
Abstract
Background
Validated outcome measures are essential for assessment and treatment of children with disabilities. The Children’s Hand-use Experience Questionnaire (CHEQ) was developed and validated for use in Western countries for children with unilateral hand dysfunction. This study aimed to perform a cross-cultural adaptation and investigate reliability for the Arabic CHEQ.
Methods
Translation and cross-cultural adaptation were performed in four phases: (i) forward-translation and reconciliation with feedback from parents and typically developing children from Jordan (n = 14); (ii) backward-translation and review; (iii) cognitive debriefing with parents and/or their children with unilateral hand dysfunction (n = 17); and (iv) review and proofreading. In the psychometric analyses, 161 children from Jordan (mean age [SD] 10y 8 m [5y 8 m]; 88 males) participated. Internal consistency was evaluated with Cronbach’s alpha. Test-retest reliability was evaluated in 39 children with intraclass correlation coefficient (ICC) and weighted kappa (κ).
Results
Synonyms of four words were added to accommodate for different Arabic dialects. On average, 93% of children with unilateral hand dysfunction and their parents understood the CHEQ items. One response alternative, ‘Get help’, to the opening question was unclear for 70% of the respondents and need further explanation. Two items about using a knife and fork were difficult to comprehend and culturally irrelevant. High internal consistency was demonstrated (Cronbach’s alphas 0.94- 0.97) and moderate to excellent ICC (0.77–0.93). For 18 individual items, κ indicated poor to good agreement (κ between 0.28 and 0.66).
Conclusions
After the suggested minor adjustments, the Arabic CHEQ will be comprehensible, culturally relevant and reliable for assessing children with unilateral hand dysfunction in Jordan.
Introduction
Globally, between 93 and 150 million children live with some form of disability, and most of them live in developing countries (United Nations Children’s Fund [UNICEF], 2013). These children need rehabilitation to increase their participation and level of independence in performing daily life activities. Children’s experience of activity performance is an important part of the rehabilitation, and assessments like the Children’s Hand-use Experience Questionnaire (CHEQ) help determine children’s need for support and monitor treatment effectiveness along the process. The CHEQ belongs to the group of Patient Reported Outcome Measures (PROMs), which support patients’ self-reflection and raise clinicians’ awareness of patient concerns (Greenhalgh et al., 2018). However, most of these instruments have been developed and validated in Western countries and may reflect the daily life activities in that cultural context. Using these instruments directly in a different cultural context may give erroneous results. More than 400 million people live in Arabic-speaking countries, which have a substantial population of children with disabilities. The estimated incidence of cerebral palsy for children in Jordan is about 0.36% – higher than in Europe and the USA (Attieh et al., 2010). However, there is a shortage of culturally-adapted instruments to be used in Arabic-speaking countries (Geisinger, 1994; Gladstone et al., 2008; Kakooza-Mwesige et al., 2018)
The CHEQ is an established PROM, developed for children with unilateral hand dysfunction such as unilateral cerebral palsy, obstetric brachial plexus palsy or upper-limb reduction deficiency (Skold et al., 2011). It evaluates the perceived experience of using the affected hand in bimanual daily life activities (Skold et al., 2011; Wallen & Stewart, 2015), and its validity and reliability have been evaluated in previous studies (Amer et al., 2016; Ryll et al., 2018; Skold et al., 2011). The CHEQ was designed and developed to be an international instrument and has been translated into 14 languages (www.cheq.se) and used in descriptive and interventional studies (Cohen-Holzer et al., 2017; Hermansson et al., 2013; Hines et al., 2019; Ryll et al., 2017). The English language version of the CHEQ (Skold et al., 2011) was previously forward-translated into Arabic. However, exclusively literal translation may distort the intent of the instrument and lead to misleading results due to cultural differences (Wagner et al., 1998; Yu et al., 2004). Therefore, a systematic translation and cross-cultural adaptation process is recommended, focussing on both the semantic and content aspects, rather than only on literal translation (Wild et al., 2005; Yu et al., 2004). Nevertheless, the cross-cultural adaptation is not, in itself, sufficient to suggest using any PROM clinically. Investigating psychometric properties to assure the validity and reliability of the adapted instrument is necessary (Amer et al., 2018; American Educational Research Association et al., 2014; Bullinger et al., 1993; Erkin et al., 2007).
