
Abstract
Introduction
This study investigated the relationship between sensory processing, respiratory sinus arrhythmia, and social participation in people with psychiatric disorders.
Method
This study recruited 30 participants, primarily women, from a psychiatric university hospital with a mental health diagnosis listed in the Diagnostic and Statistical Manual of Mental Disorders Fifth Edition (mean age: 37.7 ± 16.0 years). Sensory processing, autonomic nervous function, and social participation were measured using the Adolescent/Adult Sensory Profile®, respiratory sinus arrhythmia, and World Health Organization Disability Assessment Schedule, respectively. Through mediation analysis, a model wherein sensory processing mediated the relationship between respiratory sinus arrhythmia and social participation was developed.
Results
Social participation was moderately to highly correlated with Adolescent/Adult Sensory Profile® quadrants (excluding sensory seeking) and respiratory sinus arrhythmia. Furthermore, the mediation analysis revealed that sensory avoiding mediated the relationship between respiratory sinus arrhythmia and social participation, consequently counteracting the direct relationship.
Conclusion
A mediation model was constructed, which indicated that individuals with psychiatric disorders and low parasympathetic nervous system activity expressed higher sensory processing quadrant of sensory avoiding. Ultimately, this was associated with reduced social participation.
Introduction
Social participation and interpersonal relationships are essential for the physical and mental health of people with psychiatric disorders such as depression and schizophrenia. Additionally, social participation positively impacts physical well-being and life expectancy and is important for psychological and emotional stability (Shor et al., 2013). However, people with severe mental illness spend more time alone and are less likely to participate in social activities (Walsh et al., 2002). Consequently, these factors reduce life expectancy because of an increased risk for cardiovascular and metabolic disorders (Plana-Ripoll et al., 2019). In addition, social identity, interpersonal relationships, and group activity participation can improve participants’ psychological well-being and mental health (Cruwys et al., 2013). Therefore, continued participation in group activities, including community involvement, is critical to promoting recovery and preventing relapse from mental illness.
In occupational therapy, therapists enhance self-esteem and productivity using recreational and expressive creative activities. Particularly, this psychosocial treatment is offered in many psychiatric and day hospitals (Arbesman et al., 2013). Furthermore, these interventions address occupational engagement through various strategies and approaches such as social skills training and cognitive behavioral therapy (D’Amico et al., 2018). Hitch et al. (2015) examined the evidence investigating mental health occupational therapy published between 2000 and 2013. The top 10 most cited articles independently examined various aspects, including stress, sensory processing, and participation. However, the relationship between these aspects remains unexplored.
Organisation for Economic Cooperation and Development (OECD) countries widely use length of stay (LOS) as a parameter for assessing hospital efficiency. International surveys have shown that the number of hospitalized patients with psychiatric comorbidities continues to increase (Ngo et al., 2013). Consequently, these patients are likely to experience longer LOS, reflecting compromises to the quality of life and care experience. Furthermore, this highlights the inefficiencies in the healthcare system. Therefore, occupational therapists should consider effective ways to promote social participation among hospitalized patients.
Over the last few decades, the need for interventions associated with people with mental illnesses who have sensory problems has emerged globally (Champagne & Stromberg, 2004). Sensory processing is the organization of sensory information from the body and environment that enables effective interaction with the physical and social environment. Sensory processing assessment and intervention are commonly performed in occupational therapy (Brown et al., 2019). The Sensory Profile® (SP; Dunn, 2001) refers to a series of sensory processing assessment tools comprising questions divided into three major categories, namely, sensory processing (auditory, visual, vestibular, tactile, complex sensory, and oral sensory), coordination, and behavioral and emotional responses, with parents (observers) reporting the frequency of behaviors and the examiner tabulating scores. The four-quadrant conceptual model (low registration, sensory seeking, sensory sensitivity, and sensory avoiding) is central to interpreting the sensory profile. Furthermore, classification is based on neurological thresholds and behavioral responses. The Adolescent/Adult Sensory Profile® (AASP) has been used with adolescents and adults with various psychiatric conditions, including schizophrenia and autism spectrum disorders (ASDs). Particularly, these illnesses exhibit specific sensory processing patterns not found in healthy controls (Brown et al., 2002). Increasingly, interventions for specific sensory processing have been developed based on this assessment, which apply bottom-up changes to their characteristics (Andersen et al., 2017). An intervention for specific sensory processing involves the use of a sensory room. Sensory rooms refer to special environments that promote relaxation and self-organization (Champagne & Stromberg, 2004). Sensory rooms in psychiatric departments typically contain various items and furniture (e.g., rocking chairs, stress balls, weighted blankets) to enhance sensory input.
