
Abstract
Background
Patients undergoing elective endovascular treatment for cerebrovascular diseases (CBVD) may face mental health challenges that impact their quality of life (QoL). However, this issue is still rarely addressed in neuro-endovascular research literature and clinical practice. Our single center ongoing project ONIRIC aims to assess anxiety and depressive symptoms, coping, and QoL in CBVD patients treated via endovascular approaches.
Methods
We prospectively enrolled a cohort of patients undergoing elective endovascular procedures over a 6-month period. Patients completed the State-Trait Anxiety Inventory (STAI-S and STAI-T), the Beck Depression Inventory-version II (BDI-II), the Brief Coping Orientation to Problems Experienced Inventory (Brief-Cope), the Euro-QoL 5D-5L, and the World Health Organization Disability Assessment Schedule (WHODAS 2.0) questionnaires at the baseline, and at discharge.
Results
We included 25 patients (13 females): mean age 60 ± 12.5 years. There was a significant improvement in state anxiety and depressive symptom scores at discharge: the BDI-II scores significantly differed from the ones at baseline (p < .01), as well as the STAI-S scores (p < .01). The coping and QoL scores did not show any changes.
Conclusions
To our knowledge, this research represents one of the few prospective studies examining the psychological and neuropsychological outcomes associated with elective neuro-endovascular treatment of CBDV. Despite the small sample size, our preliminary findings, are consistent with recent literature in related fields, contributing valuable insights to the broader understanding of how these factors influence clinical management. Future directions include the collection of follow-up data, essential for deepening our understanding of this complex and sensitive issue.
Introduction
Because of improved quality and availability of brain imaging techniques, the number of detected unruptured intracranial aneurysms (UIA) or unruptured cerebrovascular diseases (CBVD), such as arterovenous malformation (AVM) or dural arterovenous fistula (DAVF), is increasing. 1
The decision to treat an incidentally detected vascular malformation is based on a balance between the risks of future rupture and the complications of preventive treatment. For instance, in case of UIA, helping-decision instruments, such as the Unruptured Intracranial aneurysms treatment score (UIATS) could be used. 2 Furthermore, other factors can influence the decision-making process, especially the psychological burden: the treatment itself can serve as a source of reassurance, conversely, the ongoing presence of the aneurysm perpetuates the fear of rupture. 3 Indeed, little is known about the reassurance effect of treating an aneurysm/cerebrovascular malformation or the persistence of anxiety symptoms in patients who are aware to carry a CBVD. Even treated patients may have persistent worry and a proportional reduction in quality of life (QoL), due to the concern of developing another aneurysm or a recurrency. 4 Although mental health disorders are common in the general population, they are rarely considered during the assessment of a patient's medical history prior to neuroendovascular procedures, 5 and, despite their crucial role in determining QoL and supporting the comprehensive care of patients with CBVD, this aspect remains largely neglected in both literature and clinical practice, as highlighted in a recent systematic review. 6 Moreover, the studies tackling this issue are mainly focused on aneurysms and brought controversial results.7–9
To fill this gap, we investigated anxiety and depressive symptoms, coping strategies, and QoL in a cohort of patients whose undergone elective endovascular procedure for CBVD, within an ongoing project at our Institution (ONIRIC, Outcome in Neurointerventional Radiology Indication and Complications). The project consists of assessing mental health status and QoL at the baseline, post-procedure, and at 3-, 6-, and 12-month follow-ups. Here, we report and discuss the preliminary results of baseline and post-procedure evaluation of an initial cohort of patients (N = 25).
Materials and methods
Patients
Between July and December 2023, we recruited a consecutive sample of patients eligible for elective endovascular treatment at Fondazione IRCCS Istituto Neurologico Carlo Besta (FINCB). The study was carried out in accordance with the recommendations of the Declaration of Helsinki, the STROBE cohort reporting guidelines, 10 and supported by the Italian Ministry of Health (RC 2025). The protocol was approved by the ethics committee of the FINCB (internal ref: 01/2022; amendment approved 8 March 2023, internal ref: 13). Patients were assessed the day before the procedure, after they gave specific written informed consent. A psychological evaluation was performed in a dedicated room by an expert neuropsychologist (CR) at both time points to minimize inter-rater variability. After the procedure and prior to discharge, the psychological assessment was repeated in the same setting. Data were collected and anonymized in a dataset according to the current GDPR privacy law. 11 Each assessment lasted about 30 min. The study flow is represented in Figure 1.
