
Abstract
Introduction
Stroke is a vascular disorder that affects the brain’s blood vessels, including intracerebral hemorrhage and cerebral infarction, and is a leading cause of disability and mortality worldwide (Sacco et al., 2013). Stroke can result in partial paralysis or complex dysfunctions, such as impairments in speech, comprehension, or memory, depending on the location and severity of the injury, etc. It can also lead to chronic or long-term disability (World Stroke Organization, 2019). People with disabilities often experience limitations in daily activities and restrictions in participation (Singam et al., 2015).
A rehabilitation approach that facilitates meaningful participation for individuals with chronic disabilities is essential (Cardol et al., 2002). Rehabilitation enhances daily living skills, fosters individual autonomy, supports the establishment of social roles, and aids in adaptation to new lifestyles (Young & Forster, 2007). Such rehabilitation has positive effects on physical, cognitive, and social aspects of functioning and well-being (Hopman & Verner, 2003). However, many individuals experience persistent participation restrictions following a stroke, and their daily activities are often confined to their home environments (Ada et al., 2003).
Assistive technology (AT) encompasses both systems and services that apply knowledge and technology to devices, equipment, instruments, or software to support users in engaging in purposeful and productive activities and leading an independent life (World Health Organization, 2016). Assistive Technology Devices (ATDs) are defined as products that enhance users’ abilities and enable them to perform actions, tasks, and activities independently (LaPlante et al., 1992). However, if users’ functional needs and their willingness to actively participate are not considered, ATDs may negatively impact their capabilities, social engagement, and overall participation (Scherer & Glueckauf, 2005). Additionally, users may abandon ATDs, leading to issues regarding the appropriateness of ATD prescriptions and resource waste (Wessels et al., 2003).
Multifaceted factors including personal, environmental, contextual, psychosocial, and social elements play a role in the effective adoption and application of AT, as described in various AT frameworks. Among these, the Human Activity Assistive Technology (HAAT) model emphasizes the importance of active engagement in a given environment and highlights the need to consider personal factors, including physical, cognitive, and emotional aspects, for the optimal use of AT (Cook & Hussey, 2002). Additionally, the Matching Person and Technology (MPT) model focuses on identifying and addressing personal attributes such as ability, experience, and attitude toward AT use, emphasizing that the user’s perspective is central to AT selection (Scherer, 2002, 2005). Beyond understanding AT frameworks, it is crucial to investigate the factors influencing AT usage and the number of ATDs utilized by actual users.
It has been reported that the factors influencing the number of ATDs used are associated with personal aspects such as physical safety, emotional security, and the maintenance and promotion of independence in goal-oriented activities (Gitlin, 1995). Previous studies have shown that individuals with greater difficulties in activity and participation, such as executing tasks, performing actions, and engaging in life situations, tend to use more ATDs (Agree & Freedman, 2000). This relationship is influenced by the extent to which individuals have opportunities for autonomy and greater independence, depending on their level of activity and participation (Gjessing et al., 2018). Additionally, cognitive function has been identified as a key factor in the effective use of ATDs (Sheffield et al., 2013) and in the adoption of new and diverse ATDs (Jutai et al., 2007). Consequently, cognitive function is recognized as a significant variable that facilitates ATD use (Wessels et al., 2003). Furthermore, advanced age (Spillman, 2004) and higher levels of anxiety have been found to increase ATD use (Wielandt et al., 2006). Studies examining the relationship between activity, participation, and ATD usage have reported a strong correlation between the number of ATDs used and an individual’s occupational roles, cognitive function, and psychological factors (Byun et al., 2015). Moreover, as individuals age, they frequently encounter increased difficulties and greater dependency in performing daily activities, reinforcing the importance of age as a relevant determinant (Kylberg et al., 2013).
While participation is often described as an outcome in stroke rehabilitation, it has also been reported to mediate the relationship between intrinsic factors such as cognition and anxiety and extrinsic factors such as ATDs and environmental support (Botticello et al., 2014; Hammel et al., 2015). ATDs can enhance participation by promoting functional independence, while individuals with higher participation levels may actively seek ATDs to support their engagement in meaningful activities (Federici et al., 2016; Lenker & Paquet, 2003). Given this bidirectional relationship, further research is needed to explore the mediating role of participation in the broader framework of aging, cognition, and psychological factors.
Häggblom-Kronlöf and Sonn (2007) emphasized the importance of understanding users’ functional factors to meet the needs of potential ATD users in daily life. While previous studies have explored the relationships between age, cognition, and participation in ATD use, none have examined their pathways and influences on the number of ATDs used by community-dwelling individuals with mild cognitive impairments after a stroke.
In a study by Häggblom-Kronlöf and Sonn (2007), it was reported that a comprehensive understanding of users’ functional factors is essential to meet the needs of potential ATD users in daily life. Although previous studies have examined the relationships between age, cognition, and participation in ATD use, no studies have analyzed the pathways and influences among these factors in determining the number of ATDs used by community-dwelling people with mild cognitive impairments following a stroke. In this study, age, anxiety, and cognition were designated as exogenous variables influencing other factors, while participation was set as a mediating variable, and the number of ATDs used was defined as the final endogenous variable. The purpose of this study is to develop a path analysis model examining the relationships among demographic characteristics, cognition, anxiety, and participation in explaining the number of ATDs used by community-dwelling individuals recovering from stroke with mild cognitive impairments.
