
Abstract
Against the background of a lack of screening instruments for measuring depressive symptoms in Colombian adolescents and preadolescents, this study aims to establish the internal consistency reliability, component structure and the concurrent and discriminant validity of the Kutcher Adolescent Depression Six-Item Scale (KADS-6) among preadolescent school students in Sincelejo, Colombia. Participated 710 youth (10.8 years of age ± .75 years) divided into two groups to cross-validate analyses that were undertaken to determine the internal consistency reliability, as well as the concurrent and discriminant validity, of the KADS-6 among preadolescents. Results show that over 95% of the sample did not report problems understanding any of the items on the KADS-6. The KADS-6 had acceptable levels of internal consistency reliability, concurrent and discriminant validity and was unidimensional. In conclusion, The KADS-6 is well understood by Colombian preadolescents and has adequate psychometric properties in adolescents, rendering it acceptable for use with Colombian preadolescents.
Keywords
Introduction
Major Depressive Disorder (MDD) is one of the most prevalent mental disorders and one of the most important causes of disability (Klaufus, et al., 2022; Nazari et al., 2022). It is characterized by periods (of at least 2 weeks) in which individuals display substantial changes in their mood, cognition, and motivation (APA, 2013).
Among children and adolescents, the disorder presents differently with adolescents more often reporting symptoms of irritability, than depressed mood. The prevalence of depression among adolescents has been reported as 5.9% for girls, 4.6% for boys, and 5.6% overall, roughly twice the rate observed among children (2.8%).
Unfortunately, there are few screening measures for depressive symptoms among Colombian youth which are correctly interpreted, reliable and valid (Kocalevent, et al., 2014; Ministerio de Salud y Protección Social, 2013). This hampers the ability to recognize depression and to intervene appropriately to prevent or minimize negative outcomes. The screening measures that are currently being used in Colombia with children and adolescents include the Children’s Depression Inventory (Segura Camacho et al., 2010), the Zung Self-Rating Depression Scale (Cogollo, et al., 2006), the Composite International Diagnostic Interview (WHO, et al., 2011), and the CES-D 10 (Pineda-Roa, et al., 2019; Villalobos-Galvis & Ortiz-Delgado, 2012). While these measures have been used in Colombia they are associated with many limitations including the fact that many of them (CDI, CES-D 10, Zung, CIDI) were adapted from adult measures and hence do not adequately capture how depression is manifested and experienced in children and adolescents (Cogollo, et al., 2006; Pineda-Roa et al., 2019; Villalobos-Galvis & Ortiz-Delgado, 2012). They also tend to require extensive training (CIDI) and are often expensive to acquire or use (CDI, CIDI). In addition, The CDI can only be interpreted by staff who have extensive professional training. The KADS-6 does not have these limitations as it was designed for use with children and adolescents, is inexpensive to acquire and use, does not require extensive professional training, and has been shown to be valid and reliable across a wide range of languages and cultures (Lowe, et al., 2018; Quintão, et al., 2015). The current study seeks to examine the internal consistency reliability, component structure and validity of the KADS-6 among Colombian children and adolescents.
Method
Participants
The participants for the study consisted of seven hundred and ten (N = 710) Grade 5 students attending a cross-section of government-funded public and privately-funded elementary schools in Sincelejo, Colombia. Seventeen schools were initially randomly selected to take part in the study. The project was presented to school principals and their academic staff. From the initial 17 schools selected to take part, 13 schools (76.5%) agreed to collaborate. Within each school which took part, all Grade 5 classrooms in each school were sampled. No compensation for participation was given to schools, students or parents. From a total of 861 students invited to participate, 710 (82.5%) agreed to collaborate handing over signed informed assent and informed consent forms.
Approximately three quarters of the students (539 students or 75.9% of the sample) attended public schools and 89 pupils attended private schools (11.4% missing). Just over half (n = 422, 59.4%) of the sample were males. Participants were on average 10.8 years of age (±0.75 years) and ranged in age from 8 to 13 years. Most students had parents whose highest level of education was secondary school or less (53.9%) and who worked in manual or skilled labour jobs (76.6%).
