
Abstract
Background
Educational technology’s rapid evolution has resulted in an increase in the adoption of virtual reality (VR)-based educational modules in medical and nursing education.
Purpose
To develop and integrate a 360-degree video depiction of medical facilities into occupational therapy educational curriculum, and assess its impact on students’ learning through a questionnaire survey and text-mining.
Method
Participants included 62 first-year occupational therapy majors from the 2022 and 2023 cohorts. The participants viewed a 360-degree video of three facilities (one psychiatric hospital and two general hospitals) in a class on their smartphones. They responded to self-administered questionnaires on the VR experience, including a free comment question that was subjected to text mining.
Findings
Early clinical exposure facilitated by VR benefited students. The ease of viewing images, enhanced understanding of the rehabilitation facilities’ environment, and a significant boost in learning motivation after class were evident. The data revealed students’ growing excitement for future 360-degree video-based classes and their high satisfaction with facility tours.
Conclusion
This study demonstrated that early experiential learning using VR effectively motivates occupational therapy students and deepens their understanding of clinical environments.
Introduction
Early clinical exposure (ECE) is an educational approach evident in medical education that includes the early exposure of students to actual patients in clinical and social settings. ECE deepens students’ understanding of the roles of hospitals and healthcare professionals. Prior research has found several benefits of ECE, emphasizing that it enhances communication skills, clinical competence, teamwork, empathy development, and motivation for self-learning in the preclinical period (Basukala & Chaudhary, 2021). Early exposure to clinical cases has also been shown to enhance students’ understanding of medical knowledge and motivation for self-learning (Aggarwal et al., 2021; Tayade et al., 2021). However, while the importance of ECE is becoming increasingly recognized, institutional cooperation is essential for its implementation, and the process of moving to the institution must also be considered because it requires significant coordination and time.
In recent years, there have been reports of educational initiatives using virtual reality (VR) in medical (Buitron de la Vega et al., 2022) and nursing (Hu et al., 2023) departments. Among the dynamic advances in educational technology, VR has been highlighted as a promising tool for providing immersive and interactive experiences. Furthermore, VR has shown the potential to foster essential soft skills such as communication, decision-making, time management, and critical thinking among healthcare students (Mørk et al., 2024). There have been reports of using VR in hospital tours (Zertuche et al., 2020) and in surgical site experiences (Speidel et al., 2023). Despite these positive accounts, it has also been suggested that the frequency of VR usage in occupational therapy education is not high, partly due to the time and cost associated with constructing virtual environments (Grant et al., 2021). Among the advanced video formats, 360-degree videos enhance the motivational impact of traditional videos and allow for the creation of realistic and authentic teaching-learning scenarios. Although 360-degree videos offer less interactivity than fully immersive VR, they still provide more engagement than conventional video technology, primarily through its user-controlled omnidirectional view (Rosendahl & Wagner, 2024). In nursing education, for example, studies have shown that students engaged in actual simulations experience the highest level of immersion, followed by those observing through VR, while students observing via television exhibit the lowest level of immersion (Dang et al., 2018). Although VR provides a lower sense of immersion than actual simulations, it is widely acknowledged as an innovative educational strategy that enhances learning outcomes through experiential learning. Despite the variability in the overall quality of evidence (Woon et al., 2021), interest in VR as a teaching tool continues to grow.
Furthermore, students who actively utilize the tools and communication features available within VR for collaborative tasks can effectively transfer their knowledge and apply it to real-life physical examination settings. This suggests that the immersive 360-degree video instructional design has the potential to complement traditional clinical training in medicine (Davidsen et al., 2024). From this, using a 360-degree video for facility tours can overcome geographical barriers, bridge gaps in understanding and experience by simulating real-world environments, and enhance student engagement and motivation in occupational therapy settings. Additionally, VR can provide a controlled learning environment where students can repeatedly practice and refine their skills without posing any risk to patients. However, incorporating VR into ECE has not been extensively compared to traditional ECE, thus indicating a need to explore its unique benefits, particularly in terms of immersive learning, logistical convenience, and replicability that traditional ECE alone cannot fully achieve.
However, there are various challenges to incorporating VR into medical education, including the initial cost of installing a VR system. Additionally, faculties require specialized training in creating teaching materials and providing support to students on how to use the system. For educational institutions, ensuring the accessibility and affordability of VR technology is essential for its widespread adoption as an innovative educational tool. Nonetheless, recent findings indicate that 360° VR photos can be a relatively low-cost and easily implemented educational tool for ECE, as they offer an immersive clinical experience while facilitating knowledge acquisition and spatial orientation (Speidel et al., 2023). Therefore, this study developed the idea of creating and utilizing simple VR images of facilities so that students can experience the atmosphere of the facilities while staying on campus.
