
Abstract
Background
Despite the clearly identified roles and need for occupational therapy in primary care, guidance on a consistent global response is lacking.
Purpose
This study aimed to gain insight into the global state of occupational therapy primary care services.
Method
Data from an online survey of the 100 WFOT member organisations was grouped by country income levels; weighted global means and ANOVA were calculated.
Results
Fifty-nine member organisations from five world regions responded, 33 (55.9%) representing high-income countries. Activities of daily living was the most addressed area; other health facilities (e.g., mental health services, rehabilitation services) were reported as a common setting. People with developmental disabilities, those with chronic illness/needs, and older adults were most likely to receive occupational therapy primary care services, with a higher likelihood of being financed by government (public) in one-on-one settings. Workforce supply, funding and training were consistently reported as key limiting factors for the profession in primary care.
Implications
While recognizing regional histories and needs, it behooves the profession to work collectively to advance its capacity to provide primary care services. Key enablers to advance this area include workforce initiatives and funding access in line with a global workforce strategy for occupational therapy.
Introduction
The terms primary health care and primary care, while often used interchangeably, are distinct concepts separately defined by the World Health Organization (WHO) (Muldoon et al., 2006). In some countries there are overlapping functions, associated with increased integration of health care systems and funding models such as universal health coverage (Carey et al., 2013), or with links with broader social assistance policies (International Labour Organization, 2017; Vaitsman et al., 2009). Both concepts (primary care, primary health care) are based on a holistic overview of individuals and systems, versus a biomedical model of health, with key aims of providing service accessibility and affordability, moving toward health promotion and disease prevention. This paper is specifically focused on primary care, which supports first-contact, accessible, continuous, comprehensive and coordinated person-focused care (World Health Organization, 2024). Primary care services are offered as close as possible to their community using an interprofessional approach with intersectoral collaboration (Epperly et al., 2019). These services are recognized as the foundation of an effective and efficient health system (Starfield et al., 2005; van Weel & Kidd, 2018).
The importance of primary care has been increasingly recognized given ageing populations (World Health Organization, 2020), the shift required from acute care to chronic disease management (World Health Organization, 2013), and clients’ increasing complexity (Marengoni et al., 2011). Similarly, the critical need for rehabilitation services (Cieza et al., 2021; Jesus et al., 2019), including within primary care (Seijas et al., 2024), and workforce shortages of professionals (World Rehabilitation Alliance, 2024), have been identified.
Numerous roles for occupational therapists exist, for example, skills assessment, adaption and re-training, delivering self-management programs, prescribing assistive technology, and supporting caregivers (American Occupational Therapy Association, 2020; Bolt et al., 2019; Donnelly et al., 2022; Silva & Oliver, 2020). The evidence confirming the impact and cost-effectiveness of occupational therapy in improving health outcomes continues to grow (Garvey et al., 2015; Gillespie et al., 2022).
Despite the clearly identified roles and need for occupational therapy in primary care, and regional examples of implementation (Bolt et al., 2019), guidance on a consistent global response is lacking. There is great variability in the establishment and organisation of the profession in different countries (World Federation of Occupational Therapists, 2020) that requires a clearer understanding of occupational therapy service delivery and funding in primary care settings to improve sustainable growth. Health service mapping is a useful approach for taking stock of services and supporting informed planning from a strategic perspective (Sekhri Feachem et al., 2017). Consistent with the World Federation of Occupational Therapists’ (WFOT) (2024) Global Strategy for the Occupational Therapy Workforce, this study aims to gain a better understanding of the global state of occupational therapy services in primary care. Specifically, this research aimed to answer the following questions: 1. How is primary care defined in occupational therapy settings across the globe? 2. What services are being provided? 3. In what settings are these services being offered? 4. What populations are being served? 5. What are the models of service delivery? 6. How are services funded and who is involved in providing services? 7. How well are population primary care needs met? 8. What supports are in place to advance occupational therapy primary care services?
Methods
This project was overseen by an international project team appointed by WFOT. This team met online and was comprised of WFOT representatives and occupational therapists with expertise in primary care from Australia, Brazil, Canada, Hong Kong, Jordan, Saudi Arabia, South Africa and Sweden. Multi-informant mapping methodology was used including the following steps: defining primary care, identifying informants, survey design, data collection, data analysis and manuscript preparation (Price et al., 2019). Achieving an agreed definition of primary care prompted the project team to explore interpretations as a preliminary component of the final survey.
