
Abstract
Background
Balloon guide catheters (BGCs) have been associated with higher rates of first pass effect (FPE) in endovascular thrombectomy. Large-bore aspiration catheters (ACs) placed at the face of the embolus may mimic the flow arrest effect seen with BGCs; combined use and its effect on FPE have not been previously well-studied. This study aims to evaluate the impact of this dual-device strategy on achieving FPE.
Methods
We conducted a retrospective cohort study across three sites (2018–2024). A multicenter registry was queried for adult patients with anterior circulation acute ischemic stroke treated with thrombectomy. The primary outcome was rate of FPE (modified Treatment in Cerebral Infarction (mTICI) 2C/3 on the first pass). Multivariable logistic regressions for likelihood of FPE were performed.
Results
973 patients were included, with a median age of 69 years (IQR 59–79). BGCs were used in 26.3%. Large-bore ACs were used in 68.7%. In most cases, large-bore ACs were used without a BGC (BGC-: 77.5% vs. BGC+: 43.8%, P < .001). FPE was achieved in 3—0.6% of procedures. BGC usage was significantly associated with FPE (aOR: 1.94, 95% CI: 1.01–3.72, P = .04). When sub-stratified by BGC use, large-bore AC use was found to be significantly associated with FPE only when a BGC was not used (aOR: 3.34, 95% CI: 1.01–12.14, P = .04).
Conclusion
BGC use is associated with an increased likelihood of FPE; when BGCs were not used, large-bore ACs were significantly associated with a higher likelihood of FPE. These findings are important when considering which tools contribute to successfully achieving FPE.
Key messages
Introduction
In anterior circulation large vessel occlusion acute ischemic strokes, rapid treatment and reperfusion are essential to ensure favorable clinical outcomes. 1 First pass effect (FPE) is defined as a single pass of a device with complete revascularization of the occlusion.2–5 Patients in whom successful FPE is achieved have been found to have higher functional independence rates, reduced mortality, reduced symptomatic hemorrhage, and decreased neurological worsening.6–9
Balloon-guide catheters (BGCs) have been used in thrombectomy for proximal flow control with favorable performance. 10 With advancements in technology, new large-bore (inner diameter ≥0.070”) aspiration catheters (AC) have been introduced.11–15 While previous studies demonstrate that the chance of FPE is higher with BGC use, and separately with large-bore AC use, there is limited data on the use of both large-bore ACs in tandem with BGCs.16–21 It is hypothesized that increased rates of FPE with BGCs may be buffered by the use of a distal large-bore aspiration catheter at the face of the clot, which may mimic the flow arrest affect seen with BGCs. With this assumption in mind, it is unclear as to whether the use of a BGC in conjunction with a large-bore AC provides any added benefit. This study aims to analyze the relationship between BGCs, large-bore ACs, and FPE to determine which procedural tools during the thrombectomy may lead to overall better clinical outcomes.
Methods
De-identified data may be made available upon reasonable request to the corresponding author. This observational study was approved by the institutional review board with waiver of informed consent at each institution. This analysis was reported per STROBE guidelines.
Patient selection
A multicenter registry (2018-2024) was queried for adult ischemic stroke patients across three comprehensive stroke centers in the United States. The inclusion criteria were patients presenting with an anterior circulation stroke (internal carotid artery [ICA], middle cerebral artery [M1, M2, and M3/M4]) treated with mechanical thrombectomy. Patients who did not have complete procedural data were excluded.
Outcomes
The demographic data included age, sex, comorbidities (hypertension, diabetes, atrial fibrillation, hyperlipidemia, and prior stroke), antiplatelet/anticoagulant use prior to hospital admission, and tobacco use. Stroke characteristics were also included, such as last known well to puncture time, occlusion location (ICA, M1, M2, M3/M4), and the presence of tandem occlusions. Procedural parameters included: intravenous thrombolysis usage; anesthesia type (general or monitored anesthesia care/conscious sedation); BGC use (Walrus [Q’Apel, Fremont, CA, USA], Cello [Medtronic, Dublin, Ireland], Emboguard [Cerenovus, Miami, FL, USA], Flowgate [Stryker, Kalamazoo, MI, USA], Dr Banner [EOSolutions, Las Vegas, NV, USA], or Merci [Stryker, Kalamazoo, MI, USA]); large-bore AC use (inner diameter ≥0.070”); thrombectomy technique (aspiration only, conversion to combination stent retriever and aspiration); number of passes; number that had a single-pass procedure; and rate of FPE (defined as achieving TICI 2c or 3 recanalization in a single pass). Figure 1 shows a case example.
