
Abstract
Introduction
Motor function deficits, including poor posture control and balance, are common in individuals with schizophrenia and may have impacts on their occupational performance in work and daily activities (Putzhammer & Klein, 2006). Poor balance performance was correlated with body composition, metabolic syndrome, negative symptoms, and cognitive functions (Vancampfort et al., 2012). The rates of falls in psychiatric settings were found to be higher compared to general hospital settings, with a range of 4.1–6.4 falls per 1,000 occupied bed days, as opposed to 3.1 to 3.7 falls per 1,000 occupied bed days in general hospitals (Scanlan et al., 2012). Furthermore, injurious falls were more prevalent in mental health facilities (44.5%) than in community hospitals (37%) and general acute hospitals (33.4%) (Healey et al., 2008). Remarkably, individuals diagnosed with schizophrenia constitute a significant majority in psychiatric setting (National Health Insurance Medical Statistics, 2022) and had a 7.5 times higher risk of falling and were more likely to experience repeated falls than patients with neurosis (Tseng et al., 2013).
It is suggested that proper assessments of balance and training programs should be developed to improve function and participation for this clinical population (Feldman et al., 2020). Some studies have used force plate and gait analysis instruments to measure the balance function of individuals with schizophrenia (Marvel et al., 2004; Putzhammer et al., 2004). Marvel et al. (2004) used a force plate to measure the magnitude of postural stability and found that, compared to the healthy population, individuals with schizophrenia have subtle yet quantifiable disturbances in the control of posture and balance. However, force plates are generally expensive and difficult to implement in clinical settings (Visser et al., 2008). In contrast, field balance assessments may offer advantages in terms of ease of use and practicality for clinical settings (Horak et al., 1997).
The common field balance assessments for various populations include the Tandem walking test (TW), Star excursion balance test (SEBT), One-leg stance (OLS), Functional reach test (FRT), Timed up-and-go test (TUG), Romberg test, Force platform, Mini-balance evaluation systems test (Mini-BESTest), and Berg balance scale (Tyson & Connell, 2009). Several specific balance assessments have been examined for psychometric characteristics in intellectual disability groups (Blomqvist et al., 2012) and the elderly (Blankevoort et al., 2013).
The unique characteristics of balance in individuals with schizophrenia may limit the application of field balance assessments used for the general population to this clinical population. A larger anterior-posterior postural sway is noted in people with schizophrenia during unreliable somatosensory conditions when standing on a sway support surface (Teng et al., 2016). Furthermore, the impaired physical balance performance in people with schizophrenia is associated with negative symptoms, cognitive functions, as well as the dosage of antipsychotic medication and its side effects (Vancampfort et al., 2013). Indeed, only a few studies have explored the reliability and validity of the aforementioned balance assessments for individuals with schizophrenia. These include one that used the tandem gait test to assess gait and static balance (Jeon et al., 2007) and another that used the Flamingo balance test to assess whole-body balance (Vancampfort et al., 2012). To identify specific balance assessments that are easy to use and quick to administrate in clinical settings, five specific balance assessments were investigated in this study, including the Star excursion balance test (SEBT), One-leg stance (OLS), Functional reach test (FRT), Timed up-and-go test (TUG), and Tandem walking test (TW).
The study aimed to examine the test-retest reliability, concurrent validity, and discriminant validity of five balance assessments battery for individuals with schizophrenia. The optimal cutoff scores to differentiate fallers and non-fallers for specific assessments were also determined by using conventional receiver operating characteristic curve (ROC) analysis.
Methods
Study design
With convenience sampling, participants were recruited using flyers and word of mouth from a psychiatric hospital, a community psychiatric rehabilitation center, and a long-term care facility in southern Taiwan. The study was approved by the Institutional Review Board of the Kaohsiung Medical University Hospital (KMUHIRB-SV(II)-20160013). All participants provided written informed consent before their participation.
Participants
Initially, participants who had a history of falls within a year were referred from the study institutions through the medical records (n = 50). Of them, 14 participants met the eligibility criteria (i.e., faller group). And then, the other 14 age-matched participants (±3 years) without a history of falls were further recruited from the study sites (i.e., non-fallers group). One was dropped out from each group during the study process due to not able to follow the test protocol.
The inclusion criteria were: (1) aged 20 (the legal age of adults in Taiwan) to 64 years, (2) diagnosed with schizophrenia according to DSM-IV or DSM-5 by psychiatrists, (3) being able to walk at least 10 m independently without a walking aid, and (4) being able to follow simple instructions. To assess this, we designed three basic movements with corresponding instructions: standing with the feet shoulder-width apart, raising both hands forward, and performing a forward lunge.
Exclusion criteria included: (1) those with a diagnosis of visual impairment, neurological disease (such as Meniere’s disease), musculoskeletal dysfunction, brain injury or organic psychiatric disorder, and (2) those with a history of epilepsy, alcohol or drug abuse.