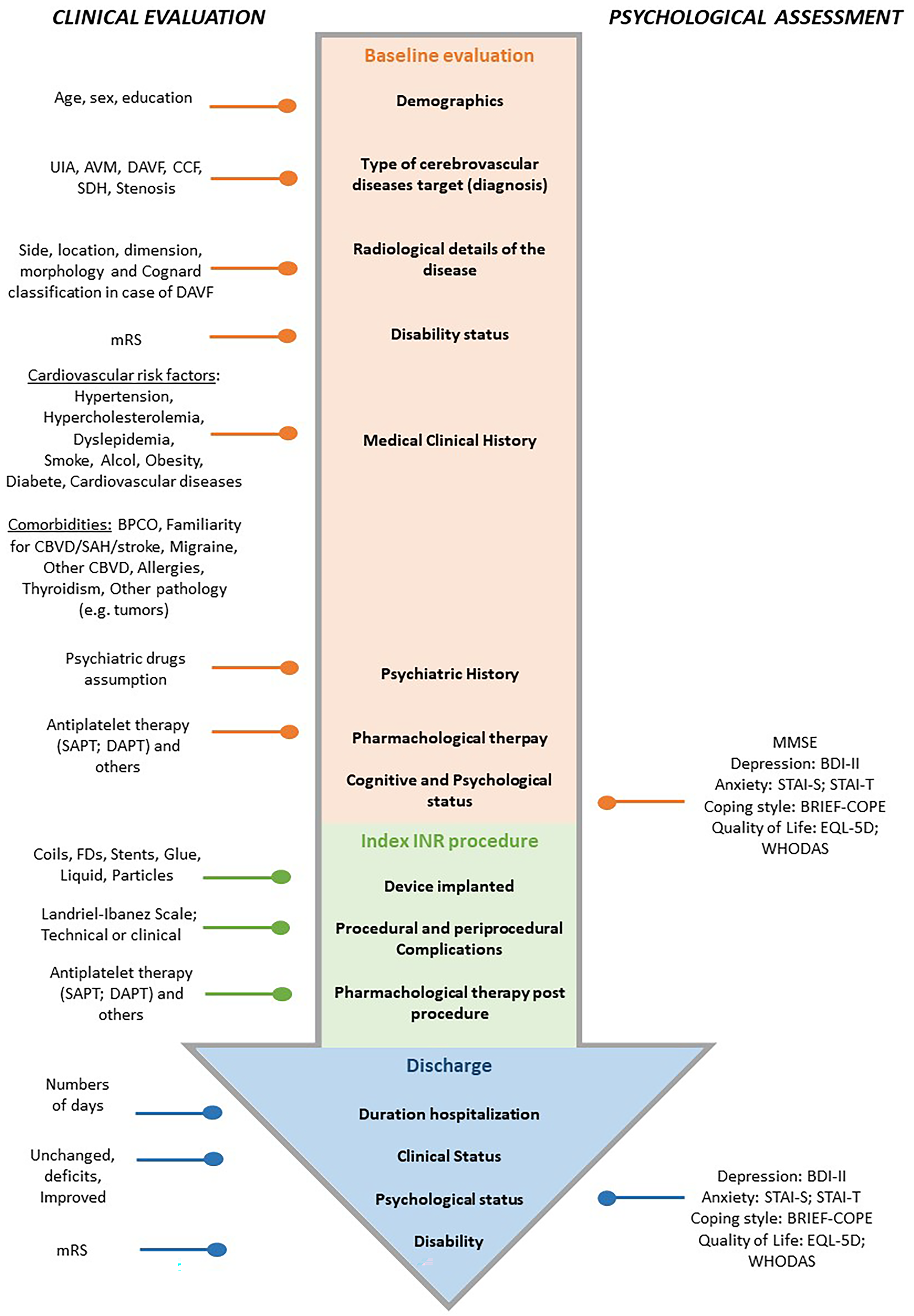
Study flow diagram.
General and clinical variables
At baseline, we recorded the sociodemographic data, symptomatology of the patients (e.g. ocular symptoms, headache), diagnosis of CBVD and radiological characteristics (side, location, morphology). We recorded also comorbidities including cardiovascular risk factors (hypertension, hypercholesterolemia, dyslipidemia, smoke, alcohol, obesity, diabetes, other cardiovascular diseases) and previous anamnestic relevant information (other serious pathologies such as tumors, drugs assumption etc.).
Level of independence was recorded at the baseline and at discharge using the modified Ranking Scale (mRS), a measure of functionality commonly used to assess patients after a stroke or CBV accident. 12 The mRS is scored on a scale from 0 to 6, where 0 is no symptoms, 5 is confined to bed, and 6 is death.
Concurrently, we assessed the level of global cognitive integrity through the Mini Mental State Examination (MMSE). 13
Regarding the index endovascular procedure, we recorded the type of the device implanted, as well as the technical and clinical complications occurred during the procedure or at discharge (none, thrombosis, hemorrhage, etc.). Pharmacological therapies before and after the index procedure were also registered. To categorize the complications after the endovascular treatment we chose the Landriel-Ibanez Scale. 14 It is divided into four grades based on the severity of the complications and the type of treatment required.
Significant adverse events (AEs) were documented differentiating in serious adverse events (SAEs), mild adverse events (MAEs), related or unrelated to the procedures. SAEs were defined as an AE with clinical relevance and permanent deficit or prolonged hospitalization. 15 MAEs were defined as an AE with clinical relevance but transient. 15
Psychological and QoL variables
To assess the psychological status, a series of validated instruments were utilized.
Depressive symptoms were evaluated considering the two weeks prior to the scheduled intervention, with the Italian version of the BDI-II,16,17 which includes 21 items. It uses a three-point Likert scale with a total score ranges from zero to 63. The severity of depressive symptoms was rated according to the criteria reported in Beck et al. 17 and other studies 18 : “no depression” (<13), “mild depression,”14–19 “moderate depression,”19–28 and “severe depression” (>30).
Anxiety symptoms were examined through the Italian version of the STAI-S and STAI-T.19,20 Those scales consist of 20 questions for state-anxiety, and 20 questions for trait-anxiety. This instrument uses a 4-point Likert-type scale, with a total score ranging from 20 to 80. 20 According to Spielberg, 20 the severity of anxiety is graded into: “no anxiety symptoms” (<40), “mild anxiety” (40–50), “moderate anxiety,” (50–60) and “severe anxiety disorder” (>60).