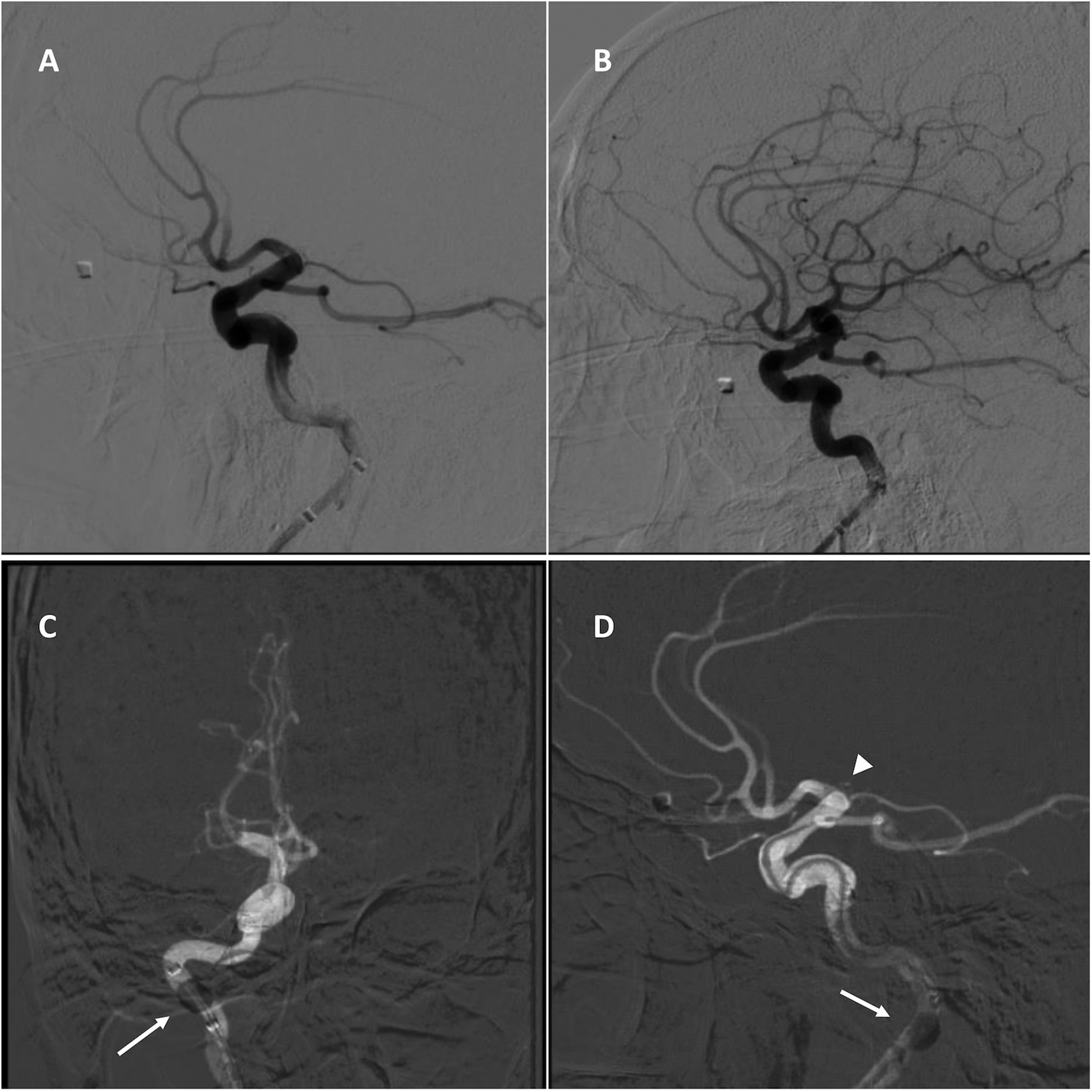
An example of a patient with a M1 segment of the middle cerebral artery occlusion. (A) Pre-treatment lateral angiography view demonstrating occlusion. (B) Post-treatment lateral angiography view demonstrating complete reperfusion (Modified Thrombolysis in Cerebral Infarction 3) after two thrombectomy passes. (C) Anterior–posterior angiography view showing inflated balloon guide catheter (arrow). (D) Lateral angiography view showing an inflated balloon guide catheter (arrow) and navigation to deliver a large-bore aspiration catheter (arrowhead) to the face of the clot.
Clinical outcomes examined were modified Rankin Scale (mRS) score at baseline and 90-day follow-up, National Institutes of Health Stroke Scale score at baseline and discharge, final modified Treatment in Cerebral Infarction (mTICI), and 90-day mortality.
The primary outcome was the rate of FPE, defined as mTICI 2C/3 on the first attempt. Secondary outcomes included final rate of reperfusion (mTICI 2b-3), final rate of excellent reperfusion (mTICI 2c-3), and mRS at 90 days. Large-bore ACs were defined as ACs with an inner diameter of ≥0.070”.
Statistical analysis
Continuous variables were reported as medians and interquartile ranges (IQR), and categorical variables were summarized as frequencies. Comparisons between patients who underwent BGC-assisted thrombectomy (BGC+) and those who underwent endovascular thrombectomy (EVT) did not involve the use of a BGC (BGC-) subgroups were performed using Student's t-test, chi-square tests, and nonparametric equivalents. Multivariable logistic regressions for the likelihood of achieving FPE were performed using the following clinically significant covariables: age, sex, comorbid conditions known to affect rate of FPE (i.e., hypertension, diabetes, atrial fibrillation, hyperlipidemia, prior stroke), antiplatelet/anticoagulant use, tobacco use, pre-stroke mRS, admission National Institutes of Health Stroke Scale (NIHSS), tandem occlusions, occlusion site, intravenous (IV) thrombolytic use, thrombectomy technique (i.e., aspiration only or conversion to combination aspiration and stent retriever), balloon-guide catheter use, and large-bore aspiration catheter use). Multivariable regressions were performed in all included patients, and in BGC+ and BGC- patients separately. Unadjusted odds ratios (OR) and adjusted odds ratios (aOR) with 95% confidence intervals (OR) were reported. Variance inflation factor (VIF) was assessed to assess multicollinearity. Receiver operating characteristics curve analysis yielded areas under the curve (AUC) with 95% CI. Significance was pre-specified at .05. Missing data were minimal and not imputed. Analyses were conducted using JMP v18.0.0 (SAS Institute Inc., Cary, NC, USA).
