
Abstract
Background and Purpose
Nonrandomized studies have found Balloon Guide Catheter (BGC) use to improve technical and functional outcomes in patients undergoing mechanical thrombectomy (MT).
Materials and Methods
We performed a retrospective analysis on prospectively collected data of consecutive ischemic stroke patients undergoing MT at our institution (December 2020-October 2021). Interventions where BOBBY BGC (BBGC, MicroVentionTM, Aliso Viejo, CA) was used were identified. Baseline demographics and clinico-radiographic characteristics were retrospectively collected and analysed using descriptive statistics.
Results
A total of 43 patients received BBGC-MT (male: female = 26:17, median age 72 years [IQR 62-82]). The most common occlusion site was the middle cerebral artery (MCA) (60.4%). Over half (51.2%) received intravenous thrombolytics. The BBGC tracked well over tortuous aortic arches (type II 34.8%, type III 16.3%), with median arteriotomy-to-perfusion time of 29 min (IQR 20-46). Thromboaspiration was used as first-line MT technique in 69.7% cases, with 1 (IQR 1-2) median MT pass achieving modified TICI (thrombolysis in cerebral ischemia) scores of 3 and 2b/3 in 74.4% and 95.3% respectively. Our overall first pass effect (FPE, defined as mTICI 3 after firs-pass) and modified FPE (defined as, mTICI 2b/3 after first-pass) rates were 51.1% and 79.1% respectively, with rates of 92.3% and 100% respectively when stentretriever and thromboaspiration were combined. The median reduction in National Institutes of Health Stroke Scale (NIHSS) was 9 (IQR 4–15, p < 0.0001), with a median 90-day modified Rankin Score (mRS) of 1.5 (IQR 0-2).
Conclusions
BOBBY BGC use resulted in a high first-pass effect rate and may contribute towards improved functional outcomes.
Introduction
A series of randomized controlled trials over the past decade have established revascularization with mechanical thrombectomy (MT) as the standard-of-care for acute ischemic stroke patients presenting within 24-h of a large vessel occlusion stroke.1,2 However, the endovascular technique employed for revascularization varies from stent-retriever thrombectomy (ST) to direct-aspiration-first-pass-technique (ADAPT) to a combination of the two, with a recent randomized clinical trial finding ADAPT to be non-inferior to ST in terms of recanalization-rate and 3-month modified Rankin Score (mRS). 3 Regardless of the technique used, non-randomized comparative data have found proximal flow-arrest with a balloon-guide catheter (BGC) to significantly improve recanalization rates (modified thrombolysis in cerebra ischemia, mTICI scores), increase first-pass effect (FPE) rate, reduce embolization in new and same vascular territories, and independently predict functional outcomes.3–10 As FPE gains wider acceptance as the premier metric for a technically successful MT, 11 in conjunction with the abatement of traditional reluctance to BGC use (e.g. comparable major groin complications, 12 comparable tortuous arch navigation, 13 compatibility with large-bore (0.058–0.070 inch) aspiration catheters, 3 ) their real-world use has increased across large MT registries.4–7 Data suggesting superiority of BGC over conventional guide catheters have now been made available from multi-national real-world MT registries,4–7 metanalyses,8–10 and subgroup analyses of randomized clinical trials; 14 for ST MT,4–7 ADAPT and both, 15 causing the American Heart Association (AHA) guidelines 1 to recommend their use as “maybe beneficial” over conventional cervical guide catheters alone (class IIa; level of evidence C). Despite their advantages, the universal adoption of BGCs has been hindered by cumbersome balloon preparation techniques, concerns over trackability and the inability to advance larger bore aspiration catheters through previous BGCs.4–7 The BOBBY BGC (BBGC, MicroVentionTM, Aliso Viejo, CA) is an 8 French short-sheath compliant guide-catheter, with an 8.4 French outer-diameter and 0.086-inch inner-diameter, providing 95cms working length. The balloon is 10 mm in diameter and length upon maximum inflation (e Figure 1). We present the first clinical experience with the BBGC when used during MT.