Hence, this study aimed to perform a cross-cultural adaptation and psychometric analyses of the Arabic version of the CHEQ. More specifically, it aimed to determine if it is comprehensible and culturally relevant to the respondents and if the instrument demonstrates internal consistency and test-retest reliability.
Methods
This study was performed in two steps. The first step was cross-cultural validation and adaptation of the Arabic version of the CHEQ. The second step was psychometric analyses of the Arabic version of the CHEQ by assessing its internal consistency and test-retest reliability. The data collection was carried out by authors AA, MMA and one occupational therapist.
The data were collected in Jordan after the Institutional Review Board at Jordan University of Science and Technology provided ethical approval for the study with reference numbers 26/97/2016, 7/103/2017 and 15/117/2018 and was performed in accordance with the ethical principles of the Declaration of Helsinki (The World Medical Association, 2013). The participants received written and oral information about the study. Subsequently, parental informed consent and child assent were obtained.
Instrumentation
The CHEQ consists of 30 items representing bimanual activities, divided into two age versions: the younger children version (3–8 years) containing 21 items, and the older children version (6–18 years) containing 27 items; the two versions share 18 items. Parents or caregivers can answer the CHEQ as a proxy, which is recommended for younger children, or together with the child. For each item, an opening question asks about the typical performance of the item: ‘Do you usually use one hand, both hands together, or get help?’ with three alternative responses ‘One hand’, ‘Both hands’ and ‘Get help — how does it work if you try for yourself?’ After answering the opening question, three questions ask about the child’s experience of using the hand in that activity: (1) ‘How do you think your hand works?’ (2) ‘How much time do you need to do the whole task, compared to peers?’ (3) ‘Does your hand function bother you in this activity/situation?’ A four-category rating scale with verbal anchors on each end is used for each question, allowing for responses to all items and a calculation of an overall measure for the child on each of the three CHEQ scales: Hand function, Time taken and Feeling bothered. More information can be found at www.cheq.se and in previous studies (Amer et al., 2016; Ryll et al., 2018; Skold et al., 2011).
Participants and procedure
Step 1. Cross-cultural adaptation
The translation and cross-cultural adaptation was conducted in four phases (Wild et al., 2005) (Figure 1). Phases of the cultural validation process of the Arabic Children’s Hand-use Experience Questionnaire (CHEQ).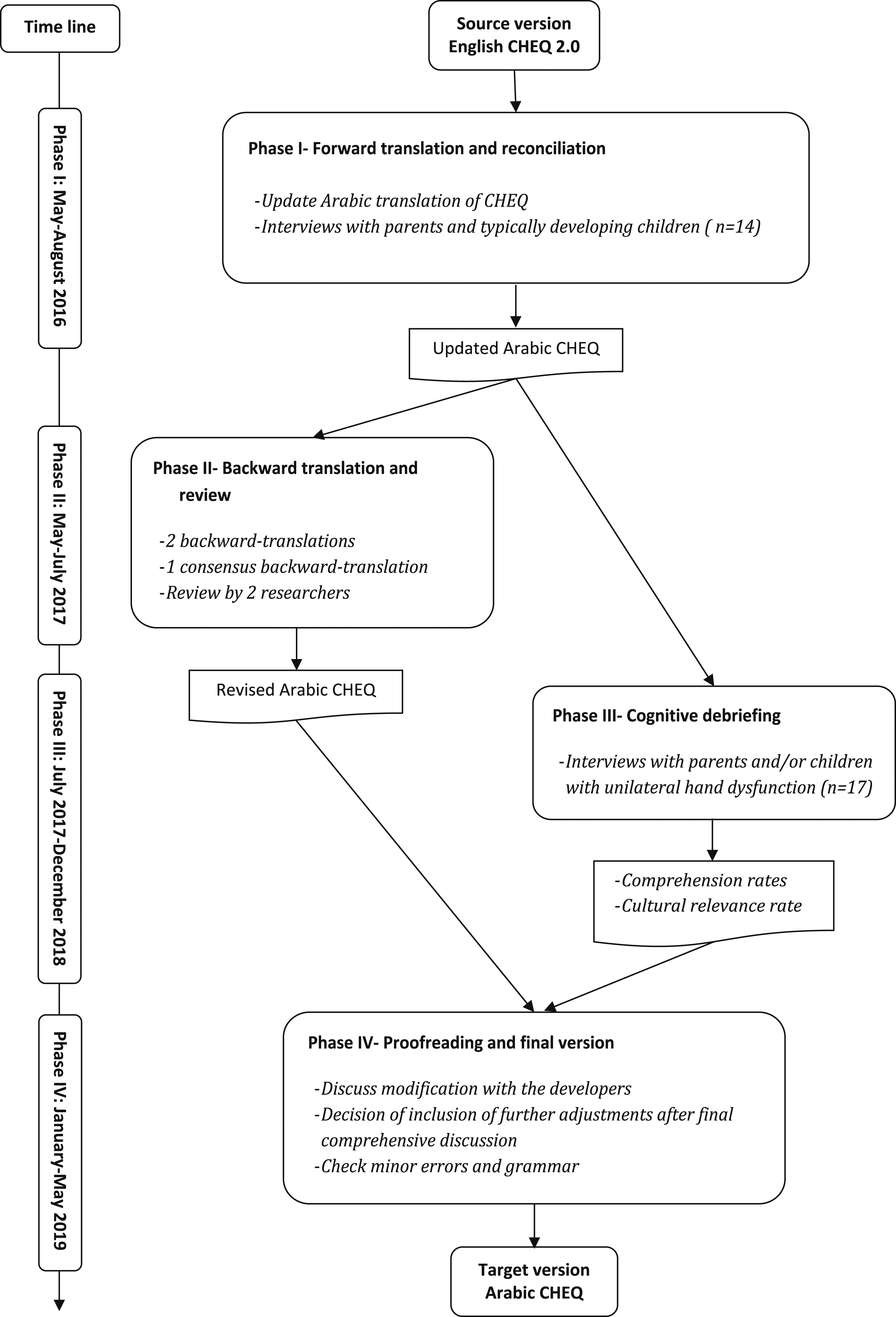
Descriptive information of the participating children and parents.
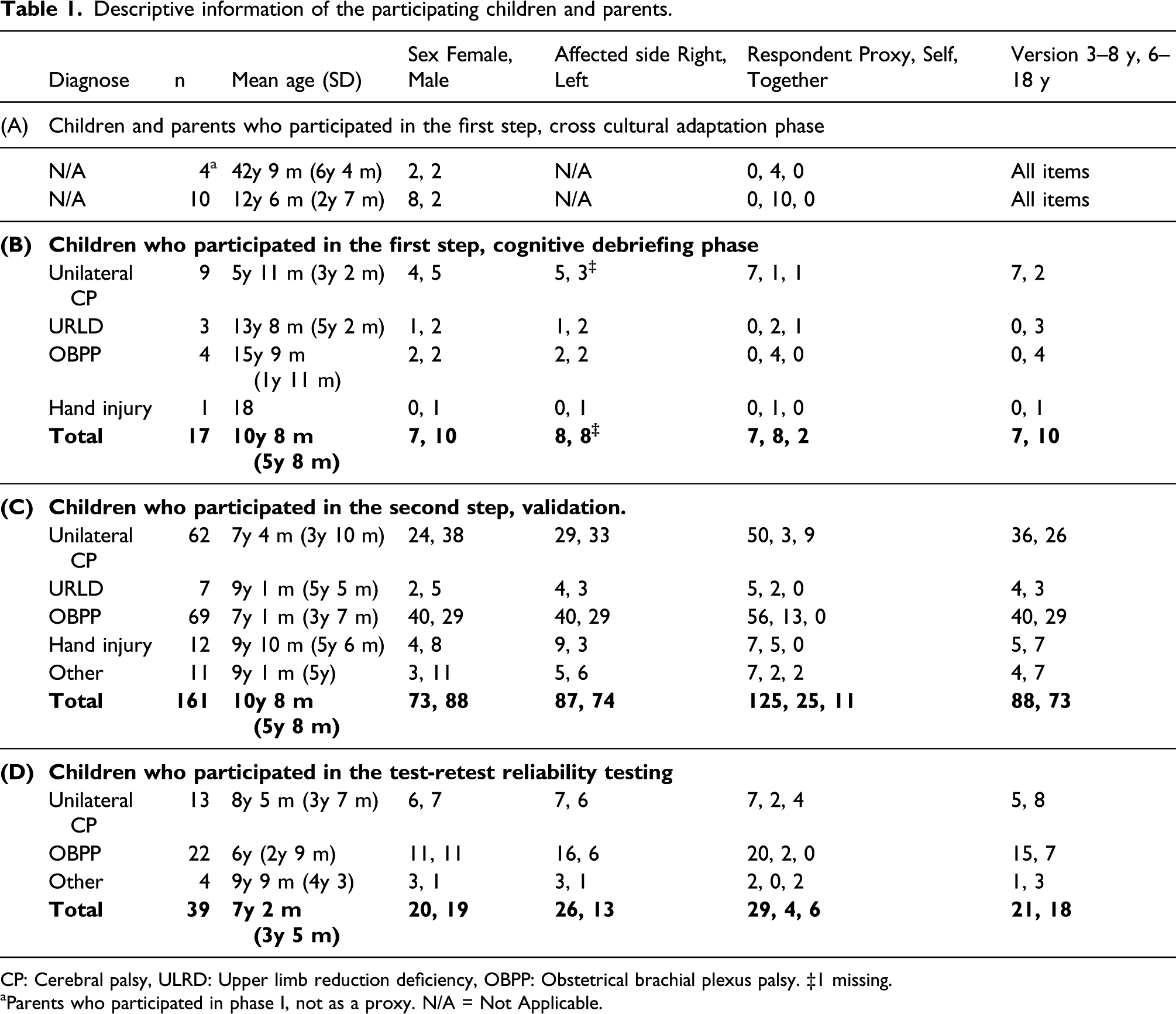
CP: Cerebral palsy, ULRD: Upper limb reduction deficiency, OBPP: Obstetrical brachial plexus palsy. ‡1 missing.
aParents who participated in phase I, not as a proxy. N/A = Not Applicable.
Phase II: The updated Arabic version was independently back-translated into English by two groups of researchers who were native Arabic speakers, fluent in English, and had no access to the original English version of the CHEQ.