A descriptive survey design (Portney & Watkins, 2009) was used to collect data. WFOT representatives developed an initial draft survey, informed by the literature on primary care, primary healthcare and occupational therapy primary care, that the project team enhanced by adding region-specific information. Email exchange, and three meetings produced 14 versions of the survey before reaching final consensus. The final survey sections included: definition clarification; settings; populations served; models used; services/interventions provided; financing of services; legislation; service providers; member organisation involvement (e.g., training opportunities and other supports); educational requirements; human resources; and factors influencing evolution of primary care.
Respondents ranked their degree of agreement using a four-point Likert scale (frequently, occasionally, rarely, never/not applicable) with a comments section. The survey, conducted in English, concluded with seven close-ended questions (and associated comments sections) and two open-ended questions (factors impacting the need for occupational therapy primary care services; invitation to provide any other information).
The delegates from 100 WFOT member organisations were invited to participate through an online survey link (Survey Monkey). An email, including the survey link, was sent from WFOT on the 6 September 2023 to request survey completion by 31 October 2023. Non-responders were contacted twice, including an extended deadline of 19 January 2024. Survey respondents provided consent for WFOT to include their de-identified data in aggregated reports of findings.
The data were entered into the Statistical Package for the Social Sciences (Version 29.0). The responses were grouped by country income levels (low, lower-middle, upper-middle, high) (World Bank, 2024). Weighted global means and standard deviations were calculated for the questions requesting an estimation of frequency (frequently = 4, occasionally = 3, rarely = 2, never/not applicable = 1) based on the assumption that the ordinal scale variables could justifiably be treated as interval variables (Nunnally, 1978). The weighting was based on the number of responding member organisations for each country income level as a proportion of the total number of possible countries within each of these levels (World Bank, 2024). To assess the similarities and differences in the means across country income levels, one-way analyses of variance (ANOVA) and Tukey’s post-hoc tests were conducted. Effect sizes were interpreted based on Cohen’s (1988) criteria: small = 0.2; medium = 0.5; large ≥0.8. For the other questions (e.g., training opportunities), frequencies (percentages) were calculated.
Free text data was analysed using a content analysis approach to condense extensive and varied raw text data and link to the survey objectives. An inductive approach was employed, and respondents’ free text comments were categorised by the first two authors, and subsequently discussed to reach consensus. This approach involved categorising concepts by frequencies to develop cross cutting themes. Within a quantitative survey, the goal of collecting free text was to provide context and assist in interpreting the numerical survey data (Elo et al., 2014).
Results
The final sample included 59 (59% response rate) member organisations representing the following world regions: Africa (n = 10); Americas (n = 10); Asia Pacific (n = 11); Europe (n = 24); Middle East (n = 4). The countries/territories were in the following income level categories: low (n = 4; 6.8%); lower-middle (n = 11; 18.6%); upper-middle (n = 10; 16.9%); high (n = 33; 55.9%). The country of one member organisation (1.7%) is unclassified.
Six countries indicated their agreement with the WHO definition of primary care. Other definitions were provided by 18 respondents, with several using the terms primary health care and primary care interchangeably; common elements included the concept of primary care as providing the first level or gateway to health care (10 responses) and references to integrative and community-based/nonhospital approaches (12 responses). Other elements reported included accessibility to services and community approaches.
Fifty-five countries provided free text examples of primary care services currently available in their country, aligned to the full human lifespan, across age groups and across clinical conditions. Commonly mentioned services included immunisation, community rehabilitation, chronic disease management, mental health and health promoting or preventive initiatives. The breadth of responses received was representative of primary care in general and not specific to occupational therapy.
Occupational therapy primary care services provided.