Methods
Research participants and selection criteria
This study was approved by the Institutional Review Board of Konyang University (Ref. no: KYU-2018–022-02). Participants were community-dwelling people recovering from stroke. They were informed of the study’s purpose, procedures, content, and measures to protect private information before providing informed consent. The inclusion criteria were diagnosis of stroke by a neurologist; living at home; adults with stroke (over 19 years); those with normal or mild cognitive impairment (Korean Mini-mental State Examination (Kang et al., 1997, K-MMSE) scores above 18) (Jutai et al., 2007); and understand the purpose of the research and agree to participate. Exclusion criteria were individuals with communication difficulties and non-ATD users. Exclusion criteria were those with communication difficulties. A total of 233 participants answered the survey, but 37 were excluded due to no history of stroke (n = 25), incomplete answers, or did not-use of ATDs (n = 12). Thus, the final analysis included 196 participants. According to the Maximum Likelihood Estimation (MLE) method in Structural Equation Modeling (SEM), a sample size of at least 100 to 150 is required, with 200 considered more appropriate (Hair et al., 2006). Therefore, the sample size in this study was deemed appropriate.
Research procedures
This study was conducted between September 2018 and January 2019. Using a convenience sampling method, participants were recruited from public health centers, welfare centers, and home-visiting rehabilitation service centers. Data collection was carried out by occupational therapists at each institution, and the researcher provided training on data collection procedures and evaluation items to minimize inter-rater errors. Data were collected either in a designated space within the institutions or in participants’ home environments. Demographic characteristics and the number of ATDs used were reported by participants and their family members through a semi-structured questionnaire, while data on cognition, participation, and anxiety were collected by the evaluators.
Measurements
Number of Assistive Technology Devices used
The number of ATDs used in various activities, such as activities of daily living, electronic information access, and mobility, was surveyed. The number of ATDs used was assessed based on the National Assistive Technology Center’s (NATC) classification system. Usage was categorized into 12 areas: personal medical treatment, skills training, orthoses and prostheses, and recreation (NATC, 2019), along with 111 subcategories. A checklist reflecting this classification system was used to investigate the number of ATD items used by participants.
Korean version of Montreal Cognitive assessment (K-MoCA)
We used the Montreal Cognitive Assessment (MoCA) tool, which was developed by Nasreddine et al. (2005) and translated by Lee et al. (2008). This tool is divided into spatiotemporal/executive, vocabulary, attention, sentence structure, abstraction, recall, and orientation sections. The maximum score is 30. Normal cognitive function is defined as a score above 23, and a score below 22 is classified as mild cognitive impairment (Lee et al., 2008). The reliability of the instrument in this study was 0.84.
Beck Anxiety Inventory (BAI)
We used the 21-item Beck Anxiety Inventory (BAI) tool developed by Beck et al. (1988) and translated by Yook and Kim (1996). This tool measures anxiety across the cognitive, emotional, and physical domains. The scoring is based on a Likert scale from 1 to 4, with higher scores indicating greater anxiety. In previous studies, the internal consistency reliability was reported to have a Cronbach’s α of 0.91 (Yook & Kim, 1996), and in this study, the reliability was 0.95.
Utrecht Scale for Evaluation of Rehabilitation-participation (USER-participation)
We used a measurement tool developed by Post et al. (2012) and translated by Lee et al. (2017). This tool consists of three sections: measuring frequency of participation in various activities, restriction of activity due to disease or health status, and satisfaction with activities. The scoring system for each section is different. Frequency is scored from 0 to 5, restriction is scored from 0 to 3, and satisfaction is scored from 0 to 4. The sum of each section’s score is converted to a 100-point scale, with higher scores indicating higher participation rates. In previous studies, the reliability for frequency was reported with a Cronbach’s α of 0.60–0.75, α = 0.85–0.91 for restriction, and α = 0.78–0.88 for satisfaction (Lee et al., 2017). In this study, the reliability of the measurement tool was α = 0.81 for frequency, α = 0.88 for restriction, and α = 0.84 for satisfaction.
Statistical analysis
Demographic characteristics were analyzed using frequency distributions, and normality was assessed through skewness and kurtosis. Pearson’s correlation analysis was conducted to evaluate reliability. Analyses were performed using the statistical software packages SPSS 22.0 and AMOS 24.0 (IBM Corp, Armonk, NY, US).
Path analysis
SEM was used to test the hypothesized associative relationships among latent and observed variables (Kline, 2010). Path analysis used a parallel mediation model to analyze the independent effects of multiple mediators on ATD usage, assessing their direct and indirect influences. In the path model, all variables are measured simultaneously, making directionality of relationships unclear. Correlations analysis was used tointerpret these relationships, and non-correlated variables can be linked based on previous studies (Moon, 2009).
Path analysis was performed to verify the hypothetical model of the number of ATDs used and to analyze the relationship. Maximum Likelihood Estimation (MLE) was used for parameter estimation of the model representing the associations in the path analysis. In order to evaluate the goodness of fit of the model, the chi-square, Goodness of Fit Index (GFI), Tucker-Lewis Index (TLI), Normed Fit Index (NFI), Comparative Fit index (CFI), Root Mean-squared Residual (RMSEA) and Standard RMR (SRMR) was checked.