Two other researchers, also native Arabic speakers and fluent in English, compared the semantic equivalence of the back-translated English version, the original English version and the updated Arabic version. Subsequently, the developers of the CHEQ (authors LH and A-CE) were consulted to help solve discrepancies between the versions.
Phase III: The updated Arabic version was tested to confirm semantic equivalence to the original and investigate its cultural relevance (Acquadro et al., 2008; Wild et al., 2005). Children with different types of unilateral hand dysfunction and their parents, who were able to read and understand Arabic, were recruited. In total, 17 subjects participated (Table 1B). After answering the CHEQ, the participants were interviewed individually, using a retrospective cognitive interviewing technique (DeMuro et al., 2012; World Health Organisation [WHO], 2015). They were asked to paraphrase each question, explain why they selected their answers, and report if any word or expression was unclear. Notes were taken during the interviews. The participants also filled in a table to mark the cultural relevance of each item. For each question and item, we calculated the proportion of respondents who paraphrased it correctly and the proportion of respondents who indicated that it was culturally relevant.
Phase IV: Revisions to the Arabic CHEQ were suggested and discussed with the original developers. This produced the target version of Arabic CHEQ.
Step 2. Psychometric testing
A convenience sample of 161 children in Jordan with different types of unilateral hand dysfunction answered the CHEQ to investigate its reliability (Table 1C). About 55% of the respondents answered the CHEQ 3–8 years version, and 78% of respondents were parents. To investigate test-retest reliability, 39 children and/or their parents answered the CHEQ again between 14 and 21 days later (Table 1D) (Shoukri et al., 2004).