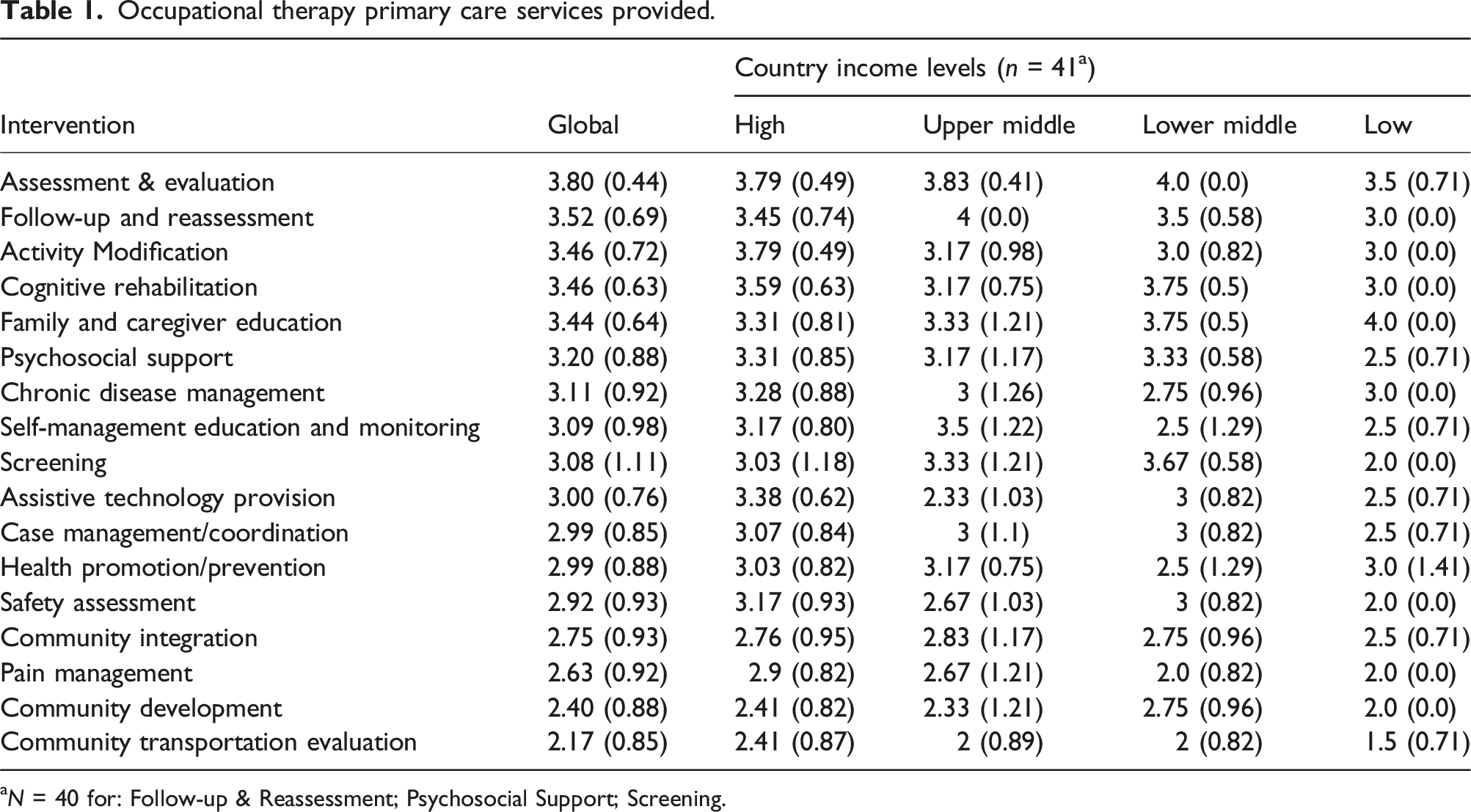
aN = 40 for: Follow-up & Reassessment; Psychosocial Support; Screening.