Results
Of 973 included patients, the median age was 69 years old (IQR 59–79) and 46.5% were female (Table 1). The most common comorbidity was hypertension 68.4% (Table 1). A total of 14.7% of patients had experienced a prior stroke and 42.9% of patients had a history of tobacco use (Table 1). Most occlusions were in the middle cerebral artery (MCA) (82.5%). Approximately 88.2% of patients had a pre-stroke mRS of 0-2 and median admission NIHSS was 15 (IQR 10-20) (Table 1).
Demographics.
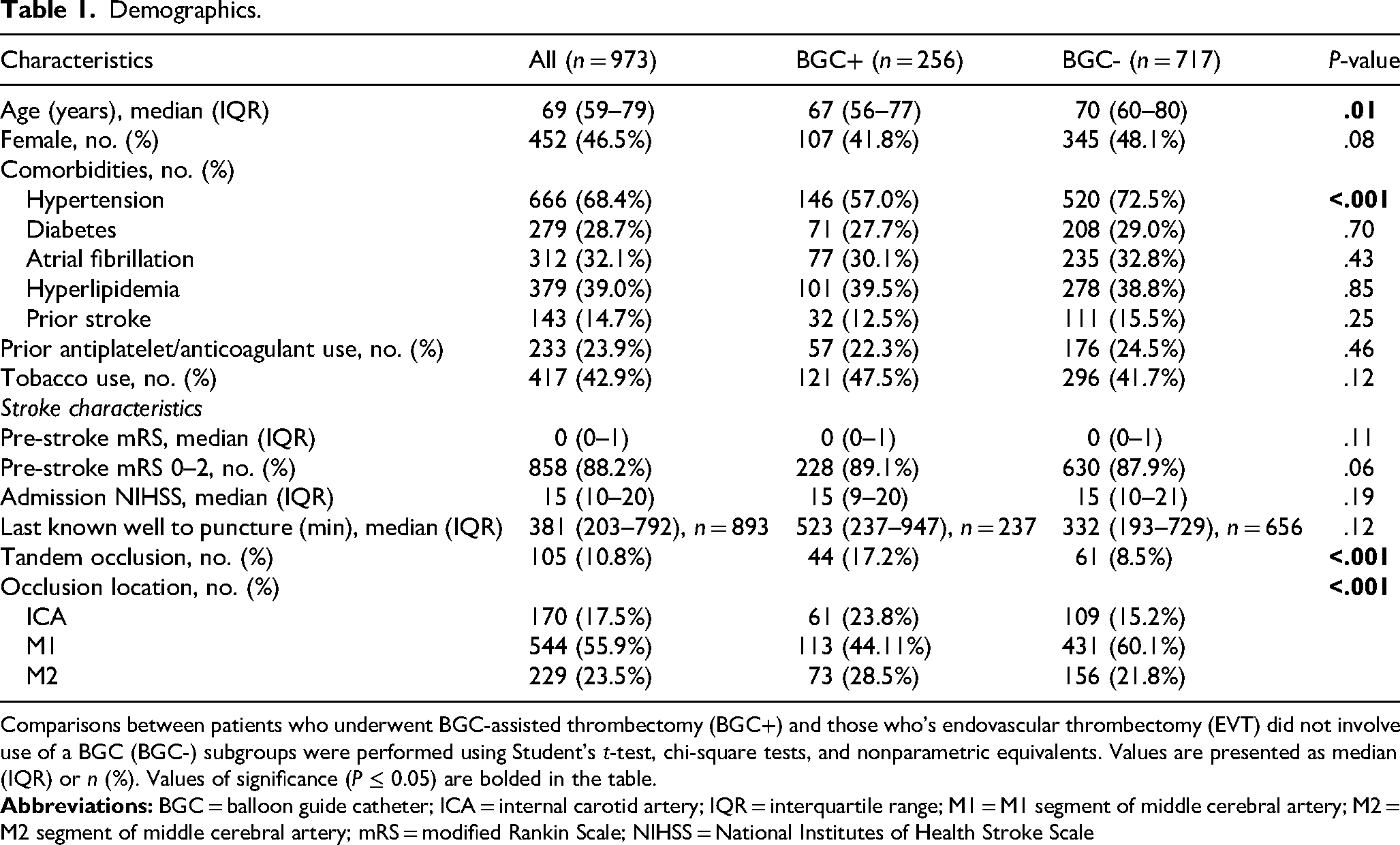
Comparisons between patients who underwent BGC-assisted thrombectomy (BGC+) and those who's endovascular thrombectomy (EVT) did not involve use of a BGC (BGC-) subgroups were performed using Student's t-test, chi-square tests, and nonparametric equivalents. Values are presented as median (IQR) or n (%). Values of significance (P ≤ 0.05) are bolded in the table.
