
Abstract
Background
Metacognitive abilities in daily functioning and their relationship to older adults’ participation have not been sufficiently explored. Prior research has mainly focused on cognitive performance without fully addressing its functional implications.
Objective
This descriptive quantitative study aimed to describe older adults’ self-reported everyday difficulties related to their metacognitive abilities, their participation patterns, and the correlation relationships between them.
Methodology
A total of 186 community-dwelling Israeli older adults (125 women; mean age 73.44yr ± 8.25) completed a demographic questionnaire, the Daily Living Questionnaire (DLQ), and the Adult Subjective Assessment of Participation (ASAP).
Results
Participants reported more difficulties in complex participation activities (e.g., paying bills, navigating unfamiliar environments) than in structured routine tasks. They also reported more difficulties in executive functions (EF) than in memory and executive monitoring. Cognitive difficulties were correlated with lower participation frequency (r = −.34, p < .001), reduced activity diversity (r = −.34, p < .001), and increased need for assistance (r = −.41, p < .001).
Conclusions
Findings highlight the need to assess metacognition functionally, as cognitive challenges significantly affect participation. Integrating subjective cognitive and participation assessments may lead to better prevention and intervention strategies among the older population.
Introduction
Life expectancy worldwide has risen in recent years. People aged 85 years or older are estimated to exceed 12% of the entire population by 2050 (Piscitelli et al., 2020). The aging process and the associated epidemiology of advanced age point to increased vulnerability during this life stage. The increased rates of illness and disability coincide with a combination of financial and social difficulties (Bitzur & Shaked, 2019). The aging process is usually accompanied by an increasing prevalence of illness and disability, decreasing physical and mental abilities, and a lack of personal and social resources (Bitzur & Shaked, 2019; Marik, 2010). As part of the natural aging process, decreased cognitive and metacognitive functions also occur (Phillips et al., 2002; Zelazo et al., 2004).
Metacognition is defined as an individual’s knowledge concerning their own thinking and performance processes. It includes two main components: self-awareness and executive functions (EFs; Alvarez-Bueno et al., 2017), including planning, initiation, inhibition, self-monitoring, problem-solving, and working memory. The EFs are used mainly in unconventional activities and allow people to cope with unfamiliar situations and adapt their behavior to changing circumstances (Ardila, 2018; Gilbert & Burgess, 2008; Zoltan, 2007). In addition, EFs are crucial for independence in daily functions and participation in social, occupational, and professional daily life (Katz et al., 2011; Lezak et al., 2004). Specifically, cognitive deficits correlate to difficulties performing daily tasks in older adults (Rosenblum & Elimelech, 2021).
Previous studies have indicated that EFs have the maximum capacity to predict decreased functional abilities and participation (Bell-McGinty et al., 2002; Cahn-Weiner et al., 2002). The World Health Organization ([WHO], 2001) defined participation as involvement in a life situation. Participation in the everyday occupations of life is a vital part of human development and the lived experience through which people acquire skills and competencies, connect with others and their communities, and find purpose and meaning in life (Baum, 2011). Studies have identified participation in various environments as a significant factor explaining high levels of life satisfaction and health and wellness among older adults (Harper, 2000; Njegovan et al., 2001).
Many studies indicated deterioration in daily task performance, participation, and leisure relative to EFs in older adults. Most used standardized, objective, and performance-based measures for EFs (Bertrand & Willis, 1999; Goverover et al., 2009; Marson & Hebert, 2006); only a few examined self-reports of everyday difficulties in activities tied with cognitive deficiency (Rosenblum et al., 2017). Although each method has distinct advantages and disadvantages (such as subjective bias), the literature presents self-report measures as a reasonably accurate representation of real-world performance (Papaliagkas et al., 2017; Schmitter-Edgecombe et al., 2011).