Methods
This was a retrospective, observational, study conducted at our institution from a prospectively maintained database after receiving a waiver from the Institutional Review Board on the need to obtain informed patient consent given the retrospective nature of the study. The study was performed under the guidelines outlined by the Declaration of Helsinki. Between December 2020 and October 2021, 128 consecutive patients underwent MT. All patients ≥18 years with a confirmed large-vessel occlusion (internal carotid artery (ICA), M1 or proximal M2 segments of middle cerebral artery (MCA), A1 segment of anterior cerebral artery (ACA), basilar artery, P1 segment of posterior cerebral artery); time from last-known-well under 24 h, baseline National Institutes of Health Stroke Scale (NIHSS) (NIHSS) score ≥4; and premorbid mRS score ≤3 were included. During this period, all patients treated by the senior author underwent MT with the aid of the BBGC. Patients transitioned to comfort measures were excluded. Baseline CT/MR angiographic findings (occlusion site, aortic arch type), last-known-well to arteriotomy and arteriotomy-to-recanalization times, final modified TICI (thrombolysis in cerebral ischemia) scores including the fist-pass effect (defined as mTICI 3 after first-pass), modified-FPE (defined as, mTICI 2b/3 after first-pass), symptomatic intracranial hemorrhage (ECASS-II definition), 16 and 90-day mRS scores for BBGC patients were collected. Device specifications and schematic are depicted in eFigure 1. The BBGC was prepared ex-vivo by purging the luminal air via injection of 50% of iodinated contrast (Visipaque, Iodaxonal 320 mg/ml) through the balloon lumen while keeping the balloon tip of the BBGC immersed in a saline bowl, with the balloon constrained using gentle manual pressure to prevent ex-vivo balloon inflation (an analogous technique is described elsewhere for preparation of the Scepter and Scepter Mini balloon microcatheters (Microvention, Aliso Viejo, CA). Contrast injection was stopped when no more air bubbles could be purged from the balloon lumen and gentle pressure could be felt by the operator constraining the balloon. The balloon preparation duration was less than 20 s in all instances. Of the 128 mechanical thrombectomies performed within the study-period, all consecutive BBGC thrombectomies were performed by a senior neurointerventional fellow under the direct supervision of a senior attending (B.D.J), with 12-years of interventional experience. All mechanical thrombectomies performed with the BBGC comprised of a triaxial system using a 0.055inch to 0.070inch distal access catheter (eFigure 1) and a 0.017inch to 0.021inch microcatheter. The final angiographic run was retrospectively reviewed by 2 neurointerventionalists to confirm the mTICI score. In the event of a differing opinion between the 2 investigators, another neurointerventionalist (not involved in the case) reviewed the data, and all 3 investigators came to a consensus regarding the results. All patients had a 3-month follow-up clinic visit when their 90-day mRS scores were recorded. When this was not possible, a mRS score was obtained based on a telephone interview or their mRS score was constructed based on chart-review.