This study aimed to develop and integrate a VR depiction of medical facilities into occupational therapy educational curriculum, and assess its impact on students’ learning through a questionnaire survey and text-mining. We hypothesized that VR-based ECE would allow students to experience the atmosphere of facilities without having to leave the university campus, thus increasing their motivation. Based on the survey results, we tested this hypothesis using text mining (Kocbek et al., 2016; Shikama et al., 2021).
Methods
Study design and setting
We developed VR-based ECE videos and integrated them into the occupational therapy educational curriculum. The videos were previewed on campus for first-year occupational therapy students majors commencing their studies in 2022 and 2023. Subsequently, a survey and text mining were used to examine the impact on student learning.
Participants
Participants were 62 first-year students majoring in occupational therapy (29 male students and 33 female students; Mean age = 18.1 years, SD = 0.5) at a university in 2022 and 2023 who attended the relevant classes.
Viewing procedure
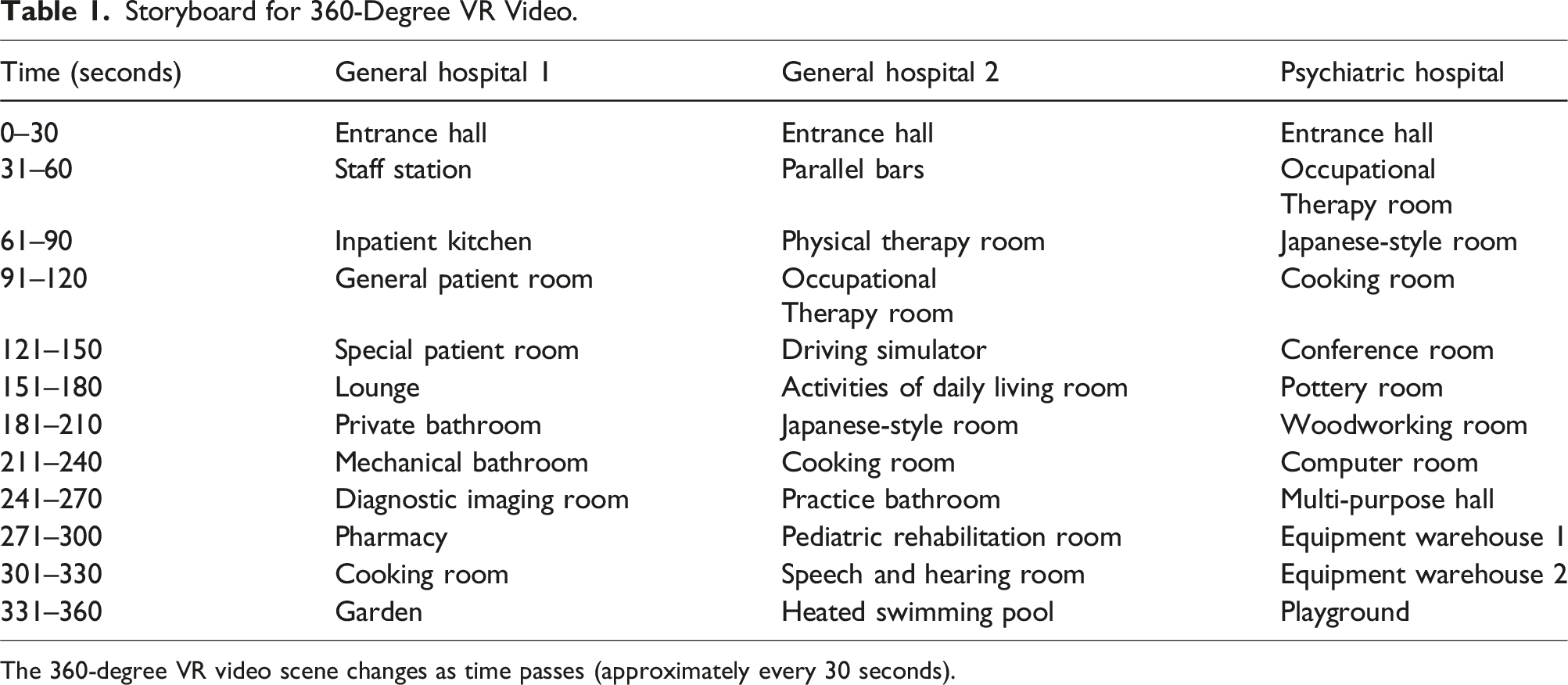
Images captured by a VR camera can be uploaded to the Hacosco store, a VR content-sharing platform, to enable VR to be experienced on a standard smartphone. Therefore, with an Internet connection, original VR experiences are possible worldwide (Figure 1). In this study, a 360-degree video was employed to view an environment similar to actual clinical situations. To begin with, the teacher responsible for the class filmed three facilities (one psychiatric hospital and two general hospitals) with a VR camera (Ricoh Theta Z1; RICOH IMAGING COMPANY Ltd) individually in an environment where patients were not visible. Edited 360-degree videos of the facilities were made available at the Hacosco store (Hacosco Inc) in advance, and QR codes were prepared for viewing. During the class, students scanned the QR code displayed on the screen in front of them with their smartphones, played it back in the VR binocular view, and set their smartphones on the VR goggles VRG-D02PBK (ELECOM Co., Ltd) to watch it. In this case, as a sanitary consideration, a protective mask VR-MS50 (ELECOM Co., Ltd) was used to prevent contamination, and the equipment was disinfected with alcohol. To avoid eye fatigue, prolonged continuous viewing time, and visually induced motion sickness, the