Results
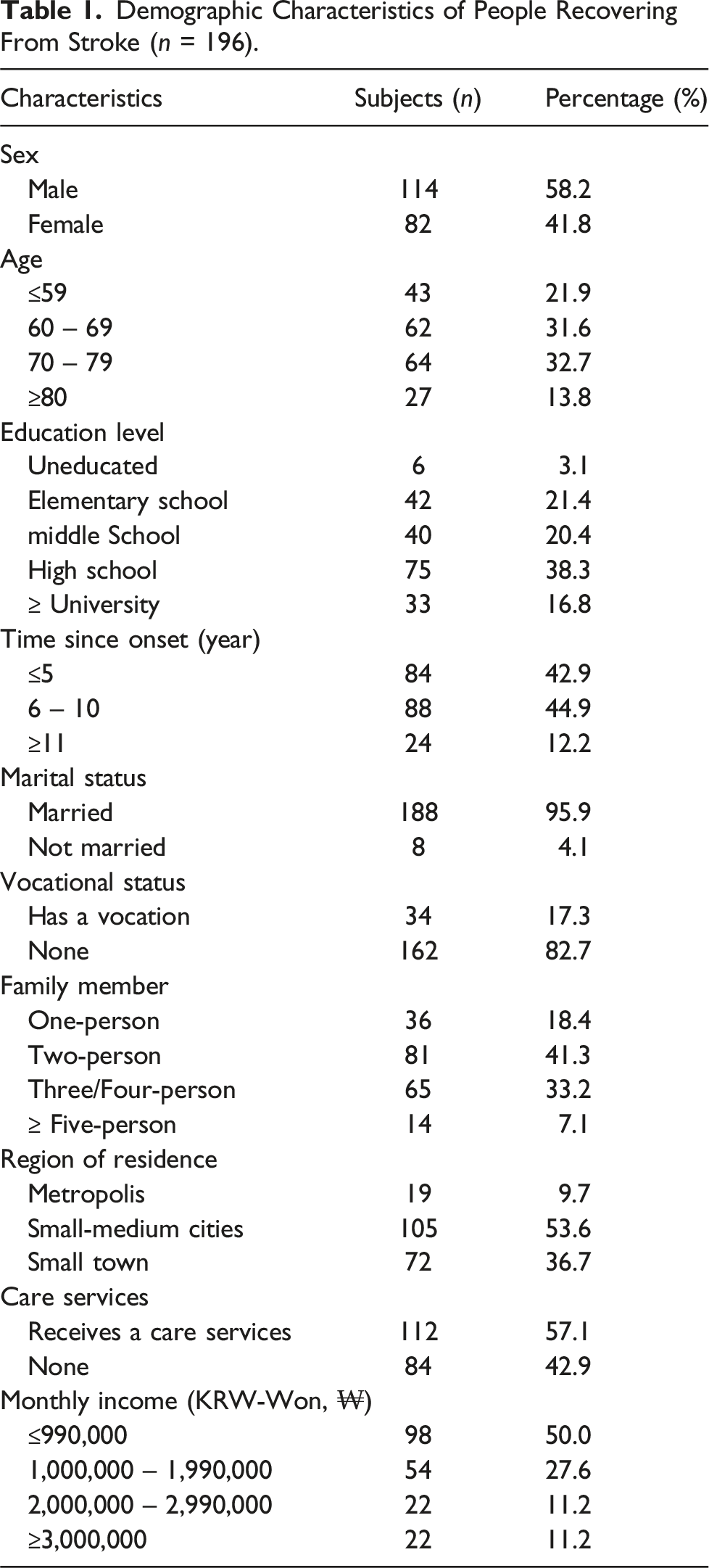
Demographic characteristics
Demographic Characteristics of People Recovering From Stroke (n = 196).
The descriptive statistics for variables
Descriptive Statistics for Variables (n = 196).

Number of ATDs used by people recovering from stroke
Number of ATDs Used of People Recovering From Stroke (n = 196).