Results
Between December 2020 and October 2021, 128 patients underwent MT at our institution of which 43 patients (who were consecutively treated by the senior author) received BBGC guided MT (male: female = 26:16, median age 72 years [IQR 62-82], Table 1). Final stroke etiology was determined to be related to cardioembolism (65%), large-artery atherosclerosis (7%), embolism from undetermined source (16.3%), carotid artery dissection (7%) and other causes (4.7%). Thrombo-embolic occlusions occurred in MCA in 60.4% (M1 34.9%, M2 23.2%, M3 2.3%), ICA in 9.3%, tandem (ICA/M1-M2) in 21%, A1 in 2.3%, and basilar/P1 in 7%. Over half (51.2%) received intravenous thrombolytics. The median last-known well to arteriotomy and arteriotomy-to-recanalization times were 266.5 min (IQR 150-430) and 29 min (IQR 20-46) respectively. The first-pass thrombectomy modality was ADAPT (69.7%) or ADAPT + ST (30.3%). The BBGC tracked well over tortuous aortic arches (type II 34.8%, type III 16.3%, Figure 1); and was inflated under fluoroscopic guidance within the mid-cervical ICA (74.4%), common carotid artery (18.6%) and vertebral artery (7%). Two patients underwent BBGC guided carotid artery stenting with a 10 mm diameter PRECISE carotid stent (Cordis, Santa Clara, CA) in one, and a relatively stiffer carotid WALLSTENT (Boston Scientific, Valencia, CA) in the other (eFigure 2). There were no instances of arterial dissection, balloon-rupture or premature balloon deflation. The median number of thrombectomy passes was 1 (IQR 1-2), with final recanalization rates (eFigure 3): mTICI 3 (74.4%), mTICI 2b (20.9%), mTICI 2b/3 (95.3%). Our FPE and modified FPE rates were 51.1% and 79.1% respectively. The FPE and mFPE rates when ADAPT and ST was performed (n = 13) were 92.3% and 100% respectively. Overall mortality rate was 9.3% (comfort-directed goals of care [n = 3], and refractory