participants were paired and took turns watching a 6-min video of each facility for a total of 18 minutes (three facilities per participant). Table 1 shows the storyboard for the 360-degree video. During the viewing, the instructor provided an overview of each facility and verbally explained their features, such as the ceramic, woodworking, and pediatric rehabilitation rooms, and activities of the daily living room, and observed the viewing in the classroom. System diagram of delivery using cloud storage. Storyboard for 360-Degree VR Video. The 360-degree VR video scene changes as time passes (approximately every 30 seconds).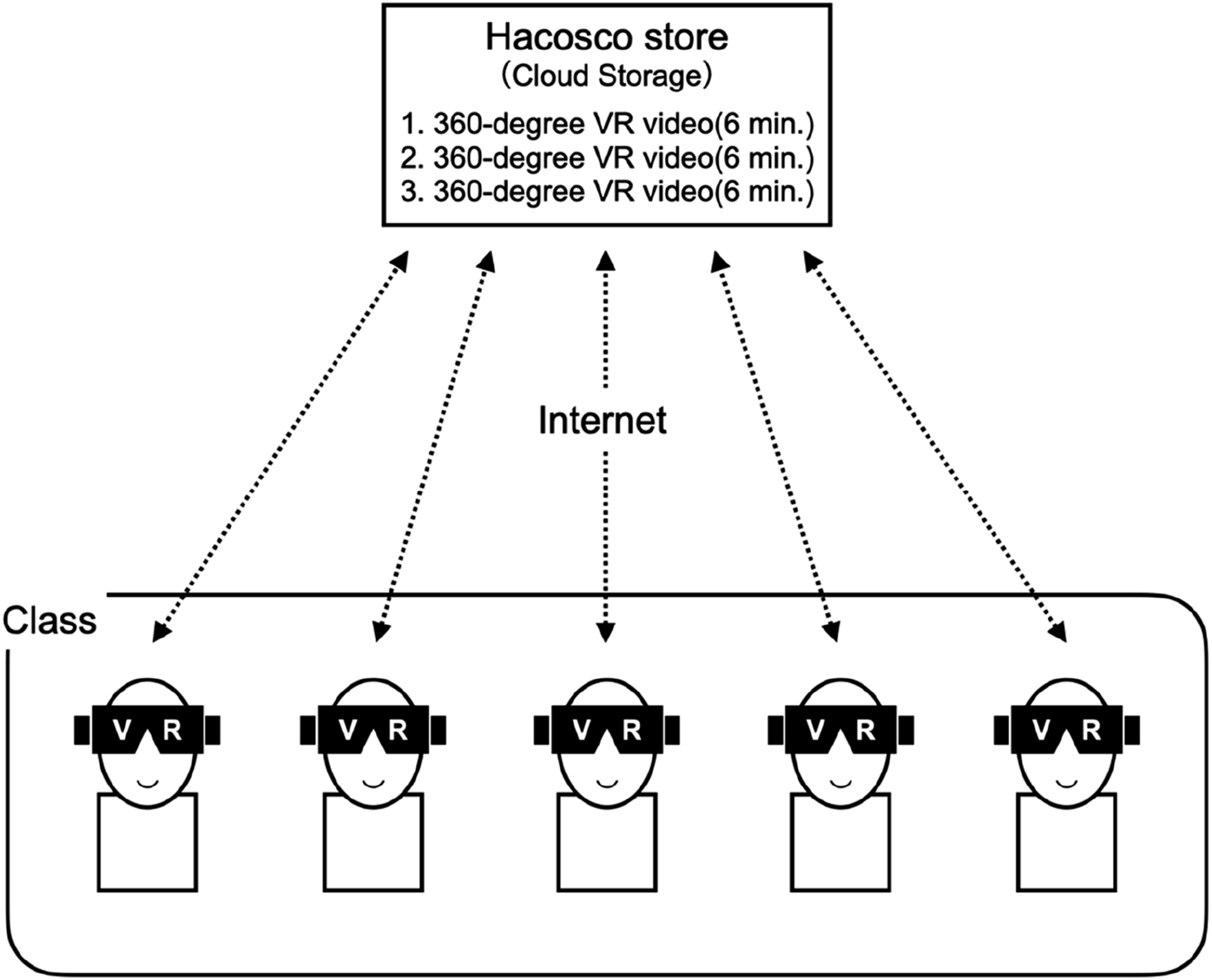
Survey method
The teachers responsible for the class distributed anonymous self-administered questionnaires to the students after the class. The questionnaire included questions regarding age, gender, whether they had visited rehabilitation-related facilities, and whether they had previously viewed VR. The following five items were answered on a 10-point scale, from 1 (not at all applicable) to 10 (very applicable): (1) I can understand VR effectively conveyed the facility’s atmosphere, (2) The introduction of the VR of the facilities in this study was visually elucidatory, (3) I feel more motivated to learn after the class, (4) I want to experience classes using VR in the future, and (5) I am satisfied with this VR visit of the facilities. In addition, we asked respondents about their impressions of the program through free comments.
Ethical considerations
The study respected the participants’ autonomy and adopted an opt-out consent process for participation. All participants were provided with detailed written information about the purpose of the study, expected risks and benefits, voluntary nature of participation, and handling of their data. Participants had the right to choose not to participate in the study after receiving this information and could express this intention unconditionally at any time. In this study, we provided participants with ample opportunity to decline participation, but no students opted out. In addition, personal information was strictly anonymized, and technical measures were taken to protect data to safeguard participants’ privacy and ensure data security. This study was approved by the Ethics Committee of the University (Approval no.: 552).
Analysis method
