
Abstract
Introduction
Currently studies indicate the need to incorporate the user`s perspective in the testing of new assistive technologies. The objective of this paper is to test a baropodometric insole prototype for monitoring and treatment weight-bearing asymmetry, according to the Participatory Design.
Methods
We used a qualitative case study approach during the testing phase of the baropodometric insole prototype. The focus group approach addressed topics related to the experience and accessibility of the potential user in conjunction with professionals, researchers, and physiotherapy students. Facilitators, barriers, and requirements for the device were collected through audio recordings of the discussions during and after prototype testing.
Results
Key steps in the prototype testing process were divided into (1) Test of the prototype according to the Participatory Design, divided into Who, When, How, and Why the potential user was involved in the study; and (2) Facilitators, barriers and requirements to improve the prototype.
Conclusions
The baropodometric insole prototype can be seen as a promising device for monitoring and treating weight-bearing asymmetry.
Introduction
The brain and machine interface allows technological devices to facilitate potential sensorimotor learning mechanisms through neuroplasticity (Oweiss & Badreldin, 2015). The inclusion of people with disabilities in the innovation process necessitates considering user perception, addressing ableism barriers, and addressing limitations in knowledge to enhance accessibility between users, their context, and developed technology (DeFalco et al., 2022). As a result, device rejection rates increase, reflecting the small insertion of technological devices in the market (Greenhalgh et al., 2016). The construction of a participatory method that includes the users is especially important for chronic non-communicable diseases, as they require devices that can compensate for mental deficiencies, communication barriers, and motor skills impairment that, in most cases, are permanent (Powell et al., 2016; Winstein et al., 2016).
Stroke is the third leading cause of death and disability in the world, and it is responsible for 56% of somatosensory impairment of the lower limbs in its chronic phase (GBD 2019 Stroke Collaborators, 2021; Gorst et al., 2019). Weight-bearing asymmetry is a common impairment after stroke associated with a higher risk of musculoskeletal injuries (Wang & Newell, 2012), functional impairments related to gait, and balance (Gorst et al., 2019). These deficits result in an excessive cost of energy during gait (Aqueveque et al., 2017), increased risk of falls (Sackley, 1991), and, consequently, limited mobility and restricted social participation within the community (Aqueveque et al., 2017). Lastly, the awareness and self-adjusting of the weight-bearing asymmetry are impaired due to somatosensory deficits in individuals with hemiparesis (Crosby et al., 2021).
Generally, individuals after a stroke have a more common pattern of overload in the non-paretic lower limb (Birnbaum et al., 2021). Evaluation by posturography has shown to be an instrument with good reliability and reproducibility to quantify body weight distribution and displacement of the center of mass (Genthon et al., 2008). Although posturography is reliable for measuring body weight distribution, it is not practical for clinical use. Conventional balance assessment and quantitative gait measures have low reliability and are not adequate to assess weight-bearing asymmetry (Inazawa et al., 2014; Kamphuis, de Kam, Geurts & Weerdesteyn, 2017; Martins et al., 2011; Mohan et al., 2021). Task-specific interventions, such as walking, sitting, standing, and sensorimotor stimulation, can correct weight-bearing asymmetry, but assistive technology devices can also help (Lin et al., 2018; Liu et al., 2016; Sheikh et al., 2016).
Previously, the project’s development phase described the system design and the testing with healthy individuals to find the ideal positioning of the sensors and the calibration procedure for the baropodometric insoles (Inazawa et al., 2014). Based on this study, the authors recommend that testing be initiated with individuals with weight-bearing asymmetry. In this way, future research should obtain the user’s perception of the device’s functionality. Now, in the testing phase, we intend to integrate experiences and insights from potential users and developers. Participatory Design method involves users and developers in testing, enabling adaptive technology, improving usability and accessibility, and promoting inclusive and innovative solutions for people with disabilities (Cook, 2008; Spinuzzi, 2005). Participatory design is described in the development of new technologies in clinical and home settings for people with disabilities after stroke. Kjörk et al. (2022) through a workshop composed of focus group and potential users, described the process of developing a device for home care in post-stroke patients. The authors concluded that the integration between researchers and potential users resulted in a tool considered easy to use. Wang et al. (2022), developed and tested a portable device for muscle recruitment and to develop muscle strength and endurance. Thus, with the prototype developed, the main functions of the device were achieved, the participants accepted user participatory design, and the authors recommended that the approach be adapted for all rehabilitation and assistive technology development.