Studies examining the autonomic nervous system (ANS) using physiological measures have found that children with sensory processing disorders generally exhibit lower parasympathetic nervous system (PNS) activity at rest in contrast to typically developing children (Schaaf et al., 2010). Furthermore, severe symptoms of sensory processing disorders in childhood significantly indicate a higher likelihood of being diagnosed with a lifelong anxiety disorder (McMahon et al., 2019). However, to date, no studies have investigated the relationship between sensory processing characteristics and autonomic function in adolescents and adults. The sympathetic nervous system (SNS) serves as the autonomic division that transmits excitatory stimuli to various organs throughout the body. These stimuli increase heart rate, vasoconstriction, pupil dilation, and sweat secretion. The PNS functions in calming physical activity and has antagonistic effects on the SNS such as heart rate phenomena. Collectively, these systems influence heart rate, respiration, sweating, pupil dilation, salivation, and several other physical processes. Moreover, ANS activity has been estimated using heart rate variability (HRV) based on the indices of both high- and low-frequency HRVs.
Notably, respiration and HRV are closely related. Respiratory sinus arrhythmia (RSA), in which heart rate decreases during the expiratory phase and increases during the inspiratory phase, is a noninvasive tool to measure PNS effects (Porges, 1995, 2007). Decreased HRV has been reported as ANS dysfunction in various psychiatric disorders, including schizophrenia, bipolar disorder, ASD, depression, and panic disorder (Arora et al., 2021). Moreover, decreased HRV suggests an imbalance between the SNS and PNS. Consequently, several individuals with mental illnesses have more problems with the PNS than with the SNS.
Current research focuses on RSA, which reflects the PNS function. According to the polyvagal theory (Porges, 1995, 2007), the PNS comprises two vagal complexes, namely, dorsal and ventral. Particularly, the dorsal complex generates life-sustaining defensive responses, while the ventral complex inhibits such responses and maintains social engagement. Thus, the mindfulness approach improves awareness by cultivating sustained attention to bodily sensations. Mindfulness breathing exercises interact with the neural networks involved in executive functioning and emotional regulation. For example, deep breathing incorporated in yoga activates cardiopulmonary baroreceptors and reflexively decreases SNS activity helping to improve RSA (Heckenberg et al., 2018). However, the relationship between sensory processing, parasympathetic functioning, and social participation in people with mental illnesses has not been investigated comprehensively. As a result, it remains unclear whether interventions involving sensory processing and enhancement of parasympathetic functioning positively impact social participation in people with mental illnesses. In the 1920s, the American physiologist Walter Cannon first described the fight-or-flight response (Cannon, 1929), which forms part of the first phase of Hans Selye’s general stress response theory (Selye, 1956). Recently, studies found that children exposed to stressful experiences such as pain could exhibit more sensory processing problems (McLean et al., 2021). Thus, a decrease in RSA in individuals with psychiatric disorders is anticipated to affect sensory processing.
This study investigated whether sensory processing and RSA are associated with impaired interpersonal relationships and social participation in people with mental illnesses. Based on the fight-or-flight response, this study hypothesized that RSA affects sensory processing. Particularly, (1) sensory processing and RSA are related to social participation and (2) sensory processing mediates the relationship between RSA and social participation.
Method
Participants
Participants who received occupational therapy at a university hospital and had a modified global assessment of functioning score of 67 or lower were recruited for this study. The modified global assessment of functioning consists of a scale (ranging from 1 to 100) used to evaluate adult social, occupational, and psychological functioning. Higher values indicate good mental health. A score of 67 or less indicates challenges in social, professional, or school functioning (e.g., sometimes taking an extended break or stealing money). The participants demonstrated various mental illnesses such as schizophrenia, ASD, depression, bipolar disorder, and eating disorders. Individuals identified by psychiatrists to have difficulty understanding or participating in the study because of dementia or traumatic brain injury were excluded.
The Medical Ethics Committee of the authors’ university approved this study [details blinded for peer review]. All participants were informed of the study details and only those who provided signed informed consent were included.