cardiac arrest 3 days after thrombectomy [n = 1]). One patient had a symptomatic intracranial hemorrhage (2.3%). Peri-operative complications included M2 microperforation after 2nd stentreriever pass (n = 1), embolism in new (n = 3) and same (n = 3) vascular territories. Among survivors, the discharge NIHSS reduced by a median 9 points (IQR 4-15, p < 0.0001). At median follow-up of 3.5 months (IQR 1-6), one patient died from sepsis while the survivors had a median 90-day mRS score of 1.5 (IQR 0-2). For the 27 patients for whom a 90-day mRS was available, about 81.5% patients had good (mRS score of 0-2) functional outcomes (reaching 92.3% among the 13 patients with FPE).
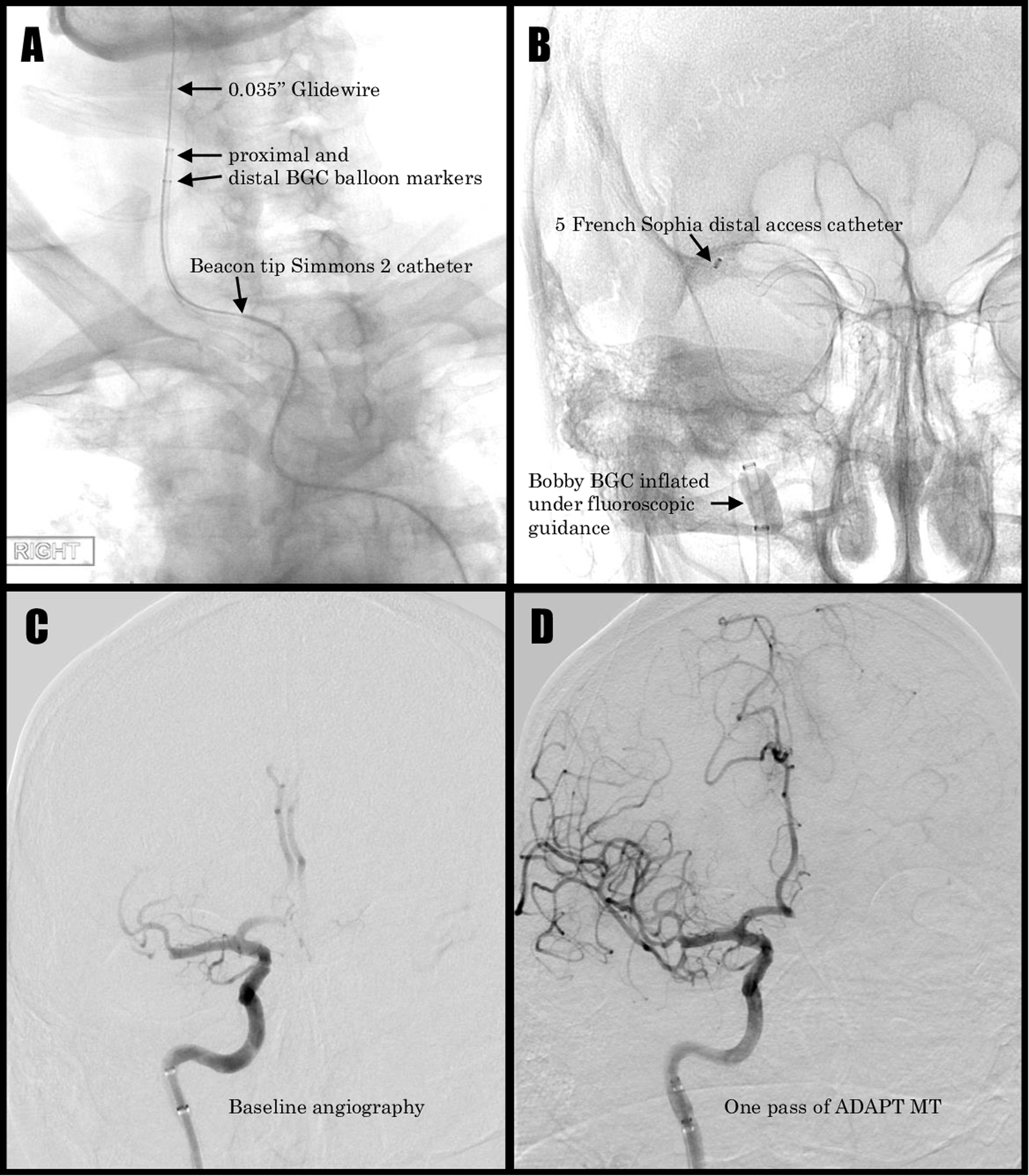
Bobby BGC guided mechanical thrombectomy 80-year-old man with right middle cerebral artery (MCA) occlusion:
Study characteristics.
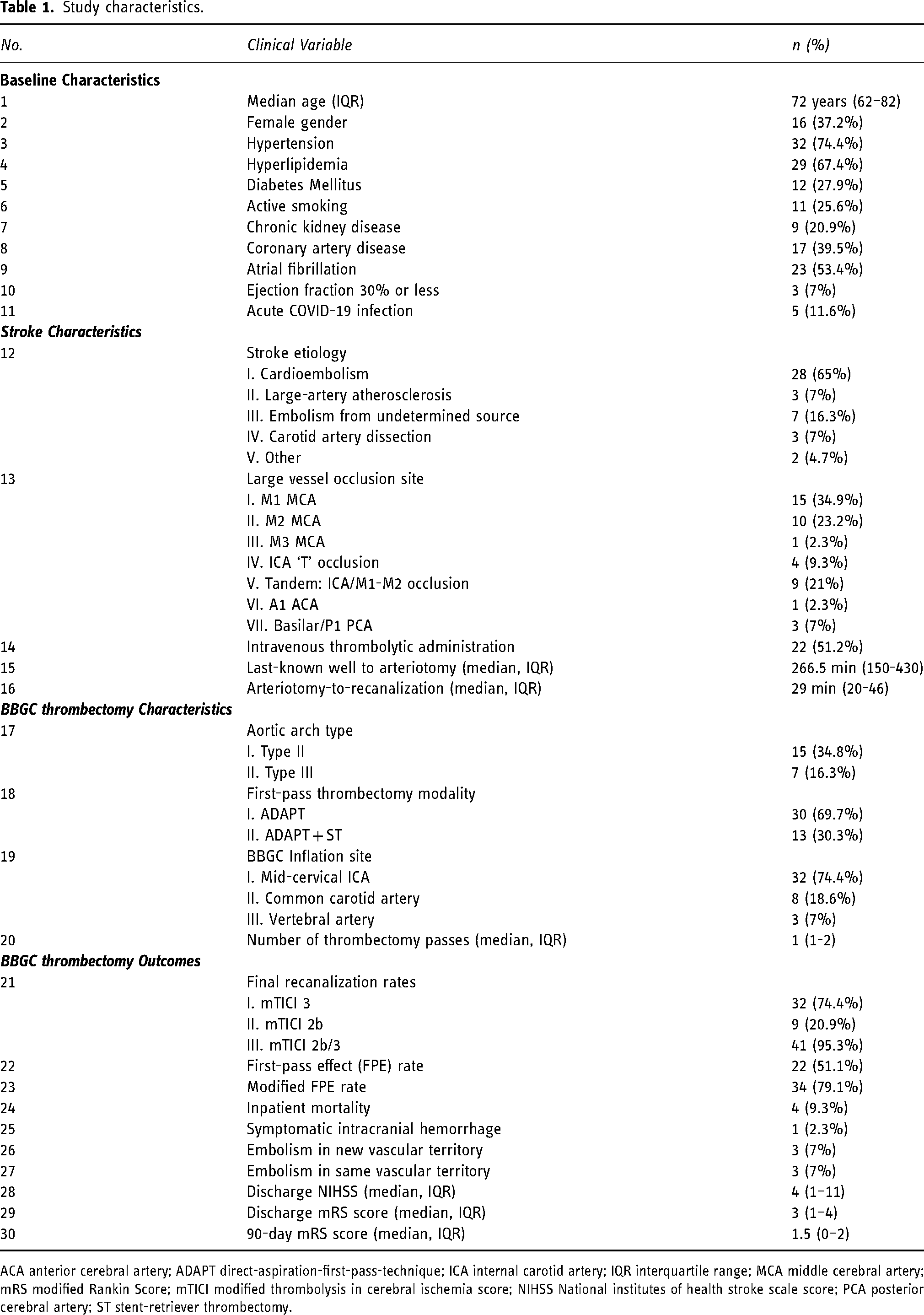
ACA anterior cerebral artery; ADAPT direct-aspiration-first-pass-technique; ICA internal carotid artery; IQR interquartile range; MCA middle cerebral artery; mRS modified Rankin Score; mTICI modified thrombolysis in cerebral ischemia score; NIHSS National institutes of health stroke scale score; PCA posterior cerebral artery; ST stent-retriever thrombectomy.
Discussion
Our case series of 43 patients is the first clinical experience reported for BBGC guided MT. Our overall FPE (51.1%) rate is comparable to that seen with other BGC MT studies (63.1%, 8 42.3%, 10 eFigure 4). Our FPE and mFPE rates for ADAPT using 0.055–0.070-inch aspiration catheters are comparable to previous MT studies that utilized mixed (balloon and conventional) guide-catheters: FPE 33.4% versus 22–37% and mFPE 70% versus 40–55%. 