Our study aims to: (1) To investigate a baropodometric insole prototype for monitoring and treatment of weight-bearing asymmetry and (2) To visualize the facilitators, barriers, and requirements for the technology to be tested.
Methods
Study design
This study was conducted during the testing phase. We used a qualitative case study approach based on the Participatory Design. The testing phase of the baropodometric insole prototype was carried out at the outpatient clinic of the physical therapy department of a university. The Standards for Reporting Qualitative Research checklist was used to ensure transparency and quality of the study (O'Brien et al., 2014).
The prototype equipment consists of a pair of baropodometric insoles that monitor weight-bearing asymmetry using two layers of plastic material and pressure sensors to adapt to different types of footwear. The baropodometric insoles consist of control boards with microcontrollers and a vibration system, providing tactile feedback to the user’s hemiparetic lower limb. They include pressure sensors to detect weight asymmetry, enabling real-time monitoring and reducing functional limitations and injury risks (Figure 1) (Inazawa et al., 2014). Baropodometric insoles facilitate motor training and the prescription of exercises for gait, balance, and transfers, promoting mobility and physical activity. In addition, these devices help individuals achieve rehabilitation goals in home and community settings, increasing their ability to maintain independence in activities of daily living (Martins et al., 2011). Components of the prototype baropodometric insole. A Baropodometric insole prototype. B Static position to determine the limit of symmetry between the affected and unaffected hemibody. C Mobile health application developed to diagnosis and monitoring weight-bearing asymmetry.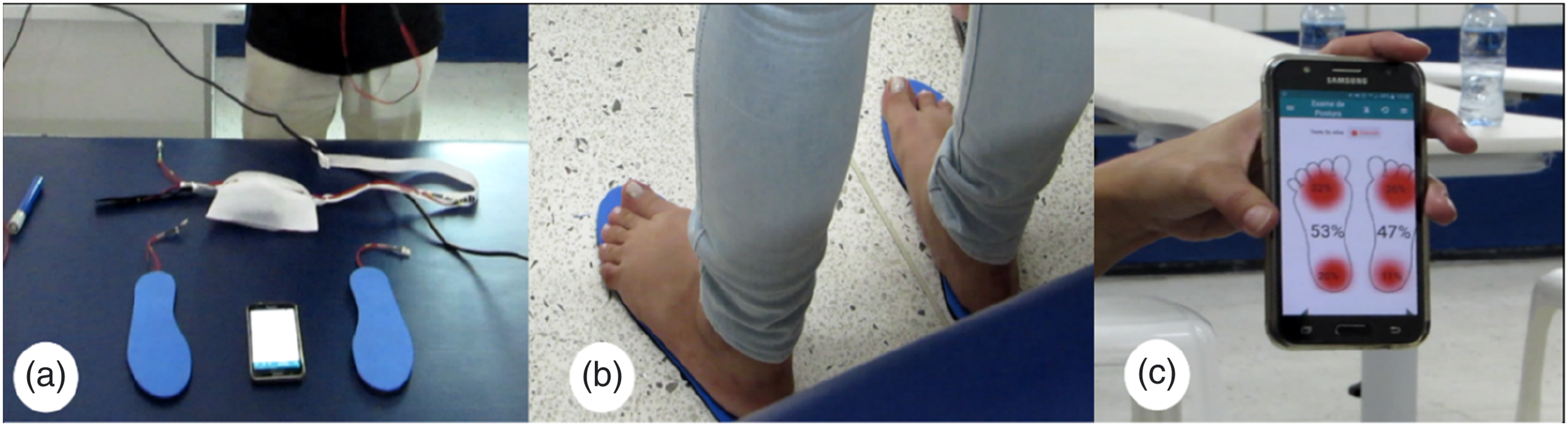
Participants included in the focus group.
Theoretical structure
The implementation of assistive technology in rehabilitation holds promise for individuals with disabilities, as it encompasses a range of products, systems, and services that enhance functional capacity, foster participation, and promote inclusion in all aspects of life. (World Health Organization, 2022). Assistive Technologies are increasingly being used in mobile health applications to improve patient care. Mobile health (mHealth) is defined as a medical and public health practice supported by mobile devices such as cell phones, patient monitoring devices, personal digital assistants, and other wireless devices (World Health Organization, 2022). Through digital solutions, mHealth facilitates user monitoring (Bradway et al., 2017), increases users’ access to health services (Matthew-Maich et al., 2016), promotes self-management (Zhou et al., 2020), and reduces costs (Iribarren et al., 2017).