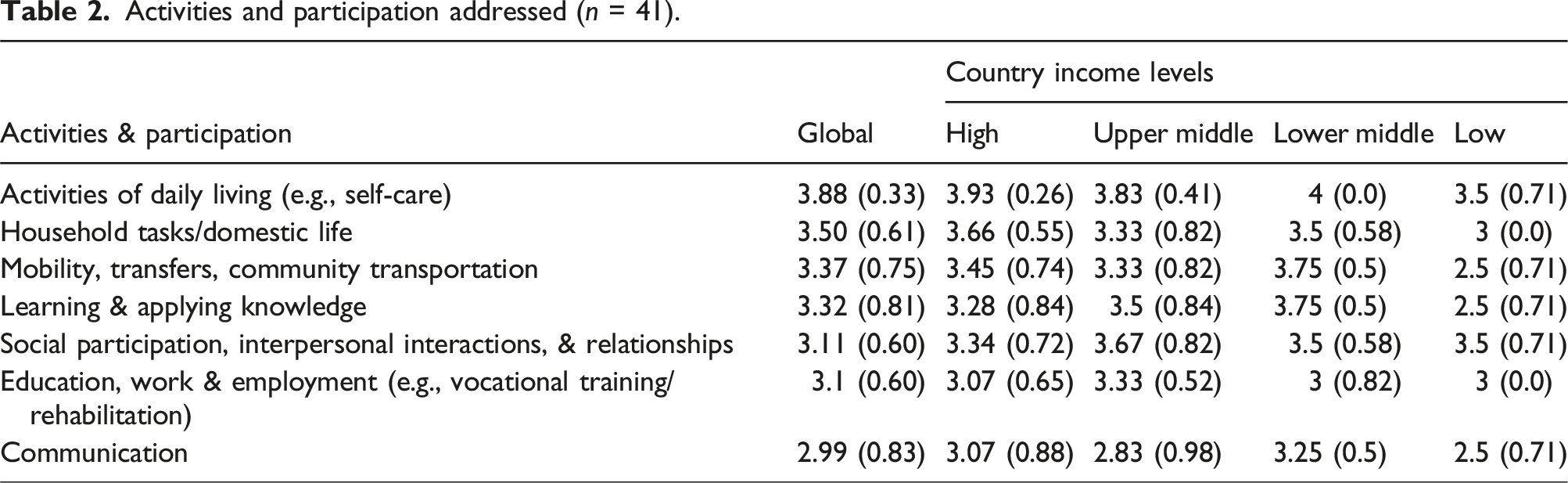
Activities and participation addressed (n = 41).
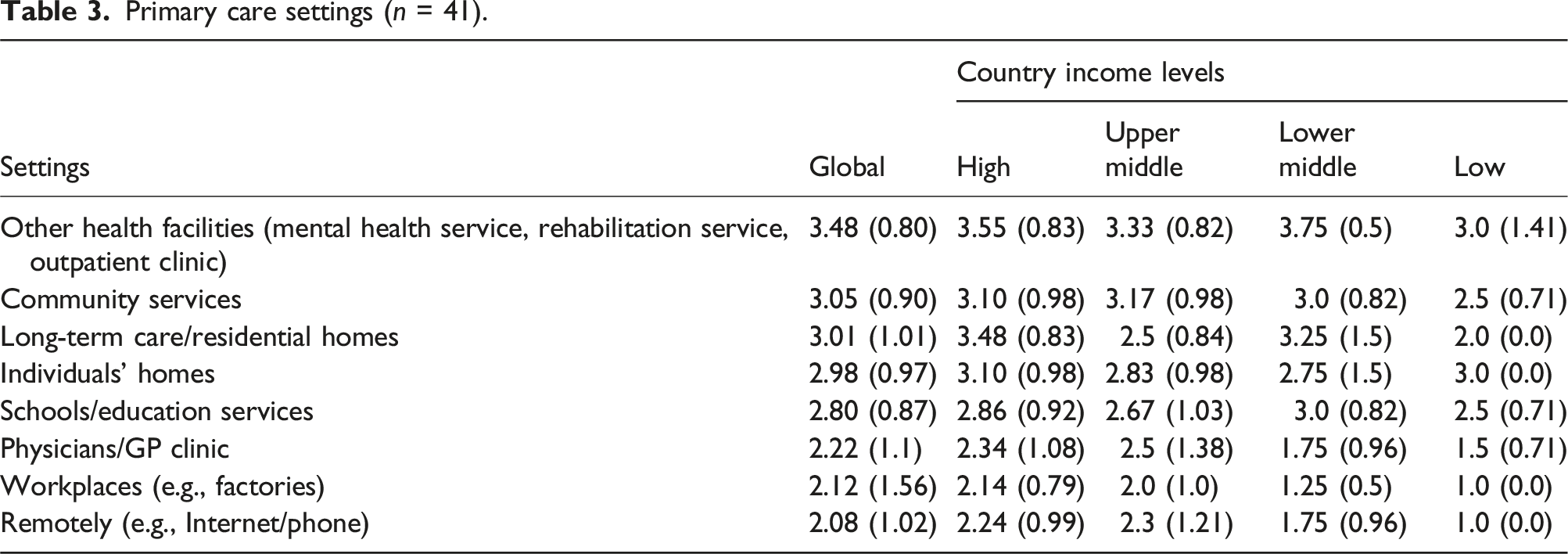
Primary care settings (n = 41).