Most procedures used femoral access (97.9%), and 36.6% were treated with IV thrombolysis (Table 2). BGCs were used in 26.3% of cases (256/973) (Table 2). The most common BGC used was the Walrus catheter (Q’Apel Medical, Fremont, CA) (41%; Table 2). Large-bore ACs were used in 68.7% of procedures; in most cases, large-bore ACs were used without a BGC (77.5% vs. 43.8%, P < .001) (Table 2). FPE was achieved in 30.6% of procedures; there was no significant difference in the rate of FPE between BGC+ (29.7%) and BGC- (31.0%) procedures (P = .71, Table 3).
Procedural characteristics.
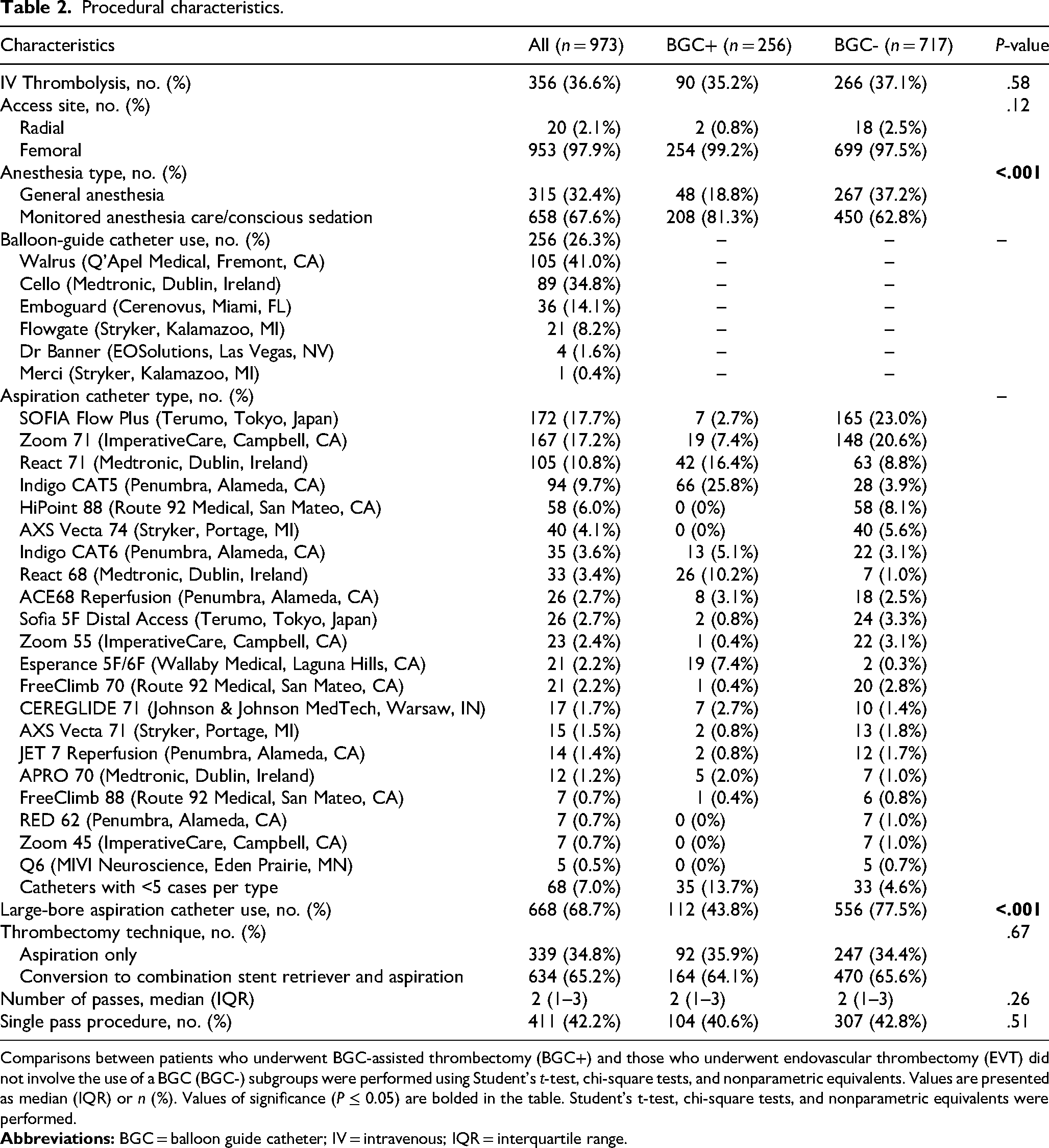
Comparisons between patients who underwent BGC-assisted thrombectomy (BGC+) and those who underwent endovascular thrombectomy (EVT) did not involve the use of a BGC (BGC-) subgroups were performed using Student's t-test, chi-square tests, and nonparametric equivalents. Values are presented as median (IQR) or n (%). Values of significance (P ≤ 0.05) are bolded in the table. Student's t-test, chi-square tests, and nonparametric equivalents were performed.