Three tests were used:
(i) Internal consistency (homogeneity) among items under each CHEQ scale. The internal consistency test was performed for the shared items that all participants in both versions had answered (i.e. 18 items answered by 161 children), and for each age version separately (i.e. 21 items and 27 items answered by 21 and 18 children, respectively) by calculating Cronbach’s alpha coefficient. An alpha value >0.80 was desirable (Tappen, 2010);
(ii) Test-retest reliability for the total raw score of each CHEQ scale, for the shared items, and for each age version separately, was investigated by calculating the intraclass correlation coefficient (ICC) (two-way mixed effects model with absolute agreement) (Koo & Li, 2016). An ICC of 0.5-0.75 was considered as moderate, 0.75–0.9 as good and > 0.9 as excellent (Liljequist et al., 2019).
Finally, (iii) Test-retest reliability at the individual item level for each scale was investigated by calculating linear weighted kappa (κ) (Vanbelle, 2016). The κ was calculated for the 18 shared items (n = 39) and for each age version separately (n = 21 and n = 18, respectively). The strength of the agreement was interpreted as follows: poor agreement for κ≤0.40, fair to good agreement for κ between >0.40 and <0.75, and excellent agreement for κ ≥0.75 (Fleiss et al., 2003, P.598-626). SPSS version 25 was used to perform the statistical tests (IBM, 2017).
Results
Step I. Cross-cultural adaptation
Results from cross-cultural analyses of the Arabic version of the children’s hand-use experience questionnaire.
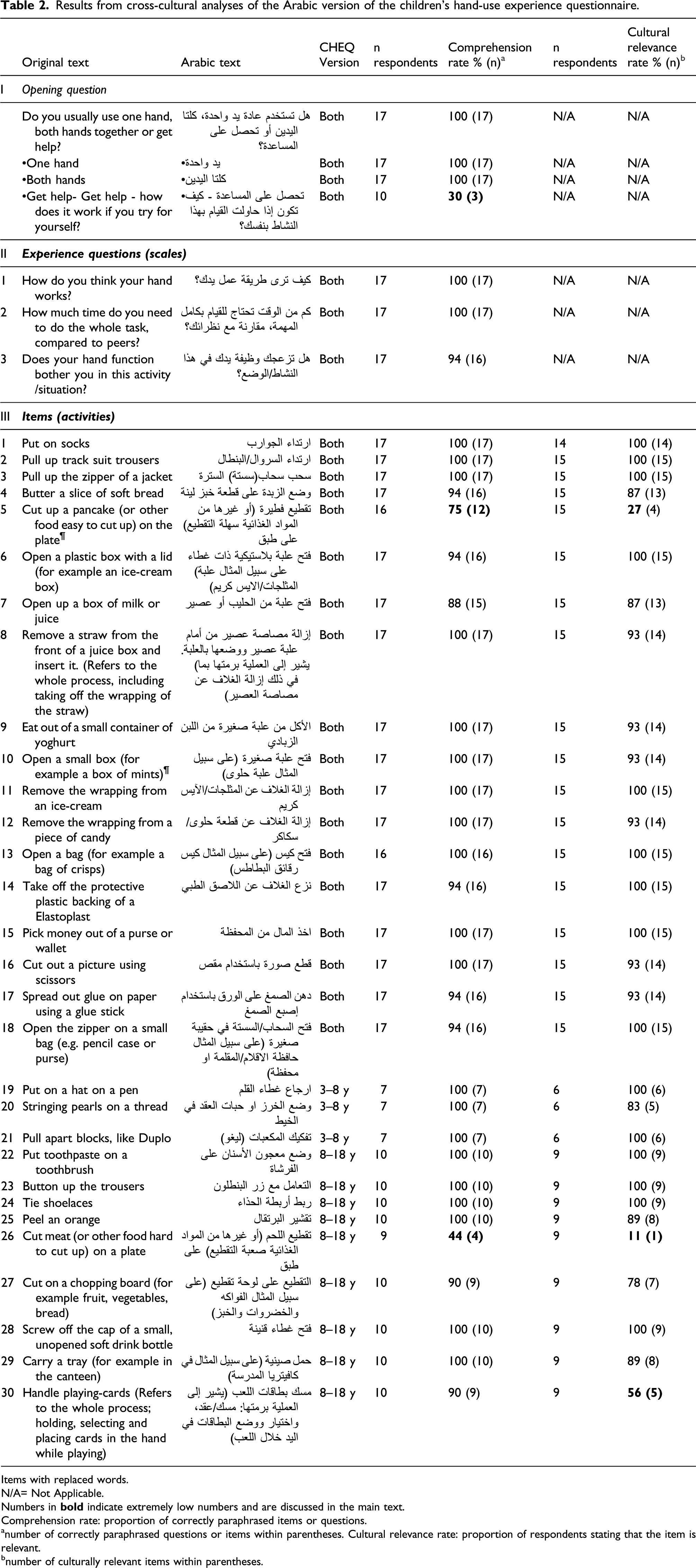
Items with replaced words.