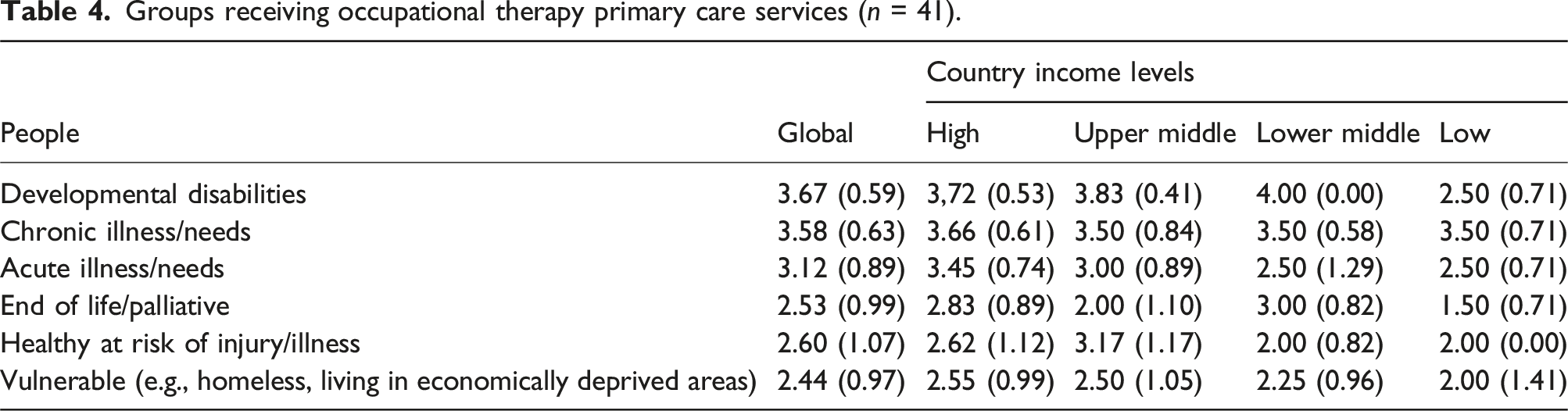
Groups receiving occupational therapy primary care services (n = 41).
The following population age groups, in descending order of weighted means (n = 41), were reported to receive occupational therapy primary care services: older adults (≥65 years: 3.57; 0.62); young children (birth-5 years: 3.53; 0.71); children (6–12 years: 3.51; 0.73); adults (19–64 years: 3.46; 0.74); adolescents (13–18 years: 3.25; 0.73). The ANOVA revealed a significant effect only for adolescents [F (3, 37) = 3.90, p = .028, η2 = 0.24]; the mean for high-income countries (3.52, SD = 0.63) was significantly higher than that for low-income (2.00, SD = 0.00) countries.
The following models of primary care service delivery, in descending order of weighted means (n = 41), were reported: one-on-one = 3.73 (0.49); groups = 3.17 (0.64); communities = 2.69 (0.90). One member organisation reporting using telehealth. The ANOVA revealed no significant effect for any of the models.
Occupational therapy primary care services are financed by the following stakeholders, in descending order of weighted means (n = 41): government (public) funding = 3.62 (0.75); private-individuals = 2.92 (1.00); private-insurers = 2.47 (1.07); not-for-profit/charitable organisations/nongovernment organisations = 2.46 (1.03); employers = 1.95 (0.96). The ANOVA revealed a significant effect for government funding [F (3, 37) = 9.49, p < .001, η2 = 0.44]; there was a significantly lower mean for lower-middle income (2.50, SD = 1.29) versus upper-middle income (4.00, SD = 0.00) and high income (3.86, SD = 0.44) countries.
The areas in which national or state/provincial legislation impacts the provision of occupational therapy primary care services in descending order of weighted means (n = 59) include: financing of primary care = 2.23 (0.73); regulation of primary care = 2.22 (0.70); primary care policy = 3.00 (0.59); quality standards for primary care = 2.18 (0.70); workforce development = 3.68 (0.83). One member organisation reported that although the primary care services designated in the country include intervention areas for occupational therapy, the profession is not specified. Another respondent reported that occupational therapy primary care service provision in the country is not impacted by legislation but rather by government policy and financing. The ANOVA revealed a significant effect for workforce development [F (3, 54) = 3.81, p = .02, η2 = 0.17]; the mean for low income (1.25, SD = 0.5) was significantly lower than that of upper-middle income countries (3.40, SD = 1.08). The ANOVA also revealed a significant effect for regulation of primary care [F (3, 54) = 3.86, p = .01, η2 = 0.18]; there was a significantly lower mean for low income (1.25, SD = 0.5) versus lower-middle (3.18, SD = 1.17), upper-middle (3.30, SD = 0.95), and high (3.21, SD = 1.19) income countries.