Peri-procedural and post-procedural outcomes.
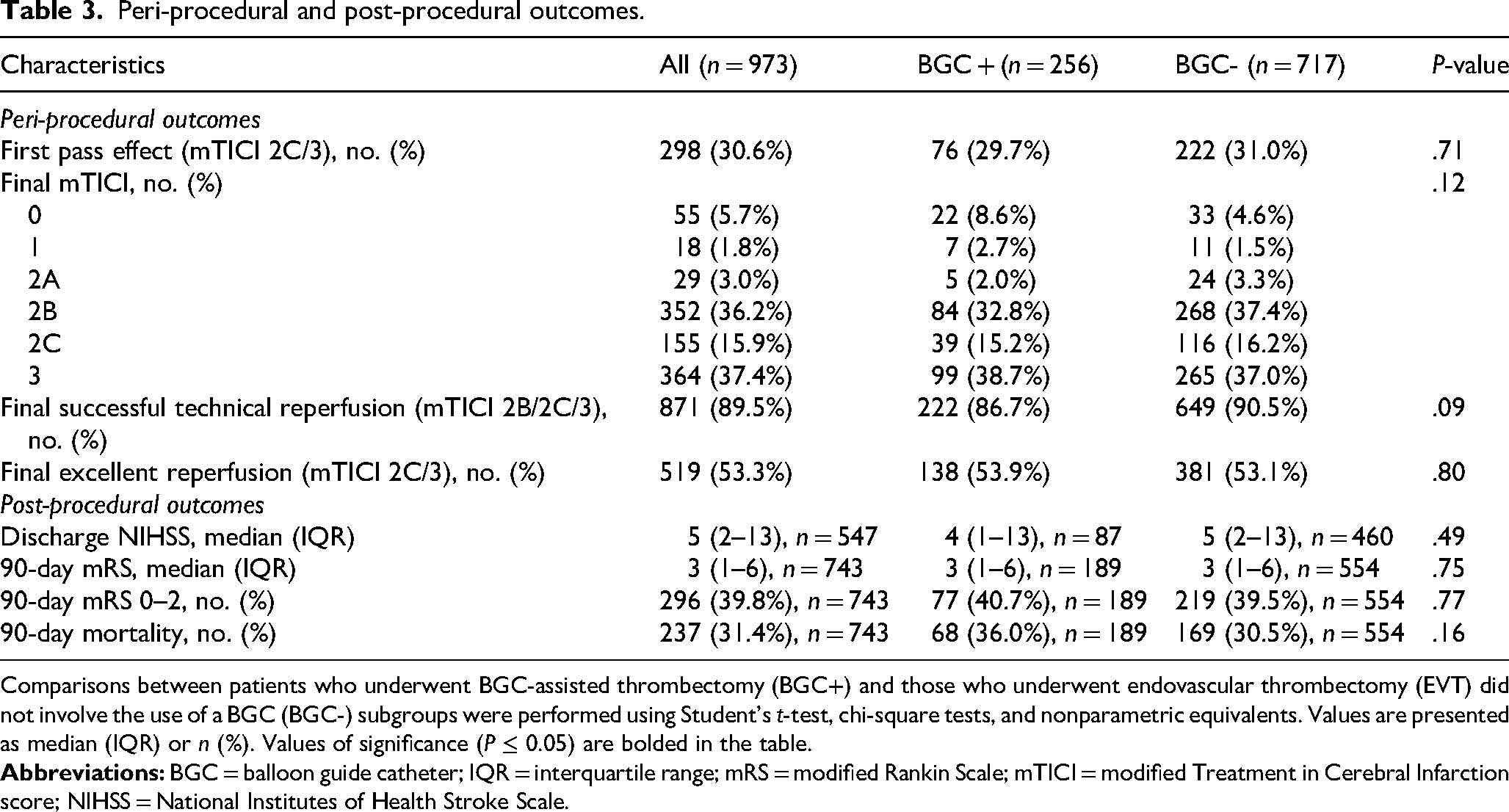
Comparisons between patients who underwent BGC-assisted thrombectomy (BGC+) and those who underwent endovascular thrombectomy (EVT) did not involve the use of a BGC (BGC-) subgroups were performed using Student's t-test, chi-square tests, and nonparametric equivalents. Values are presented as median (IQR) or n (%). Values of significance (P ≤ 0.05) are bolded in the table.
Multivariable regression analyses
In multivariable regressions for FPE in the overall patient cohort, BGCs were independently associated with higher odds of FPE (aOR: 1.94, 95% CI: 1.01-3.73, P = .04), while large-bore ACs were not significantly associated with FPE (P = .07) (Table 4). Among only BGC+ patients, large-bore ACs were not significantly associated with FPE when controlling for other covariables (P = .13) (Table 5).
Logistic regressions for the first pass effect for all included stroke patients.