11 Notably, our FPE and mFPE rates for combination MT (ADAPT + ST) are higher than previous observations (eFigure 5): FPE 92.3% versus 20–32% and mFPE 100% versus 48–68%.8,10,11 Our mortality (9.3% vs. 17%)8–11 and symptomatic intracranial hemorrhage (2.3% vs. 4%)9,10 rates are also comparable to prior observations with BGC-MT. About 81.5% patients had good functional outcome at their 3-month clinical follow-up (eFigure 6), which is higher in comparison to landmark RCTs on MT (46%) 2 and BGC-MT metanalyses (59.7%, 8 59.5%, 9 51.6%. 10 ) This was higher for FPE patients (92.3%) and exceeds good functional outcomes reported in prior FPE cohorts (56%). 11
The BOBBY BGC differs significantly from previously available BGCs in its design, and the technique used for its preparation. Its design is similar to that of dual lumen balloon microcatheters such as the Scepter and the more recently the Scepter Mini (Microvention, Aliso Viejo, CA) microcatheters. Specifically, unlike other BGCs, which rely on aspiration and reinflation for eliminating air from the balloon lumen, the BBGC relies on purging of air from the balloon lumen by contrast injection allowing for effective elimination of most air-bubbles, and to-date we have not observed air bubbles following in-vivo inflation in any of our patients. Not only does this help prevent symptomatic air-embolism should there be an inadvertent balloon rupture; but also allows for more uniform balloon expansion avoiding asymmetrical stress on the arterial wall or torquing and kinking of the BGC. Such an inflation mechanism also obviates the need for ex-vivo pre-inflation preserving its original profile, which we believe allows for the BBGC to track better in tortuous cervical vasculature in comparison to prior BGCs (Cello, Medtronic, Irvine USA; Flowgate, Stryker, Rayneheim, USA). In our series, we did not encounter any difficulties with tracking of the BBGC in tortuous cervical vasculature, including traversing the BBGC via the lumen of freshly placed carotid stent constructs (eFigure: 2).