Existing self-report functional questionnaires usually focus on everyday function or cognitive symptoms but do not integrate both dimensions (Rosenblum et al., 2017). The Daily Living Questionnaire (DLQ; Toglia, 2004) was designed based on a broad conceptualization of function as described by the International Classification of Functioning, Disability, and Health (WHO, 2001). It was developed for clinical purposes to assess everyday difficulties that individuals with executive dysfunctions may experience. It was found to be a valid tool for detecting difficulties in daily activities/participation related to cognitive impairments among adults between 18 and 85 yr of age (Panovka et al., 2023; Rosenblum et al., 2017). However, researchers have not studied its relationships to everyday participation patterns. Therefore, the purposes of this study were to (1) describe older adults’ self-reported everyday difficulties in activities tied with EF abilities and their participation patterns and (2) examine the correlation relationships between those everyday difficulties in activities and participation patterns.
Methods
Participants
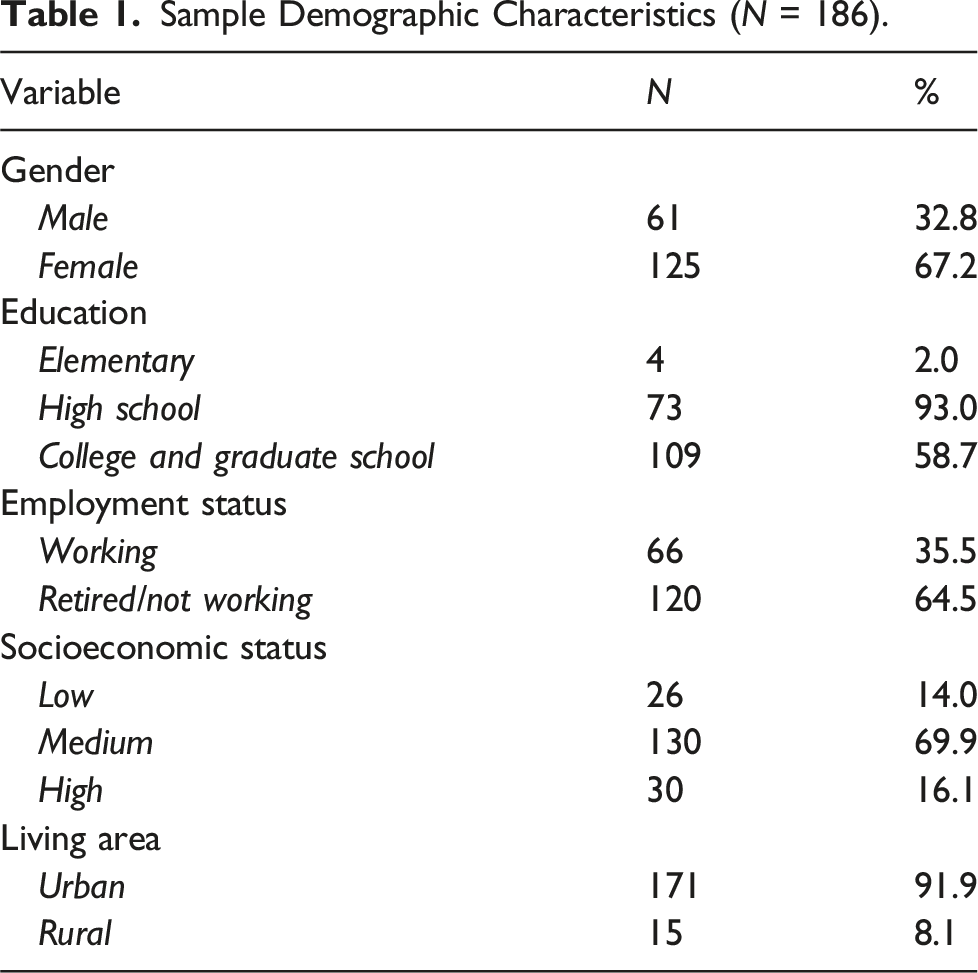
Sample Demographic Characteristics (N = 186).
