
Abstract
Background
First-pass effect (FPE) in endovascular thrombectomy (EVT) is strongly associated with clinically favorable outcomes. Atrial fibrillation (AF)-related strokes have been shown to be associated with greater rates of FPE in acute large vessel occlusions (LVOs). In this study, we aimed to assess the association between AF and achieving FPE in medium vessel occlusions (MeVOs).
Methods
A prospectively maintained registry of adult ischemic stroke patients at a comprehensive stroke center between October 2019 and October 2023 was retrospectively screened for inclusion. Patients undergoing EVT for a MeVO were included. Univariable and multivariable logistic regressions with 2500 bootstrap iterations for FPE and mFPE was performed using covariables that were clinically and/or statistically significant. Adjusted odds ratios with 95% confidence intervals (CIs) were reported. Regression performance was assessed using area under the curve (AUC) from receiver operating characteristics curve analysis.
Results
34.4% of patients with MeVO achieved FPE and 58.2% achieved mFPE. In multivariable logistic regression models, AF was independently associated with lower likelihood of FPE, and AF and prior antiplatelet/anticoagulant use were independently associated with lower likelihood of mFPE. Models for FPE and mFPE had AUCs of 0.80 (95% CI [0.75–0.85]) and 0.86 (95% CI [0.78–0.94]), respectively.
Conclusion
AF was associated with a significantly lower likelihood of FPE and mFPE in EVT of MeVOs. This may suggest a need to prepare for additional passes and rescue intraprocedural strategies for MeVO in patients with AF.
Introduction
Endovascular thrombectomy (EVT) is the standard of care for acute ischemic stroke (AIS) treatment. 1 The first-pass effect (FPE), or the ability to achieve complete reperfusion following a single pass, is a valuable indicator of clinically favorable outcomes following EVT, associated with improved functional outcomes, lower rates of symptomatic intracranial hemorrhage, and mortality. 2 Similar benefits of FPE have also been seen in medium vessel occlusions (MeVOs).3–5
The rate of FPE for large vessel occlusions (LVOs) and MeVOs in multicenter registries have ranged from around 20% to 60%.3,6–11 Numerous factors, including clot composition, interventional approach, patient comorbidities and vasculature impact the ability to achieve FPE. Predictors of complete FPE in LVO have been found to be older age, female gender and use of balloon guide catheters. 6 However, factors influencing the rate of FPE in MeVOs are not as well-characterized.
Atrial fibrillation (AF) is a major risk factor for cerebrovascular stroke, with the relative risk of stroke in patients with AF ranging from 5.6 to 17.6 of that observed in patients without AF.12–14 Although AF is commonly associated with LVOs, MeVOs can also be seen with AF.15–17 In a recent study analyzing DIRECT-SAFE data, AF-related strokes were associated with significantly higher rates of FPE in LVO AIS. 18 In this study, we assess the association between AF and achieving FPE in MeVOs treated with EVT.
Methods
Deidentified data are available from the corresponding author upon reasonable request. This analysis was approved by the institutional review board with waiver of informed consent, and results were reported in accordance with the Studies in Epidemiology guidelines.
Patients
Patients receiving care at a comprehensive stroke center between October 2019 and October 2023 were retrospectively screened for inclusion from a prospectively maintained database of consecutive adult ischemic stroke patients. Patients were included if they had evidence of an MeVO in a middle cerebral artery segment on computed tomography (CT) angiography and were treated with thrombectomy.
Data collection
Demographic data collected included age, sex, and comorbid conditions. Stroke-related data collected included Alberta Stroke Program Early CT Score (ASPECTS) from noncontrast CT, relative occlusion location (proximal: distal M2 branches, distal: M3/M4 branches), and laterality of occlusion from CT angiography. Decision to pursue thrombolytic treatment and thrombectomy treatment was per multidisciplinary stroke team consensus. First-line thrombectomy approach (i.e. aspiration-only or combination of aspiration and stent-retriever) and devices used intraprocedurally was per the neurointerventionalist's discretion. Clinical outcomes collected included discharge and 90-day modified Rankin Score (mRS).
Outcomes
The primary outcome was FPE, defined as achieving modified Treatment in Cerebral Infarction (mTICI) 2C or 3 after the first thrombectomy pass. The secondary outcome was the modified FPE (mFPE), defined as achieving mTICI 2B, 2C, or 3 after the first thrombectomy pass.