Measurement Instruments
The study used a concurrent cross-sectional design. Sensory processing, social participation, and RSA were measured using the AASP, the World Health Organization Disability Assessment Schedule (WHODAS 2.0), and pulse wave measurement and analysis.
Characteristics of Sensory Processing
The AASP is a 60-item questionnaire that evaluates daily sensory processing and its impact on behaviors. Furthermore, it consists of statements such as “If I sense a strong odor in a store, I leave the store or move to another sales area.” Participants rated each statement on a five-point scale (1 = almost never and 5 = almost always). The AASP comprises four quadrants (low registration, sensory seeking, sensory sensitivity, and sensory avoiding), each containing 15 items. The full evaluation of the participants for these items is the “total quadrant score,” also referred to as the total quadrant. Low registration is a condition in which a stimulus is difficult or unnoticeable. Furthermore, the neurological threshold is high and thus the response may be delayed or absent. Consequently, the behavior observed is often relatively passive. Similarly, the neurological threshold is high for sensory seeking, which refers to weak responses to stimuli and active attempts to experience them, as observed in the study. Sensory sensitivity refers to a strong response to stimuli where a reaction to an external stimulus is perceived as excessive. The neurological threshold is low and the observed behavior is often passive. Sensory avoidance refers to an active avoidance response to a stimulus. The neurological threshold is low and the behavior observed is typically active (van den Boogert et al., 2022). The 60 AASP items encompass experiences related to the sensory processing categories, namely, taste, smell, movement, vision, touch, activity level, and hearing (Brown et al., 2002). The Japanese version of the AASP was developed by first translating the scale items into Japanese, back-translating them, and then obtaining the original author’s approval. Reliability was evaluated based on a sample of 1198 non-clinical and 172 clinical group participants by calculating Cronbach’s alpha coefficient for each quadrant, which was greater than 0.80.
Social Participation Measurements
The WHODAS 2.0 is a self-administered assessment tool developed by the World Health Organization and has been validated for its reliability. Particularly, WHODAS 2.0 comprehensively evaluates mental and physical functions and social participation related to a wide variety of disorders (Koopmans et al., 2020). Furthermore, WHOSA 2.0 is a highly generalizable tool standardized to assess health and disability. It comprises 36 questions in six areas (i.e., cognition, mobility, self-care, interaction with others, activities of daily living, and participation in society), evaluated through self-evaluation, interviews, and writing by agents. Each question is rated on a five-point Likert scale, with lower scores indicating better health.
Autonomic Nervous System Function Measurement
ANS function was measured in a private room maintained at a temperature of 25°C and approximately 50% humidity. Upon entering the room, the participants took a 5-minute break and were instructed to sit on a chair at a 90-degree reclining angle and look at the gazing point on the computer screen. Their pulse waves were recorded for 3 minutes while they were sitting in the chair, using a Polyplex (Nihon Santech). The measurements were sampled at 1 kHz and stored using a dedicated computer and software (Input monitor; Nihon Santech). In the data analysis, the RR interval peaks were set using Cardio Peak for preprocessing. The noise level was set according to the data provided by Porges and Bohrer (1990). Furthermore, editing and quantification of HRV were performed using the CardioEdit and CardioBatch programs (Brain-Body Center, University of Illinois at Chicago, IL, USA). The inter-beat interval series was linearly interpolated and filtered to remove spontaneous breathing (0.12–0.40 Hz) in RSA. Specifically, a low threshold of 0.12 Hz was used because healthy participants often report respiratory rates lower than 0.15 Hz (Saboul et al., 2014). Notably, these results are mathematically equivalent to a steady-state spectral analysis. Moreover, the method is not influenced by respiration and complies with the assumptions required for parametric statistics. The RSA data were quantified in consecutive 30-second epochs.
Statistical Analysis
The data were analyzed in two steps. Statistical analysis was performed using SPSS Version 26. All analyses were two-tailed and the alpha level was set to 0.05.
The correlation between the total WHODAS 2.0 score (social participation), each quadrant of AASP (low registration, sensory seeking, sensory sensitivity, and sensory avoidance), and RSA was examined using Spearman’s rank correlation coefficient.