To be included in the sample, students needed to be present at school on the day of data collection; their parents must have provided their written consent to take part in the study and students needed provide their written assent. The ethics committee of the Corporación Universitaria del Caribe (CECAR) provided their approval to conduct this study.
Measures
Kutcher Adolescent Depression Scale-6 (KADS-6)
The KADS was created to address the need for a depression screening instrument for adolescents (Brooks, et al., 2003; LeBlanc et al., 2002). The six-item version was created from the original 11-item measure to serve as a brief screening instrument for Major Depressive Disorder among adolescents (Kutcher & Chehil, 2008). The six-item version of the scale measures four affective symptoms, one somatic symptom of depression and one cognitive symptom of depression among students, 12–17 years of age. Respondents record their responses to each question using a 4–point Likert scale (0-Hardly ever, 1-Much of the time, 2-Most of the time, 3-All of the time). A score of six (6) or more is suggestive of a possible diagnosis of depression for that respondent, and requires further assessment by a clinician (Kutcher & Chehil, 2008). The six-item version of KADS has good sensitivity (92%) and specificity (71%) (LeBlanc, et al., 2002). It has been validated in different languages, including Spanish, Portuguese, Persian and Polish and has been used extensively across many countries in the world (Mojs, et al., 2015; Quintão, et al., 2015).
The applicability and interpretability of the KADS-6 for use with Colombian adolescents and preadolescents was examined using a four-step procedure. The first step involved an expert review of measures of depression used in Colombia. The second step involved the translation of the KADS-6 into Colombian Spanish and the back-translation of the KADS-6 into English to examine the quality and fidelity of translation. The third step involved an examination of the translated KADS-6 by expert judges, to provide their opinions as to how well the overall measure and individual items of the KADS-6 might be in measuring depressive symptoms among Colombian children and youth. The fourth step involved a think-aloud interview to examine how Colombian pre-adolescents understood each item and based on their feedback, the carrying out of modifications to items 1 and 6 of the instrument.
Adolescent Depression Rating Scale (ADRS)
The ADRS is a 10-item measure of depressive symptoms designed for adolescents (Revah-Levy et al., 2007). Reponses for each item is indicated as either true or false. The ADRS has been found to have acceptable levels of internal consistency reliability (α = .74–.79) as well as good concurrent validity, as shown by large correlations with the Hamilton Depression Rating Scale (.56), the Beck Depression Inventory-II (.82) and the Clinical Global Impression — Severity Scale (.52).
Revised Children’s Anxiety and Depression Scale (RCADS)
The Revised Children’s Anxiety and Depression Scale (RCADS) is a 47-item self-report questionnaire which measures symptoms of anxiety and major depressive disorder (Chorpita, et al., 2015). Responses are scored on a 4-point Likert-scale from 0 to 3 (0 = Never, 1 = Sometimes, 2 = Often, and 3 = Always). The 10-item major depression disorder subscale has an internal consistency reliability of 0.79 for school based samples of children 6–18 years of age (Ebesutani et al., 2012) while the 6 item measure of generalized anxiety had an internal consistency reliability of 0.84 (Kösters, et al., 2015).
Visual Analogue Scale — Anxiety (VAS-Anxiety scale)
The Visual Analogue Scale - Anxiety (VAS-Anxiety) is a single question which asks respondents to indicate their level of anxiety using a 100-mm horizontal line. Participants completed one version of the measure according to their current feelings of anxiety (state anxiety) and another according to their levels of anxiety over the past 6 months (trait anxiety). The VAS - Anxiety scale is a self-rated measure, with the poles labelled “no anxiety or fear” on zero end point and, “worst possible anxiety or fear” on the 100-end point for both versions of the measure (Aitken, 1969).
Procedure
The Colombian Spanish version of the KADS- 6 was administered to a sample of 710 Grade 5 students from 13 elementary schools across Sincelejo. Participants were informed that their participation was completely voluntary, and they could withdraw from the project at any time. Questionnaires were distributed and students were given time to complete the package of measures. Completed questionnaires were returned to one of the investigators or a research assistant at the end of the session.
