
Abstract
Introduction
While epidural blood patch can be an effective management option in lumbar pseudomeningoceles in certain clinical settings, its utility in the cervical spine is unclear. The aim of this study was to evaluate the safety and effectiveness of percutaneous aspiration and autologous blood patch for post-operative durotomy related pseudomeningoceles within the cervical spine.
Methods
A single institution retrospective review detailing 3 patients with durotomy related pseudomeningocele following posterior cervical spine surgery was completed.
Results
In all three cases, aspiration with subsequent injection of autologous epidural blood patch successfully treated each pseudomeningocele. One patient required more than one intervention, while the other two were successfully treated after one procedure. All three patients improved clinically without need for additional surgery.
Conclusion
Percutaneous aspiration and epidural blood patch can be used to safely manage post-operative pseudomeningoceles within the posterior cervical spine.
Introduction
Pseudomeningoceles are cerebrospinal fluid (CSF) leaks that result from an opening in the dural-arachnoid layer that results in an extra-dural accumulation of spinal fluid. Among iatrogenic etiologies, durotomy related pseudomeningoceles are a rare complication that can occur following posterior cervical spine surgery. Dural tears have an estimated incidence between 0.8% to 3.9% follow posterior cervical spine surgery, with 7% to 32% of these tears requiring additional intervention for persistent CSF leak. 1 Management of post-operative cervical durotomy related pseudomeningoceles is variable and includes lumbar drain placement, bed rest, and possibly revision surgery in refractory cases. Regarding post-surgical lumbar pseudomeningoceles, image-guided percutaneous aspiration with blood patch has been shown to be an effective, albeit infrequently reported, management strategy of this complication in certain clinical settings.2–6 While several case-series have suggested that this method may be used successfully within the lumbar spine, there exists a paucity of literature documenting if this strategy can be used safely and successfully in the cervical spine. Here, we present our experience using percutaneous aspiration with autologous blood patch in managing complicated post-operative cervical pseudomeningoceles.
Methods
We retrospectively identified all of the patients at our single centre institution who underwent a percutaneous image-guided aspiration and autologous blood patch for management of a post-operative pseudomeningocele following posterior cervical spine surgery. Ultimately, three patients were identified on who the procedure was attempted. The patients’ clinical history, hospital and treatment courses, and pertinent image were subsequently collected and presented. IRB was not required by our institutional due to the small size of the presented case-series.
Prior to the procedure, coagulation labs are ordered and verified to be within normal limits to reduce the risk of an expanding hematoma after blood patch administration. Identifying the location of the suspected leak is imperative as the blood patch should be performed as close to that site as possible. All patients should have a pre-procedure non-contrast MRI with sagittal T1, T2, and Short-Tau Inversion Recovery (STIR) sequences, as well as axial T2 sequences. The site of leak typically has a finger-like extension of fluid arising from the dura of the laminectomy site communicating dorsally with a larger superficial fluid collection. From a technical perspective, the procedure was performed with the patient in the prone position under CT fluoroscopic guidance. A radiopaque grid was placed over the dorsal neck and a limited non-contrast planning scan was performed to localize the site of leak and percutaneous access point. The skin was then marked and the needle path was measured to determine the needle length needed. Subsequently, local anesthetic was administered at the spinal level of interest Next, an 18-gauge Quincke spinal needle was advanced into the subfascial midline posterior to the appropriate spinal level of the pseudomeningocele. The needle is advanced until the tip is located as close to the posterior edge of the dura but within the fluid collection. Care is made not enter the thecal sac. 3.5-inch needles are almost always adequate for reaching the target depth. However, larger edematous patients may need 5-inch or 6-inch needles. Depth is confirmed with CT fluoroscopy set at a 2.5mm slice thickness. Furthermore, a small injection of air can also be performed to confirm extradural/extrathecal placement. Iodinated contrast is not typically needed as the combination of CT visualization and injected air allow for adequate visualization of the pertinent anatomy. At this point, the collection is aspirated. If possible, the pseudomeningocele is aspirated completely to collapse the CSF cavity. Careful attention is then made to keep the needle firmly in place within the collapsed cavity just overlying the suspected dural leak site. Multiple 10-cc syringes are then used to draw blood from a peripheral IV, usually located in an upper extremity. The autologous blood should be injected within 30 s of draw to prevent clotting within the syringe. The amount of blood injected is determined based on the patient's symptoms. When patients begin to complain of upper extremity radicular symptoms, or experience chest pressure or paresthesias, the injection would be halted. Alternatively, if the proceduralist begins feeling resistance to injection, the blood patch would also be halted. Both of these are surrogate markers for the creation of a significant extradural pressure gradient to prevent the egress of CSF through the dural leak. Of note, the volume of injected blood is usually equal to slightly less than the amount of fluid that was aspirated.