A mediation analysis using SPSS Process Macro (Preacher & Hayes, 2008) was conducted on the items that were significantly correlated with social participation. Particularly, social participation comprised the objective variable, while RSA and sensory processing quadrants were the independent variables. A bootstrap method was used to assess the mediation path, namely, the indirect effect of the independent on the dependent variable through the mediation variable. Estimates of indirect effects were computed using 5000 bootstrap samples and 95% bias-corrected confidence intervals (CIs) were constructed from the sampling distribution. The mediation effect in this study was considered significant at p < .05 if there were no 0s within the 95% CI and the null hypothesis of no mediation effect was rejected (Preacher & Hayes, 2004, 2008).
Results
Diagnosis Name and Number of Participants.
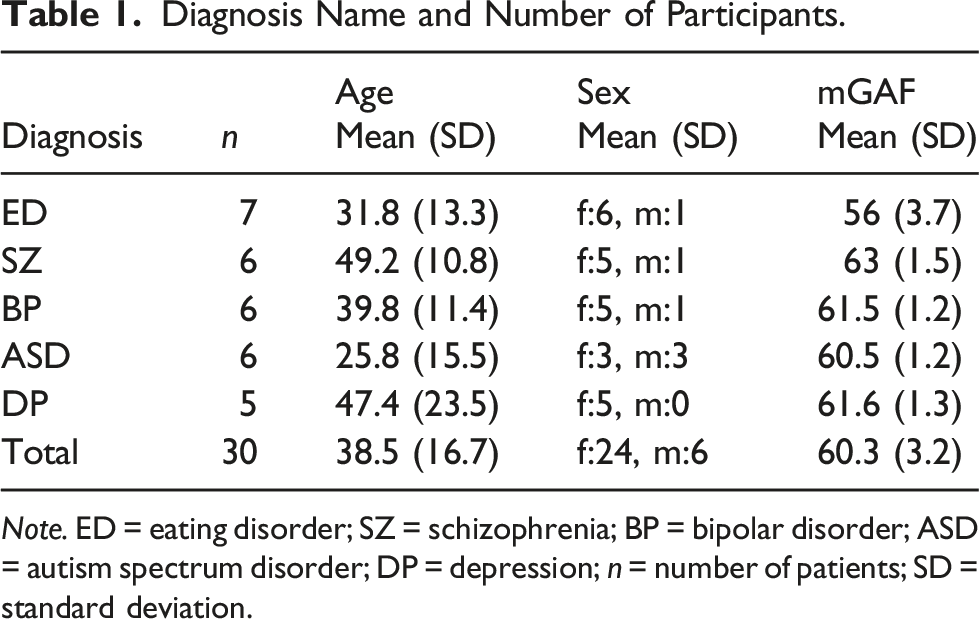