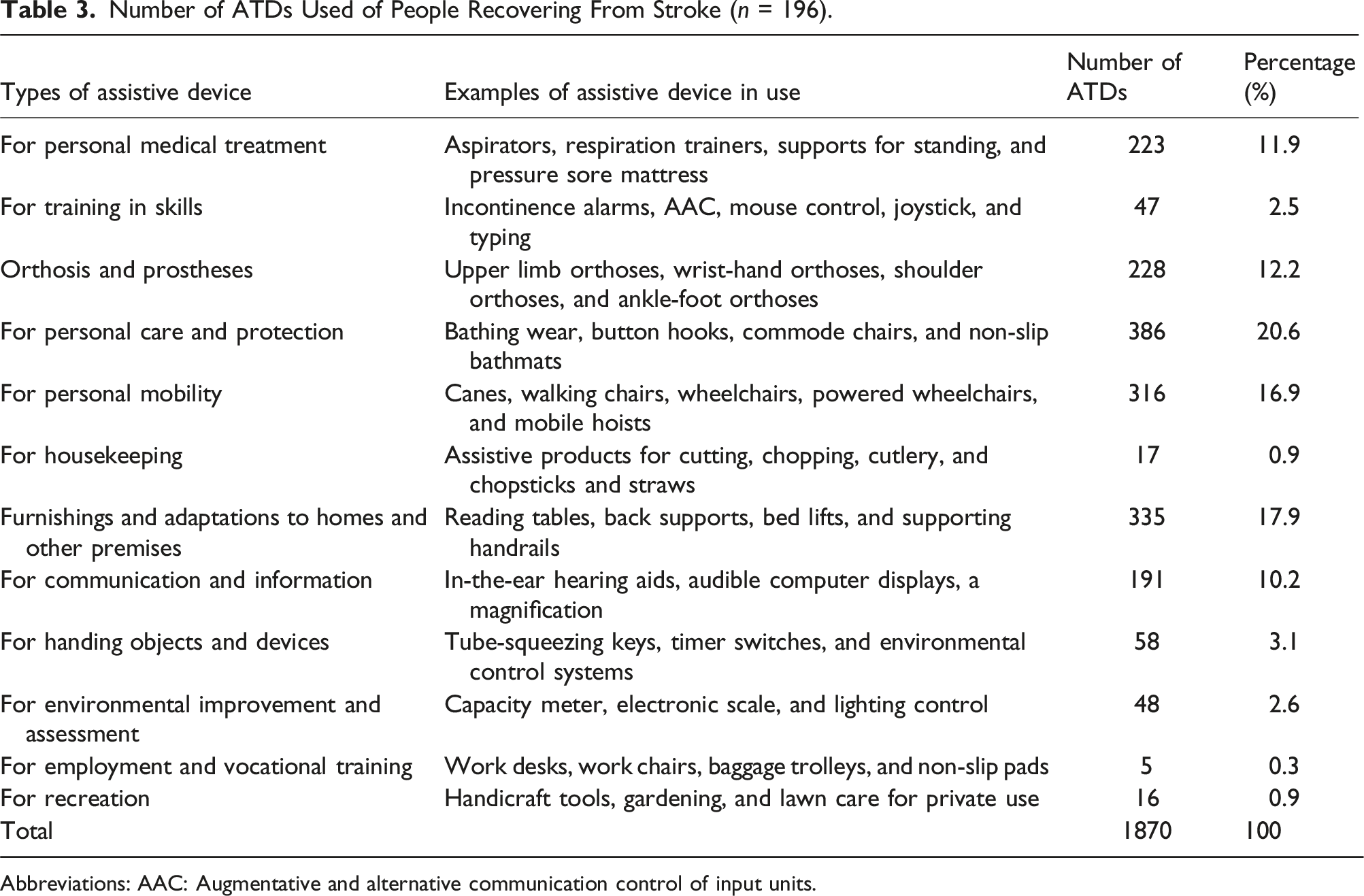
Abbreviations: AAC: Augmentative and alternative communication control of input units.
Correlation analysis of variables
Correlation of Variables Related to Number of ATDs Used (n = 196).
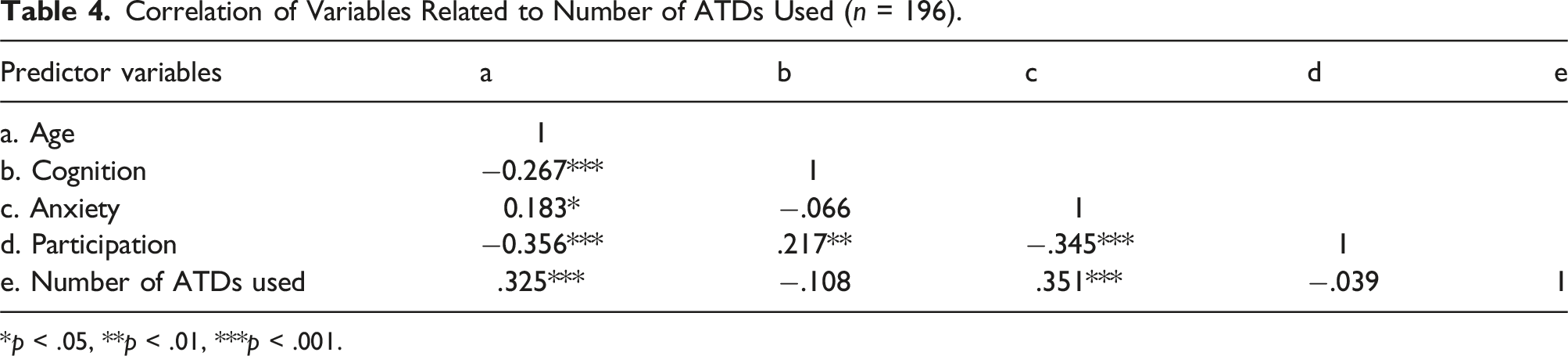
*p < .05, **p < .01, ***p < .001.