Instruments
Demographic questionnaire
A short demographic questionnaire was used to collect factual information about participants, including age, gender, education level, socioeconomic status, and living area, to describe the study population.
Daily Living Questionnaire
The Daily Living Questionnaire (DLQ; Toglia, 2004) assesses self-reported everyday difficulties experienced by individuals with higher-order cognitive impairments. It is based on a broad conceptualization of function as described by the International Classification of Functioning, Disability, and Health (ICF; WHO, 2001) and was designed to reflect common challenges reported by individuals with cognitive difficulties. A distinctive feature of the DLQ is that, unlike many other self-report scales, it explicitly asks individuals to rate the degree of cognitive difficulty they experience while performing everyday activities and executive function-related tasks.
The DLQ consists of 52 items, scored on a 4-point scale (from 1—no cognitive difficulty to 4—unable to perform) with higher scores indicating more difficulties reported. It is divided into two main parts, each with specific subcategories. Part A – Activities and Participation, evaluates difficulties in instrumental activities of daily living (IADLs) across four domains: (A1) Household Tasks, include routine domestic activities such as meal preparation and home organization; (A2) Activities Involving Language and Comprehension assess cognitive-linguistic abilities, including reading and following instructions; (A3) Community and Social Participation, examines engagement in social interactions and independent navigation in public spaces; and (A4) Complex Tasks, involve cognitively demanding activities that require executive functions such as problem-solving, planning, and working memory, including managing finances and following multi-step instructions. Part B – Cognitive Symptoms and Impairments, assesses self-reported cognitive difficulties that impact daily functioning across three domains: (B1) Executive Function Components evaluate abilities such as working memory, cognitive flexibility, planning, problem-solving, and organization, which are essential for adapting to complex tasks; (B2) Memory, focuses on difficulties in recalling information, including prospective memory and general forgetfulness in everyday activities; and (B3) Executive Monitoring, examines self-awareness and the ability to assess and regulate one’s cognitive performance, including recognizing errors and adjusting strategies while performing tasks.
The DLQ has demonstrated strong construct validity, expert and face validity, and high internal consistency across different populations, including healthy adults and individuals with neurological conditions (α = .94–.97; Rosenblum et al., 2017).
Adult subjective assessment of participation
The Adult Subjective Assessment of Participation (ASAP; Jarus et al., 2005) is a self-report scale designed to evaluate adults’ participation levels in daily activities. It consists of 52 activities grouped into nine categories: (a) domestic life, (b) recreation and leisure entertainment/recreation, (c) taking care of children and other adults, (d) learning and applying knowledge, (e) recreation and leisure: physical activities and sports, (f) self-care, (g) recreation and leisure: quiet activities, (h) religion and spirituality, and (i) vocation. Respondents rate the participation subscale items from 1 (once or twice in the past 4 months) to 7 (several times a day or done in the past but was given up).
The ASAP includes four subscales: (a) frequency, which consists of a diversity score (the number of activities the respondent currently participates in and the percentage of activities within each category) and an intensity score (the average frequency of participation in each category); (b) level of enjoyment; (c) level of satisfaction with performance; and (d) social context of participation (i.e., with whom the activities are performed). Construct validity was established through factor analysis, confirming the categorization of different occupations. Additionally, ASAP demonstrated discriminant validity by differentiating between individuals with and without disabilities based on their scores for activities categorized as ‘currently participating in' and ‘given up' (Jarus et al., 2005).
Procedure
Following institutional ethical approval from the University of Haifa, potential participants from various regions of Israel were provided with explanations regarding the study’s purpose, rationale, and their expected participation. Informed consent was obtained from all participants before they completed the demographic questionnaire, DLQ, and ASAP. Assistance was provided as needed for reading instructions and completing the questionnaires.