Note. ED = eating disorder; SZ = schizophrenia; BP = bipolar disorder; ASD = autism spectrum disorder; DP = depression; n = number of patients; SD = standard deviation.
Results of the Correlation Analysis.
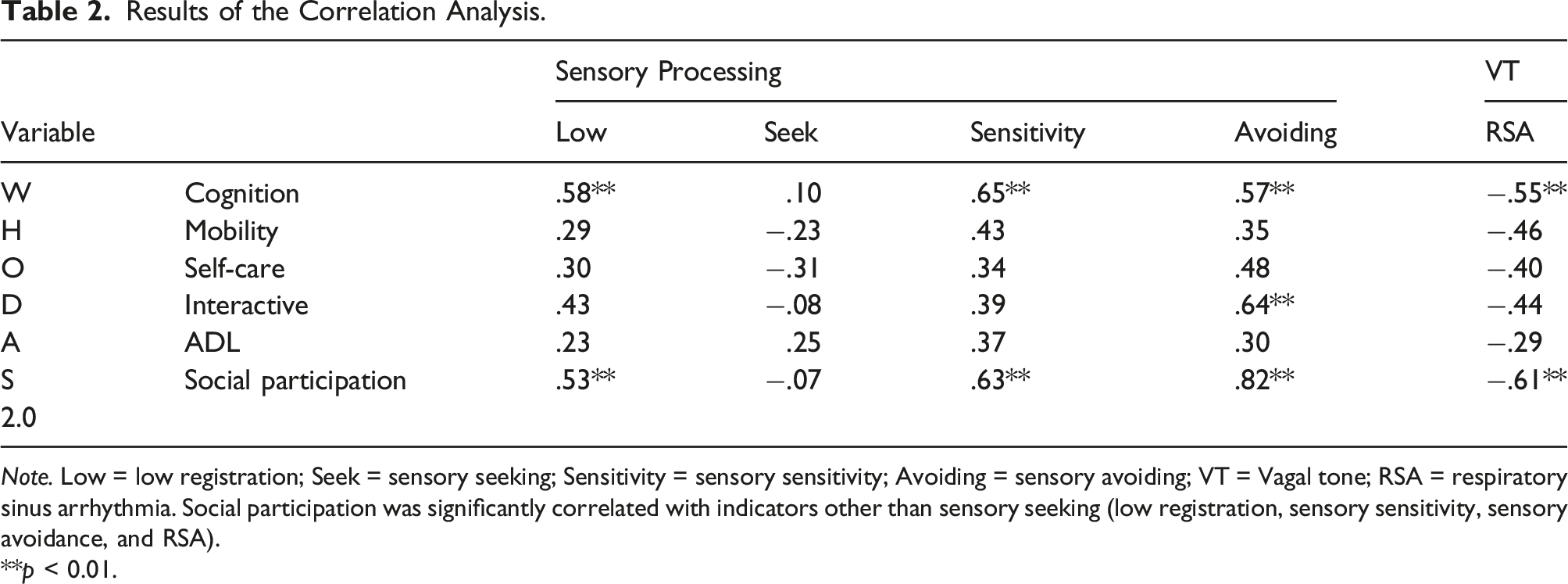
Note. Low = low registration; Seek = sensory seeking; Sensitivity = sensory sensitivity; Avoiding = sensory avoiding; VT = Vagal tone; RSA = respiratory sinus arrhythmia. Social participation was significantly correlated with indicators other than sensory seeking (low registration, sensory sensitivity, sensory avoidance, and RSA).
**p < 0.01.
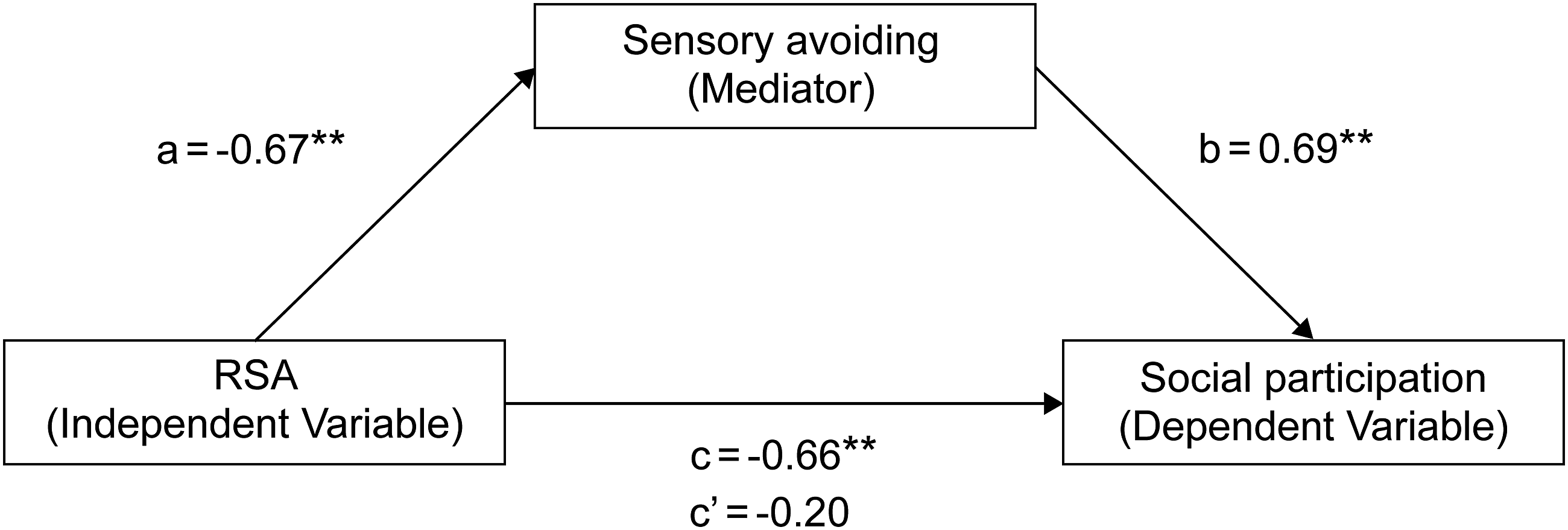
Results of mediation analysis with sensory avoidance as the mediating variable. Individuals with lower PNS activity have higher sensory avoidance scores, which is associated with limited social participation. Standard partial regression coefficients for values of a, b, and c for high sensory avoiding (M + 1SD) and c’ for low sensory avoiding (M-1SD). **: p < .01, *: p < .05.