N/A= Not Applicable.
Numbers in
Comprehension rate: proportion of correctly paraphrased items or questions.
anumber of correctly paraphrased questions or items within parentheses. Cultural relevance rate: proportion of respondents stating that the item is relevant.
bnumber of culturally relevant items within parentheses.
Phase II: Twenty-nine of the 30 items (97%) had retained their semantic meaning through the translation process. In one item, ‘Handle playing-cards....’, a change in semantic meaning was due to an incorrect forward-translation wherein the English word ‘handle’ had been translated to an Arabic word equivalent to ‘hold’. It was suggested to change the Arabic translation of the item to better reflect the meaning in the original English version.
Phase III: The comprehension rate of each item and question was between 20–100% (mean 93%), and the cultural relevance was considered high for 27 of the 30 items (78–100%, mean 90%) (Table 2). Comprehension and cultural relevance were lowest for the two items that involved the use of a knife and fork. The ‘Get help’ response alternative to the opening question showed low comprehension, and the item about handling playing-cards was reported as culturally irrelevant by four participants.
Phase IV: Suggestions were made to clarify the response alternative ‘Get help’ by adding further explanation to the Arabic CHEQ: ‘how do you evaluate your hand if you try performing this activity by yourself without help?’ Consequently, after proofreading and controlling for grammar errors, a target Arabic version of the CHEQ was suggested.
Step II. Psychometric testing
Internal consistency and test-retest reliability for the total raw score of the Arabic version of children’s hand-use experience questionnaire (CHEQ).
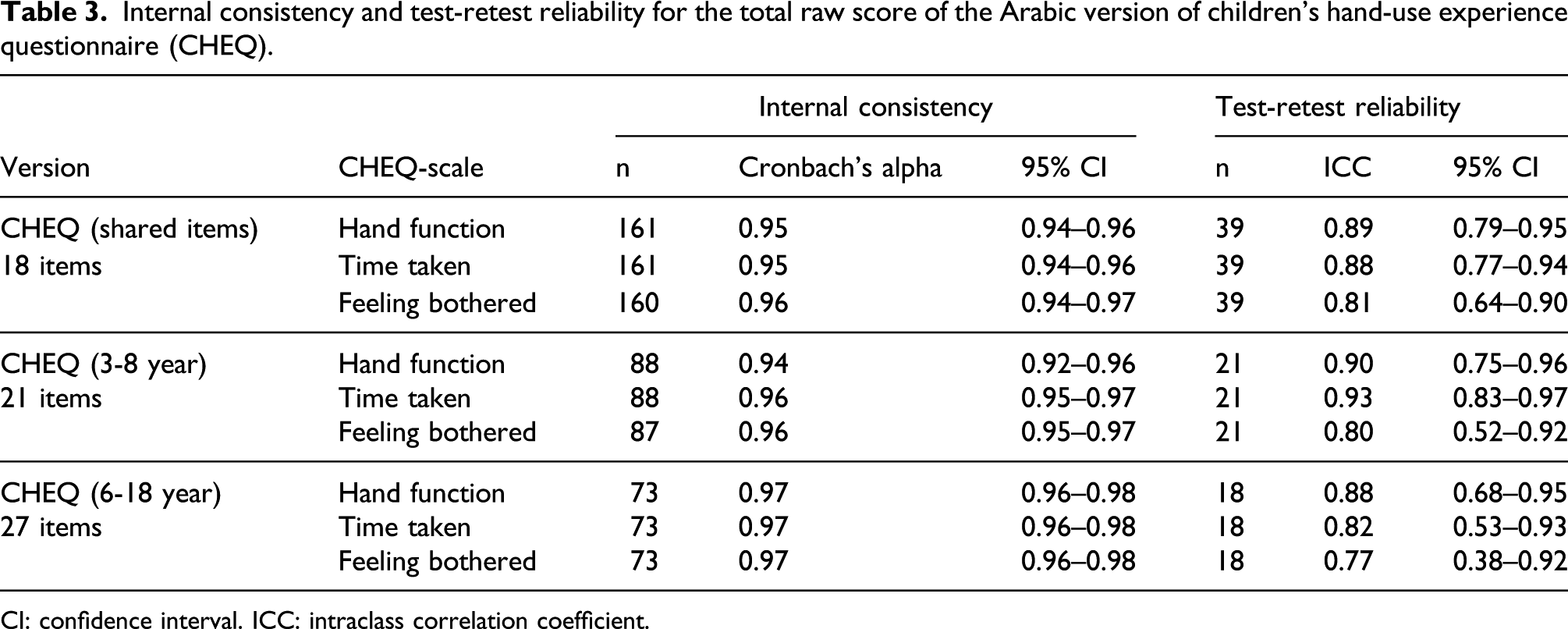
CI: confidence interval. ICC: intraclass correlation coefficient.