The basic information regarding the virtual facility tour items was presented as percentages, and the average values were calculated. To objectively analyze the open-ended response data, quantitative text analysis was conducted. Quantitative text analysis is a method that involves converting large amounts of textual data into numerical values for analysis, quantification, and visualization. The KH Coder software used here employs multivariate analysis, allowing for the elimination of biases stemming from the analyst’s theories or perspectives, thereby ensuring the objectivity and reliability of the analysis (Higuchi, 2016, 2017).
Initially, the open-ended responses were organized in Excel format, and the text data were analyzed using KH Coder Ver. 3.0. For morphological analysis, the Japanese morphological analysis tool Chasen (Matsumoto et al., 2002) was employed to segment the text at the word level. KH Coder is widely used for statistical analysis of text data and supports various methods such as co-occurrence network analysis and hierarchical cluster analysis (Higuchi, 2017). Chasen is recognized as a highly reliable tool for morphological analysis of Japanese text. To enhance the objectivity and reliability of the analysis, the standardization of synonyms and extraction of compound terms were conducted through discussions among multiple researchers.
The analytical procedure was as follows: First, free-response statements were converted into Excel data. Next, the data was input into the KH Coder, pre-processed, and divided into morphemes by Chasen, a morphological analyzer that extracts words and compound words. This process divided the words “VR facility tour” into the words “VR,” “facility,” and “tour.” Words that we did not want to divide were extracted as compound words. Subsequently, words with the same meaning were extracted using the Key Words in Context concordance function to check the context of the words before and after the extracted words to be analyzed. Resultantly, it was confirmed that “rehabilitation,” “rehab,” and “rehabilitate”; “occupational therapy” and “OT”; “facility” and “place”; “tour,” “see,” and “can see” were synonyms. Therefore, these words were replaced with “rehabilitation,” “occupational therapy,” “facility,” and “tour,” respectively. Hierarchical cluster analysis was then performed to identify combinations of words with similar patterns of occurrences, and a co-occurrence network was created to identify closely related words in the sentences.