The BBGC has a larger inner diameter (0.086 in.) compared to some of the other BGCs (8F Cello - 0.075 in., 8F Flowgate - 0.084 in.) (online supplement). Despite their proven utility, the inability of these prior BGCs to accommodate large bore aspiration catheters had constituted a significant limitation in the utilization of these older BGCs. The utilization of larger aspiration catheters is important for the removal of long clots or clots within the proximal intracranial circulation since the suction force generated at the aspiration catheter tip, and hence efficacy of clot removal is proportional to r, 4 where r is the radius of the aspiration catheter.2,17 The recent availability of BBGC and other larger inner diameter BGCs, Walrus (Q’Apel, Fremont, CA) or BOSS (Marblehead Medical, Maple Grove, MN), overcomes the limitation posed by prior BGCs and allows for BGC utilization with larger bore aspiration catheters. 19 The BBGC allowed us to confidently utilize 0.071 in. inner diameter aspiration catheters for intracranial aspiration (6F SOPHIA, eFigure: 1). The larger lumen of BBGC also allows for reliable placement of carotid stents through their lumen under flow-arrest, providing protection from distal embolism in the acute stroke setting in patients with tandem arterial occlusions, especially since in these patients, despite a potentially unstable carotid bifurcation plaque, the use of distal protection devices is infrequent.17,18
Other than being a single-centre, single-proceduralist guided (B.D.J.), retrospective study, all of which potentially introduced selection biases limiting the external validity of our results; our study-limitations also include the lack of a comparative BGC-cohort (e.g. the Walrus/BOSS BGC) and a blinded angiographic and clinical outcomes adjudicator. The authors believe that adequate data, albeit non-randomized, have shown superiority of BGC over conventional guide catheters for MT, and thus did not include a comparative non-BGC cohort. Though only 7% of our cohort had posterior circulation strokes limiting our findings to the anterior circulation; however, the authors find the ease of navigability of the Bobby BGC into the vertebral arteries worth reporting. Finally, an ascertainment bias introduced by the 90-day loss of follow-up may have influenced the observed functional outcomes. Poor navigability and experience are common causes to BGC reluctance; however, the senior author (B.D.J) has found the Bobby BGC to be easily navigable even in the hands of trainee neurointerventionalists in patients with tortuous aortic arch and carotid anatomy. The authors also note that the Bobby BGC has a quick and familiar preparation method with rapid in-vivo inflation and deflation.
Conclusion
BOBBY BGC guided MT resulted in an overall high FPE rate that is comparable to previously published BGC-MT data, with comparable mortality and symptomatic intracranial hemorrhage rates. BOBBY BGC use when stentretriever and thromboaspiration are combined, may result in even higher FPE/mFPE rates in comparison to prior BGC-MT studies, with more patients demonstrating higher functional independence regardless of the MT technique.
Supplemental Material
sj-docx-1-ine-10.1177_15910199221104920 - Supplemental material for BOBBY balloon guide catheter thrombectomy in large-vessel occlusion stroke: Initial experience
Supplemental material, sj-docx-1-ine-10.1177_15910199221104920 for BOBBY balloon guide catheter thrombectomy in large-vessel occlusion stroke: Initial experience by Karan Topiwala, Coridon Quinn, Tapan Mehta, Kamran Masood, Andrew Grande, Ramachandra Tummala and Bharathi Jagadeesan in Interventional Neuroradiology
Footnotes
Author contributions
KT has full access to all of the study data and takes full responsibility for the integrity and accuracy of the data analysis. Study concept and design: KT, BDJ. Data-acquisition, analysis and interpretation, manuscript drafting, revision and final approval: All authors
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.