Statistical analysis
Continuous data were summarized as medians with interquartile ranges (IQR); categorical data were summarized as frequencies. Baseline demographics were analyzed with the entire cohort, and then when stratified by FPE and mFPE. Univariable and multivariable logistic regressions with 2500 bootstrap iterations were performed for the outcome of FPE and mFPE using covariables that were clinically and/or statistically significant: age, sex, hypertension, hyperlipidemia, diabetes mellitus, coronary artery disease, AF, prior stroke, tobacco use, antiplatelet/anticoagulant use, premorbid mRS, admission National Institutes of Health Stroke Scale, ASPECTS, laterality of occlusion, relative occlusion location, thrombolytic administration, and thrombectomy approach (combination aspiration/stent-retriever vs aspiration-only). Adjusted odds ratios (aORs) with 95% confidence intervals (CI) were reported. Regression performance was assessed using area under the curve (AUC) from receiver operating characteristics curve analyses. Missing data was minimal and not imputed. Significance was prespecified at p ≤ .05. Statistics were conducted in JMP v18.0.0 (SAS Institute, Inc., Cary, NC).
Results
Of 67 patients meeting inclusion, the median age was 70 years (IQR 63–82), and 49.3% (33/67) were female (Table 1). The most common comorbid condition was hypertension (82.1%, 55/67) (Table 1). Approximately one-third of patients had AF (34.3%; 23/67) (Table 1). Most patients had proximal MeVOs (88.1%; 59/67) (Table 1). Thrombolytics were administered in 34.3% (23/67) of patients, and most patients were treated with aspiration-only thrombectomy (61.2%; 41/67) (Table 1).
Baseline demographics.
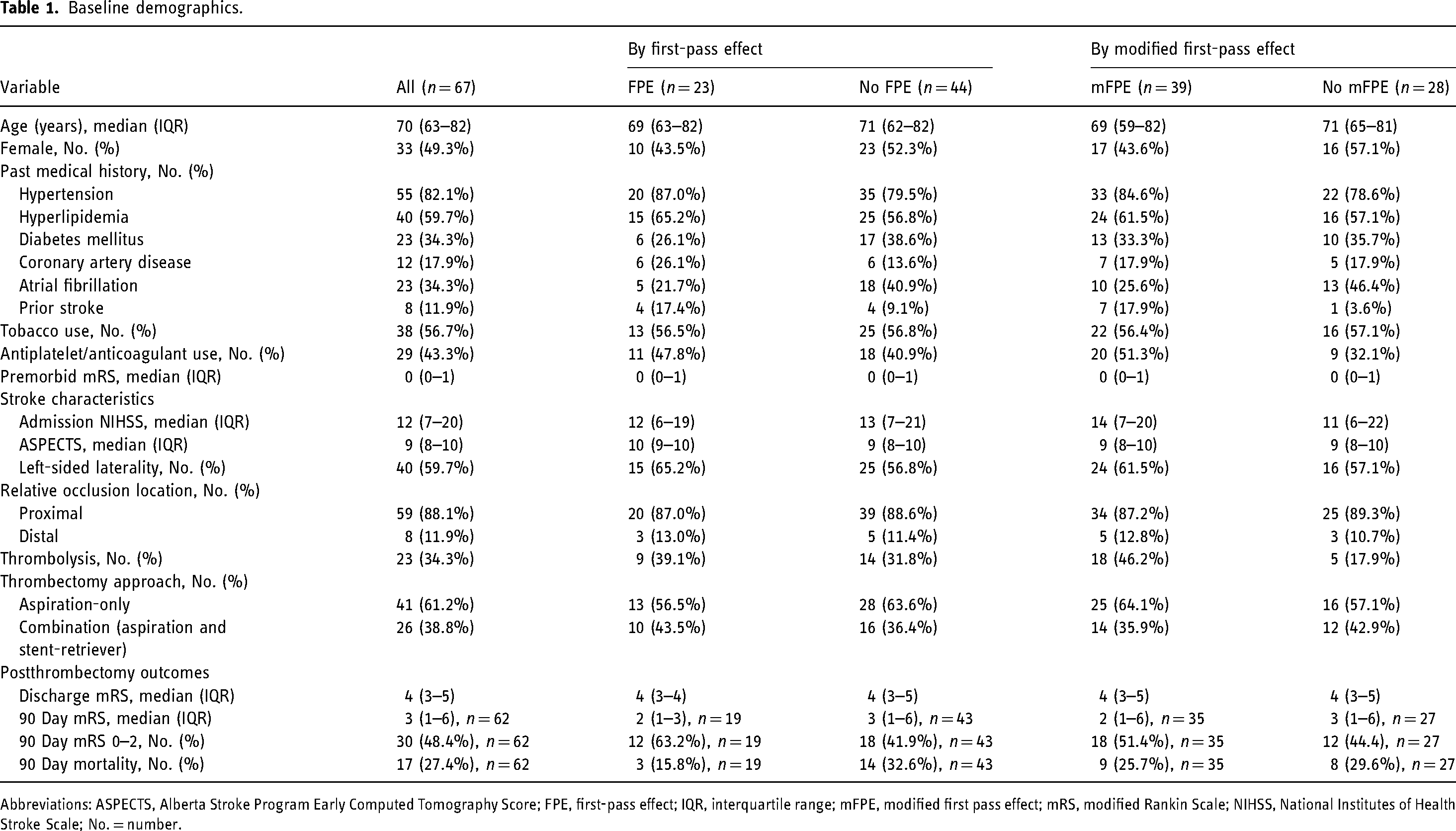
Abbreviations: ASPECTS, Alberta Stroke Program Early Computed Tomography Score; FPE, first-pass effect; IQR, interquartile range; mFPE, modified first pass effect; mRS, modified Rankin Scale; NIHSS, National Institutes of Health Stroke Scale; No. = number.