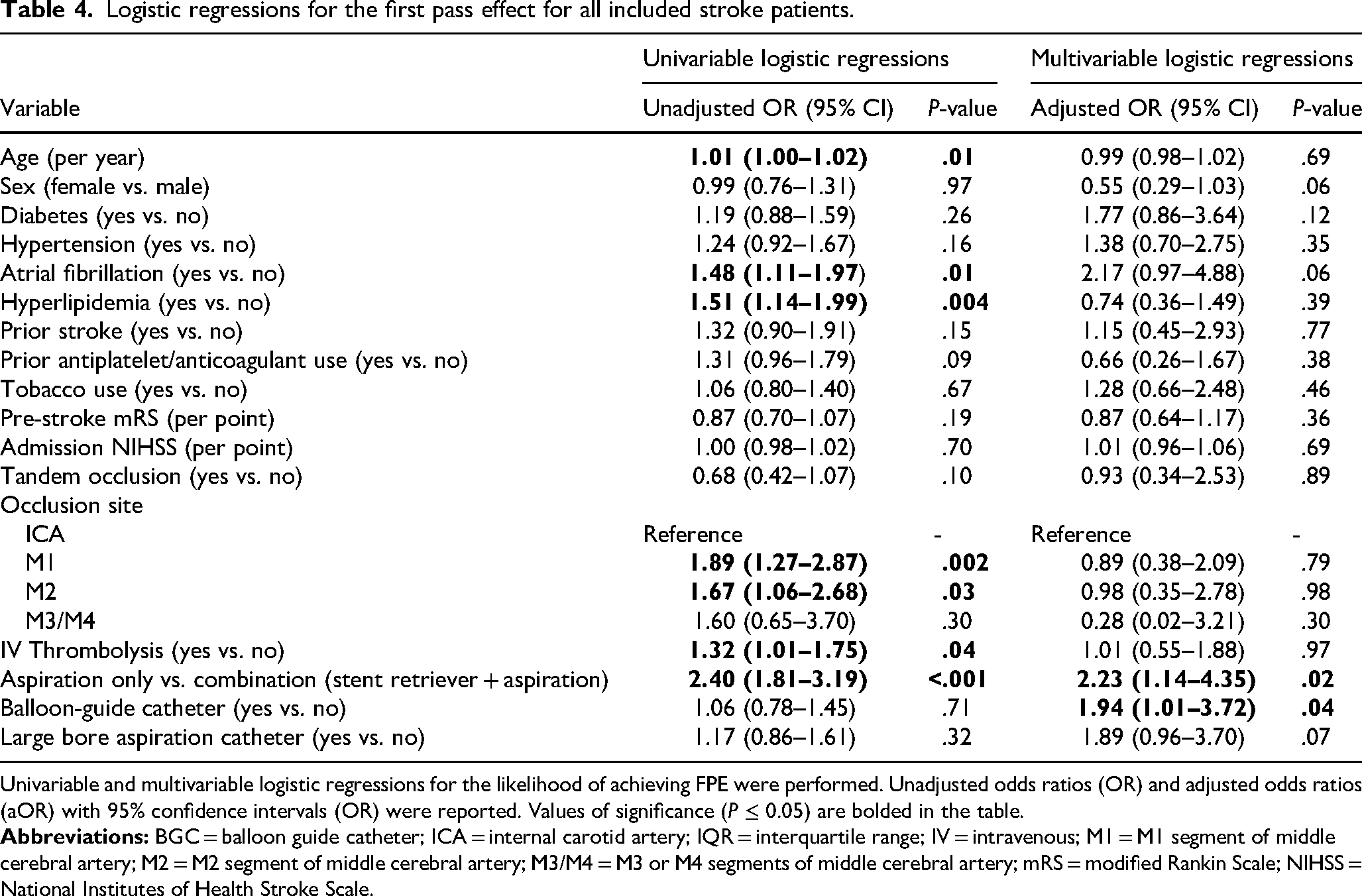
Univariable and multivariable logistic regressions for the likelihood of achieving FPE were performed. Unadjusted odds ratios (OR) and adjusted odds ratios (aOR) with 95% confidence intervals (OR) were reported. Values of significance (P ≤ 0.05) are bolded in the table.
Logistic regressions for the first pass effect in patients treated with and without balloon guide catheters.