User involvement is recommended in the construction of technological devices. Knowledge of the real needs and expectations of users, improvements in design, usability, and identifying potential problems at an early stage of the device development cycle are examples of barriers to overcome (Shah et al., 2009). Without these requirements, the chances of abandoning new technologies increase. Currently, user engagement and adherence to such technologies are below expectations, being a relevant challenge for developers (Postel-Vinay et al., 2018). To address these concerns, user-centric approaches allow developers to reflect user needs, integrating user and technology. User-centered design is an approach used in human-machine interaction which includes the idealization, implementation, adaptation, and functionality of technological devices (Graham et al., 2019). User involvement, unlike old models, confronts the hierarchy in which developers were seen as superior. Different approaches use user-centered design assumptions. When the user can understand and use the system in the testing phase, the use of the Participatory Design is recommended (Wright & Mccarthy, 2010).
Participatory Design, which involves collaboration between users and developers to create new technologies, is often used to construct assistive technologies for people with disabilities (Spinuzzi et al., 2005; Xiao et al., 2005). User engagement allows the exposure of their perspectives, enabling the process of problem-solving and application of new technologies in everyday life, especially in accessibility issues. In addition, different points of view on problem-solving happen in the multidisciplinary team, by integrating experience from different professionals from health and technology fields of expertise (Xiao et al., 2005). Participatory Design is described at different stages of studies, for example, in the design of new ways of applying existing technology to the testing of new technologies (Merkel & Kucharski, 2019; Spinuzzi et al., 2005).
Participants and recruitment
In September 2019, a public invitation was previously announced for students, professionals, professors, researchers, and post-stroke individuals who attended a forum discussing the theme “Assistive Technology”. Forum participants were briefly informed about the study, and the researchers and developers contacted those who agreed to participate. The multidisciplinary team was recruited to represent developers and health professionals, including physical therapists and students participating in rehabilitating the potential user. The potential user had restricted mobility attributed to a different way of walking. Her complaint was recurrent and identified in the asymmetry as the cause for her gait being different from other people.
Data collection and data analysis
The focus group developed a semi-structured interview to evaluate and adapt the technology product based on feedback from potential users during and after testing the prototype. The semi-structured interview was composed of open questions using a predefined set of questions to guide the discussion. According to the Participatory Design following the recommendations of good research practices (Postel-Vinay et al., 2018), the focus group was planned in the following steps: 1. Who are the participants? Refers to the reason why the participants were included in the survey. Targeted at the context of the user, multidisciplinary team, and moderator. 2. When are the participants involved? In this study, the potential user was involved during the prototype testing phase. In this phase, the potential user, multidisciplinary team, and developers exposed their experiences related to the use of the prototype, in order to improve the technical requirements of the baropodometric insole prototype. 3. How are participants incorporated into the testing of the technology? It refers to the assessment methods and instruments and the way the participants were integrated. 4. Why should participants be involved in technology testing? This step is focused on validating the acceptance of the prototype. Lastly, to define prototype improvement requirements.
The focus group addressed issues related to the experience and accessibility of the potential user in their context, facilitating potentialities, barriers/difficulties, and the requirements for the device. Data were collected through audio recordings of discussions during and after testing. The results of this study were described in the content analysis items, informing the descriptive statistical analysis of the analyzed recordings. As for the qualitative results, the statements of the volunteers involved in the forum were described in the items “Facilities and facilitators for the prototype application”, “Barriers and obstacles for the prototype application” and “Requirements to improve the prototype”.
The analysis of the content from the transcribed speeches followed four steps: (1) Pre-analysis: reading the transcribed text to obtain a general understanding of the entire content; (2) Coding: dividing the text into fragmented units of meaning (e.g. paragraphs, sentences, periods, or words individually expressing some perception); (3) Categorization: distributing units of meaning by categories of interest (intentional or induced), and (4) Interpretation: recognizing the issues that predominated in the discourse and understanding the perceptions of the study participants. Transcriptions were made in Excel™ software, and perceptions were fully transcribed for a complete analysis and the speeches presented in the results. Participants were identified by codes, preserving their confidentiality.