Data collection procedures
The balance assessments were carried out by the primary investigator, a senior occupational therapist, who works in the psychiatric rehabilitation field. The test order of the balance assessments was determined randomly. Depending on the needs of participants, a rest time of 1–3 minutes was given between each test to prevent fatigue. All participants did the five balance assessments battery twice. The interval between the test and retest was 7–14 days. The force plate testing was administrated before the retest session. The Clinical Global Impressions scale (CGI) (Busner & Targum, 2007) and Brief Psychiatric Rating Scale (BPRS) (Chang et al., 1986) were used to assess the severity of the overall psychiatric symptoms of an individual. With participants’ consent, the principle investigator interviewed the clinical personnel responsible for the participants’ care, such as senior nurses or therapists, to complete the CGI scale, assessing the observed symptoms, behaviors, and functions of the participants over the past week. The CGI scale is rated on a seven-point scale: 1 being normal, not at all ill, and 7 being among the most extremely ill patients (Busner & Targum, 2007). The clinical personnel were blinded to the study purpose and the results of the balance tests. The BPRS was administered by the primary investigator. The daily dosages of antipsychotic medications were extracted from medical records and calculated into chlorpromazine equivalent dosages in accordance with established literature guidelines (Inada & Inagaki, 2015). A chlorpromazine equivalent represents a dosage of an antipsychotic drug equivalent to an oral dose of 100 mg chlorpromazine (Fargason & Birur, 2021).
Balance assessments
Star excursion balance test (SEBT)
The SEBT was set up on the ground with eight lines extending radially outward from a center point, and the angle between the lines is 45°. The participant stood on one leg barefoot, and the other leg stretched along with one of the lines to the maximum distance without falling to the ground. The further the extended distance, the better the performance of the dynamic posture control. The elongation distance was normalized using the length of the extended leg, and the performance was expressed as a percentage of lower limb length (Gribble et al., 2012).
The measurements were administered in three directions recommended by previous research, including anterior, posteromedial, and posterolateral movements (Hertel, 2008). The order of the tested leg (i.e., standing leg) and the three directions of measurement were determined randomly.
Three trials in each direction were made with each foot separately, timed at 10 seconds between each trial, and 20 seconds between different directions (Bouillon & Baker, 2011). The values of SEBT were determined with the average of the standardized scores (percentages) in each direction of the dominant and non-dominant leg (Coughlan et al., 2012). The test-retest reliability of the SEBT in healthy adults was previously established in a study, showing moderate to good reliability (ICC from .67 to .87) (Kinzey & Armstrong, 1998). It took about 10–15 minutes to perform the SEBT testing procedures.
One-leg stance (OLS)
The standing leg was decided by the participant, after trying to stand on one leg twice and the best result was used for analyses (Rolland et al., 2009). The participant was first asked to stand on one leg with eyes open and then with eyes closed to maintain each balance for up to 30 seconds. During the test, the participant placed their hands on the iliac crest and kept their elbows slightly bent with their legs at a 30-degree angle of hip and knee flexion. The time (seconds) was stopped when the participant lost balance or the foot was placed on the floor. The test-retest reliability of OLS was good (ICC = .88) in young people with mild to moderate intellectual disability (Blomqvist et al., 2012). It took about 3–5 minutes to perform the OLS test.
Functional reach test (FRT)
A horizontal ruler was fixed to the wall parallel to the ground at the participant’s shoulder height level. The participant stood at the dominant side close to the wall barefoot with their shoulder flexed at 90° with elbows and wrists straight. In this position, the middle finger position was marked as the starting position. The participant was then asked to keep the feet on the ground and bend forward to extend the arm to the maximum distance, without leaning to the wall. The distance (cm) measured from the starting position to the place the arm moved forward extensively was noted and the average of three trials of reach distance for analysis (Merchan-Baeza et al., 2014). The test-retest reliability of FRT was excellent in older adults using nursing homes either for those without cognitive impairment (ICC = .83) or with mild cognitive impairment (ICC = .87) (Ferreira et al., 2021). It took about 3–5 minutes to perform the FRT test.
Timed Up-and-Go test (TUG)
The participant sat in an armless chair with their back against the chair back, and was then asked to get up from the chair, walk three m, turn and walk back to sit on the chair to complete a continuous movement. The period was timed from the start sitting position to returning and sitting on the chair. The average of the two attempts (in seconds) was used for analysis (Blankevoort et al., 2013). The test-retest reliability of TUG has been reported as high in community-dwelling older people (ICC >.93). Moreover, the discriminant validity of TUG was excellent, which can distinguish individuals who were older, with falls history, and using a walking aid (Lin et al., 2004). It took about 3–5 minutes to perform the TUG test.
Tandem Walking test (TW)
The participants crossed their hands on the chest to eliminate the effects of arm balance (Jeon et al., 2007), and then walked 10 steps with heel-to-toe, with no gap between each step. The TW testing measured under eyes-open condition and then eyes-closed condition with one practice before each condition. The test result was the maximum number of correct consecutive steps up to 10 steps that the participant walked. The following situations were considered a failure: taking a side step, making a space between the feet, and opening the eyes in at eyes-closed condition. The Intra-class reliability (between-day) of TW was established in healthy adults (ICC from .71 to .78) (Koyama et al., 2018). It took about 5–10 minutes to perform the TW test.
Force platform
The force platform was utilized to establish concurrent validity with the five balance assessments battery. The force platform measures postural control and balance using center of pressure (COP) parameters, which has been considered reliable (ICC = .77–.99) and valid (r = .62–.88) in several populations (Blomqvist et al., 2012; Harro & Garascia, 2019; Li et al., 2016). Although limited studies have explored the psychometrics of the force platform for individuals with schizophrenia, it has been used to assess the balance function of individuals with schizophrenia (Kent et al., 2012).
A portable Kistler Force Plate (50 cm × 60 cm) (model 9260AA6, Kistler Instruments, Switzerland) was used, and the data was collected with frequency of 100 Hz. Participants stood with hands placed at the waist and had tested under four test conditions (i.e., feet placed at shoulder-width or feet close together with eyes open or closed). In each test condition, three trials of standing for a maximum of 30 seconds were given. Five COP parameters were recorded, including displacement speed, displacement area, anteroposterior displacement, left-right displacement, and total displacement. The mean of three trials of the COP parameters in each condition was used for analysis. It took about 40 minutes to perform the force platform test.