Results
Questionnaire responses
Questionnaire responses were received from all 62 students enrolled in the course (valid response rate: 100%). Overall, only 35% (n = 22) of the participants had previously visited a rehabilitation facility, and only 23% (n = 14) had experienced viewing through VR. Regarding the ECE using VR, the average score on understanding the atmosphere of the rehabilitation facility well using VR was M = 8.45, SD = 1.44. The average score on the introduction of VR to see the facilities as convenient and accessible was M = 8.21, SD = 1.66. The average rating for motivation to learn after the VR class was M = 8.76, SD = 1.44. The average score on wanting to experience more classes through VR in the future was M = 8.03, SD = 2.12. Finally, satisfaction with the VR facility visit showed a high level of satisfaction with an average of M = 8.52, SD = 1.78.
Free writing responses
Frequent words
Top 50 Featured Words With Their Frequencies.
Hierarchical clusters
The results of the hierarchical cluster analysis showed that the clusters could be classified into five categories. The first cluster included “class,” “this time,” “rehabilitation,” “interest,” “tour,” “facility,” “room,” “hospital,” “go,” and “reality.” The second cluster included “VR,” “use,” “first time,” “sensation,” and “fun.” The third cluster included “atmosphere,” “understand,” “inebriate,” “slightly,” “professional experience,” and “currently.” The fourth cluster included “fascinating,” “self,” “friend,” and “currently.” The fifth cluster included “personal experience,” “image,” “occupational therapy,” “opportunity,” and “good.”
Interpreting the five clusters, based on the similarity of the words, the first cluster could be considered to represent the facility tour as a class, the second cluster as the use of VR, the third cluster as the time spent experiencing it, the fourth cluster as the appearance of self and others in VR compared to regular viewing, and the fifth cluster as the image of occupational therapy.
Co-occurrence network
A co-occurrence network was created to visualize learning using VR during the early experience training. We set the minimum number of occurrences for aggregating the co-occurrence network to four. A larger circle indicates more occurrences in the network, and a line between words indicates their co-occurrence and relevance. Line thickness indicates the strength of the association, and the color of the circle indicates the