Data saturation was reached when the transcribed data provided the maximum amount of information about the potential user’s perspective. The extracted data was reviewed by two members. The data was then discussed together by the multidisciplinary team to ensure that similar content was classified and to determine whether subject categories should be adapted. The number of meaning units was used to calculate the frequency of distribution of perceptions by categories. We defined four intentional categories to allocate units of meaning by classes named (1) Guidelines: gathering the fragments listed by the forum moderator (prototype developer) to address general rules, principles, and explanations addressed to the participants; (2) Team’s perceptions: units from the speech of the multidisciplinary team; (3) User’s perception: speech from the potential user; and (4) Empty speech: speech with meaning that not related to the subject. Except for the empty speech, the fragments were redistributed into four other categories determined by reading and, for this reason, called induced categories (usage instructions, potentialities, limitations, and doubts) (Sousa & Santos, 2020).
Ethical considerations
This study was approved by the research ethics committee (CAAE: 79602117.9.3001.5054) of the University and complied with guidelines and standards for research involving human beings (resolution 466/12 of the National Health Council). An informed consent form was signed by each individual.
Results
Content analysis
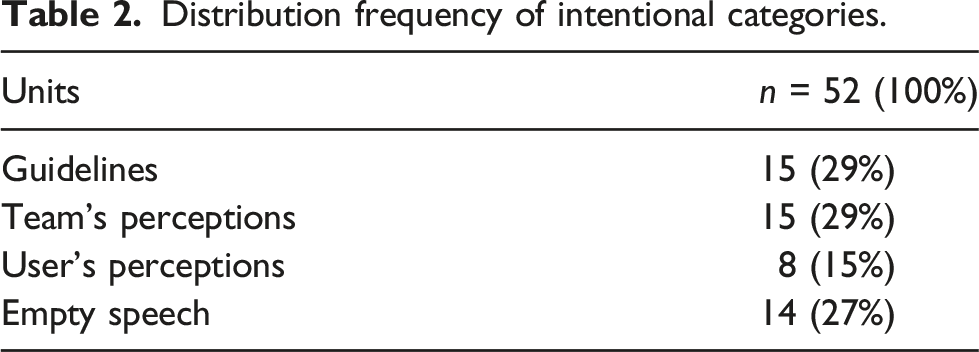
The transcribed text extracted 52 fragments a total of which 38 fragments were redistributed for context assessment. Guidelines filled 29% of the fragments and the Team’s perceptions predominated over the speech, which was expected since we only have one potential user in the discussion. Among the Team’s perceptions, the moderator’s speech was more present, revealing insights that emerged in Real-time. Limitations and potentialities also mentioned, favoring the creation of a list of requirements.
Distribution frequency of intentional categories.
Frequency of induced categories.
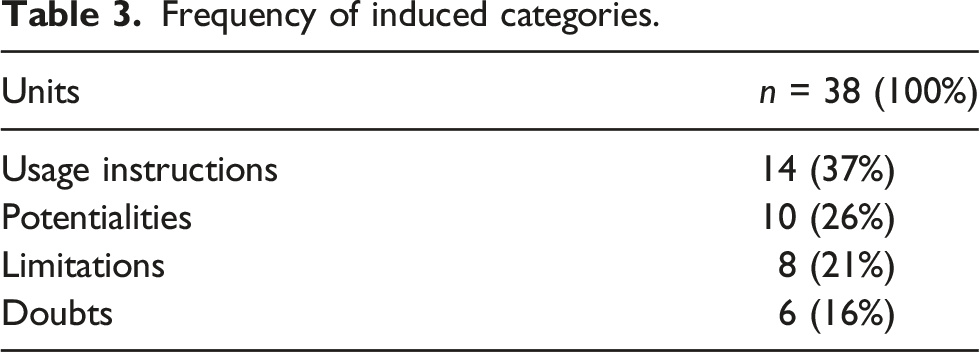
The content analysis allowed understanding perceptions to reach a collective discourse that pointed out barriers and facilities of the system and a list of requirements to improve the prototype, confirming the relevance of involving users in the technological testing process. The induced categories emerged after the content analysis revealed that the discourse can be redirected based on the perception of the potential user and the interactive discussion. Usage instructions, potentialities, and limitations that became the core of the discussion were distributed in 84% of the fragments of the induced categories.
Involvement of participants - who?
The moderator chosen had the most experienced in the construction of health technologies, capable of guiding the discussion on relevant topics. The multidisciplinary team was composed of researchers in the field of neurofunctional physiotherapy and engineering, and students who accompanied the potential user in their rehabilitation process, as well as other hemiparetic and hemiplegic individuals.