First-pass effect
One-third of MeVO patients achieved FPE (34.3%; 23/67) (Table 1). In a multivariable logistic regression model, only AF (Yes vs No (Reference), aOR 0.08, 95% CI [0.01–0.63], p = .02) was significantly associated with FPE (Table 2). The multivariable regression had AUC of 0.80 (95% CI [0.75–0.85]).
Logistic regression for first pass effect in medium vessel occlusion thrombectomy.
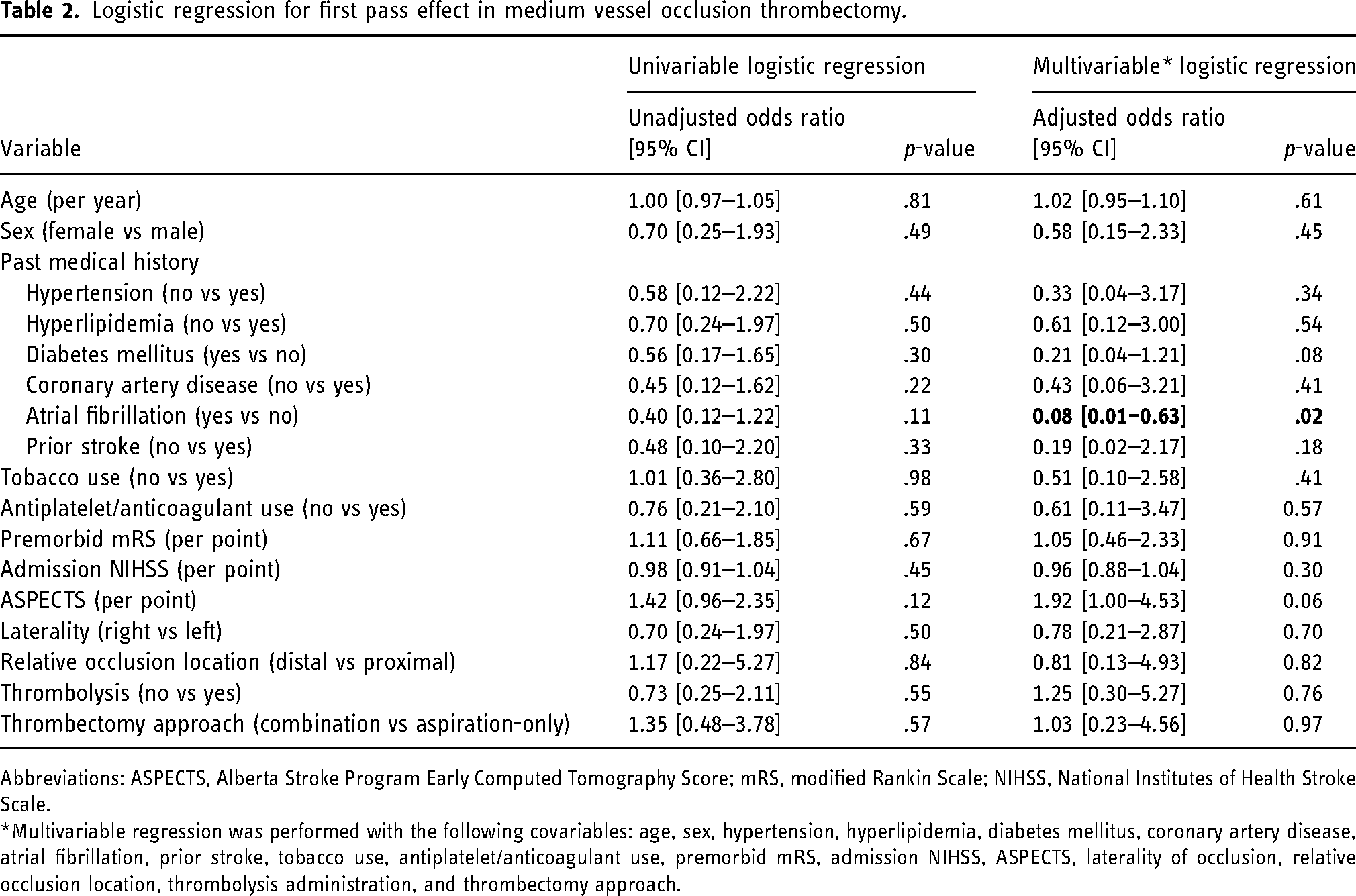
Abbreviations: ASPECTS, Alberta Stroke Program Early Computed Tomography Score; mRS, modified Rankin Scale; NIHSS, National Institutes of Health Stroke Scale.