Statistical analysis
The data were analyzed with SPSS version 22.0. Chi-square test and independent t test were applied to compare the demographics between the fallers and non-fallers groups. The significance level was set at p value <.05.
The test-retest reliability was determined by the intraclass correlation coefficient (ICC), standard error of measurement (SEM), and minimal detectable change (MDC). The ICC was determined using a two-way mixed model with absolute agreement. Subsequently, according to the administration of specific balance measurement, ICC (3, K) values were reported for the SEBT, FRT, and TUG, while ICC (3, 1) values were reported for the OLS and TW (Koo & Li, 2016). The 95% confidence interval (CI) of an ICC value greater than .75 indicates good reliability (Koo & Li, 2016; Portney & Watkins, 2009). The SEM was used to evaluate the error of the test, which represents the degree of variation of the test and retest scores. A smaller SEM suggests higher reliability. The MDC refers to the minimum change difference between the test and retest scores that exceed the random error threshold (Portney & Watkins, 2009). Generally, an SEM% less than 10% is considered acceptable, and an MDC% less than 30% suggests the MDC value is acceptable (Smidt et al., 2002).
In terms of concurrent validity, considering the small samples (N = 26) and the non-normal distribution of the balance measurement data based on the Shapiro-Wilk normality test, Spearman’s rho (rho = rs) was used to calculate the correlation with force plate COP parameters. When evaluating the strength of concurrent validity, coefficient values of 0.5 or above suggest strong correlation, values between 0.3 and 0.5 suggest fair correlation, and values between 0.1 and 0.3 suggest poor correlation (Cohen, 1988).
Finally, discriminant validity was investigated with analysis of covariance (ANCOVA), controlling for gender, age, dosages of antipsychotic medications, and demographics with significant differences between fallers and non-fallers (i.e., vocational rehabilitation, CGI, and BPRS) to examine whether the balance measurement could discriminate between fallers and non-fallers.
Conventional ROC analysis was further performed to calculate the cutoff scores that yielded the highest combined sensitivity and specificity concerning distinguishing between the two groups. The discriminatory ability of the model was assessed using the area under the curves (AUC). The AUC value of 0.5 is considered the point of nondiscrimination, the value of 1.0 represents a test with perfect discrimination (Hoo et al., 2017).
Results
Participants
Participants’ Demographics.
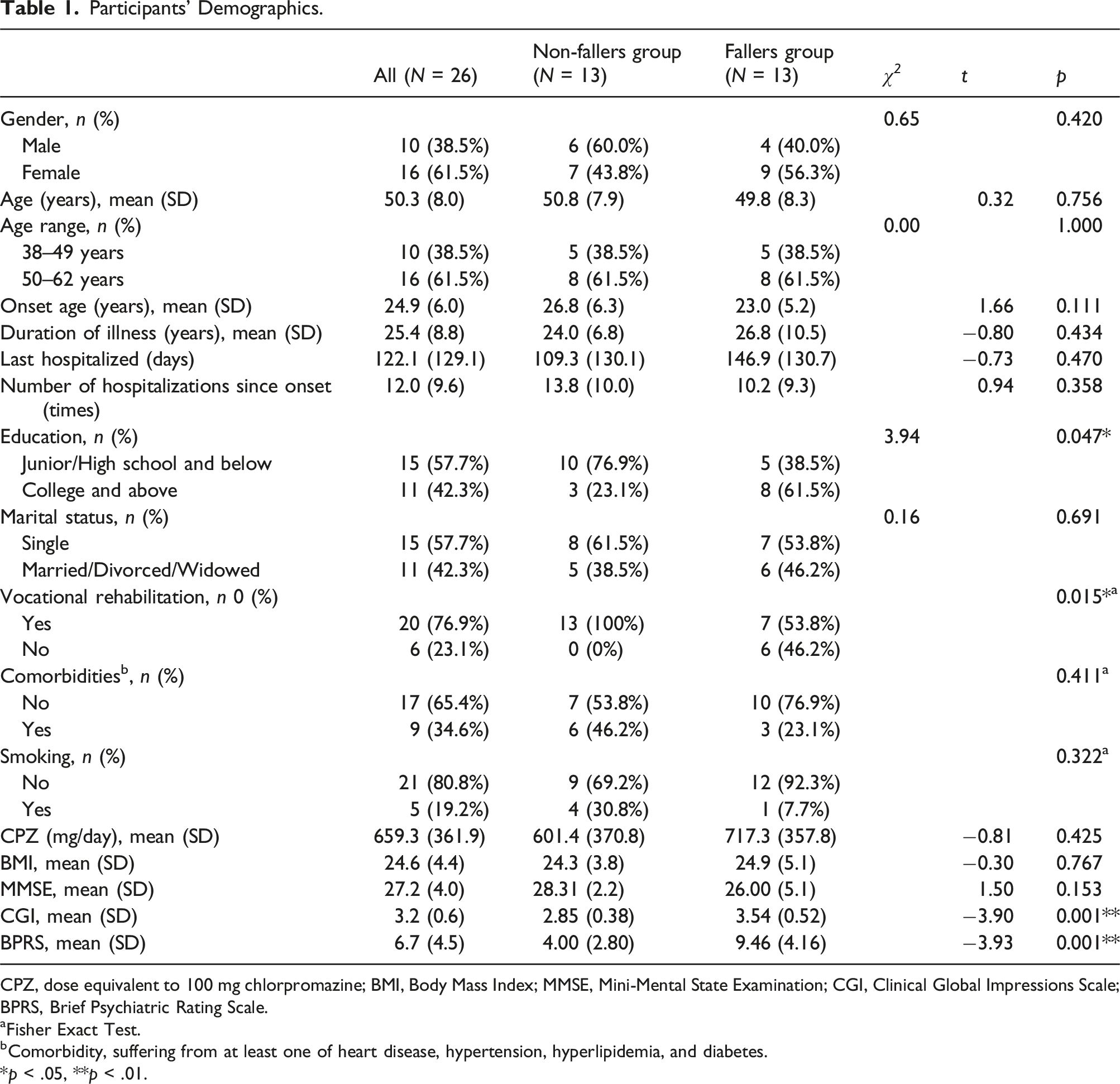
CPZ, dose equivalent to 100 mg chlorpromazine; BMI, Body Mass Index; MMSE, Mini-Mental State Examination; CGI, Clinical Global Impressions Scale; BPRS, Brief Psychiatric Rating Scale.