Results
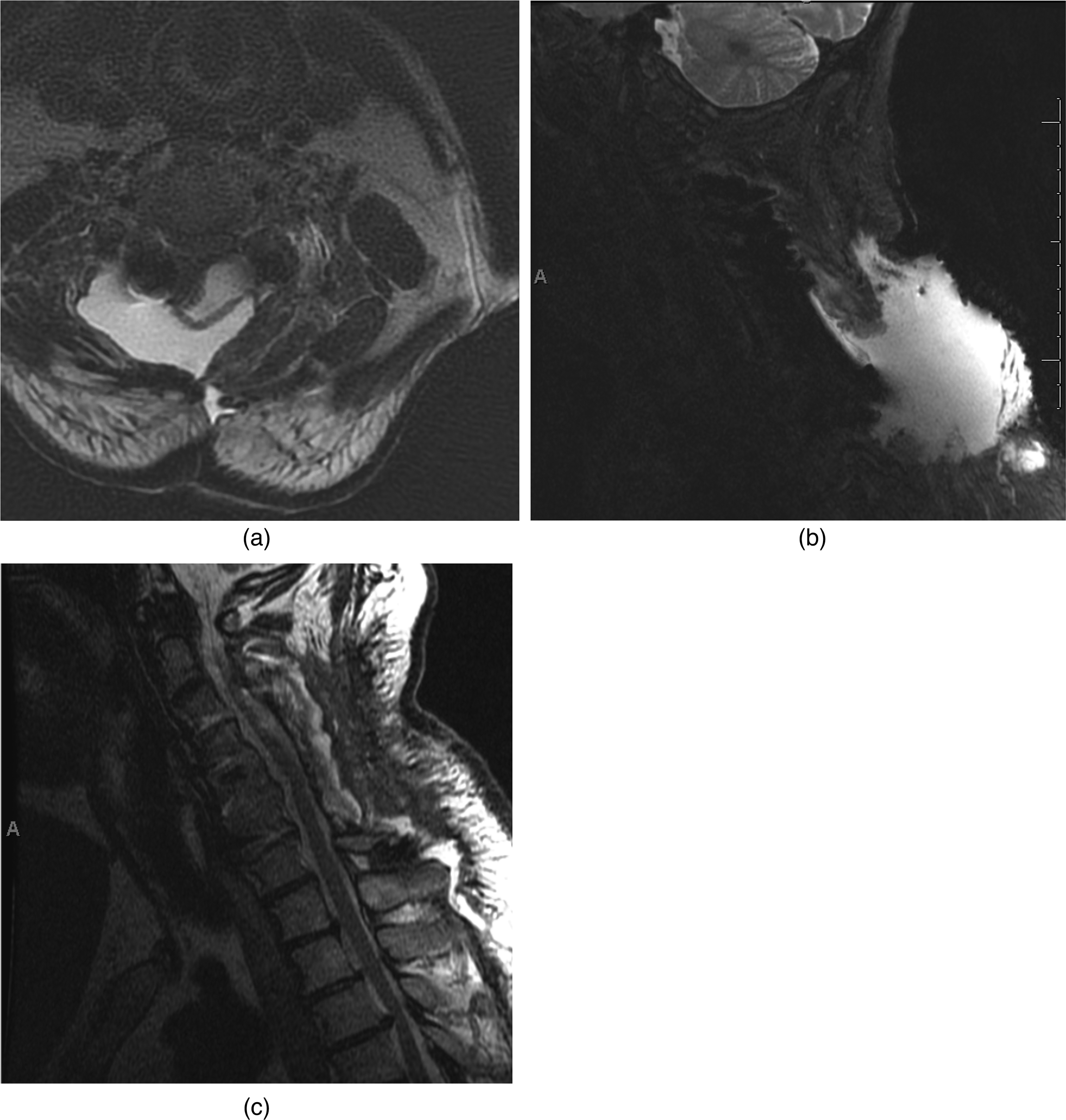
(a) Axial T2-weighted MRI imaging demonstrating no CSF signal around the spinal cord. (b) Sagittal T2-weighted MRI of the cervical spine demonstrating large posterior pseudomeningocele, prior to intervention. (c) MRI image demonstrating resolution of pseudomeningocele after percutaneous aspiration and blood patch.
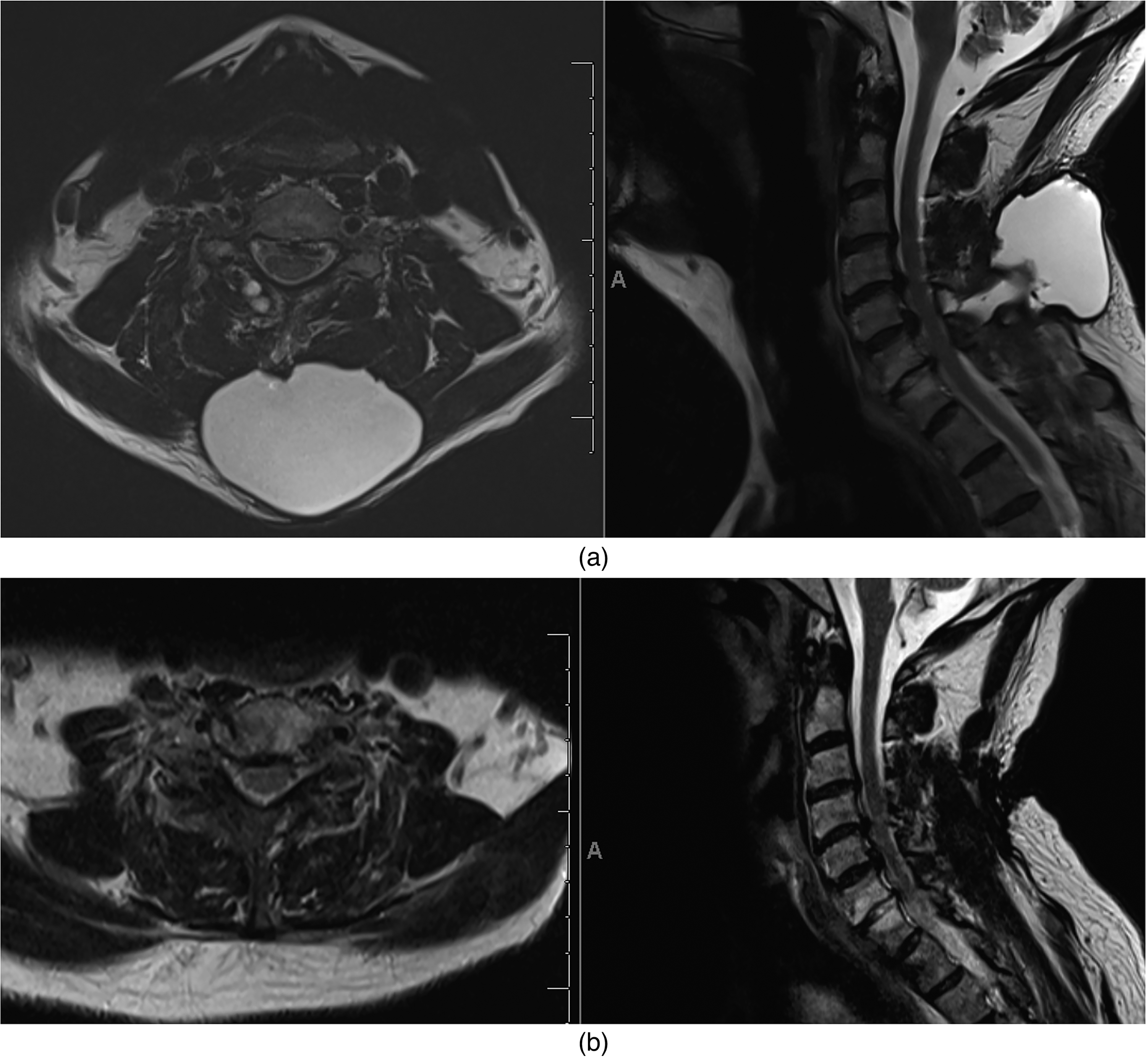
(a) Axial and sagittal T2-weighted MRI images demonstrating large posterior cervical spine pseudomeningocele prior to intervention. (b) Correlative axial and sagittal post-interventional images demonstrating near complete resolution of pseudomeningocele following percutaneous aspiration and epidural blood patch.
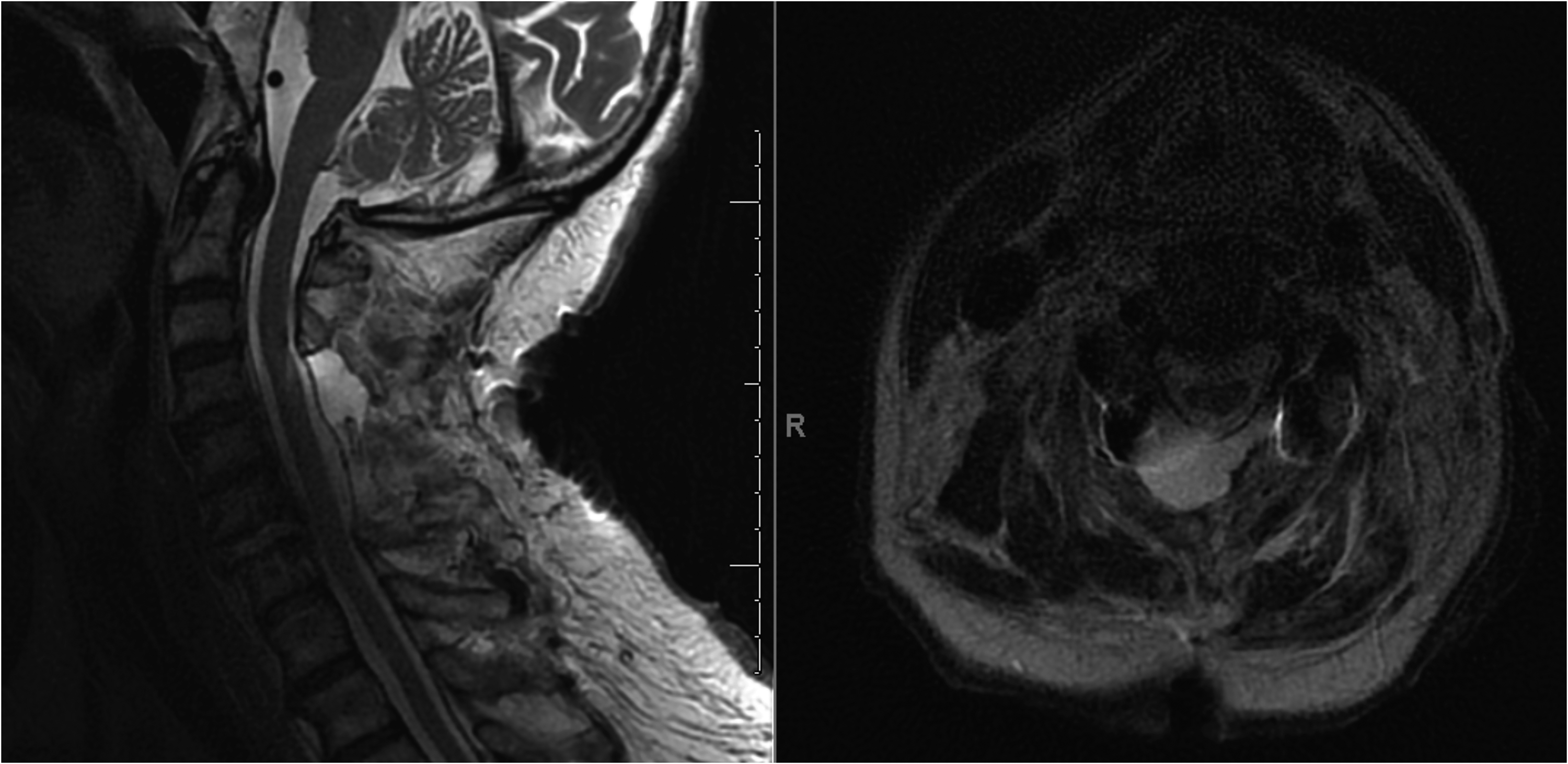
Sagittal and axial T2-weighted MRI images demonstrating pseudomeningocele prior to intervention. No follow up images were obtained.
Conclusions
A simple pseudomeningocele can be observed and often resolves spontaneously, however complications including neurological deficits from spinal cord or root compression and CSF leak leading to meningitis may ensue. 