Coping strategies were measured with the Italian version of the Brief-Cope questionnaire, 21 a shortened version of the COPE questionnaire, pointing out effective or ineffective ways to cope with a stressful life event. “Coping” is broadly defined as cognitive and/or behavioral effort to manage specific external/internal demands exceeding personal resources or, more simply, as processes of response to stressors, 22 such as being hospitalized and undergoing endovascular procedure. COPE questionnaire is often used in health-care settings to ascertain how patients are emotionally responding to a serious circumstance, including a cancer diagnosis, heart failure, injuries, assaults, natural disasters, financial stress, or mental illness. 23 It uses a 4-point Likert scale to indicate how frequently each strategy is adopted. The Brief COPE consists of 28 items, which are grouped into 14 coping strategies, which can be further grouped into three overarching coping styles, “Problem-Focused,” “Emotion-Focused,” and “Avoidant coping style.”
The scores for the three overarching coping styles are presented as average scores (sum of item scores divided by number of items), indicating the degree to which the respondent has been engaging in each one of them. 24
QoL was measured by using the Euro-QoL-5D-5L, 25 and the 12-item version of the World Health Organization Disability Assessment Schedule 2.0 (WHODAS 2.0) questionnaire. 26 For both instruments, we used the corresponding Italian version.27,28
The EQ-5D-5L is the most widely adopted generic preference-based QoL measure, including five domains: mobility, self-care, usual activities, pain/discomfort and anxiety/depression. Each domain is assessed with five possible response options ranging from “no problems” to “extreme problems.” The overall health is rated on a visual analog scale (VAS) ranging from 0 “worst imaginable” to 100 “best imaginable.”
The 12-item version of the WHODAS 2.0 is a generic QoL instrument developed by the WHO to provide a standardized method for measuring health and disability across cultures. It was developed from a comprehensive set of International Classification of Functioning, Disability and Health items, that is sufficiently reliable and sensitive to quantify the impact of a surgical treatment.
We chose to include both the WHODAS 2.0 and the EQ-5D-5L instruments, as they offer complementary perspectives on QoL construct. Although the WHODAS 2.0 may be less sensitive to short-term changes—given that it assesses functioning over the previous 30 days—it provides a more comprehensive evaluation of disability and QoL, making it particularly valuable for long-term follow-up assessments (e.g. at 3/12 months). In contrast, the EQ-5D-5L, while more concise, is highly responsive to short-term fluctuations in health-related QoL, thus capturing early post-treatment changes more effectively. 29
All the instruments reported above are widely applied in clinical studies as reported in a recent systematic review. 6
Statistical analysis
Variables are summarized by means with standard deviation, or medians with interquartile ranges (IQRs) or ranges. Normality of the distribution of each questionnaire was tested using the Shapiro–Wilk W-test. Categorical variables were compared using the chi-squared or the Fisher's exact test. Within-group comparisons were carried out using the Wilcoxon signed-rank test. Variables were analyzed only for participants who had complete data across all administered instruments (listwise deletion). Data were analyzed using Stata Statistical Software, version 16 (College Station, TX 77845, USA). All statistical tests were two-tailed; differences were considered statistically significant at an alpha level of .05.
Results
General and clinical variables
A total of 25 patients were assessed before and after elective endovascular treatment. Patient's characteristics are reported in Table 1. Within our cohort, 13/25 (52%) were females. Their mean age was 60 ± 12.5 years (range = 35–81 years). The CVBD treated were in 14 cases aneurysms, (56%), in four cases DAVF (16%), in three cases subdural hematoma (SDH) (12%), in two cases AVM (8%), in one case CCF (4%), while in the last one left-sided carotid stenosis (4%).
Characteristics of the included patients (n = 25) at the baseline.
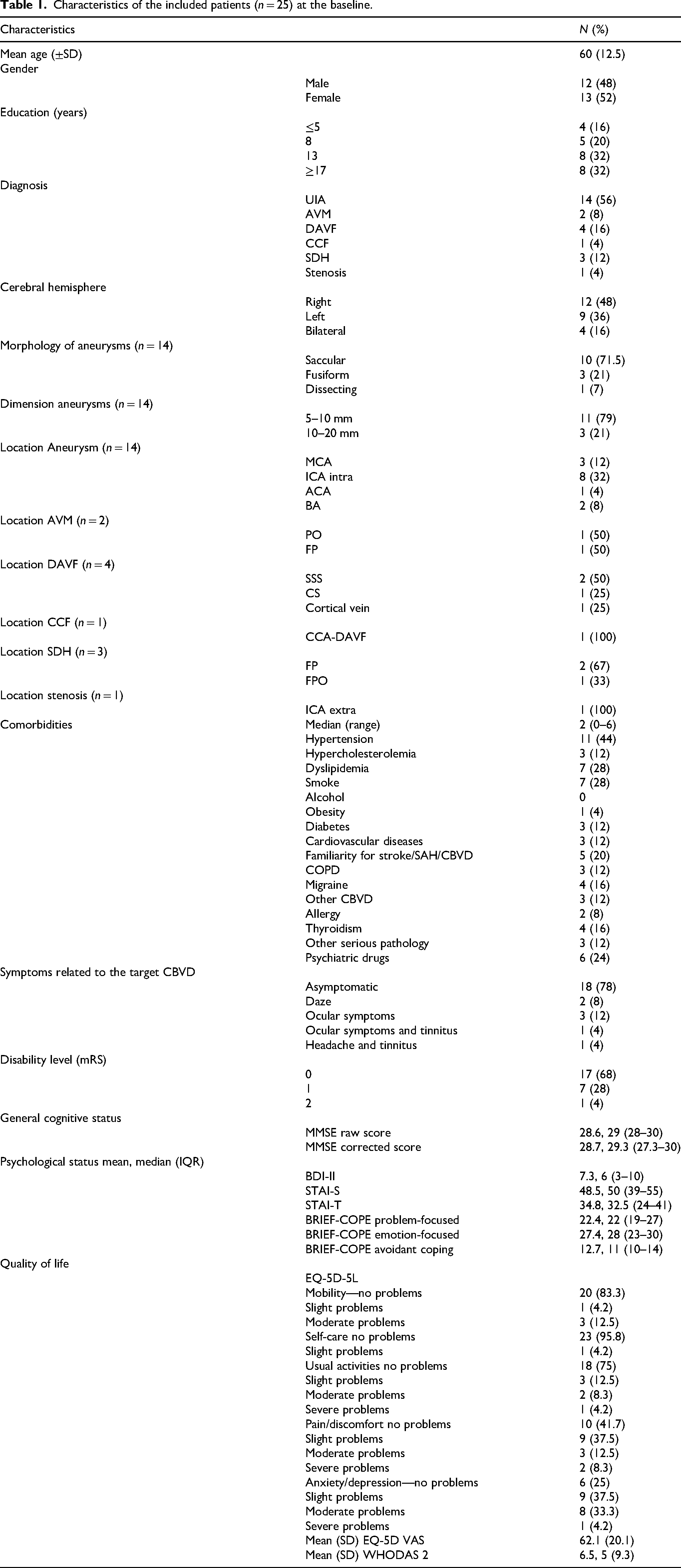
The majority of the diseases were located in the right hemisphere (12; 48%), while nine were in the left one (36%) and four bilateral (16%, SDH). The aneurysm morphology was in 10 cases saccular (71.5%), in three cases fusiform (21.4%) while in one dissecting (7.1%). The dimension of the aneurysms was in 11 cases between 5 and 10 mm (79%), the other four cases ranged between 11 and 15 mm (21%). The exact location of the CBVDs treated are listed in Table 1.