Statistical Analysis
Before conducting any formal statistical analyses, missing values were substituted, using an expectation maximization procedure for missing responses on the KADS- 6, RCADS – MDDS, ADRS, VAS-Trait Anxiety (VAS-TA) and VAS –State Anxiety (VAS-SA) items. Little’s test following the expectation maximization procedure was significant (Chi-Square = 21,280.42, DF = 20,756, Sig. = .005) indicating that the data were not missing completely at random. An inspection of results of the EM procedure indicated that all of the missing data occurred for the RCADS – MDDS items, with missing values for individual items ranging from 33.8% and 67.5%. Despite the high levels of missing data for the RCADS – MDDS items, a comparison of the non-estimated and the estimated values revealed that they were close in size, with the differences ranging from 0.006 to 0.289 points on a 5-point scale (Mean difference = .082). Following the substitution of missing values, the sample was then split into two halves using the study identification numbers (those with odd vs. even study identification numbers) in order to obtain two relatively comparable groups (n1 = 355 and n2 = 355). The first half of the sample served to establish the psychometric properties of the KADS-6, while the second half served to cross-validate the initial findings.
The process used to examine the psychometric properties of the KADS - 6 involved first examining the internal consistency reliability of the KADS - 6 (Cronbach L J, 1951). Following this, the concurrent validity of the KADS - 6 was examined using the RCADS - Major Depression sub-scale and the ADRS. The discriminant validity of the KADS - 6 was estimated using the VAS - Trait Anxiety and the VAS - State Anxiety measures. A principal components analysis (PCA) of the KADS - 6 was conducted to examine the dimensional structure of the KADS-6.
The analyses were then repeated in order to cross-validate the psychometric properties of the KADS - 6 using the second half of the sample. This procedure was intended to enhance the strength of the validation of the KADS - 6 (de Rooij et al., 2020).
Results
Validation Sample
Reliability and Validity
A total of 355 children, aged 8–13 years (146 girls and 209 boys) were included in the initial analysis of the psychometric properties of the Colombian version of the KADS-6. The internal consistency reliability of the KADS-6, the ADRS and the RCADS were .72, .71, and .78 respectively.
Analyses of the validity of the KADS-6 suggested that the instrument had an acceptable degree of concurrent validity. Scores on the KADS-6 were correlated .51 with the major depression disorder subscale of the RCADS-MDD and .58 with the ADRS, indicating a moderate degree of concurrent validity. The KADS-6 also demonstrated discriminant validity by weak correlations with the RCADS-Anxiety (r = .15), as well as with the visual analogue scales for state and trait anxiety (VAS-S and VAS-T, r = .21 and .23, respectively).
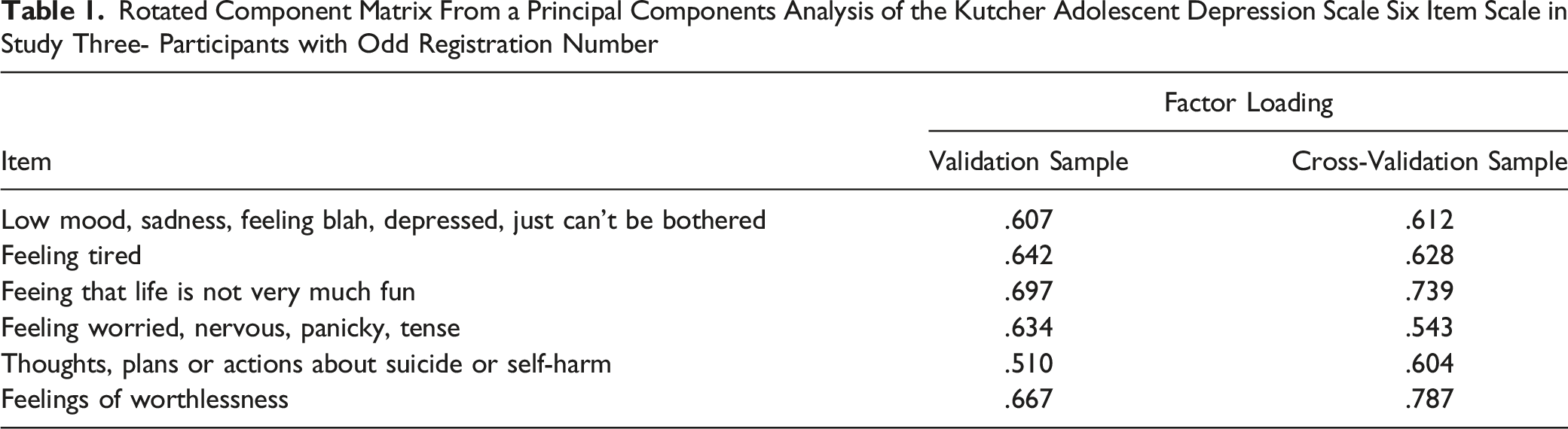
Structure of the KADS-6
Rotated Component Matrix From a Principal Components Analysis of the Kutcher Adolescent Depression Scale Six Item Scale in Study Three- Participants with Odd Registration Number
Cross Validation Sample