The potential user had reduced mobility due to right-sided hemiparesis with weight-bearing asymmetry contralateral to hemiparesis and wore an ankle-foot orthosis for permanent assistance while walking. The potential user is a married woman, vain, with incomplete primary education and an income of approximately two minimum wages. About two years ago, the potential user underwent physiotherapy treatment in an outpatient environment and frequently requested some intervention to correct the weight-bearing asymmetry, especially in a community environment.
Participants involvement - when?
The testing phase was conducted in a clinical environment, the potential user was required to perform activities usually performed in the rehabilitation service and in their daily lives such as walking and going up and down stairs. The performance of the baropodometric insoles and the connection with the application were monitored by the multidisciplinary team. In addition, the physical therapists who previously supervised the potential user’s rehabilitation were tasked with monitoring the activities performed. The potential user described the stimuli of the baropodometric insoles and operated the app, together with the multidisciplinary team.
Participants involvement - how?
The choice of interaction through the focus group allowed all participants to emphasize their perspectives on the issues of prototype testing. The moderator was elected to direct the discussion based on his experience as a researcher and technology developer (Figure 2). Although the guiding questions followed the recommendations according to the Participatory Design, participants were stimulated to expose their ideas and stimulate discussions on relevant issues. Focus group. The focus group was composed of one potential user who presented asymmetry in distribution due to hemiparesis after stroke, a multidisciplinary team was formed by twelve students, five physical therapists (professors and researchers), and one moderator, a doctor in electrical engineering, responsible for the design of the prototype baropodometric insoles. The moderator was in charge of conducting the group discussion involving all the participants to answer the questions aimed at improving the prototype of the baropodometric insoles. An audio recorder was used during the focus group for recording and later analysis of the speeches.
The diversity of the multidisciplinary team in terms of academic background and areas of knowledge was seen as a positive point, capable of enriching the discussion. Researchers and professors contributed with the clinical experience and lived through years of assistance to individuals with motor disabilities, among them, weight-bearing asymmetry. Some students present followed the rehabilitation process of the potential user in an academic internship, so it was possible that some observations could arise due to the weekly contact with the potential user, and that could help in the use of the prototype outside the rehabilitation service. When asked about using the prototype, the potential user was encouraged to contribute relevant information. The insertion of the potential user in the testing phase influences the improvement of the prototype, with possible future changes. The semi-structured interview identified the requirements of the multidisciplinary team and potential users.
Participants involvement - why?
During the prototype testing phase, the potential user exposed her perception regarding the acceptance of the baropodometric insole prototype. Based on this information, it was organized the potential user’s report into three stages: Facilities and facilitators for the prototype application; Barriers and difficulties for the prototype application, and Requirements to improve the prototype.
Facilities and facilitators for the prototype application
Positive considerations pointed out by the potential user revealed three main characteristics of the prototype. The first was highlighted by its ability to satisfactorily perform the actions for which it was developed. Moderator (Electrical Engineering): “It is correcting the discharge with the feedback, which is interesting both for therapy and for watching something… it is responding exactly to what it was designed for.” “Here, folks... Just a little... We are positioning the sensors... I adjusted it with an elastic accessory. I think you will collaborate a lot. See, one of the vibration sensors is already in position, and then you can adjust or change its position, but now it is fixed”.
The second and third characteristics pointed out by the comment of the potential user refer to the comfort of the insole and the quick adjustment of the weight-bearing asymmetry in response to the vibratory feedback. Potential user: “No, it is not [she was asked about the insole being uncomfortable]. It is just the shoe that is a little tight, but it is not bothering me too much.” “I can see that I am walking more normally”
Barriers and difficulties for the prototype application
The size of the shoes used predominated among the barriers and difficulties mentioned. The multidisciplinary team (students) and the potential user pointed to the inadequacy of the insole for the shoe size. Moderator (Electrical Engineering): "...another number of shoes would be better..." Professor (neurofunctional physical therapists): “… yes, the shoe looks uncomfortable…” Physiotherapy student: “… The insole must be a much smaller number than the one used…”.
Another difficulty involved malfunctions while handling the application, an expected feature due to the software being under development. The errors found were mainly related to measurement errors, data processing, misfit, wireless communication, and screen freezing. The malfunction was recognized by the moderator and multidisciplinary team. Moderator (Electrical Engineering): “It is offline. Funny that the engine stopped. I think it is the app. You must close everything and start over from the beginning. This app has not been tested yet, and now we see that it may crash”.