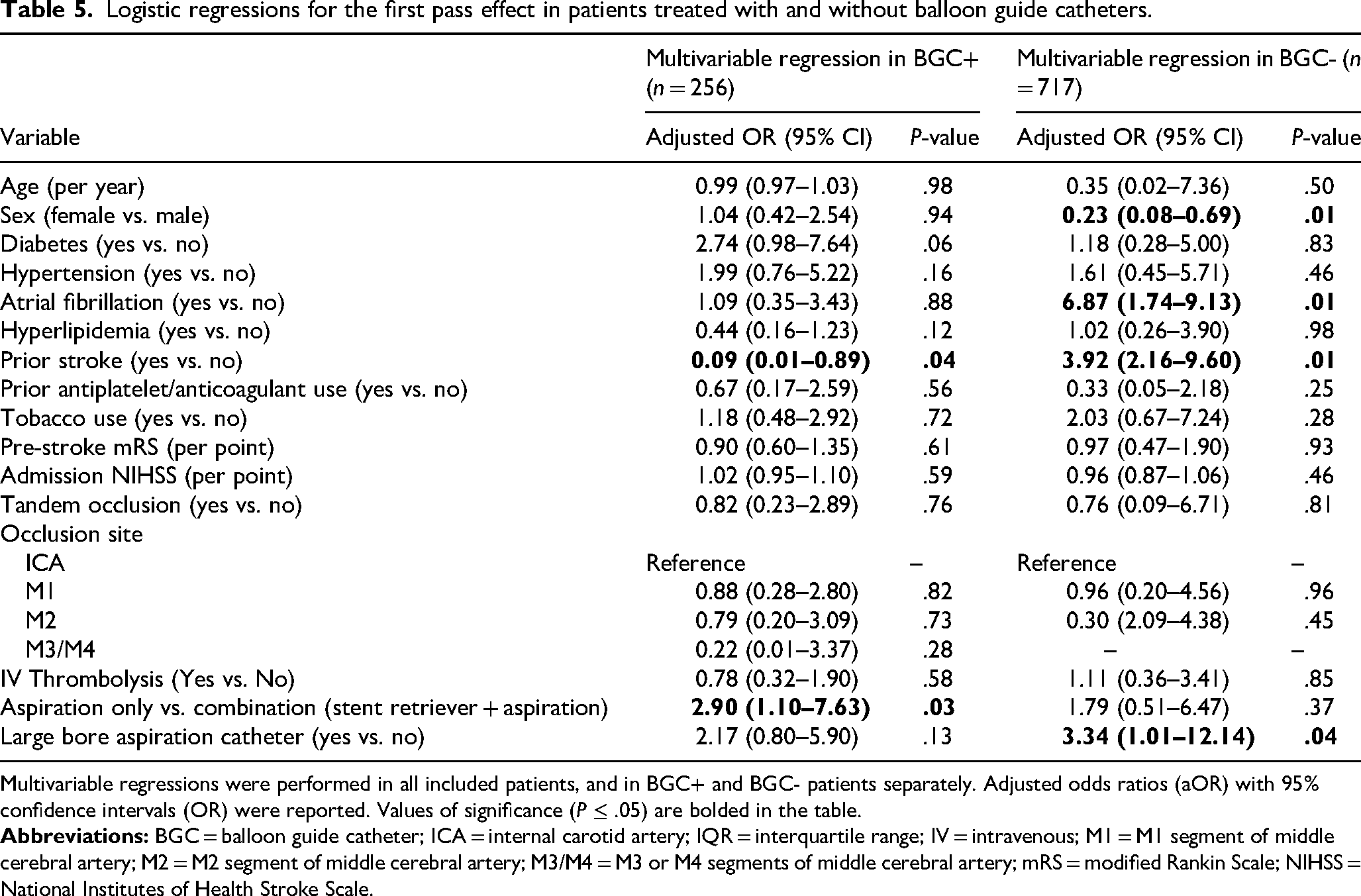
Multivariable regressions were performed in all included patients, and in BGC+ and BGC- patients separately. Adjusted odds ratios (aOR) with 95% confidence intervals (OR) were reported. Values of significance (P ≤ .05) are bolded in the table.
In cases in which a BGC was not used (BGC- cohort), large-bore ACs were significantly associated with a higher likelihood of FPE (aOR: 3.34, 95% CI: 1.01-12.14, P = .04) (Table 5). The AUC for multivariable regressions for FPE in the BGC+ and BGC- cohorts were 0.73 (95% CI: 0.72-0.74) and 0.84 (95% CI: 0.82-0.86), respectively. There was no evidence of multicollinearity in all regression analyses (VIF < 1.5 for all terms).
Post-Thrombectomy outcomes
The median number of passes was 2 (IQR 1-3) (Table 2). Final technically successful reperfusion (mTICI 2B/2C/3) was achieved in 89.5% of cases with a median number of passes of 2 (IQR 1-3), and final excellent reperfusion (mTICI 2C/3) was achieved in 53.3% of cases (Table 3). There were no significant differences in the rates of final successful reperfusion between BGC+ and BGC- patients (P > .09 for comparisons) (Table 3).
There was no significant difference in the median discharge NIHSS between BGC+ (4, IQR 1-13) and BGC- (5, IQR 2-13, P = .49) patients (Table 3). Good functional recovery (90-day mRS 0-2) was achieved in 39.8% of cases, and mortality within 90-days occurred in 31.4% of patients (Table 3). There were similar outcomes in BGC+ and BGC- cohorts in proportion of patients with 90-day mRS 0-2 and mortality within 90 days (P > .16) (Table 3).
Discussion
Overall, this multicenter experience of 973 consecutive anterior circulation thrombectomies suggested that the use of BGCs for anterior circulation strokes is significantly associated with increased odds of FPE. In this analysis, large-bore ACs were not associated with increased likelihood of FPE in the presence of a BGC, demonstrating the possibility that the concurrent usage of a BGC and large-bore AC may have limited (or no) benefit. However, in cases in which a BGC was not utilized, large-bore ACs were significantly associated with higher rates of FPE. This data supports the hypothesis that large-bore ACs may have a similar proximal flow control effect due to the large distal catheter lumen mimicking an inflated BGC distally in the intracranial segment (importantly, distal to the circle of Willis collaterals), and thus, may be playing a similar role in optimizing clot retrieval in the absence of a BGC. Despite the differing caliber between the ICA and MCA vessels, no significant difference in FPE was found, suggesting that partial occlusion by large-bore ACs may be sufficient.