Measurement of hypothetical path model
Chi-square statistic and goodness-of-fit index were used to verify the model fit. The larger the chi-square, the greater the difference between the covariance matrices, which means that the model does not fit the data. The p-value of the chi-square statistic is inversely related to the chi-square, and if the p-value is larger than 0.05, the null hypothesis of the proposed model will not be rejected (Figure 1). Hypothetical path model diagram.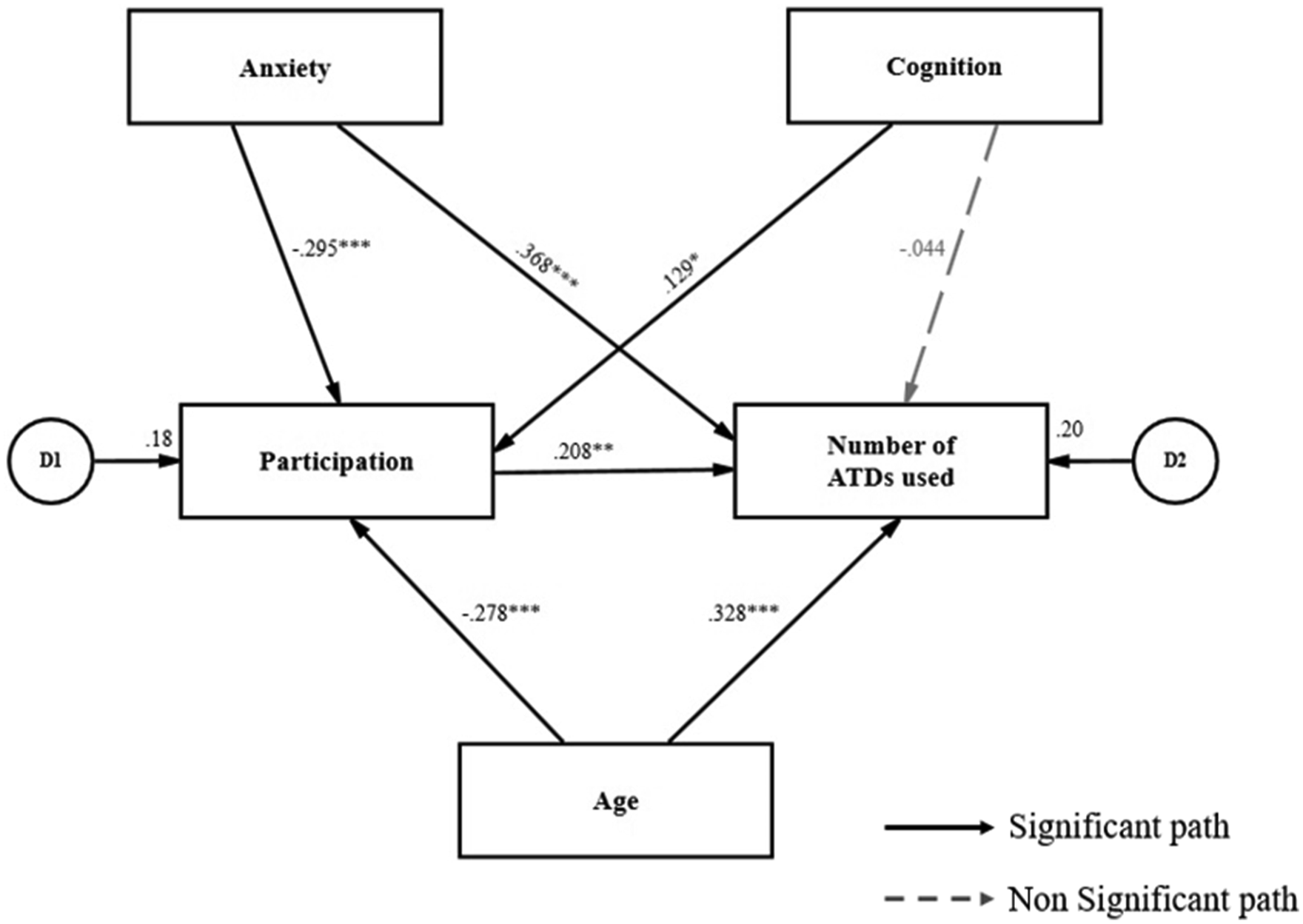
Test of Model Fit.

Measurement of modified path model
To improve model fit, modification indices (M.I.) were examined, identifying potential adjustments that could enhance statistical suitability. The results suggested that adding covariance paths between age and cognition (M.I. = 13.851, Par Change = −7.418) and age and anxiety (M.I. = 6.510, Par Change = 26.243) would significantly reduce model misfit. These adjustments were incorporated to enhance model fit and better capture the underlying relationships between variables (Kline, 2010).
After incorporating these adjustments, the theoretical validity of the revised model was reviewed. Prior research confirmed relationships were age to anxiety (Zamzam et al., 2020) and age to cognition (Lee & Kahng, 2011). In the modified path model, Age, Anxiety, and Cognition were designated as exogenous variables. Participation was set as a mediating variable that links the effects of Age and Anxiety to the endogenous variable, the Number of ATDs used. Cognition was modeled as an exogenous variable with a direct path to the Number of ATDs used.
The result of the fitness of the modified model diagram showed a chi-square of 3.724 and had a p-value of .155, exceeding .05. Other indices were TLI (.922), NFI (.969), CFI (.984), and GFI (.922) which all exceed .90, meeting the model fit. The RMSEA (≤.08 good model) was .066 and SRMR (<.05 good model) was .032, and the goodness-of-fit index for the modified model was generally good (Table 5).