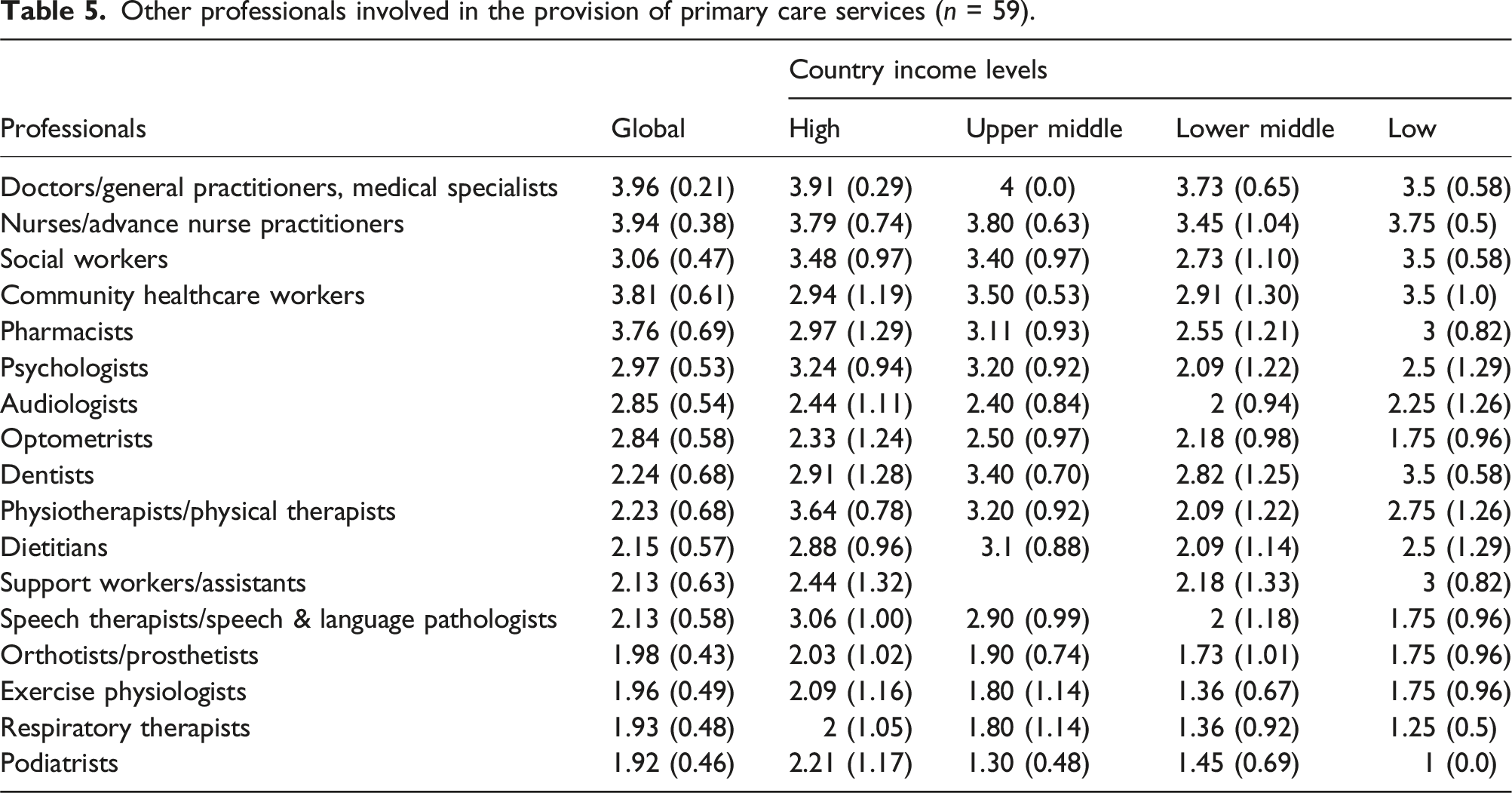
Other professionals involved in the provision of primary care services (n = 59).