aFisher Exact Test.
bComorbidity, suffering from at least one of heart disease, hypertension, hyperlipidemia, and diabetes.
*p < .05, **p < .01.
Test-retest reliability
Test-Retest Reliability of Five Balance Assessments.
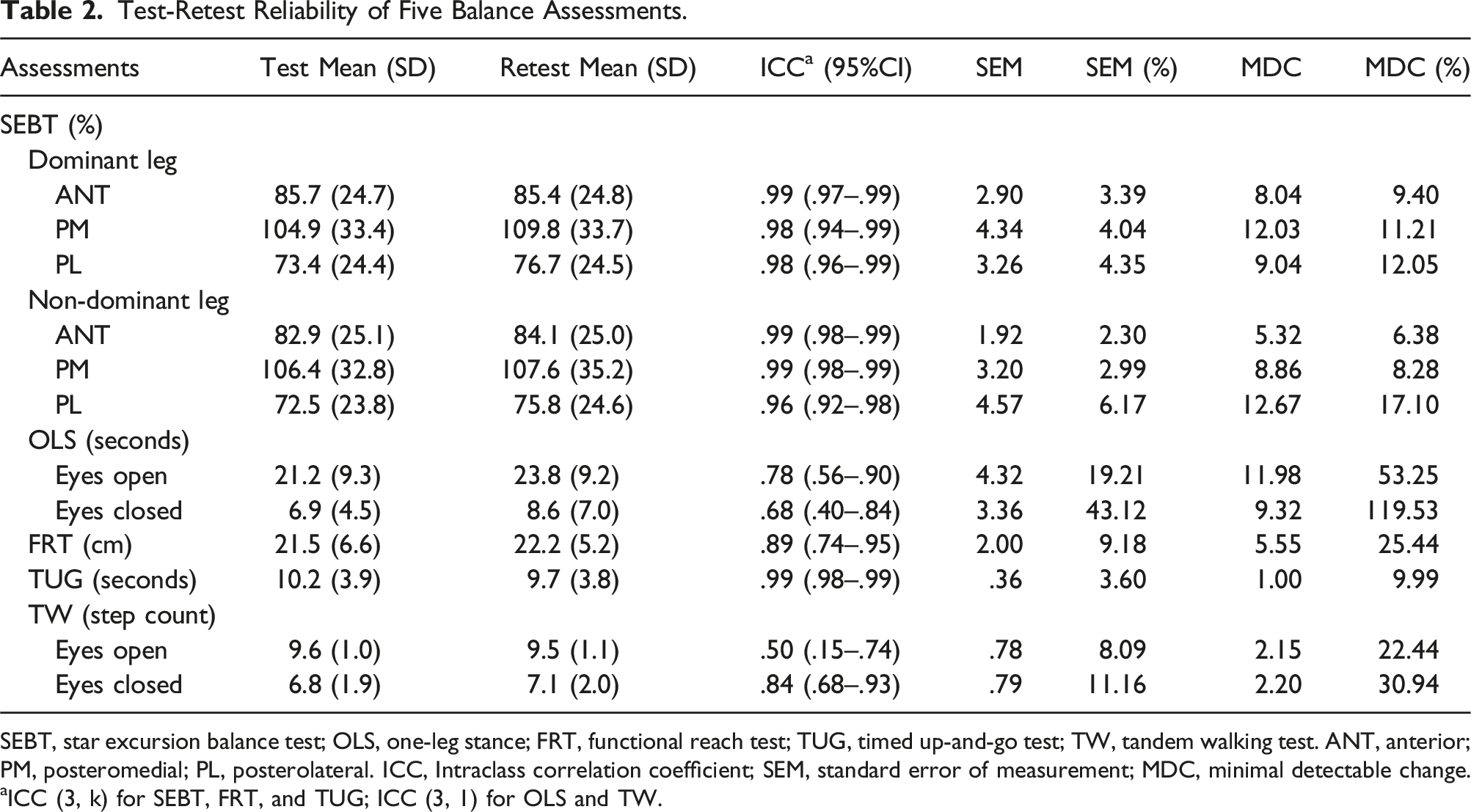
SEBT, star excursion balance test; OLS, one-leg stance; FRT, functional reach test; TUG, timed up-and-go test; TW, tandem walking test. ANT, anterior; PM, posteromedial; PL, posterolateral. ICC, Intraclass correlation coefficient; SEM, standard error of measurement; MDC, minimal detectable change.
aICC (3, k) for SEBT, FRT, and TUG; ICC (3, 1) for OLS and TW.