grouping. Here, a group of words was treated as a word group. In this case, words were classified into six word groups. Specifically, word groups consisting of “tour,” “facility,” “reality,” “hospital,” and “go,” and word groups consisting of “VR,” “fun,” “first time,” “use,” “personal experience,” and “sensation” were displayed. Among these, “tour,” “facility,” “VR,” and “fun” were highly related (Figure 2). Co-occurrence networks of free descriptions in early clinical exposure using virtual reality.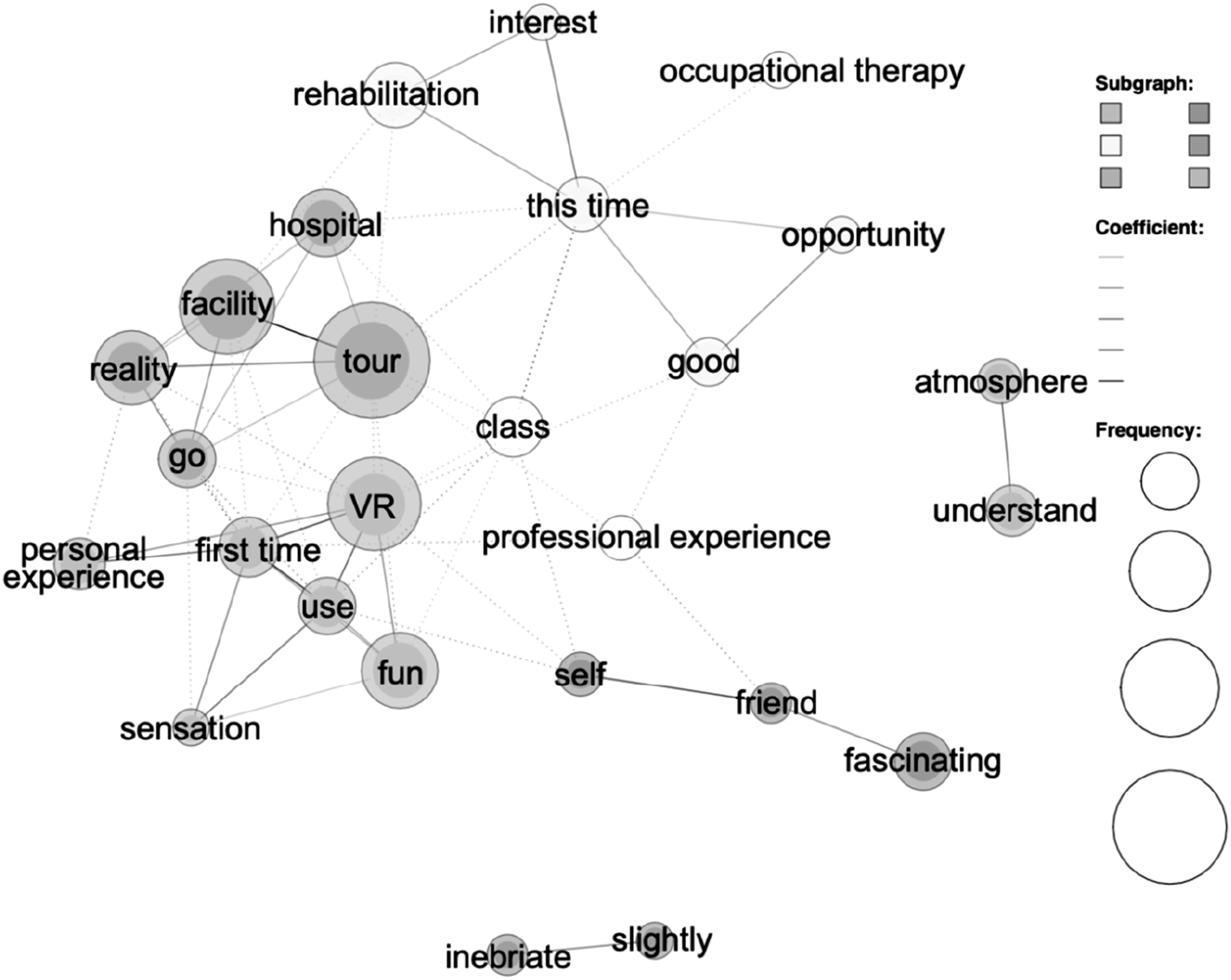
Discussion
This study aimed to evaluate the effects of VR-based ECE on occupational therapy students’ attitudes toward learning. By analyzing questionnaire data and applying text mining techniques to open-ended responses, the study assessed this VR-based approach’s impact on students’ learning motivation and comprehension of the facility. The findings indicate that virtual facility tours positively influence students, boosting their motivation to learn and deepening their understanding of the clinical environment.
Significance and challenges of using VR in the classroom
Among the 62 survey respondents (100% valid response rate), only 35% (n = 22) had previously visited a rehabilitation facility, and an even smaller proportion, 23% (n = 14), had experienced VR. These findings underscore that many students lack familiarity with the atmosphere and environment of real-world rehabilitation settings. The use of 360-degree video-based facility tours addresses this gap, providing an effective way to help students visualize clinical settings more concretely. The results showed a high average rating for understanding the facility’s atmosphere through VR, with a mean score of 8.45 (SD = 1.44). Many students reported that VR allowed them to gain a realistic sense of the facility’s environment. The perceived convenience of using VR to “visit” facilities was also rated highly, with an average score of 8.21 (SD = 1.66), suggesting that VR effectively overcomes spatial and temporal limitations. Moreover, students’ motivation to learn after the VR class was the highest-rated aspect, with a mean score of 8.76 (SD = 1.44), indicating a strong positive impact on learning motivation. The application of VR has been explored in various fields, including rehabilitation (Karamians et al., 2020), architecture (Zhang et al., 2020), and industry (Berg & Vance, 2017), illustrating its broad utility as an educational tool.