Errors in handling the application pointed out common adjustments during software development, allowing opportunities to reflect on new functions identified by the professor’s and the moderator’s observations. Professor (Neurofunctional physical therapists): “It is because it has not been configured to a dynamic shape yet (referring to using the prototype while on the go)”. Moderator (Electrical Engineering): “Oh, yes. She will feel it vibrating all the time. It will be like Zam, Zam, Zam, Zam”.
In this topic, the prototype promises better results if the errors pointed out by the study participants are considered. Thus, we realize that the device must increment new adjustments.
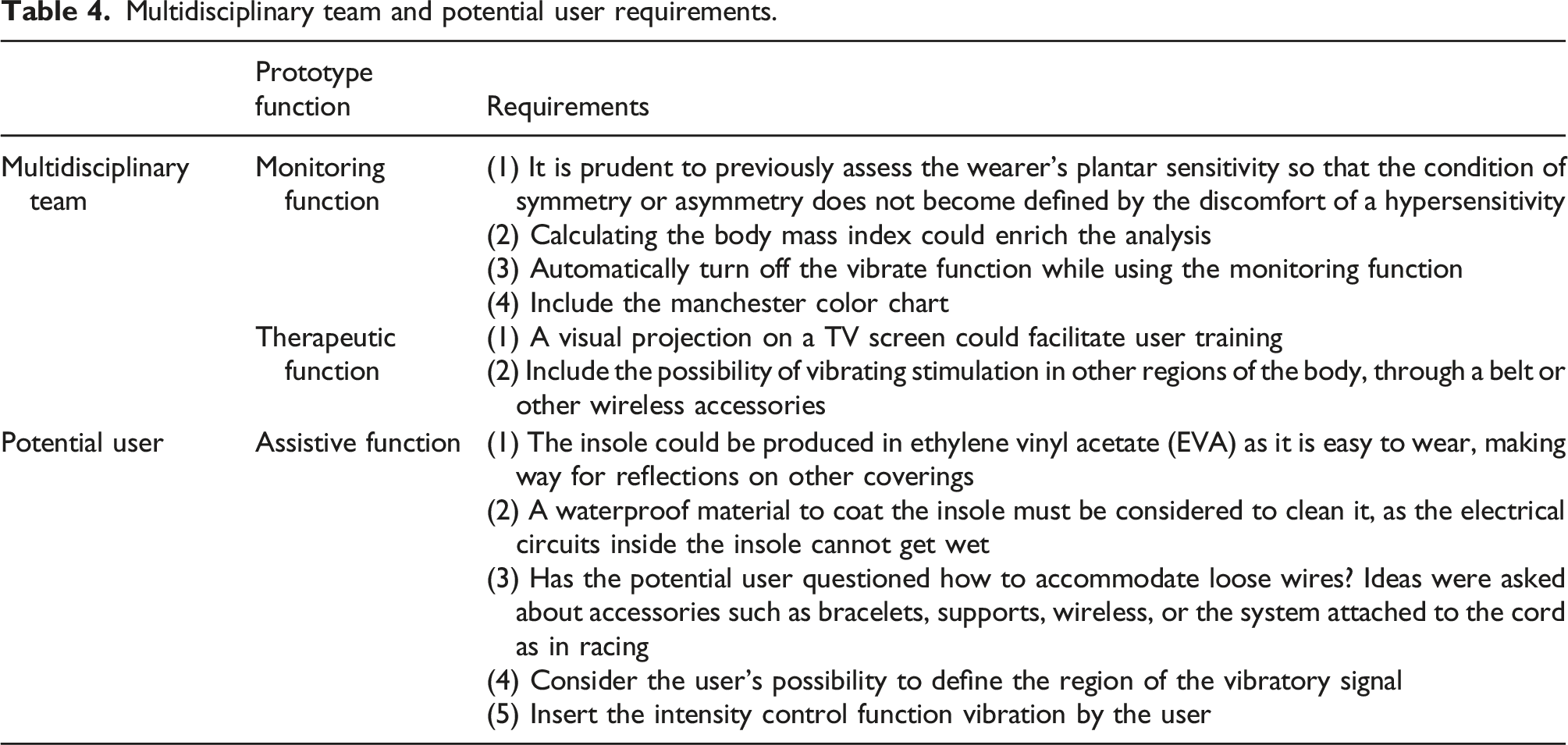
Requirements to improve the prototype
Multidisciplinary team and potential user requirements.