Concurrent validity
Concurrent Validity of SEBT With Force Plate COP Parameters (Spearman’s Rho, rho = r s ) (N = 26).

SEBT, star excursion balance test; COP, center of pressure. DS, displacement speed; DA, displacement area; APD, anteroposterior displacement, LRD; left-right displacement; TD, total displacement. ANT, anterior; PM, posteromedial; PL, posterolateral. *p < .05, **p < .01.
Concurrent Validity of the OLS, FRT, TUG & TW With Force Plate COP Parameters (Spearman’s Rho, rho = rs) (N = 26).
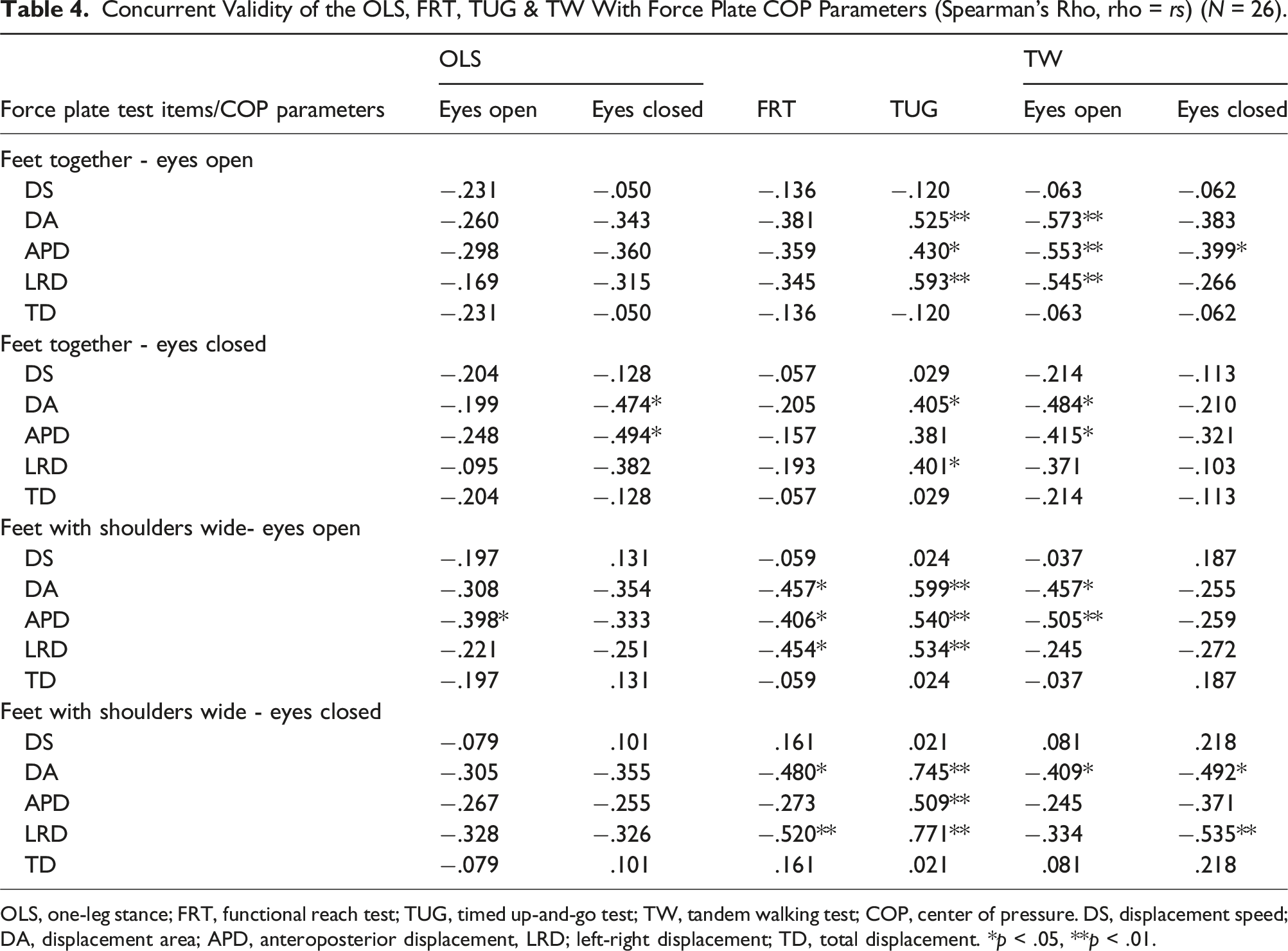
OLS, one-leg stance; FRT, functional reach test; TUG, timed up-and-go test; TW, tandem walking test; COP, center of pressure. DS, displacement speed; DA, displacement area; APD, anteroposterior displacement, LRD; left-right displacement; TD, total displacement. *p < .05, **p < .01.
Discriminant validity
Discriminant Validity Analysis Using Analysis of Covariance (ANCOVA) on Test Scores at the First Visit (N = 26).