Data analysis
Data analysis was performed using SPSS software version 25.0. Descriptive statistics, including ranges, mean scores, and standard deviations, were calculated. Paired sample t-tests with Cohen’s d effect size calculations were used to assess differences between the DLQ subscores and the ASAP. Pearson correlation analyses were conducted to examine the relationships between the DLQ and ASAP.
Results
Daily Living Questionnaire reports
Participants’ Daily Living Questionnaire (DLQ).
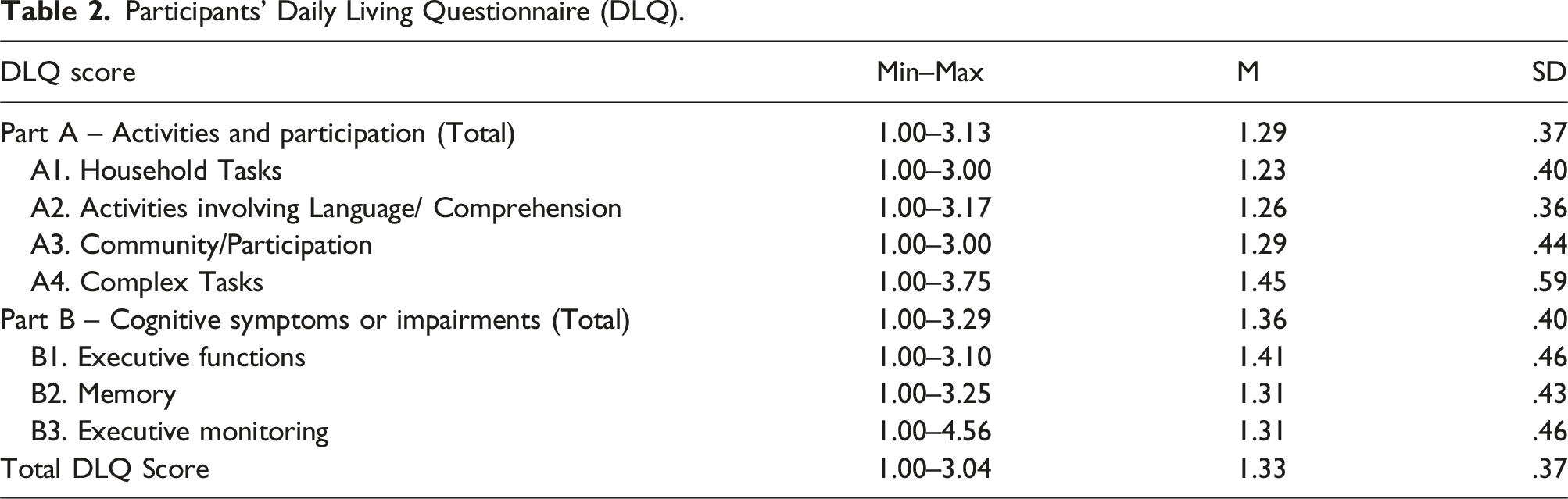
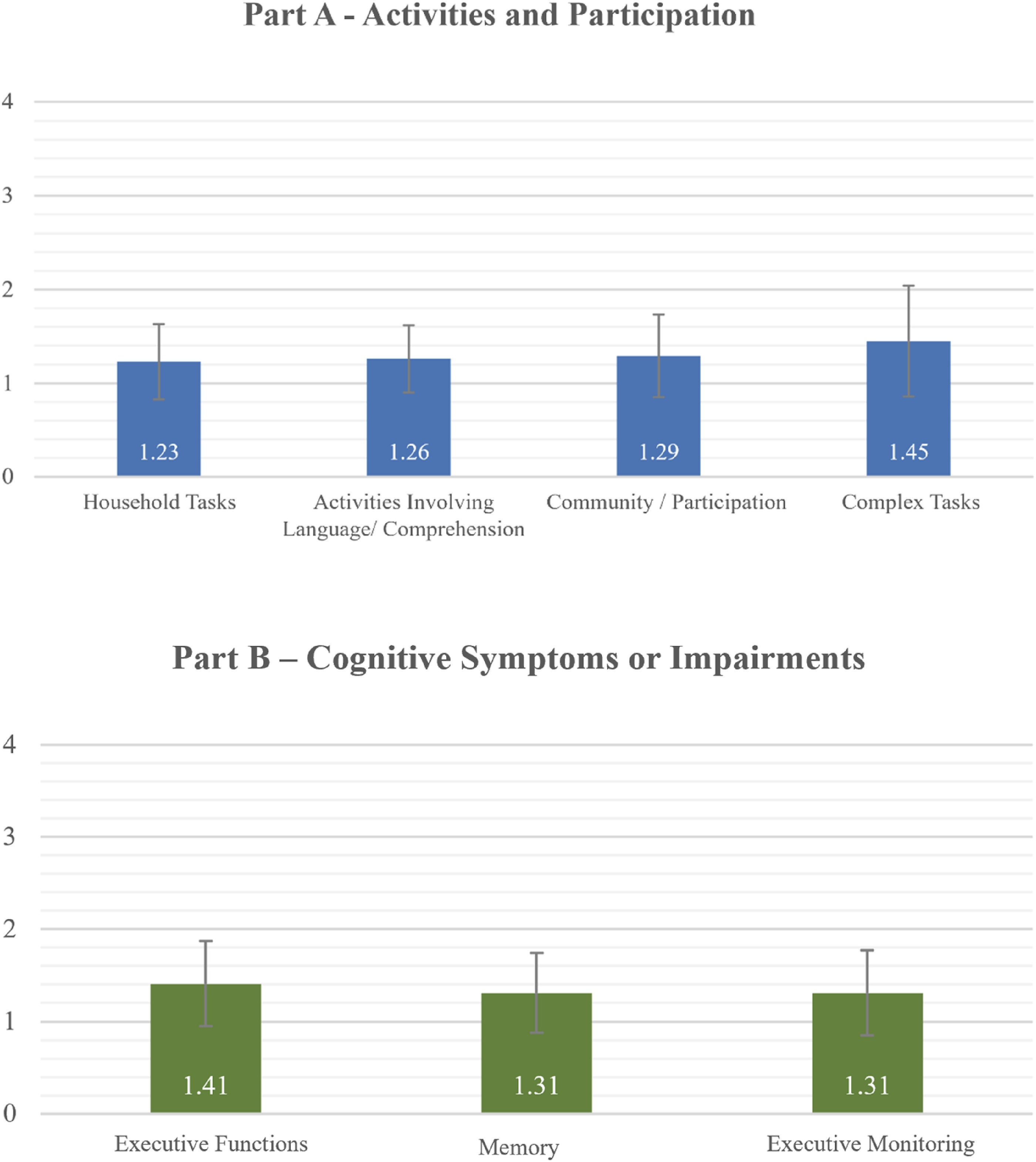
Daily living questionnaire score means and standard deviations.