*Multivariable regression was performed with the following covariables: age, sex, hypertension, hyperlipidemia, diabetes mellitus, coronary artery disease, atrial fibrillation, prior stroke, tobacco use, antiplatelet/anticoagulant use, premorbid mRS, admission NIHSS, ASPECTS, laterality of occlusion, relative occlusion location, thrombolysis administration, and thrombectomy approach.
Modified FPE
Over half of MeVO patients achieved mFPE (58.2%, 39/67) (Table 1). In a multivariable logistic regression model, AF (Yes vs No (Reference), aOR 0.04, 95% CI [0.01–0.49], p = .01) and prior antiplatelet/anticoagulant use (No vs Yes (Reference), aOR 0.05, 95% CI [0.01–0.71], p = .03) were significantly associated with mFPE (Table 3). The multivariable regression had AUC of 0.86 (95% CI [0.78–0.94]).
Logistic regression for modified first-pass effect in medium vessel occlusion thrombectomy.
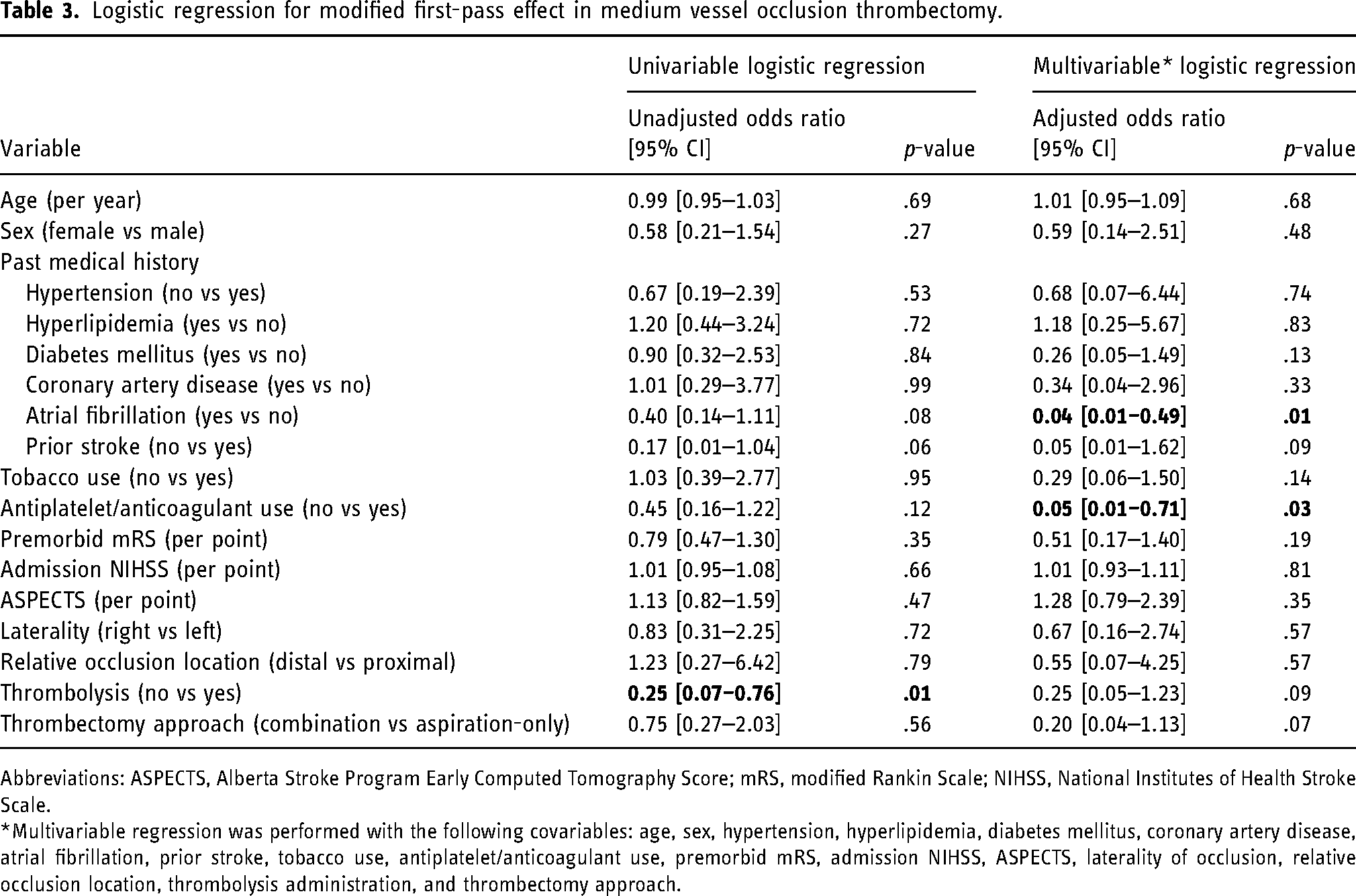
Abbreviations: ASPECTS, Alberta Stroke Program Early Computed Tomography Score; mRS, modified Rankin Scale; NIHSS, National Institutes of Health Stroke Scale.
*Multivariable regression was performed with the following covariables: age, sex, hypertension, hyperlipidemia, diabetes mellitus, coronary artery disease, atrial fibrillation, prior stroke, tobacco use, antiplatelet/anticoagulant use, premorbid mRS, admission NIHSS, ASPECTS, laterality of occlusion, relative occlusion location, thrombolysis administration, and thrombectomy approach.
Discussion
FPE is strongly associated with improved clinical outcomes following AIS for patients treated with EVT, correlated with better functional outcomes, less vascular injury, lower risk of clot fragments, and decreased time to reperfusion.2,6,19 Previous studies have shown an association between AF and achieving FPE during EVT for LVO, however, this association has yet to be widely investigated for MeVOs. 18 In our study, AF was significantly associated with lower odds of FPE and mFPE in MeVOs treated with EVT. Clinically, this may suggest a need to prepare for additional passes and rescue intraprocedural strategies to achieve reperfusion in EVT of MeVO patients with AF.