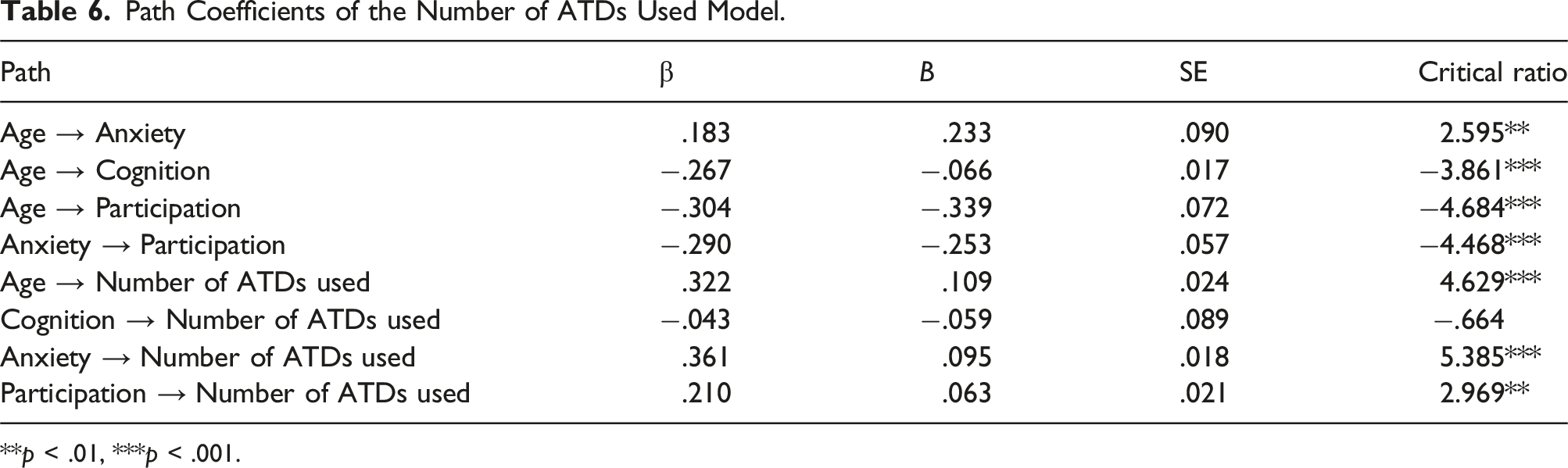
Standardized coefficients (β), which represents the degree of influence of independent variables on dependent variables in the modified path model, are presented in Figure 2 and Table 6. Factors directly affecting the number of ATDs used were participation (β = .210, p < .01), anxiety (β = .361, p < .001), and age (β = .322, p < .001). Factors directly affecting participation were age (β = −.304, p < .001), anxiety (β = −.290, p < .001). Age was found to be a factor that directly affects anxiety (β = .183, p < .01) and cognition (β = −.267, p < .001) (Figure 2). Modified path model diagram. Path Coefficients of the Number of ATDs Used Model. **p < .01, ***p < .001.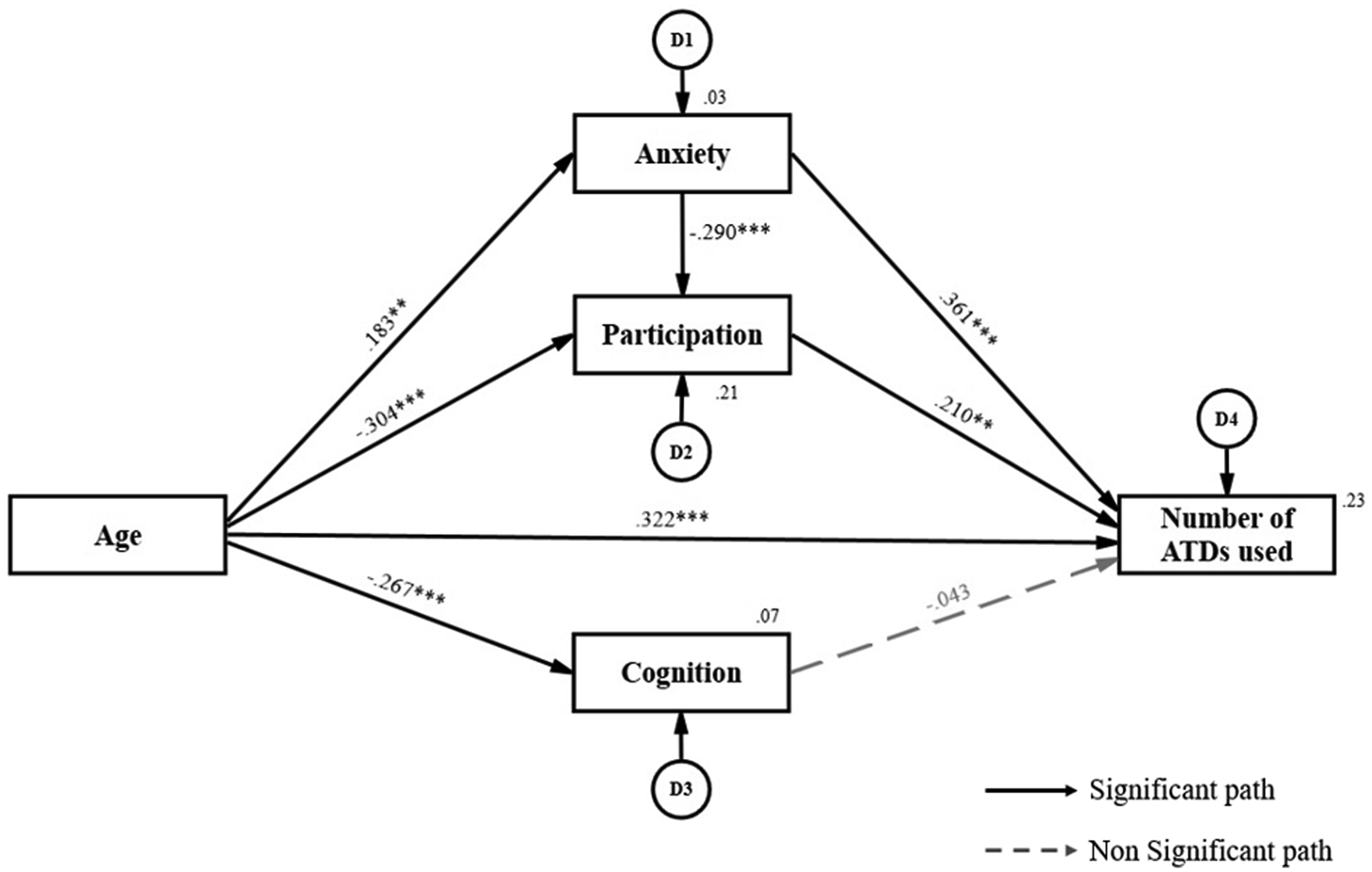
Direct, indirect, and total effects of factors
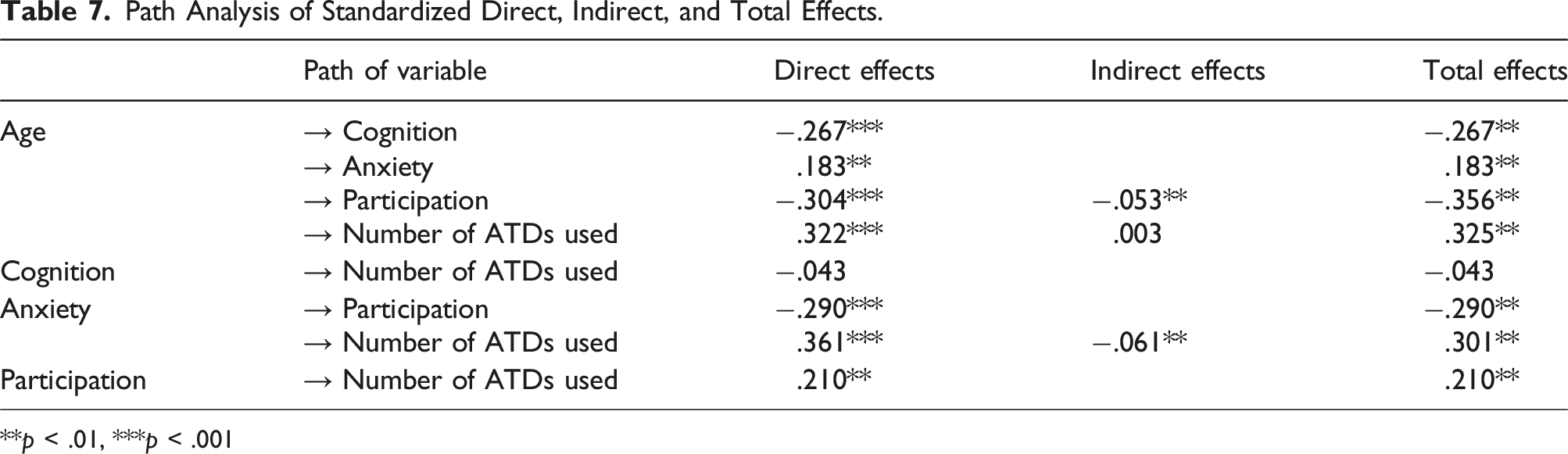
Path Analysis of Standardized Direct, Indirect, and Total Effects.
**p < .01, ***p < .001
Discussion
The level of participation of people recovering from a stroke varies from person to person (Van Der Zee et al., 2013). Path analysis showed that participation positively influences ATDs use, indicating that higher participation levels lead to greater ATD adoption. This aligns with previous research suggesting ATDs compensate for functional limitations and promote independence (Agree & Freedman, 2000; Gjessing et al., 2018).
Anxiety negatively affected participation, reducing engagement in daily activities, but directly increased ATD use, indicating greater reliance on assistive technology. This aligns with previous research indicating that ATDs compensate for functional limitations and promote independence (Agree & Freedman, 2000; Gjessing et al., 2018). These findings highlight participation as a direct determinant of ATD use, while also being influenced by anxiety. Anxiety directly increased ATD usage, while also influencing participation, which was associated with ATD adoption. Participation’s impact on ATD usage may vary depending on individual psychological and social contexts (Federici et al., 2016). While participation is associated with greater ATD use, its relationship with anxiety and ATD reliance requires further investigation. These findings suggest that participation plays a significant role in shaping ATD utilization patterns while being influenced by broader psychological and functional factors. Future research should explore how participation, in conjunction with psychological and social influences, contributes to assistive technology use in stroke rehabilitation.