Discussion
This study approached the user experience by testing the baropodometric insole prototype, according to the Participatory Design which generated guiding information about the facilitators and barriers to using the prototype in everyday life, as well as the requirements for insole adjustments. The satisfactory interaction among the study participants stimulated the insertion of the user’s perception in the testing of the proposed technology (Nasr et al., 2016). The potential user considered the experience during the testing as positive, reporting comfort when walking and a rapid correction of weight-bearing asymmetry after the vibration stimulus of the prototype. In this way, the potential user and multidisciplinary team approved the potential prototype as an instrument capable of correcting the weight-bearing asymmetry. The usefulness of digital tools, the understanding of technology by health professionals, and the understanding of patient expectations facilitate the adoption of new technologies, especially when they can be applied basis daily (Keel et al., 2022).
During the prototype testing phase, the potential user reported dissatisfaction due to the shoe size not being suitable for the insole size. The difficulty in adapting the insole to the shoes was the most prevalent report for non-adherence to the use of the insole (Guimarães et al., 2006). In the present study, the incompatibility with the user’s footwear corroborates this perception and reinforces the importance of this aspect being promptly considered in the insole improvement process. During the testing phase, the developers hypothesized that the shoe size would need to be larger than usual to be comfortable and compatible with the insole. Another possibility is to consider different sizes of insole for each user.
The software connection was another barrier encountered. As this is a device under development, incompatibilities between the insole and the software are expected. However, the difficulty of access and unfamiliarity with digital tools are potential obstacles to adoption by physical therapists and users (Keel et al., 2022). It is necessary to encourage training for physical therapists and users on the operation and handling of the baropodometric insole prototype, ensuring confidence and assuredness during use. In addition to the constant use of the device, physical therapists and users must be able to deal with limitations and unforeseen circumstances of the equipment use (O’Connell et al., 2021).
Requirements suggested by the multidisciplinary team and potential user aimed to improve the prototype for adjustments. To the potential user, the prototype requires improvements in the material chosen to manufacture the insole and changes in the intensity and positioning of the vibrating signal. Therefore, attention to comfort, aesthetics, hygiene, and portability can affect the user’s readiness to adhere to the baropodometric insole prototype, especially for self-administered devices. Aspects of monitoring and therapeutic functions provide us with information for clinical implications, especially in the acquisition of real gains for an overall improvement of the prototype, which was achieved with the multidisciplinary group during the testing phase.
The limitations present in our study; First, even though there is no ideal sample size in qualitative studies, a greater number of users could expand the perceptions of using the prototype. However, our only user was able to generate valuable information for the improvement of the prototype as she refers to asymmetric weight distribution as her main complain and the relation with aesthetic and functioning consequences arising from this deficit. Second, it is necessary to test the usability of baropodometric insoles in different users with different gait patterns, motor impairments, and genders, as well as the eventual barriers to using the software in different social classes and educational backgrounds. Thirdly, data collection was restricted to a controlled clinical setting and was conducted over a finite period. Expanding the potential applications of this emerging technology hinges on occupational therapy’s focus on enhancing activities of daily living, occupation, and leisure activities. As technology advances in future studies, the direction of application in a home and community setting and the perspective of the occupational therapist becomes key to identifying new requirements. In addition, the performance of baropodometric insoles should be tested during activities that require walking on different surfaces, for longer periods and that require greater balance. In this way, different perspectives would help us understand different social contexts, obstacles, and solutions to be faced.
Conclusion
The user experience during the use test of the baropodometric insole prototype signals the promising potential of the device for monitoring and treatment of weight-bearing asymmetry. Instructions for use and comments from the multidisciplinary team, as well as the acceptance of the potential user, predominated in the focus group. From the Participatory Design, it was possible to identify facilitators, barriers, and requirements that could be considered and adjusted for the improvement and future implementation of the prototype in future phases of this project.
Footnotes
Acknowledgements
This study is the result of a partnership between the multidisciplinary project HEMITEC (Technologies for the Conditions of Hemiparesis and Hemiplegia) and the NTAAI group (Center for Assistive Technology, Accessibility, and Innovation), coordinated by professors and researchers from the different university. The authors thank all participants for their valuable contributions.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: M, HR is a founding partner and board member of Visuri SA, which manufactures baropodometric insoles prototype. Other authors state no conflict of interest.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.