The 25 patients carried a median of two comorbidities (range = 0–6). Among the cardiovascular risk factors, hypertension was the more frequent (11; 44%), followed by psychiatric disorders (6; 24%).
In most patients, CBVD did not cause any symptoms (17; 68%); at baseline mRS was 0 in 14 patients (56%), and there were no patients with a highly compromised general cognitive status (mean MMSE raw score 28.6, range = 28–30).
Index procedures
Descriptive analysis of the elective endovascular procedure performed is detailed in Table 2.
Characteristics of the endovascular procedures.
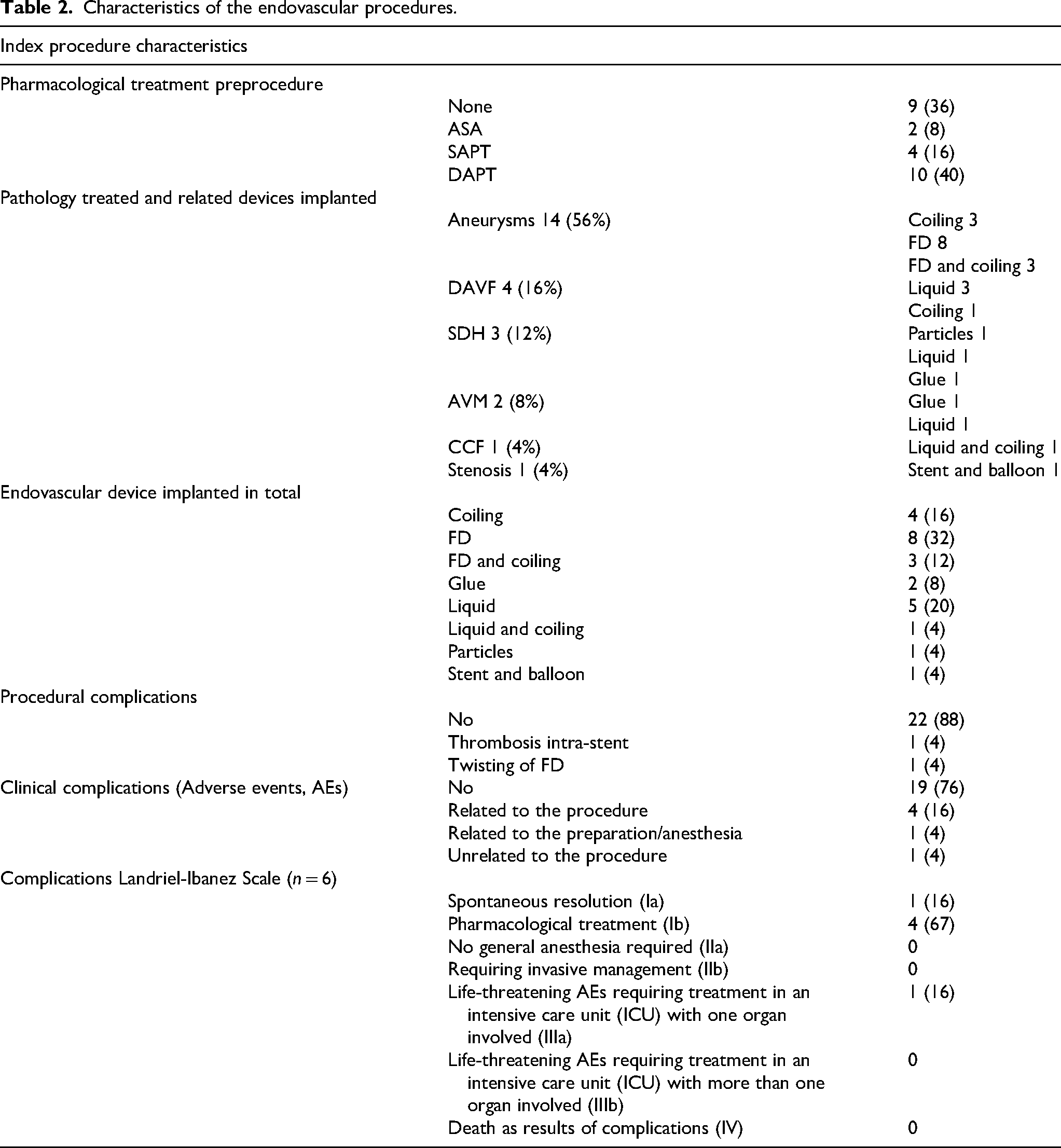
Regarding aneurysmal treatments, eight (32%) patients underwent flow diversion (FD), three coiling (12%), three (12%) were treated with a combination of stent/FD plus coiling, while the rest of CBVD (11; 44%) were treated with stent and angioplasty (carotid stenosis), glue, liquid or particles (AV shunts). Sixteen (64%) patients were pre-treated with antiplatelet therapy.