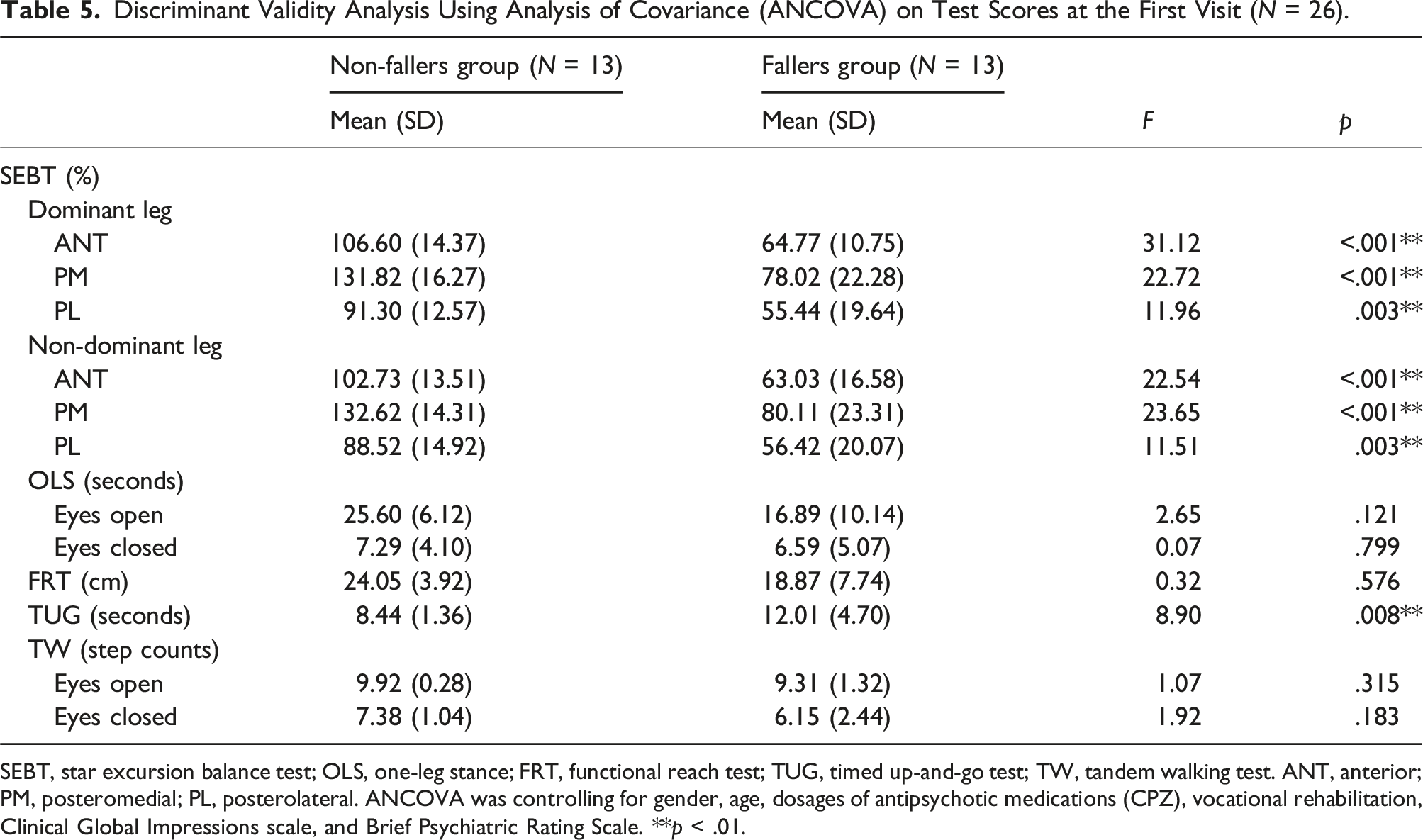
SEBT, star excursion balance test; OLS, one-leg stance; FRT, functional reach test; TUG, timed up-and-go test; TW, tandem walking test. ANT, anterior; PM, posteromedial; PL, posterolateral. ANCOVA was controlling for gender, age, dosages of antipsychotic medications (CPZ), vocational rehabilitation, Clinical Global Impressions scale, and Brief Psychiatric Rating Scale. **p < .01.
Sensitivity and specificity
Cutoff Score, Sensitivity, Specificity and AUC of the Five Balance Assessments (N = 26).