The psychometric properties of the KADS-6 were examined using the cross-validation sample of 355 children, aged 8–13 years (142 girls and 213 boys). Consistent with the validation sample, the internal consistency reliability of the KADS-6, the ADRS and the RCADS were .69, .63, and .73 respectively. Further, consistent with the validation sample the KADS-6 correlated with the RCADS – MDDS (r = .47) and with the ADRS (r = .55) providing evidence for the concurrent validity with the other depression measures. The KADS-6 correlated weakly with scores on the RCADS-Anxiety (r = .10) and with the VAS-SA and VAS-TA scales (r = .19 and .17 respectively) providing evidence for the discriminant validity of the KADS-6. Similar to the validation sample, the principal components analysis of the KADS-6 found one component underlay all of the items with all six items loading on this single component. This component accounted for 42.5% of the total variability underlying all six items.
Discussion
In our Colombian sample, the internal consistency reliability of KADS-6 were slightly lower (α = .72 validation and .69 cross-validation) than those found in other studies (Mojs, et al., 2015; Quintão, et al., 2015). However, those other studies used youth who were much older (12–24 years of age) than those who participated in our study (8–13 years of age). For instance, Quintão, et al. (2015) using a Portuguese sample of 12–18 year olds found internal consistency reliabilities ranging from .74, for a clinical sample to .80 in a school sample. Mojs, et al. (2015) found a Cronbach’s Alpha of .84 using a sample of Polish medical students 18–24 years of age.
Consistent with previous research (Mojs et al., 2015; Lowe et al., 2018; Quintão et al., 2015), one clear component emerged from the principal components analysis of the KADS-6. This component included all six items of the measure assessing the three key elements of depressive symptoms – affective, cognitive, and somatic. This broad-based inclusion of the key elements of depressive symptoms may make the KADS-6 a good measure to identify young people who may be showing symptoms consistent with MDD.
Similar to research using Portuguese and Caribbean samples (Lowe, et al., 2018; Quintão, et al., 2015), scores on the KADS-6 were moderately correlated with the RCADS and ADRS depression scales and weakly correlated with the measures of anxiety. This pattern of findings suggests that among Colombia pre-adolescent youth, the KADS-6 shows a moderate degree of concurrent and discriminant validity.
Conclusion
The results of this research suggest that the KADS-6 has acceptable psychometric properties for Colombian pre-adolescent youth and that it may be used in studies of depressive symptoms within this population.
Supplemental Material
Supplemental Material - The Validation of the Kutcher Adolescent Depression 6-Item Scale in a Sample of Colombian Preadolescents and Adolescents
Supplemental Material for The Validation of the Kutcher Adolescent Depression 6-Item Scale in a Sample of Colombian Preadolescents and Adolescents by Kelly Romero-Acosta, Garth E. Lipps, Gillian A. Lowe, Roger Gibson and Andrés Ramirez-Giraldo in Evaluation & the Health Professions
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.