Discussion
The current findings showed that low registration, sensory sensitivity, sensory avoidance, and RSA were strongly associated with social participation, while sensory seeking was not. Notably, this study demonstrated that sensory avoidance mediated the predictive relationship between RSA and social participation.
Relationship Between Sensory Processing and Social Participation
Based on the researchers’ extensive experience in clinical practice, many individuals with mental illness exhibit difficulties with sensory processing. The current study is supported by a meta-analysis that observed individuals with various types of mental illness and found that they have low registration, hypersensitivity, increased levels of sensory avoidance, and decreased sensory exploration (van den Boogert et al., 2022).
Patients with psychiatric disorders, such as schizophrenia, have atypical neural responses to sensory stimuli. Furthermore, individuals with auditory and visual processing disorders may experience difficulty selecting information from ambient noise, as exemplified by the cocktail party effect and sensory gating problems. Mismatch-negativity (MMN) potentials originating in the superior temporal gyrus near the primary auditory cortex are event-related. Specifically, they reflect the ability to automatically detect changes in sound (Erickson et al., 2016). Several studies have reported that reduced gray matter volume in the superior temporal gyrus of individuals with schizophrenia correlates clearly with MMN amplitude (Kasai et al., 2003). In addition, individuals with ASD scored higher than those with typical development in the quadrants excluding sensory search, while sensory hypersensitivity was associated with an especially low MMN (Ludlow et al., 2014). Regarding the relationship between sensory processing and social participation, Light and Braff (2005) found that smaller amplitudes of MMN in patients with schizophrenia were significantly associated with lower overall functional scores. Kawakubo et al. (2007) also reported that the MMN is an indicator of social skill acquisition, suggesting that sensory processing problems interfere with social adjustment.
Sensory profile studies have found correlations between quadrants such as low registration, sensory sensitivity, sensory avoidance, and social participation. For example, individuals with sensory processing problems exhibit more limited social participation (Kuno-Fujita et al., 2020). Furthermore, individuals with schizophrenia, bipolar disorder, and ASD yield higher sensory avoidance scores than those with typical development. Patients with depression also exhibit extreme sensory processing patterns that are higher in all four quadrants compared to healthy controls, and this has been found to be associated with depressive symptoms, including anxiety (Paquet et al., 2022). A study examining the effect of differences in sensory processing patterns on children’s participation in leisure activities found that avoidance scores were negatively correlated with a preference for social activities (Ismael et al., 2015). Moreover, the study also found correlations between social participation and the low registration, hypersensitivity, and sensory avoidance quadrants. These results support previous research findings indicating that individuals with more sensory processing problems in a larger number of quadrants were more likely to limit their social participation.
Relationship Between Respiratory Sinus Arrhythmia and Social Participation
ANS functions, specifically those mediated by the PNS, play a significant role in mammalian bonding (Porges, 2007). RSA is the respiratory component of the cardiac rhythm mediated by the vagus, an indicator of parasympathetic activity. This index reflects a mammal’s ability to flexibly adapt to subtle changes in environmental events, supporting the foundation of good social competence (Porges, 1995). Several studies have underscored an association between high RSA, favorable developmental outcomes, and adaptive behavior in newborns and infants. The results from these studies suggest that RSA is a crucial physiological component for appropriate engagement with the environment (Hofheimer et al., 1995). Furthermore, high resting RSA promotes engagement, improves social competence, and increases social flexibility (Muhtadie et al., 2015). In contrast, low resting RSA is associated with psychopathology in adolescents and adults (Beauchaine & Thayer, 2015). Thus, these study results support the finding that people with lower RSA exhibit more limited social participation. In the present study, the results of the correlational analysis showed that social participation was more restricted among people with mental illness when RSA was low. The results support previous research and provide information that increasing RSA may support social participation.