Anxiety had a direct positive effect on both participation and the number of ATDs used, but its influence on ATD usage was moderated by participation. While individuals with higher anxiety levels tended to use more ATDs, those with higher participation levels were less dependent on ATDs despite experiencing high anxiety. These results align with a previous study that found anxiety to be a factor influencing ATD usage (Wielandt et al., 2006). People recovering from stroke have difficulty in performing daily activities and forming social relationships due to anxiety (Astrom, 1996). Such enhanced anxieties are known to limit patients’ perception and learning (Knowles, 1981). Wielandt et al. (2006) reported that ATD usage increased when anxiety levels decreased, which contrasts with the findings of the present study, where higher anxiety levels were associated with greater ATD usage. However, our results suggest that participation plays a compensatory role, enabling individuals to rely less on ATDs even when experiencing high anxiety levels. A study by Song (2003) found that psychological and social anxiety decreased as individuals improved their ability to carry out daily activities. Therefore, to alleviate psychological anxiety among stroke survivors, it is necessary to promote participation, provide appropriate ATDs, and enhance their utilization.
Age had a direct effect on the number of ATDs used and an indirect effect through participation. The findings indicate that older individuals used a greater number of ATDs. Additionally, age indirectly influenced ATD usage through participation, suggesting that older individuals who engage in higher levels of participation may experience greater benefits from ATDs. This result aligns with a previous study showing that age influences ATD usage (Edwards & Jones, 1998). As individuals age, they experience both physical and psychological decline (Ritsatakis, 2008), and the speed of recovery from symptoms is slower than that of younger people with disabilities (Marini et al., 2004). ATDs play an even more critical role for older stroke survivors by compensating for health decline and functional limitations, ultimately promoting independence (Nasr et al., 2016).
On the other hand, cognition was not found to be a significant factor in the direct path affecting the number of ATDs used. In this study, to enhance the accuracy of interviews and self-reported questionnaires, only participants with a K-MMSE score of 18 or higher were included in the analysis. This suggests that within the range of normal to mild cognitive, cognitive function may not be a key determinant in explaining the number of ATDs used. Previous studies have reported that cognitive ability influences ATDs usage by affecting users’ capacity to operate the devices and recall training methods for their use (Wielandt et al., 2006). Additionally, clinical characteristics of individuals recovering from a stroke indicate that while cognitive function plays a role in the effective utilization of ATDs, its impact is more pronounced when mobility impairments are present, even if physical function is compromised (Jutai et al., 2007). These findings suggest that once cognitive function reaches a certain range, its effect on the number of ATDs used may be limited. Therefore, future research should include individuals with varying degrees of cognitive impairment to provide a more comprehensive analysis of the relationship between cognitive function and ATD usage.
Limitations and future research
A limitation of this study is the lack of measurement of exogenous variables that may influence the number of ATDs used, such as demographic and socioeconomic factors, stroke-related functional impairment, and residential environment conditions. Since ATD usage is shaped by multidimensional factors beyond individual psychological and behavioral aspects, future research should incorporate these variables for a more comprehensive analysis. Additionally, while the hypothetical path model in this study was supported by previous research, unmeasured confounding variables may still exist, potentially affecting the pathways identified. Refining the model by integrating additional variables and conducting longitudinal analyses would enhance its predictive validity. Moreover, as this study employed a cross-sectional design, it cannot establish a directional relationship between ATD usage and participation. While participation was hypothesized as a mediator, the relationship may be bidirectional, with ATD usage enhancing participation and higher participation levels driving ATD use. This dynamic may also vary across rehabilitation stages and personal contexts, requiring future longitudinal studies to determine its potential directional relationship. Furthermore, to minimize measurement bias in self-reported data, only participants with mild cognitive impairment were included, which limits the generalizability of the findings to individuals with more severe impairment. Future studies should consider a broader range of cognitive abilities to better understand the role of cognition in ATD usage. Furthermore, various mediation models, such as parallel or moderated mediation, should be explored to refine the understanding of the pathways influencing ATD usage identified in this study and provide a more comprehensive analysis.
Conclusion
The overall fitness of the path model for the number of ATDs used appears to be robust. Anxiety, Age, and participation were found to have both direct and indirect effects on the number of ATDs used, while Cognition did not show a statistically significant effect. These findings confirm the associations among key factors influencing ATD usage among community-dwelling individuals recovering from stroke with normal to mild cognitive impairment. Rather than focusing on the provision of multiple ATDs, prescribing should prioritize individualized user needs, psychological factors, and participation levels. Clinicians should assess both psychological and functional aspects, such as anxiety and participation, to ensure appropriate device selection and effective utilization. Given the aging population and rising disability rates, a strategic approach is needed to optimize ATD allocation and improve accessibility. Future research should explore the personalized prescription frameworks and strategies to enhance long-term ATD adoption.
Key findings
For community-dwelling individuals recovering from stroke with normal to mild cognitive impairment, the number of ATDs used was influenced by age, anxiety, and participation.
Prescribing ATDs for people recovering from stroke should consider multiple factors, including participation level, psychological response, and choices of activities in community living.
The prescription of individual ATDs should be based on a thorough review of the user’s actual needs, functional abilities, and environmental context to ensure appropriate and effective utilization.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by a grant from the National Research Foundation of Korea (NRF), funded by the government of Korea (MSIP; Ministry of Science, ICT, & Future Planning) (NRF-2017R1C1B5017510).