Two patients suffered from technical procedural complications. In one case an acute intra-stent thrombosis was recanalized with mechanical thrombolysis and additional stent implantation. In the other case, an FD was untwisted via angioplasty.
Four (16%) patients had AEs related to the procedure. One case suffered from right hemiparesis due to ischemic changes visible on MR diffusion-weighted images in the region of the left choroidal artery and the left frontal area (mRS at discharge = 2). The second case presented right lower limb hyposthenia due to ischemic changes visible at MRI (mRS at discharge = 3). These two cases required monitoring in the intensive care unit (level 1b of the Landriel-Ibanez Scale).
The third case upon awakening presented a mild left facio-brachio-crural deficit (mRS at discharge = 0).
The fourth case showed limitation of the right lower extremity movement with mild hypoesthesia (mRS at discharge = 0). These two last cases required pharmacological treatment with steroids (level 1b of the Landriel-Ibanez Scale).
Furthermore, one patient (4%) suffered from an AE related to a bleeding at the cervical central venous catheter implanted by the anesthetist (CVC). This case did not require any treatment besides strict monitoring and spontaneously solved (level 1a of the Landriel-Ibanez Scale).
Finally, an AE unrelated to the procedure involved one patient (4%) affected by pulmonary embolism pharmacologically cured (3a of the Landriel-Ibanez Scale, mRS 0 at discharge).
Clinical outcome
Mean days of hospitalization were 6.72 ± 4.42 (range = 2–24 days).
Most patients (21/25; 84%) had no change in their clinical status compared to admission.
Two patients presented a better mRS at discharge (2/25; 8%, mRs from 1 to 0 and from 2 to 1).
In two complicated cases, due to AEs related to the procedure, the mRS at discharge has worsened (2/25; 8%, mRs from 1 to 3 and from 1 to 2), as described in the previous section (Table 1).
Depressive and anxiety symptoms
At baseline, the mean BDI raw score was 7.28 ± 5.87 (3–10). Most of the patients had no depressive symptoms (20/25; 80%), four showed mild depressive symptoms (16%), and one moderate depression (4%). Women were significantly more depressed than men (p = .0067).
At discharge, the mean BDI raw score was 5.9 ± 5.2, with a percentage of patients without depressive symptoms roughly stable compared to baseline (19/24; 79%), while five (21%) showed mild depressive symptoms. Unfortunately, one patient did not complete the questionnaire.
At baseline, mean STAI-S raw score patients (23/25) were 48.52 ± 11.12; two patients refused to complete the questionnaire. Most of the patients (17/23; 74%) showed anxiety symptoms: four at mild level (4/23, 17%), ten at moderate level (10/23, 43%), and three at severe level (3/23, 13%). Women had a state-anxiety score significantly more severe than men (p = .0163).
At discharge, the mean STAI-S raw score was 37.58 ± 10.43 (24/25); one patient did not complete the questionnaire. The majority of patients (15/24; 62%) showed no state-anxiety symptoms, five (5/24, 21%) mild state-anxiety, three (3/24, 12%) a moderate level, and one (1/24, 4%) a severe level.
At baseline, the mean STAI-T raw score was 34.75 ± 10.47 (24/25); one patient did not complete the questionnaire. Eighteen patients (18/24; 75%) showed no trait-anxiety, three (3/24 12%) presented a mild one while other three (3/24; 12%) reported moderate symptoms. In addition, women had a trait-anxiety score significantly higher than men (p = .0195).
At discharge, the mean STAI-T raw score was 34.9 ± 11.61; one patient did not complete the questionnaire. Most patients (10/24; 71%) showed no trait anxiety, five (5/24; 21%) showed mild trait-anxiety, while other two (2/24 8%) moderate.
The groups analysis at discharge (T-test) demonstrated that both BDI raw scores and the STAI-S raw scores, significantly improved from baseline (p < .01) (Figure 2).