All CHEQ scales demonstrated total score test-retest reliability that was either good (ICC of 0.75-0.9) or excellent (ICC > 0.9). For the 18 items shared between the CHEQ age versions, ICCs ranged between 0.81 and 0.89 for the scales (Table 3). For the CHEQ (3–8 years), ICCs ranged between 0.80 and 0.93 and for the CHEQ (6–18 years), ICCs ranged between 0.77 and 0.88.
Test-retest reliability of individual items of the Arabic version of children’s hand-use experience questionnaire (CHEQ). (A) Items used in CHEQ (3–8 y) version only, n = 21. (B) Shared items between CHEQ’s age versions n=39. (C) Items used in CHEQ (6-18 years) version only, n = 18.
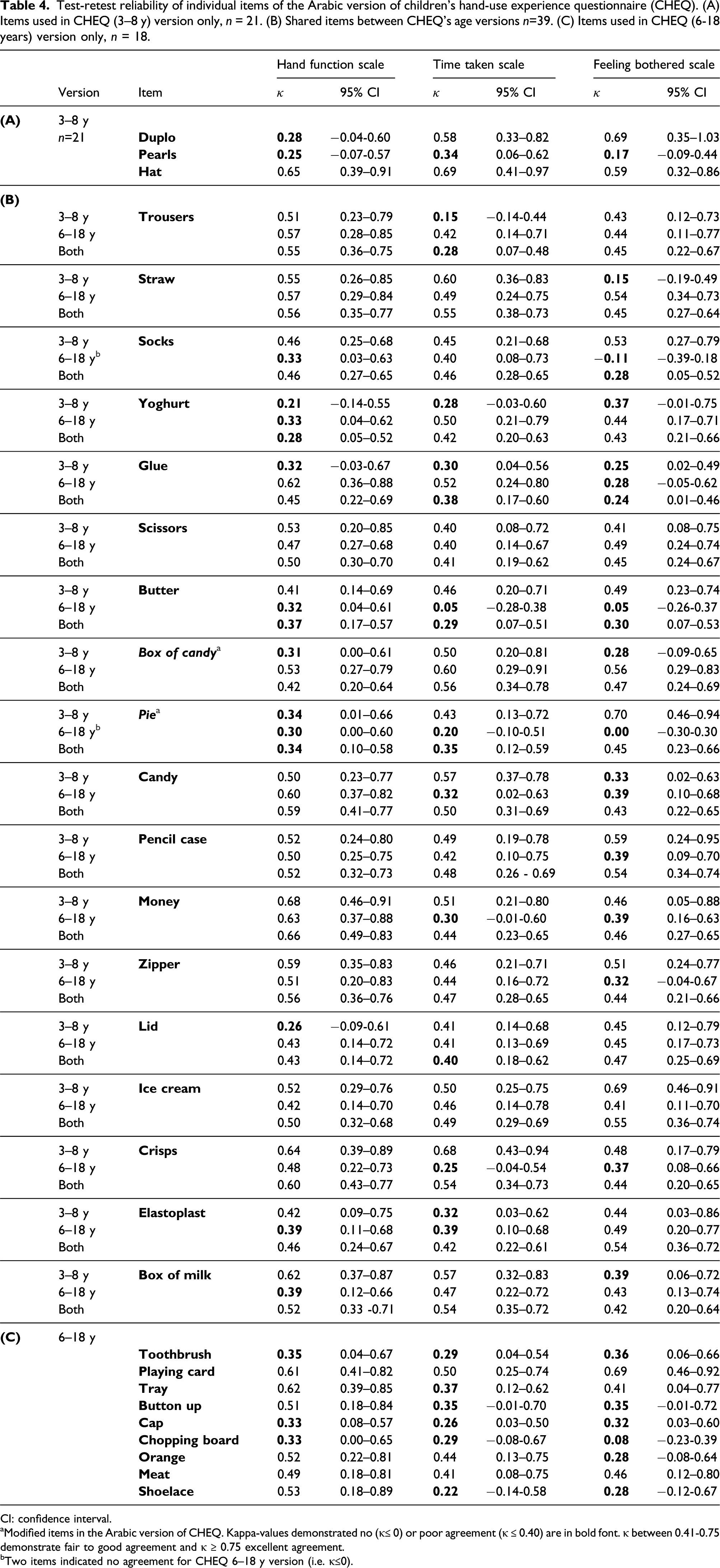
CI: confidence interval.
aModified items in the Arabic version of CHEQ. Kappa-values demonstrated no (κ≤ 0) or poor agreement (κ ≤ 0.40) are in bold font. κ between 0.41-0.75 demonstrate fair to good agreement and κ ≥ 0.75 excellent agreement.
bTwo items indicated no agreement for CHEQ 6–18 y version (i.e. κ≤0).
Discussion
This cross-cultural adaptation and validation of the Arabic CHEQ demonstrates that by minor but important adjustments, the Arabic CHEQ will be a comprehensible and reliable assessment for children with unilateral hand dysfunction in Jordan. This is supported by the high internal consistency and good test-retest reliability of the Arabic CHEQ.
We found high homogeneity between items (as measured with Cronbach’s alpha) in all CHEQ scales, suggesting that CHEQ can be used in clinical evaluation in Jordan (Tappen, 2010). This confirms previous results when using the CHEQ in other parts of the world (Amer et al., 2016). In accordance with a previous study (Amer et al., 2016), we found high test-retest reliability, especially of the total score. This supports the use of CHEQ for longitudinal follow-up of children’s habilitation service, also in Jordan.