When asked how well primary care needs are met by the jurisdictional system, the member organisations (n = 55) reported a global weighted mean of 2.31 (SD = 0.78) (4 = very well, 1 = not all). The ANOVA revealed no significant effect across country income levels. Forty-six (78.0%) member organisations reported that there is a shortage of occupational therapists for primary care services in their country/territory.
Content analysis of the free text data regarding the impact of various factors on meeting the needs for occupational therapy primary care services in their country/territory revealed the following factors: workforce supply (n = 29; 49.2%); overall funding for primary care services (n = 16; 27.1%)); lack of recognition of the occupational therapy role (n = 13; 22.0%); insufficient access to training (n = 12; 20.3%); lack of legislation/policy recognition (n = 9; 15.3%); insufficient occupational therapy positions (n = 8; 13.6%); non-prioritisation of primary care in the health system (n = 6; 10.2%). Additional insufficiencies noted were in; occupational therapy evidence/norms/standards (n = 5; 8.5%); work conditions (e.g., remuneration, resources) (n = 4; 6.8%); advocacy for the role (n = 2; 3.4%); occupational therapy expertise (e.g., clinical, awareness of relevant policies/legislation) (n = 2; 3.4%); opportunities for career progression (n = 1; 1.7%); lack of security in some regions of the country (n = 1; 1.7%); and rural versus urban disparities (n = 1; 1.7%).
Thirty-nine (66.1%) member organisations reported that occupational therapy primary care services are currently a priority area; however, the relative percentage of organisations in high income countries (56.8%) was higher than in the other country income levels. The capacity to make these services a priority had many challenges, for example, the level of government support available, the country’s more urgent immediate needs (e.g., malaria, maternal and childcare, HIV/AIDS), and variability in how primary care is defined.
Ten (16.9%) member organisations reported that occupational therapy primary care is seen as a specialty area in their country/territory. Free text revealed that although this area is not considered a speciality in the formal sense, it may well emerge as an area as some therapists are informally considered specialists.
Five (8.5%) member organisations reported that specific training is required by occupational therapists to provide primary care services in their country/territory. One commented that specific training is recommended but not necessarily required; furthermore, community and primary care programs have accreditation standards for occupational therapy and occupational therapy assistant programs. Thirty-two (54.2%) member organisations reported that training opportunities for occupational therapists in primary care are available in their country/territory. A few member organisations’ comments suggest that their capacity to provide training opportunities varies considerably. The hope that there will be increased fieldwork opportunities for occupational therapy students in this area was noted by one respondent.
The member organisations reported providing or facilitating the following supports for members in relation to primary care practice, in descending order of frequency (n = 59): publication/position statements/guidance documents = 39 (66.1%); training-in person/online = 27 (45.8%); occupational-therapy specific special interest group/s = 26 (44.1%); interdisciplinary networks = 26 (44.1%); dedicated conference streams/sessions = 24 (40.7%); social media/online forums = 23 (39.0%); dedicated section on the Web site = 15 (25.4%); professional/postgraduate certificate/diploma in primary care = 10 (16.9%). Other comments indicated that while some member organisations have developed considerable support resources, others are at the beginning of this development or have no resources to advance this area.
Discussion
Using a multi-informant methodology, this is the first study to map the global state of occupational therapy services in primary care with fifty-nine of 100 WFOT member organisations contributing. Despite the many areas of agreement reflecting the scope and value of occupational therapy, this discussion explores areas of variation and ideas for the future. Recommendations are consistent with the strategic directions of WFOT’s Global Strategy for the Occupational Therapy Workforce (2024).
The interpretation of primary care varies and is nuanced globally, with the terms primary health care and primary care being used interchangeably. Common themes included the concept of primary care as providing the first level or gateway to health care and references to integrative and community-based/nonhospital approaches. To progress the profession globally as integral in primary care, it is imperative that a shared occupational therapy philosophy and definition of primary care be articulated and be aligned with the health care system. At its heart, primary care is about flexible practitioners who work to provide comprehensive care, and reliance on local relationships that adapt to the cultural context (Meads, 2012). Although different jurisdictions have good reasons for the ways that they label and organise primary care services, it behooves the occupational therapy profession to work with a common definition, such as that proposed by the WHO. The WFOT’s position statement on primary care (2024) provides an important resource in this regard.