Participation patterns
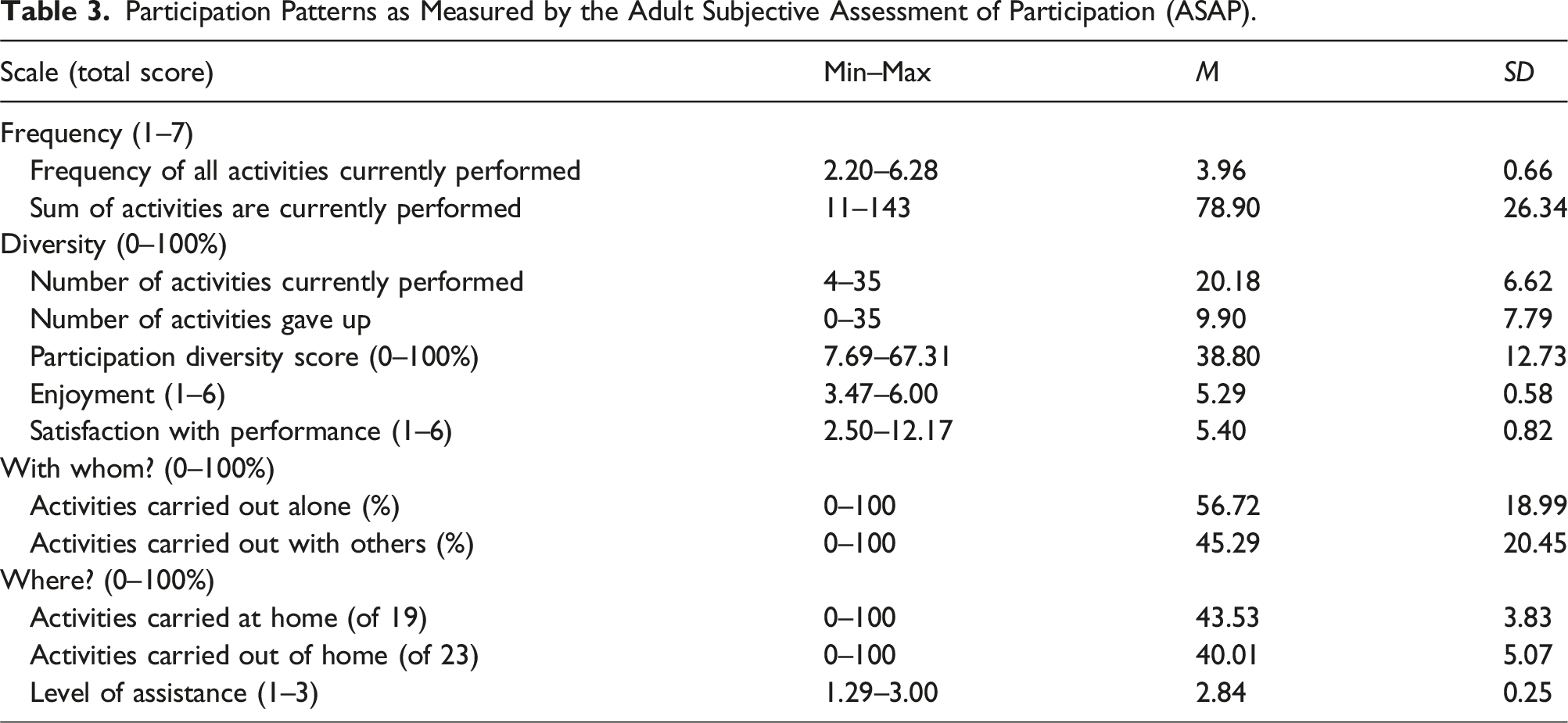
Participation Patterns as Measured by the Adult Subjective Assessment of Participation (ASAP).
Correlation between the DLQ and participation patterns
Correlations Between Self-Report of Cognitive Difficulties while Performing Daily Living Activities (DLQ) and Participation Patterns (ASAP).