Learning effects seen from free-text analysis
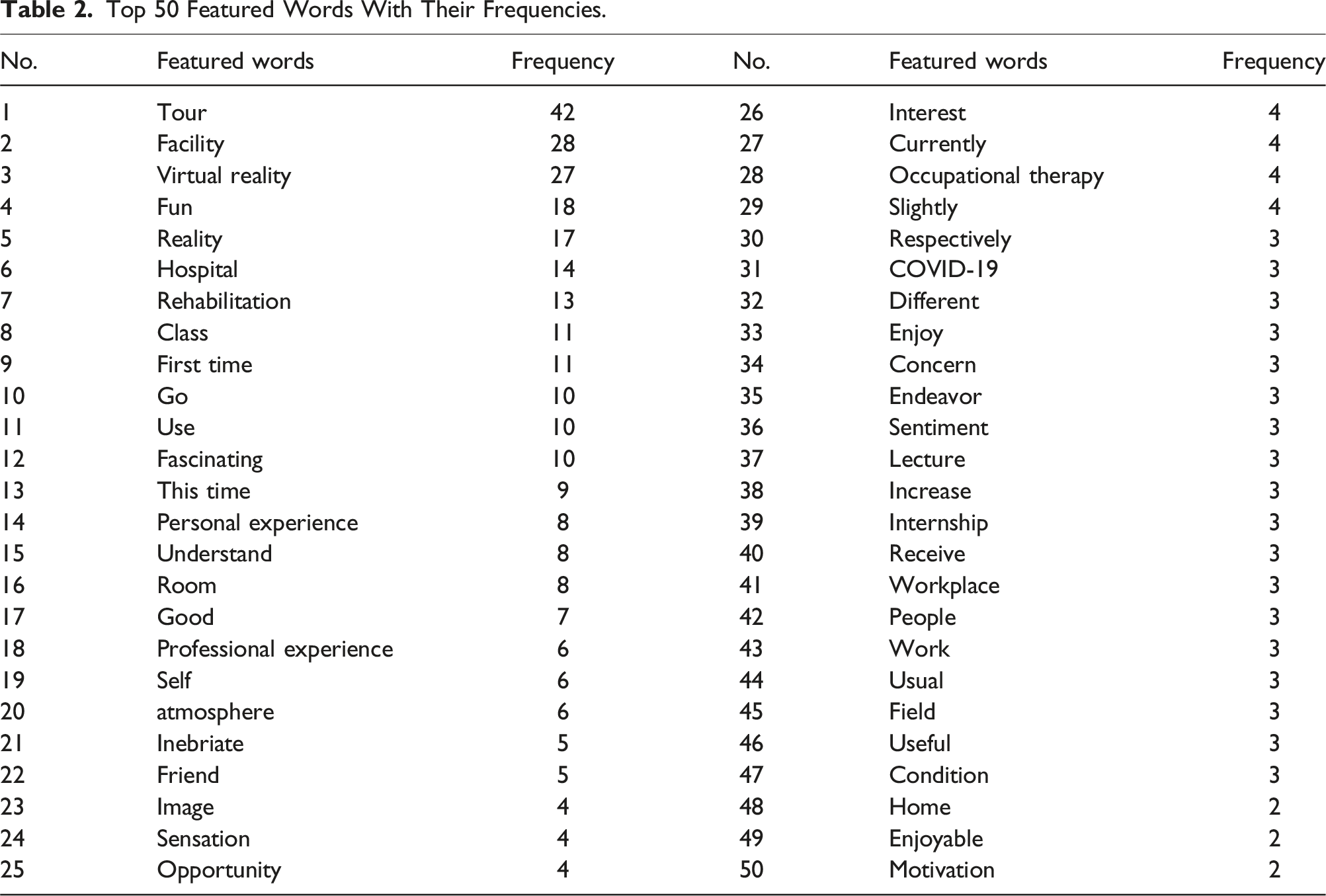
The analysis of free-text responses yielded 1,923 words, with “tour” (42 occurrences), “facility” (28 occurrences), “VR” (27 occurrences), “fun” (18 occurrences), and “real” (17 occurrences) being the most frequently used terms. This frequent mention suggests that students perceived the VR facility tour as both enjoyable and realistic. A co-occurrence network analysis showed strong associations between “tour,” “facility,” “VR,” and “fun,” indicating that the VR experience was not only engaging but also a meaningful learning activity. These findings align with Speidel et al. (2023), who reported that experiential clinical education using VR was both enjoyable and beneficial for students. The hierarchical cluster analysis identified five clusters, with the fifth cluster including terms such as “experience,” “image,” “occupational therapy,” “opportunity,” and “good.” This indicates that many students were able to form a concrete image of occupational therapy through the VR experience. Given that 65% of the students had never visited a rehabilitation facility, the use of a 360-degree video proved to be an effective way to virtually simulate the clinical environment, providing students with a valuable opportunity to experience the atmosphere and context of actual practice settings.
Improvement in motivation to learn and understanding of the facility through VR use
The high average score of 8.76 (SD = 1.44) for learning motivation after the VR class indicates that the experience greatly enhanced students’ enthusiasm for learning. This increase in motivation may be attributed to VR’s ability to provide a realistic and immersive view of clinical settings, allowing students to concretely visualize their future professional roles. Similarly, Kyaw et al. (2019) found that VR can simulate realistic clinical scenarios in a controlled environment which contributes to the effective learning of clinical skills among medical students. For occupational therapy students, early exposure to a simulated clinical environment through VR not only enhances motivation but also deepens their understanding of the profession. By allowing students to virtually experience real-world clinical settings, VR facilitates a more tangible grasp of occupational therapy practice, potentially bridging the gap between theoretical knowledge and practical application.