Strong distal aspiration flow is associated with increased FPE, likely reflecting a balance between forward flow and aspiration strength. It can be hypothesized that BGC usage improves chances of FPE through enhanced flow arrest, potentially preventing both clot fragmentation and distal embolization. 22 Moreover, BGCs may also cause a strong suction effect by blocking forward flow. Large-bore AC's increased diameter can create increased negative pressure and therefore higher suction volume. It is possible that the use of a distally-placed large-bore AC placed at the face of an intracranial occlusion may mimic the flow arrest affect seen with BGCs. When large-bore ACs and BGCs are used in tandem, this overlapping mechanism of aspiration strength and blocking forward flow may provide limited added benefit in achieving FPE. However, further hemodynamic studies are required to ascertain patterns of local flow dynamics when using large-bore ACs and BGCs.
The association between BGC use and an increased likelihood of FPE is consistent with findings in prior studies. Zaidat et al. found that the use of a BGC was associated with FPE and may improve rates of early vascularization. 2 Similarly, Blasco et al. found that BGC use specifically on anterior circulation large vessel occlusion (LVO) ischemic strokes had benefits on both angiographic and clinical outcomes with BGC+ vs BGC- FPE rates of 45.8% and 27.7% respectively. 23 In Kim et al., BGCs were associated with significantly higher rates of FPE in aspiration-only cases but not in combined aspiration-stent retriever cases. Adding aspiration in addition to stent retrieval in BGC+ cases did not have higher rates of FPE compared to BGC+ and stent retrievers in the ROSSETTI registry.24,25 Additionally, the use of large-bore ACs, as opposed to smaller sized ACs, has been studied by Pérez-García et al. and Remollo et al. in the ROSSETTI registry, and has a higher likelihood of FPE, reaffirming the use of large-bore ACs in our study.16,17 Prior work has also demonstrated that aspiration catheters of comparable size and generation yield similar results for reperfusion outcomes, regardless of the manufacturer. 15 The results from the current study for 070-type catheters are consistent with these observations. Our study, however, adds an additional, understudied component of incorporating the use of large-bore AC and a BGC together, ultimately suggesting that there may be a blunted benefit (or no benefit) to FPE with combined use when compared to when either tool is used alone. 18
These findings shed light on the relationship between proximal flow arrest with BGCs versus that obtained with larger ACs alone for anterior circulation LVOs. There may be disadvantages in both inventory and cost when large-bore ACs are used in tandem with BGCs, particularly if there is not added benefit to conjunctive use. Future cost-effectiveness analysis may allow for optimization of clinical benefit and cost containment.
Limitations
This is a real-world retrospective analysis of consecutive patients undergoing thrombectomy at three large, academic comprehensive stroke centers in the United States. Additional studies in a diverse range of locations and practice settings are needed to validate these findings and expand their generalizability. The retrospective nature of this analysis subjects the data to bias. There is a plethora of BGC and large-bore aspiration catheters currently on the market, and an expanding array of super large-bore ACs (≥0.088” ID) is being investigated. 26 There may have been device-specific compatibility issues, which may limit operator choice between using both large-bore ACs and BGCs. Moreover, the use of specific catheters and devices, including BGC use, was per the neurointerventionalists’ discretion, and the results of this analysis should not be used to specifically comment on any single aspiration catheter or BGC. Selection bias based on neurointerventionalist preference for BGC and large-bore AC in addition to technique may have influenced outcomes independent of true procedural efficacy. Additionally, another important limitation is the potential confounding effect of guide catheter positioning and the presence of vessel spasm. Distal vessel vasospasm was not documented this dataset, but it is possible that variations in catheter placement or tone influenced the efficacy of both BGCs and large-bore ACs.
Conclusion
In thrombectomies for anterior circulation strokes, BGC usage is important when analyzing the benefit of FPE on good clinical outcomes. In the absence of a BGC, large-bore AC usage contributes to increasing the chance of achieving FPE. Based on this study, there is no added benefit or increased chance of FPE when utilizing both BGC and large-bore AC.
Footnotes
Acknowledgements
None.
ORCID iDs
Ethics statement and approvals
All three institutions involved in data collection for this study had the study approved by their respective institutional review boards: University of Utah Health IRB approval: IRB_00184538; University of Iowa Hospitals and Clinic's IRB approval: 201910789; Cooper University Healthcare IRB approval: 22-096.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: RG: Consultant for Medtronic Neurovascular, Stryker Neurovascular, Rapid Medical, J&J Neurovascular, Balt. Research Funding from: Medtronic Neurovascular, Balt, Scientia, J&J Neurovascular. ES: Consultant for Medtronic, Terumo Neuro, J&J Neuro, and Rapid Medical.
TGJ: consultant for Contego Medical; grants from Medtronic and Stryker; data safety monitoring for Cerenovus; ownership/investment interest in Anaconda, StataDx, Galaxy, Basking, Freeox Biotech, Kandu, Viz-AI, Route92, and Gravity. DT: Consultant for Route 92 Medical. All other authors do not have disclosures to declare directly related to this work.
Data availability statement
De-identified data may be made available upon reasonable request to the corresponding author.