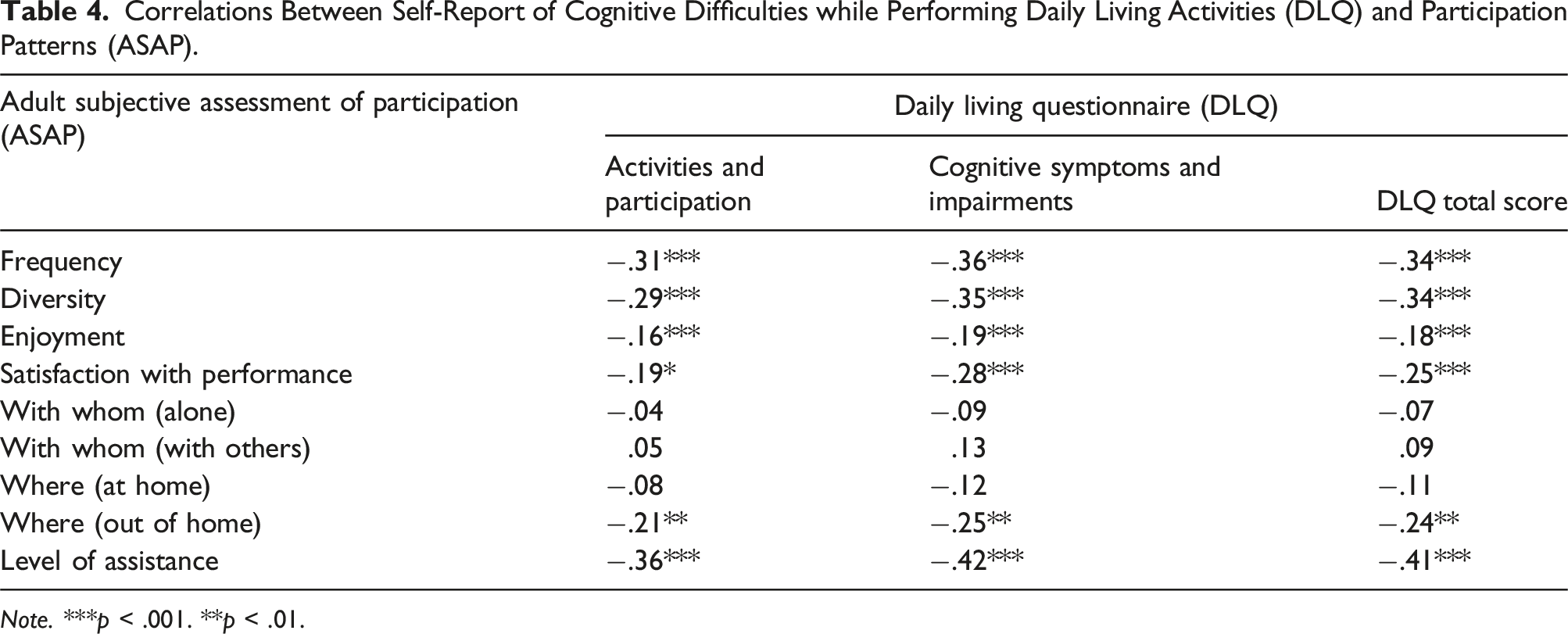
Note. ***p < .001. **p < .01.
Correlations with cognitive difficulties while performing basic and complex activities
The reporting of cognitive difficulty while performing instrumental activities of daily living (IADLs), including basic and Complex Tasks, as presented in Part A – Activities and Participation of the DLQ , was found to be significantly correlated with the frequency (r = −.31, p < .001) and diversity (r = −.29, p < .001) of all activities currently performed, as reported in the ASAP. This correlation indicated that as participants reported more cognitive difficulties in IADLs and complex tasks, they also reported fewer activity types and lower frequencies of participation. In addition, a significant correlation was found with the level of assistance the participants reported needing (r = −.36, p < .001), and significant but weak correlations were found with their level of participating in activities out of the home (r = −.21, p < .01). Thus, greater self-reported cognitive difficulties were associated with an increased need for assistance and reduced participation in community activities.
Functions related to cognitive impairments
Reported functions related to cognitive impairments, as presented in Part B – Cognitive Symptoms and Impairments of the DLQ, were found to be significantly correlated with the frequency (r = −.36, p < .001) and diversity (r = −.35, p < .001) of all activities currently performed, as reported in the ASAP. As participants reported more subjective cognitive difficulties in Part B of the DLQ, they reported participating in fewer activity types and less frequently.
Moderate significant correlations were found with the level of assistance needed (r = −.42, p < .001) and with the level of participating in activities out of the home (r = −.25, p < .01). As participants reported more cognitive impairments, they reported participating in fewer activities in the community and needing a higher level of assistance.