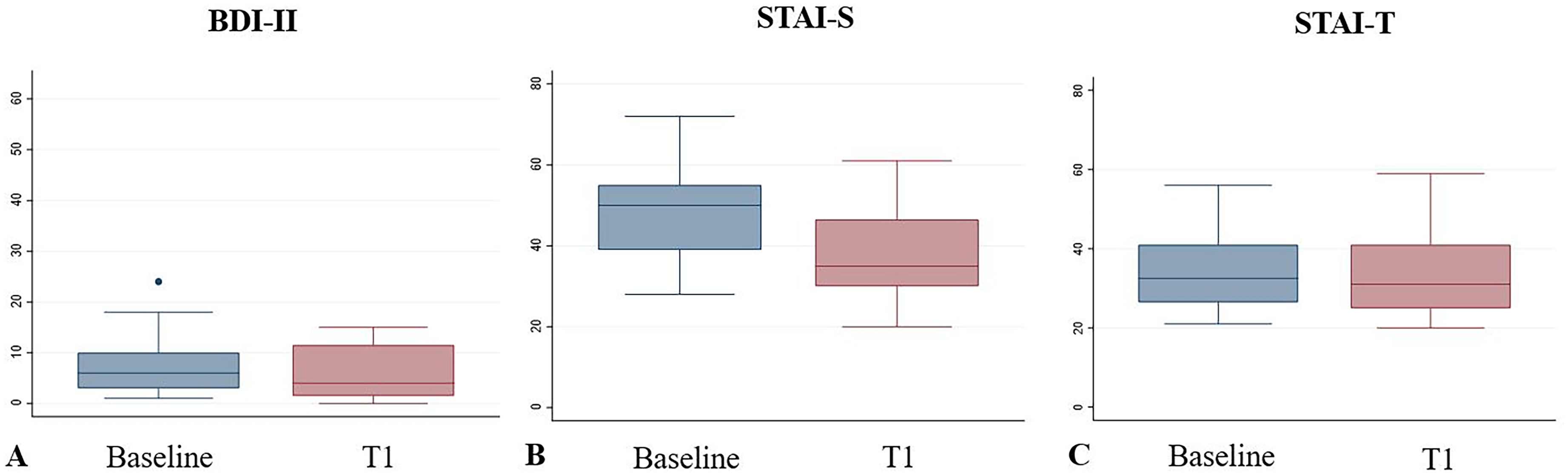
Box plots of BDI-II scores at the baseline, and at discharge. The boxes represent the IQR, horizontal lines inside boxes represent medians and tails represent the 5th–25th and 75th–95th percentile range. Dots are outliers. BDI-II, Beck Depression Inventory-II.
Coping
Two patients did not complete the Brief-COPE questionnaire (23/25). At the baseline, mean Problem-focused score was 22.4 ± 4.5, mean Emotion-focused was 27.4 ± 6.1, and mean Avoidant profile was 12.6 ± 3.5.
At discharge (22/25), mean Problem-focused profile was 22.7 ± 4.5, mean Emotion-focused profile was 28.5 ± 6.1, and mean Avoidant profile was 12.4 ± 3.2. At this moment three patients did not complete the questionnaire.
The groups analysis showed no differences in scores at discharge compared to baseline, as shown in Figure 3.
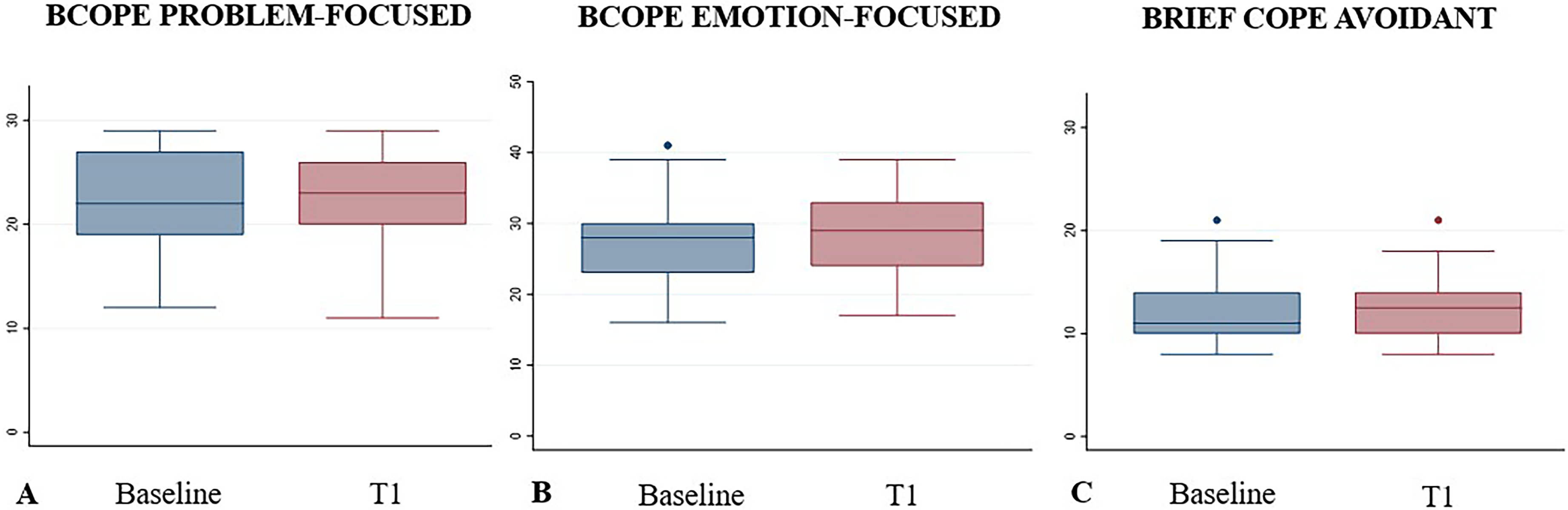
Box plots of Brief-COPE scores at baseline, and at discharge. The boxes represent the IQR, horizontal lines inside boxes represent medians and tails represent the 5th–25th and 75th–95th percentile range. Dots are outliers.
Quality of life
As for the EQ-5D-5L (24/25), at baseline most patients (18/23; 75%) reported slight to severe problems in the anxiety/depression domain, while having no issues in the remaining items.
At discharge, the majority of patients (24/25) reported slight to moderate problems for pain/discomfort (15/24; 62%) domain, with no issues in the other fields.
At baseline, mean EQ-5D VAS was 62.13 ± 20.01(23/25). Two patients did not complete the scale. At discharge, the mean EQ-5D VAS was 67.7 ± 21.8 (24/25). Only one patient did not complete the EQ-5D-5L questionnaire.