Challenges in VR use and their countermeasures
While the use of VR in education offers significant benefits, some challenges have been identified. Based on free-text responses and in-class feedback, students reported issues such as damage to smartphone screens, eye fatigue, and feelings of sickness. These problems may be related to factors like video resolution, device performance, and individual differences in susceptibility (Howard & Van Zandt, 2021; Nürnberger et al., 2021). One particularly prevalent issue is Visually Induced Motion Sickness (VIMS), which is a common concern when using VR. It presents a barrier to wider adoption in educational settings. Several countermeasures can be implemented to address these challenges. First, using high-resolution and high-frame-rate videos can help reduce the likelihood of motion sickness.
Additionally, checking the condition and specifications of students’ devices before use can help identify potential issues, and providing school-owned devices may be a practical solution when necessary. It is also crucial to advise students who are prone to motion sickness to take precautionary measures, such as taking regular breaks during the VR experience. These steps can help mitigate the adverse effects and improve the overall effectiveness of VR in educational environments.
360-Degree video in educational settings and future prospects
The findings of this study suggest that VR-based ECE is a valuable tool for occupational therapy students’ educational training. This approach is particularly beneficial when it is challenging to arrange visits to actual facilities or accommodate large groups of students at clinical sites simultaneously. By offering immersive and realistic experiences, VR can extend learning opportunities beyond time and location constraints, such as introducing students to overseas facilities or specialized environments that would otherwise be inaccessible. Additionally, 360-degree videos can help standardize the learning experience among students. Unlike in-person facility visits, where the quality and scope of the experience may vary for each student, VR ensures that all participants are exposed to the same content. This consistency reduces disparities in learning outcomes, providing a more equitable educational experience. The integration of a 360-degree video into education not only addresses logistical limitations but also supports a uniform and comprehensive approach to experiential learning in occupational therapy programs.
Limitations and prospects of the study
This study has several limitations. First, the sample was restricted to occupational therapy students from a single university, which limits the findings’ generalizability. The reliance on self-reported data is another limitation, as responses may be affected by social desirability bias. Additionally, the study lacked a control group and did not incorporate pre- and post-intervention comparisons, limiting the ability to draw definitive conclusions about the impact of VR-based education on students’ learning outcomes. We also did not assess the effects of long-term learning or the development of actual clinical skills following VR-based education. While 360-degree videos provide an immersive experience, they lack interactivity beyond allowing users to change their field of vision based on head movements. Future research should aim to include students from diverse institutions and disciplines to enhance generalizability and adopt a long-term approach to evaluate how VR-based learning influences sustained learning outcomes and clinical skill development. Employing structured questionnaires, control groups, and pre- and post-intervention measurements would offer a more robust assessment of VR’s unique benefits and limitations. Additionally, the text mining process standardized terms for consistency; however, this approach may have oversimplified nuanced differences between terms. Incorporating these nuances into a deeper analysis of the free-text responses could provide richer insights into how the qualitative themes and clusters support or elucidate the quantitative findings. From a methodological perspective, this study employed co-occurrence network analysis to examine word relationships within the dataset. Although this method is useful for identifying patterns in textual data, it is ideally suited for larger datasets to ensure more robust and meaningful associations. Moreover, while the removal of stop words was necessary for analysis, it may have affected the interpretability of the results. Future research should consider using larger datasets and explicitly reporting the retained meaningful words after stop-word removal to enhance reproducibility and transparency.
Conclusion
This study demonstrated that early experiential learning using VR effectively motivates occupational therapy students and deepens their understanding of clinical environments. The use of the 360-degree video approach notably enhanced students’ understanding of the facility’s atmosphere and increased their learning motivation. Participants also expressed high levels of satisfaction with the class. Analysis of the free-text responses also indicated that students perceived the 360-degree video as a realistic and enjoyable learning experience. Integrating 360-degree video methods into educational settings holds significant promise for enriching students’ learning experiences and supporting their future professional development.
Footnotes
Acknowledgements
We would like to thank the staff of the Oyamada Memorial Hospital, Suzuka Kosei Hospital, and Sakuranomori Hospital for their cooperation in filming the VR videos.
Author contributions
YN conceived the study, participated in its design and coordination, collected samples, analyzed and interpreted the data, and wrote the first draft of the manuscript. YK, HS, and CM participated in its design and coordination, and analyzed and interpreted the data. All the authors have read and approved the final version of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.