Finally, a significant correlation was found between the participants’ reports of their cognitive impairments and their satisfaction with performing participation activities (r = −.28, p < .001), indicating that greater cognitive impairments were associated with lower satisfaction in participation activities.
Discussion
The aims of this study were to (1) describe the everyday difficulties in activities relative to higher level cognitive abilities and the participation patterns reported by older adults, and (2) examine the correlations between them.
The differences among the activities in the DLQ domains correspond to the types and levels of stimuli involved and the cognitive resources required for task performance (Rosenblum et al., 2017). While many daily activities are performed as part of familiar routines within known environments, complex tasks require metacognitive functions such as planning, problem-solving, cognitive flexibility, and adaptation (Bottari & Dawson, 2011; Katz et al., 2011; Rosenblum et al., 2017). The findings of this study indicate that participants reported greater difficulties in complex tasks compared to routine activities. Additionally, in the second part of the DLQ, participants reported more deficits in functions requiring working memory, multitasking, and organization than in those requiring memory and monitoring. Existing literature has shown that higher-level cognitive functions decline with aging (Johnson et al., 2007; McGuire et al., 2006), impacting an individual’s ability to perform complex tasks such as instrumental activities of daily living (IADLs) and unfamiliar activities (Cahn-Weiner et al., 2002; Toglia et al., 2012).
Cognitive abilities are typically assessed using neuropsychological or cognitive tests conducted in laboratory settings. However, identifying an appropriate self-report tool with sufficient sensitivity to detect metacognitive deficits in daily functioning remains a challenge (Goverover et al., 2009; Schwartz et al., 2016). Despite their inherent subjectivity, self-reports can provide valuable insights into individuals’ perceptions of their participation in activities, offering information that may not be captured through objective assessments (Goverover et al., 2009; Rosenblum et al., 2017). Research has shown that self-reports are reliable in certain populations (e.g., Burgess et al., 2006; Engel-Yeger & Rosenblum, 2021; Stern & Maeir, 2014). This study contributes to the limited body of knowledge on self-reported cognitive functioning in the context of daily activities among older adults.
Correlation between DLQ and ASAP
Considering the participants’ self-reports on their cognitive difficulties while performing daily activities and participation patterns, this study’s results indicate a decrease in participation frequency and diversity, as well as an increase in the need for assistance, when participants reported more cognitive difficulties. The literature suggest that older adults are at risk for physical and cognitive impairments, which often lead to a loss of autonomy and participation (Anton et al., 2015; Winblad et al., 2016).
Another interesting finding of this study is the significant (though weak) correlation between cognitive deficits reported in the DLQ and out-of-home activities reported in the ASAP. This correlation suggests that as the participants experienced metacognitive deficits, they became less involved in out-of-home activities, whereas no comparable correlation was observed for in-home activities. Some studies have indicated that adults with cognitive decline tend to avoid leaving home and thus experience greater feelings of loneliness (e.g., Jylha, 2004). Other studies have identified social isolation and loneliness among older adults are risk factors for further cognitive-functioning deficits (e.g., Palmer, 2019; Rosado-Artalejo et al., 2017).
Limitations and future research
This study included only healthy older adults. Future research should include individuals with various medical conditions and cognitive decline associated with aging. Additionally, future studies could incorporate informant-based evaluation of functional abilities and participation, complementing self-reports.
Conclusions
Because metacognitive functions are essential to maintaining independent functioning among older adults, it is important to use ecological and subjective tools to assess these cognitive abilities within a functional concept. Moreover, participation plays a crucial role in health and well-being. Low participation and loneliness are among several adverse factors that negatively impact older adults’ cognitive functions. Additionally, a key priority for health professionals and clinicians working with this population is to maintain and rehabilitate functional abilities in daily living and participation across various settings (American Occupational Therapy Association, 2020; Steultjens et al., 2004). Assessing cognitive functioning, daily functioning, and participation as intertwined indices may lead to more effective prevention and intervention strategies for this population.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.