At baseline, the mean WHODAS 2.0 was 6.5 ± 9.22, and most of the (22/24) patients (92%) scored for no disability. Only one patient did not complete the form.
At discharge, the mean WHODAS 2.0 was 8.16 ± 8.99, and seventeen out of 24 patients (71%) did not recorded disability. Even in this case, one patient did not complete the questionnaire.
Group analysis indicates no changes in EQ-5D VAS and WHODAS 2.0 scores at discharge compared to baseline (Figure 4).
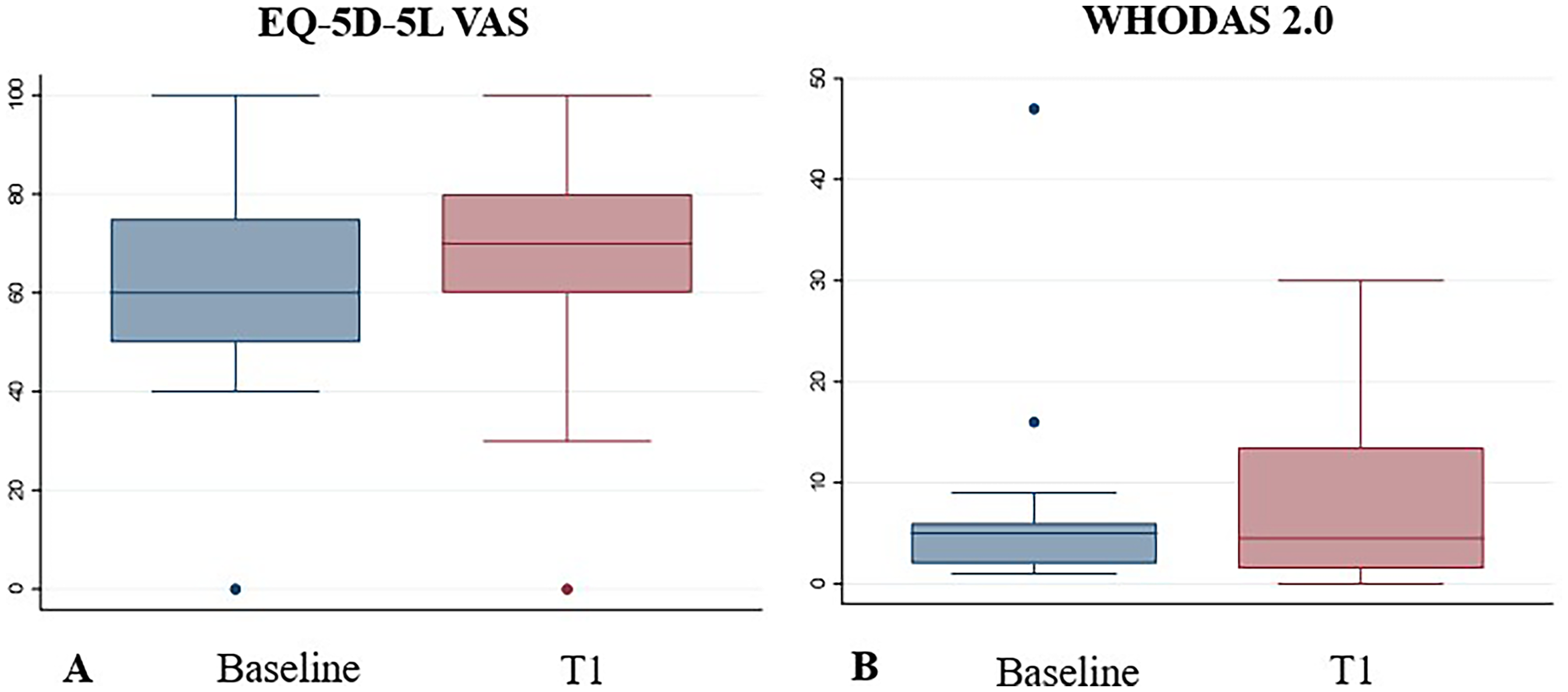
Box plots of EQ-5D VAS and WHODAS 2.0 scores at baseline, and at discharge. The boxes represent the IQR, horizontal lines inside boxes represent medians and tails represent the 5th–25th and 75th–95th percentile range. Dots are outliers.
Discussion
Currently, endovascular treatment is considered one of the first-line strategies for CBVD. However, studies on mental health in CBVD patients treated with elective neuroendovascular intervention are scarce and with discordant results. Most of the studies regarding CBVD, especially on incidentally discovered cerebrovascular malformations, have focused on functional clinical outcomes. However, a few studies have explored and reported psychological outcomes, which are equally important in a holistic approach to the patient's wellbeing.30,31 Our study aims to reduce this gap by assessing anxiety and depressive symptoms, coping strategies and QoL before and after the elective neuroendovascular treatment.
Our results show statistically significant reduction in depressive symptoms and state-anxiety (i.e. response to a specific situation) at discharge, with no changes in trait-anxiety scores. Although patients may not have fully recovered from recent treatment, they already appeared to show improvement in anxiety and depression symptoms by the time they were discharged, likely due to relief at being treated. Notably, the reduction in state-anxiety was not only statistically significant but also clinically meaningful, as patients shifted from a level indicative of mild anxiety to one consistent with the absence of anxiety.