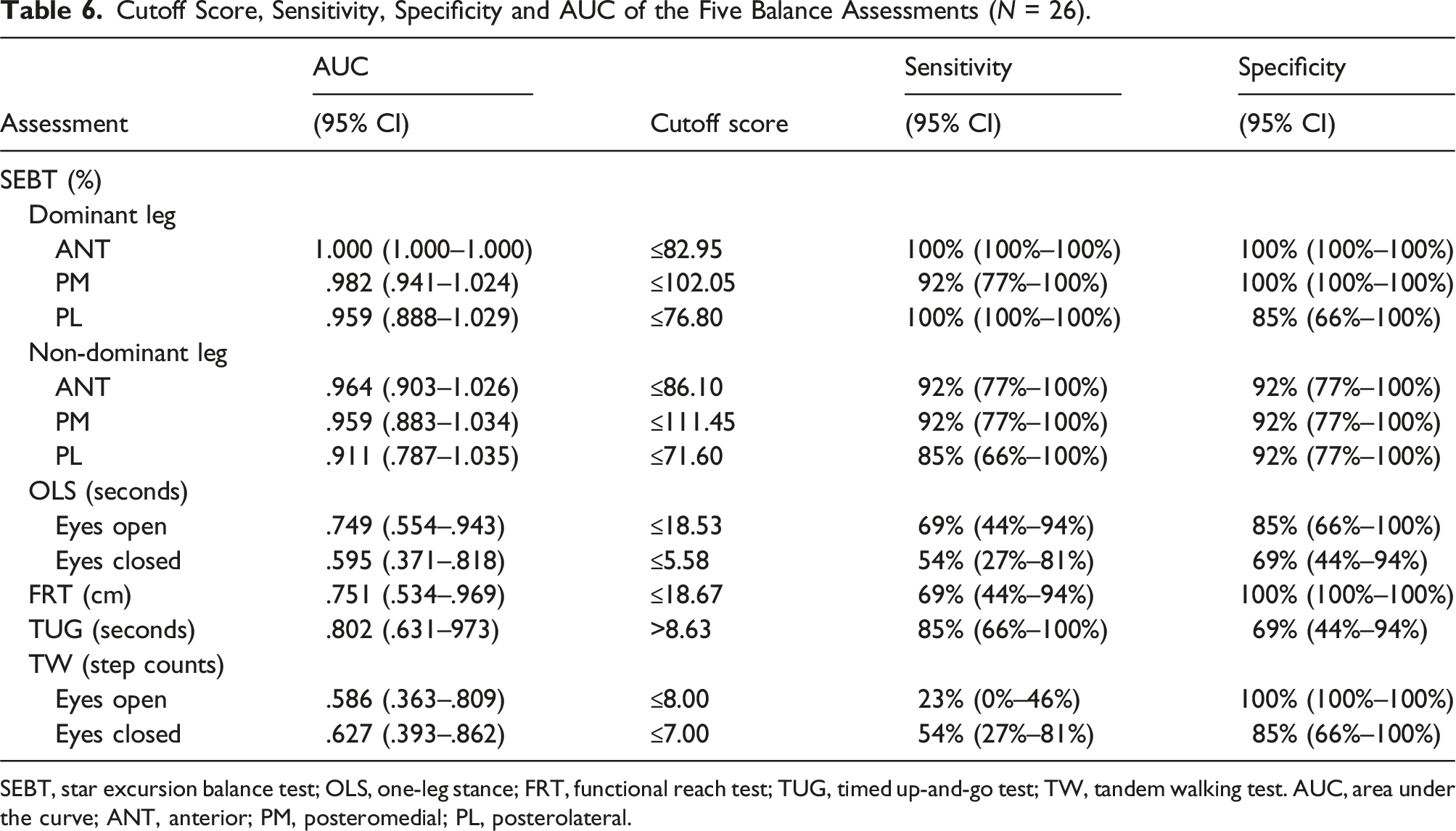
SEBT, star excursion balance test; OLS, one-leg stance; FRT, functional reach test; TUG, timed up-and-go test; TW, tandem walking test. AUC, area under the curve; ANT, anterior; PM, posteromedial; PL, posterolateral.
Discussion
To the best of our knowledge, limited studies have investigated the psychometrics of common balance field tests in individuals with schizophrenia. Only one study has explored the reliability of the Flamingo balance (i.e., OLS posture) in the Eurofit test battery in schizophrenia (Vancampfort et al., 2012). No related studies have investigated the reliability and validity of the other four tested balance assessments for individuals with schizophrenia. The findings of this study could guide clinicians and researchers in choosing appropriate balance assessments for individuals with schizophrenia.
Test-retest reliability
The results suggest that the test-retest reliability of the SEBT and TUG is good. The good test-retest reliability for the SEBT in this study is consistent with previous studies of SEBT in healthy young adults (Kinzey & Armstrong, 1998). Namely, the test-retest reliability of the SEBT is good not only for healthy young populations but for middle-aged adults with schizophrenia as well, according to the present study.
The ICC of OLS under eyes open in this study was .78, which is similar with the previous studies on young people with mild to moderate intellectual disabilities (Blomqvist et al., 2012). However, Vancampfort et al. (2012) explored the reliability of the OLS among the Eurofit test battery used for schizophrenia, and found relatively lower (ICC = .72) test-retest reliability. The different test methods between our and Vancampfort’s study might account for the discrepancy of the test-retest reliability. The balance test method in their study (Vancampfort et al., 2012) (i.e., Flamingo balance) was the number of attempts required by the participant to achieve 30 seconds in balance on their preferred foot. The study also reported 26% of the participants were unable to complete the test. In contrast, the OLS in the present study measured the best performance time in maintaining balance while standing. All participants could perform the OLS test, which might have resulted in better test-retest reliability.
The ICC for the FRT was .89 with 95% CI of .74–.95, indicating approaching good test-retest reliability for people with schizophrenia, which is consistent with a previous study of older adults in nursing home settings (Ferreira et al., 2021). Although another study pointed out that the test-retest reliability of FRT was moderate for individuals with Parkinson’s disease at an average age of 71 years (ICC = .73) (Steffen & Seney, 2008). This lower test-retest reliability might be related to the older age of the participants studied. Therefore, when the FRT is used in older adults with schizophrenia, the quality of the test-retest reliability should be considered with caution. The test-retest reliability of TUG in this study was good. Previous studies supported similar findings for both elderly (Lin et al., 2004), and dementia patients (Blankevoort et al., 2013), suggesting good test-retest reliability of the TUG for several clinical groups.
In contrast, the test-retest reliability of the TW was poor to moderate under eyes open (ICC = .50; 95% CI = .15–.74), while it was better under eyes closed (ICC = .84; 95% CI = .68–.93). The lower ICC of TW (eyes open) might be related to the difficulty of performing this measurement when the base of support is compromised in tandem gaits. While the ICC of TW under eyes-closed seemed better than the eyes-open condition, it should be interpreted with caution. The better ICC might be due to the poor performance scores in both test and retest sessions when the visual input cannot be relied on. More research is needed to examine the clinical suitability of the TW in individuals with schizophrenia.