7 Management options then include lumbar drain placement, bed rest, reinforced suturing of the surgical site if there is a leak, and surgical revision, if required. Additional methods have also been previously reported, which include open surgery with fascia lata packing combined with tension suturing, 8 and even cervical-peritoneal shunt placement for recurrent postoperative cervical pseudomeningocele. 9
While the use of aspiration and blood patch has been previously described in cases of post-operative lumbar pseudomeningoceles,2–6 its effectiveness in cases of the posterior cervical spine have not been documented. One case report detailed the use of an epidural blood patch for a traumatic anterior cervical pseudomeningocele, 10 however to the best of our knowledge there have been no reported studies investigating its utility in managing posterior pseudomeningoceles. The relative scarcity of literature on the technique may be attributed to the lower overall prevalence of cervical versus lumbar pseudomeningoceles, which is thought to be due to the comparatively higher number of performed lumbar laminectomies. 11 Furthermore, CSF dynamics are thought to play a role since there is lower CSF pressure in the more cranial, less dependent cervical spine as compared to the lumbar spine. 11
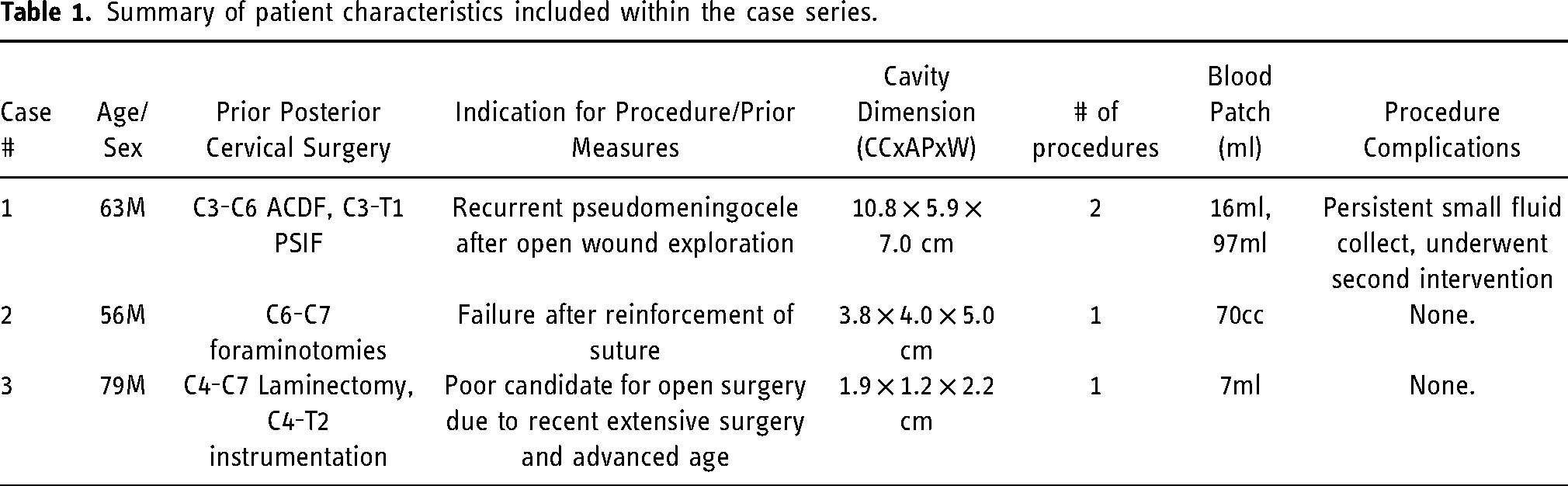
From our limited experience, post-operative durotomy related pseudomeningoceles can be managed effectively and safely with percutaneous aspiration and epidural blood patch. In two of the presented cases, the CSF drainage was persistent despite surgical revision or placement of reinforced sutures; however, epidural blood patch proved to effectively ameliorate these otherwise unmanageable CSF leaks. Though, one patient did have to undergo a second procedure due to a residual small CSF collection, there were no additional complications that occurred in the presented series (Table 1). Although none of our patients experienced procedural related complications, theoretical complications may include over injection and cervical cord compression, and meningeal irritation from subarachnoid blood.
Summary of patient characteristics included within the case series.
