase, the researchers of this study have planned for a social event where all community researchers will be acknowledged through certificates of appreciations for their research activities. This community event will also enable everyone to share their research experiences and at the same time provide the opportunity for the team to distribute the findings to facilitate the internal validity goals. Therefore, future researchers in the field of social network should not only employ PWUD but offer capacity-building opportunities in academic writings, authorship, media training, computer training, grant writing, and policy work. We also suggest that the peer engagement and community activism by harm reduction peer networks will be a key factor in the formation of harm reduction initiatives that could potentially save countless lives by targeting PWSID that tend to be more isolated from the harm reduction networks due to stigma and criminalization (Jozaghi et al., 2016; Palamar, Davies, Ompad, Cleland, & Weitzman, 2015). This goal can be achieved by further research via CBPAR in the area of public health, epidemiology, and harm reduction (Bach, Jordan, Hartung, Santos-Hövener, & Wright, 2017).
Footnotes
Authors’ Note
This study protocol has received ethical approval from the University of British Columbia’s Behavioural Research Ethics Board (Study approval #: H16-01580). The design, methodology, and approach in this study protocol by authors are not influenced or directed by the funding agency, the Canadian Institutes of Health Research (CIHR). The research goals and approach or possible research outcomes and recommendations of this study may not necessarily express the views of the CIHR or the BC Centre for Disease Control (BCCDC).
Acknowledgments
We would like to thank the Vancouver Area Network of Drug Users (VANDU) and the British Columbia/Yukon Association of Drug War Survivors for approving the project’s earlier proposal in 2016. In addition, we are thankful to SARA for Women in Abbotsford and VANDU in Vancouver for providing their space, staff, members, and resources for training the peer researchers. Finally, we would like to thank VANDU and UBC staff members for their contributions to this ongoing community-based research project. We also would like to thank the BCCDC support for facilitating the printing of surveys, consent statements, lectures and other research items.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study is supported by the Canadian Institutes of Health Research Postdoctoral Fellowship (201511MFE-358449-223266).