The threat of stroke coming from the CBVD becomes the most obvious cause of preoperative anxiety and depressive symptomatology. 4 Furthermore, it is also important to consider the stressful nature of the informed consent process and preoperative preparations. 32 All these factors may explain the higher state-anxiety scores at baseline in most of our patients (17/23; 74%). Anxiety is known to negatively influence cognitive performance; therefore, when performing neurocognitive assessment, the neuropsychologist must consider the relationship between psychological status and cognitive performance. 33 Concerning the elective treatment of individuals carrying an unruptured aneurysm, Lim et al. recommend carefully assessing information on treatment-related long-term psychological effects, such as depression. 32 Based on our results, we strongly suggest applying this paradigm also to other types of CBVD, such as AVM and DAVF.
Furthermore, studying the CBVD patients’ psychopathological status could help reveal a possible association between psychiatric traits and CBVD, with future implications in primary prevention strategies. 34
For those with a positive history of psychiatric or psychological symptoms, monitoring during the initial post-operative years may be beneficial, and some might also gain from individual psychotherapeutic treatment. In our series there were six patients under treatment for previous psychiatric disorders. The exploratory analysis showed that, already at baseline, they had significantly higher levels of depressive and trait-anxiety symptoms compared to the rest of the cohort. We are aware that this result should be cautiously interpreted, due to our small sample size.
Regarding the possible psychotherapeutic support in patients with unruptured aneurysm, Lemos et al. 35 have applied cognitive behavioral therapy (CBT) in untreated ones. They concluded that CBT reduced not only emotional symptoms but also illness perception. Similarly, CBT could be helpful in CBVD cases undergoing treatment.
Concerning quality of life, scores in our series showed no significant differences between baseline and discharge. Probably, patients were still recovering from procedure and hospitalization. Our hypothesis is that quality of life may improve over time; continued implementation of our study with one-year follow-up assessments will provide the answer.
QoL has been identified as one of the most important outcomes measures when assessing preventive treatment of CBVD. 36 In fact, functional or objective outcomes may not represent the personal experience lived by the patient. Therefore, it is important for the physicians to be aware of the preoperative psychological status of their patients, being mindful of the possible influence on treatment decision-making. 37 Few studies suggested that patients with UIA at the baseline had a reduced QoL due to their psychological status, in comparison to the general population. 4 Conversely, Dandurand et al. 36 reported that a major procedure such as preventive aneurysm treatment did not affect QoL. The literature on this topic is still scarce and debatable. Further studies investigating QoL and their postoperative changes over time are necessary. 4
As in other published studies, regarding coping strategies, 38 we did not detect any significant modifications from baseline to discharge. Interestingly, as for Problem-focused coping style, we observed in our cohort moderate to high scores both at baseline and after the procedures, indicating that patients favor a practical approach to problem solving.
Concerning the Emotion-focused coping style, in our study we registered moderate scores, indicating that patients were quite capable of regulating the emotions associated with the stressful situation. Scores of Avoidant copying style resulted low, indicating a tendency to adaptive coping strategies. These results underline the tendency of our population to be active towards the problems, focusing their actions on finding a solution and managing their emotions accordingly. Our findings align with Fukase et al., 39 who discovered that adaptive coping strategies are more prevalent among middle-aged patients, which constitutes most of our cohort.
Finally, the psychological variables could be further investigated by assessing the impact of direct endo- and extra-luminal cerebrovascular manipulation of cerebral arteries on the hypersecretion of the vaso-active and psychoactive neuropeptide Y, both in coiling and clipping procedure, as described by Bründl et al. 40 Elucidating the psychological interactions of the neuropeptide Y system with treatment maneuvers could help better understanding the neurobehavioral recovery in CBVD patients. In our study we did not investigate the biochemical changes related to endovascular treatment since we mainly focus on psychological and QoL measures. In the next future, we hope to implement this kind of analysis in a larger cohort of patients.
The main strength of our study is the prospective nature, in contrast with most of the others available in literature on the same topic, based on retrospective design. 7 Moreover, having considered elective procedures, which are rarely the topic of research, we studied a sample without the confounding factors of patients treated for CBVD in emergency.
The main limitation of this study is the small sample size, which does not allow us to infer statistically much from the data collected. The small number of cases influences the possibility of drawing definitive conclusions, emphasizing the need for larger studies to better understand the risks and outcomes associated with endovascular treatments.
Although the continuous growth of our sample size will contribute to elucidating interactions between psychological and clinical outcomes, larger and multi-centric prospective longitudinal studies remain needed.
On this regard, standardization of instruments across centers and cultures is becoming necessary to accurately determine key variables to be investigated and to compare series and outcomes. 32
Conclusion
Our study highlights the importance of exploring the complexities of psychiatric and psychological disorders in patients with chronic vascular disease (CBVD). Assessing whether enhancements to the current treatment pathways for CBVD patients can lead to reductions in anxiety improving overall wellbeing is crucial.
Such improvements may include better access to mental health resources, personalized treatment plans, and integrated care approaches that consider both physical and mental health needs.
By focusing on these areas, researchers can help inform clinical practices and policies that aim to support the mental health of CBVD patients, ultimately leading to better health outcomes and enhanced quality of life.
In the future, involving multiple centers and extending the duration of follow-up could help gather more comprehensive data on various contributing factors, such as social, environmental, and biological influences on mental health of our CBDV patients.
Footnotes
ORCID iDs
Ethical approval
The ONIRIC research project is carried out (Outcomes in Neurointerventional Radiology Indications and Complications) in accordance with the principles laid down in the Declaration of Helsinki, approved by our Ethics Committee, Lombardy Region, section Fondazione IRCCS Istituto Neurologico Carlo Besta (internal ref: 01/2022; amendment approved 8 March 2023, internal ref: 13).
Consent to participate
All participants provided written informed consent prior to enrolment in the study.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Italian Ministry of Health (RC 2025).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability
The data that support the findings of this study are available from the corresponding author, Milani Matteo, upon reasonable request.