Our results contrast with previous studies showing a positive association between AF and achieving FPE during EVT for LVOs. This suggests that the intraprocedural course in MeVOs may differ from that in LVOs in patients with AF, including aspects such as clot composition, location, and size. Erythrocyte-rich clots are associated with higher rates of successful recanalization than fibrin-rich clots; however, studies investigating the composition of cardioembolic clots have yielded heterogeneous results.20–22 A substudy of the DIRECT-SAFE trial hypothesized that the higher rate of FPE achieved in LVO patients with AF was due to mature, fibrin-rich, cardioembolic clots that are less likely to disintegrate or embolize. 18 In contrast, we postulate that these physical properties of cardioembolic thrombi associated with AF may predispose to more difficult thrombectomy courses when targeting MeVOs in comparatively narrower, more distal cerebrovasculature.
Limitations
Limitations of this study include factors inherent to the retrospective study design, including selection bias and confounding. The study was conducted at a single center, which limits generalizability. Future multicenter studies in a larger, diverse cohort are necessary to validate these results.
Conclusion
AF is associated with lower odds of FPE and mFPE in MeVOs treated with EVT. This may suggest a need to prepare for additional passes and rescue intraprocedural strategies for MeVO in patients with AF.
Footnotes
Acknowledgments
We would like to acknowledge the Cooper Acute Stroke Registry team, including stroke coordinators, research coordinators, physicians, medical students, technicians, and nurses, for their contributions.
Consent to participate
Requirement for informed consent has been waived by the IRB.
Data availability statement
Deidentified data may be made available upon reasonable request.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: TGJ is a consultant for Anaconda, Route 92 Medical, Viz.Ai, FreeOx, Blockade Medical, and MeThinks. He serves in an advisory capacity for Cerenovus and Contego Medical. He has equity in Corindus. He receives research support from Medtronic and Stryker. All other authors have no relevant disclosures to declare.
Ethical approval
This study was approved by the Cooper Hospital Institutional Review Board with waiver of informed consent (IRB# 20-371).
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.