Intuitively, with large dural tears it would be expected that any injected blood would enter directly into thecal sac and result in a chemical meningitis. However, in our limited experience with cervical blood patches, using a slow injection technique coupled with the natural outward pressure gradient through the tear prevents blood from entering the thecal sac; in fact, none of the three presented patients exhibited clinical symptoms of meningeal irritation following the procedure. We also emphasize that these blood patches likely need to be larger volume than typical post lumbar puncture blood patches since the epidural space is essentially obliterated post-surgically. Additionally, there may be concern for inhibited wound healing given that the inserted blood may prevent tissue from approximating together. However, based clinically and on the presented follow up imaging, this was not an issue in our experience. This might be explained by similar physiologic resorption rates of the blood patch and with rates of tissue healing and durotomy closure. Nonetheless, these are potential complications that should be considered when attempting this procedure.
In the third patient case, intervention was performed despite the patient being neurologically intact and without postural headache. Increased output within the posterior cervical drain and the patient being a poor repeat surgical candidate convinced us to intervene pre-emptively and the patient was subsequently able to have the drain removed. Given this case, it seems there may be a role of possible prophylactic intervention in patients without postural headache or other overt symptoms. This might serve as an avenue of future investigations.
In conclusion, cervical spine pseudomeningoceles of post-surgical or traumatic etiology can be difficult complications to manage and may persist even after re-operative open surgical repair. Our experience suggests that percutaneous blood patch can be used as an additional option in managing these challenging entities both safely and effectively.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
IRB approval
IRB approval and patient consent was not required by our institution due to the small size and retrospective nature of the presented case series.