Approximately two-thirds of the responses reported that occupational therapy is provided as part of primary care services in their country/territory, with a higher proportion in high-income countries. This latter finding might suggest that acute-care services are prioritised in the context of more limited resources, and that the early development of occupational therapy services tends to be oriented towards hospital- and rehabilitation centre-based settings. This finding seems counter to the proposed benefits of a primary care model, which is well suited to underdeveloped, rural and remote settings (Carey et al., 2013).
Assessment/evaluation were the most frequently reported tasks, with a significant effect found for assistive technology provision, with a higher mean score in high income versus upper-middle income countries. Several interpretations are possible; firstly, that funding models are more supportive of assistive technology in high income countries, or alternatively that the definition of what constitutes assistive technology varies across jurisdictions (Abbot, 2007).
The results revealed that activities of daily living (e.g., self-care) were the most reported activity, seemingly consistent with its core role in the profession. There were variations across member associations regarding which populations are being served. The results showed agreement that occupational therapy services were provided to people with developmental disabilities, chronic illness/needs, acute illness/needs, people at the end of life/palliative and healthy people at risk of injury/illness. However, a significantly lower mean for low-income countries in relation to clients with developmental disabilities was revealed. Regarding age groups, higher income countries reported a greater focus on adolescents, which contrasts with Donnelly and colleagues’ (2023) scoping review findings regarding occupational therapy in primary care that reported a predominant focus on adults and older people.
Although several funding sources for occupational therapy primary care services were reported, government (public) funding was the most frequent source, with a significantly lower mean for government funding for lower-middle-income countries. The various countries’ legislation reportedly influences how primary care is funded, the regulation, quality standards and policies surrounding primary care, as well as priorities for workforce development. Funding for primary care and team membership demonstrated differences across countries in terms of income. This is possibly an artifact of government priorities and economic systems where those with universal health coverage were more likely to have primary care services as a viable part of the sector. The impact of wealth is unclear, as some higher-income countries have fee-for-service payment models, which can be viewed as limiting access to primary care occupational therapy. For example, financial models can consider the return of investment on providing occupational therapy services alongside general practitioners (Dahl-Popolizio et al., 2023). While negating the core tenets of a client-centred view of primary care, these examples highlight the important issue of who pays.
Occupational therapy primary care services across all country income levels were predominantly provided in other health facilities (e.g., mental health services, rehabilitation services), which might align with the finding that the most frequently involved professionals include physicians, nurses and midwives. Some differences in the involvement of other health disciplines (e.g., psychologists) were observed, which may reflect both the traditional organisation of services and variable funding capacity. The role of occupational therapy in an interprofessional environment provides opportunities as well as challenges. There might also be a link to the finding that limited workforce supply and a lack of funding are major contributors to the absence of occupational therapy in primary care settings. Advancing primary care globally requires an integrated approach across disciplines; the WFOT’s Global Strategy for the Occupational Therapy Workforce (2024) provides valuable direction to enable occupational therapists to be part of a considered and evidence-informed response Additional supports required to advance occupational therapy primary care services include training opportunities, position statements and guidelines to ensure a consistent approach to the reporting of primary care research and activities (Phillips et al., 2023).
Strengths and limitations of the study
Involving occupational therapy experts from diverse regions on the project team increased the likelihood of capturing the true state of occupational therapy in primary care. As 55.9% of responses came from high income countries, the global frequencies may be skewed. Chi-square Tests of Independence of the frequencies across the country income groups were not calculated as the assumptions for conducting these comparisons were not met. The different ways that primary care is understood across countries/territories might have influenced responses. The reliance on member organisations to report on the current state of occupational therapy in primary care in their jurisdiction may have impacted data accuracy. Although the response rate of 59% is considered generally acceptable (Nulty, 2008), caution in generalising the findings to the entire profession is required.
Conclusion
This study is the first to attempt to capture the global state of occupational therapy in primary care. Findings provide valuable information to inform the future of the workforce and enhance access to occupational therapists in primary care settings. Enablers identified include funding options, improved standards for service delivery, professional development, and advocacy for supportive public policy to overcome challenges and facilitate occupational therapy primary care provision globally. Promoting practice based on best available evidence worldwide should be prioritized and will help increase access to affordable, quality occupational therapy primary care services.
Footnotes
Author contributions
All the authors participated in the development of the survey, and preparation and approval of the manuscript. The first three authors analysed the data.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.