Building and Utilizing an Intermediary Model
Notably, this study found that sensory avoidance acted as a mediator in the relationship between RSA and social participation. However, the relationship between low registration and sensory sensitivity was not supported. The results of mediation analyses indicate that parasympathetic function is associated with social participation. However, sensory processing characteristics mediated by sensory avoidance counteract this relationship. Therefore, individuals with sensory problems such as sensory avoidance are unlikely to increase their social participation simply by increasing RSA at rest, suggesting the need to assess sensory characteristics before intervention. According to Cannon (1929), sensing personal danger causes adrenaline release, increases SNS activity, and induces a fight-or-flight response. In the present study, the PNS’s activity is reduced, threatening personal safety, resulting in a relative increase in SNS activity and the behavioral pattern of avoidance. This finding suggests that mentally ill individuals have atypical sensory processing patterns and these characteristics influence their subsequent behavior (Bailliard & Whigham, 2017). Thus, it is necessary to understand the characteristics of an individual’s sensory processing, its effect on daily life situations, and how people with mental illness respond to it. From the current findings, a mediation model was developed in which parasympathetic functioning was associated with the behavioral trait of sensory avoidance, resulting in reduced social participation (Figure 1). In psychiatric occupational therapy, interventions that promote adaptation to aversive behaviors using programs such as Social Skills Training after conditioning can increase parasympathetic function. Particularly, these interventions include using the Sensory Room, mindfulness, and yoga, which may positively impact socialization (Adams-Leask et al., 2018).
Limitations
Limitations of this study are the small sample size from a single hospital and the fact that most participants were female and included a diverse range of conditions. Test power (1-β) in the correlation analysis using G*Power was 0.82 for a sample of 27 individuals, which is sufficient even when the correlation coefficient is set at 0.50. However, the present study included a variety of psychiatric disorders, which could not be examined separately. Furthermore, problems with social participation were strongly associated with one quadrant in sensory processing, namely sensory avoidance, because of decreased PNS activity. The present results indicate an overall rather than a disease-specific trend. Thus, future research should clarify these associations by conducting multivariate analyses of factors related to social participation according to the International Classification of Functioning, Disability, and Health model. Specifically, this model should consider functional and activity participation levels as well as individual and environmental factors. Age, gender and mental health have been identified as factors associated with social participation (Kiely et al., 2021) and these should be taken into account in future research.
Implications for Occupational Therapy Practice
The results of this study were used to propose a model demonstrating that reduced PNS activity is strongly associated with sensory avoidance, one of the quadrants of sensory processing, resulting in reduced social participation. Furthermore, people with low PNS activity are more likely to avoid various sensory stimuli. Thus, therapists ought to be aware of the potential relationship between PNS and differences in sensory processing in mentally ill patients. Among the quadrants of sensory processing, sensory avoidance mediates social participation. This finding suggests the importance of therapists capturing and supporting the subject’s sensory processing characteristics in advance.
Conclusion
This study investigated the relationships between social participation, sensory processing, and RSA in people with mental illness. The mediation analysis revealed that individuals with lower PNS expressed higher sensory processing traits of sensory avoidance, which is associated with lower social participation. This study also found that the fight-or-flight response to a perceived threat is a reflexive neural phenomenon. However, patterns of escape responses could contribute to reduced social participation.
Footnotes
Acknowledgments
We would like to express our sincere gratitude to all the participants who cooperated in the study and to the laboratory members for their advice in submitting the study. We would like to thank Editage (![]() ) for English language editing and journal submission support. We have authorized the submission of this manuscript through Editage.
) for English language editing and journal submission support. We have authorized the submission of this manuscript through Editage.
Author Contributions
Conceptualization: KI, RH, and TM; methodology: R, KI, HI, and TM; formal analysis and investigation: RH, KI, TM, KT, TM, and HI; writing–original draft preparation: RH, KI, and TM; writing–review and editing: KI, KT, TM, and HI; funding acquisition: KI.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was partially supported by the JSPS KAKENHI Grant-in-Aid for Early-Career Scientists (Grant number: 22K17631) from the Japan Society for the Promotion of Science and SPIRITS 2021 of Kyoto University.
Ethical Approval
This study was approved by the Medical Ethics Committee of the Graduate School of Medicine, Faculty of Medicine, and the hospital was affiliated with the Graduate School of Medicine, Kyoto University (R2819).
Informed Consent Statement
All participants were informed about the experiments, and only those who provided signed informed consent were included.
Patient and Public Involvement Data
During the development, progress, and reporting of the submitted research, Patient and Public Involvement in the research was not included at any stage of the research.