The SEM% and MDC% of SEBT, FRT, TUG, and TW (eyes open) are less than the reference values of 10% and 30% respectively, indicating that the error values of the four balance field tests are acceptable. A previous study recruited adults with moderate intellectual disability and found similar results of FRT and TUG on SEM% and MDC% to our study (Blomqvist et al., 2012). In contrast, the SEM% and MDC% of OLS under eyes open and closed are both larger than the reference value, suggesting the OLS tends to result in a large measurement error. The relatively poor stability and reliability of OLS should be applied with caution particularly when used as an outcome measure for intervention studies for schizophrenia.
Concurrent validity
Among the five balance tests, the SEBT and TUG demonstrated good concurrent validity, showing a higher percentage of statistically significant strong and fair correlation coefficients (i.e., >0.3) with the COP parameters of the force plate. Conversely, there was less correlation and lower correlation levels for the OLS with eyes open, TW eyes closed, and FRT, with few items reaching significant respectively, and the rho value fell mostly between very little or no correlation to the fair level.
A study of young people with intellectual disabilities found a significant moderate to strong correlation between the force plate parameters with the OLS at eyes open, but small or no correlation with the TUG and FRT (Blomqvist et al., 2012). In other words, the concurrent validity of FRT with the force plate is consistent with our study, but inconsistent in comparison with the OLS and TUG results. The discrepancy might be caused by the different test postures on force plate in the two studies. The better concurrent validity of the OLS in Blomqvist et al. (2012) study could be related to a similar testing posture (i.e., one-leg standing on the force plate).
Our results also found that the COP’s displacement speed and total displacement parameters did not reach significant correlation with all five balance tests. This result might be inferred from the stationary standing posture on the force plate to detect the degree of the swing of the body’s center of gravity as an indicator of balance ability. In such measurement, no obvious movement changes occurred on the force plate; thus, the displacement speed and total displacement parameters did not significantly occur.
Discriminant validity
Among all five balance tests studied, the SEBT and TUG demonstrated discriminant validity in distinguishing between individuals with schizophrenia with and without a history of falls. Previous studies have confirmed construct validity of the SEBT (Zhuang et al., 2014) and TUG (Shumway-Cook et al., 2000) in fall-risk assessment for the elderly. However, the non-significant discriminant validity of TW may be due to the poor performance of individuals with schizophrenia in this test (Jeon et al., 2007). The numbers of steps completed in the TW under both conditions were less than 10 steps, leading to difficulties in distinguishing differences in performance between the two groups.
Based on the ROC analysis, the cutoff score for each assessment was established along with sensitivity and specificity. Generally, the AUC is larger (i.e., >.8) for the SEBT and TUG, suggesting a better performance to distinguish fallers from non-fallers in individuals with schizophrenia. While the AUC is relatively lower for the OLS, FRT, and TW, the cutoff score of specific assessment for people with schizophrenia identified in the present study is similar to other populations, including OLS (eyes open) for the elderly (Seichi et al., 2014), FRT for the adults with Parkinson disease (Brusse et al., 2005), and TW for adult patients with vestibular disorders (Cohen et al., 2018). The cutoff score for the balance assessment provided in the present study can be used to identify the group with risks of falls in this clinical population.
Our study shows significant difference in psychiatric symptoms severity between the faller and non-faller groups. Previous studies have pointed out that balance impairment in patients with schizophrenia is associated with increased symptom severity (Kent et al., 2012), consistent with the findings of this study. Furthermore, one of future studies is to make use of the five balance assessments battery to predict actual falls and find out the factors that contribute to falls in individuals with schizophrenia (Fong et al., 2023).
Investigation on the possible benefits of exercise for individuals with schizophrenia is one key essential research question in this field (Vancampfort et al., 2016). While health benefits of exercise for schizophrenia have been documented, it is important to note that few studies have identified balance function and fall risk as key outcome measures for intervention (Firth et al., 2015). Future research is warranted to develop evidence-based balance training programs for this clinical population. Our study results provide suggestions on selecting the balance function assessments.
Limitations
Firstly, the study sample size was small, which might limit the generalizability of the results. Secondly, participants were characterized by their chronic stage and middle age, as well as not excluding conditions that may prevent them from safely performing these balancing assessments, such as acute metabolic syndrome, so study results should be interpreted with caution. Future research is suggested to recruit more participants with different demographics to confirm the research results. Furthermore, conducting future research with a larger sample size to investigate reference values for each specific balance measure would be beneficial. Thirdly, the concurrent validity was examined with the force plate which only provides the static balance. The concurrent validity of the dynamic balance assessments should be interpreted with caution and future studies using a dynamic balance force plate are suggested. Finally, notable differences in demographics, that is, vocational rehabilitation status, and psychiatric symptom severity measured by the CGI and BPRS, were observed between the faller and non-faller groups. These differences may influence the interpretation of discriminant validity of studied balance assessments.
Conclusion
Among the five balance assessments battery studied, the SEBT and TUG demonstrate superior reliability and validity in examining the balance functions in individuals with schizophrenia. Considering the practicality of conducting these assessments, the TUG is recommended for clinical professionals due to its relatively straightforward testing procedures. Additionally, the SEBT and TUG demonstrated a larger AUC, indicating better ability to identify fall risks in this population.
Footnotes
Acknowledgements
The authors would like to thank all participants who have participated in this study. We would further like to thank the workers of the recruited sites for their assistance in recruiting the participants.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was partially supported by the grant from the Tsyr-Huey Mental Hospital.