Although the ICC demonstrated a satisfactory total score agreement between test occasions and several of the shared items demonstrated fair to good agreement when measured by kappa-statistics, other items demonstrated poor agreement. This may reflect the uncertainty of the answers for these items, given the small sample size. In fact, fewer items had poor agreement when analysing the whole sample compared to when analysing the items in the specific age versions separately. Future studies should use a larger sample size to increase the precision of the results and to allow agreement to be tested separately between the different age versions of the CHEQ (McHugh, 2012).
The low agreement in the seven items with enough power (i.e. 39 participants) could be due either to the definition of the item or the rating scale, that is, the respondents’ understanding of the item and rating scale, or variations within the person or the rater. This needs to be studied further.
During the translation process, we used modern standard Arabic that is understandable by almost all Arabic speakers owing to its use in the education system, media, and different state facilities in Arabic countries. However, certain words can be different from one region to another in the Arab world; therefore, we added synonyms of certain words to make the CHEQ usable in a larger Arabic-speaking population. Similar adaptations of items have been made when adjusting Arabic versions of other instruments (Guermazi et al., 2012; Meidany et al., 2003). Further, replacement of words, such as ‘mints’ with ‘candies’ in this study, has been done previously when adapting other instruments for use in Arabic-speaking countries (Guermazi et al., 2012; Sabbah et al., 2003) and Uganda (Kakooza-Mwesige et al., 2018). These adaptations may have contributed to the relatively high comprehension rate achieved.
The cultural relevance and comprehension of the CHEQ items was high for children and families living in Jordan. The main concern was related to different eating styles. Knife and fork are commonly used in Western countries, while people in Jordan traditionally eat without cutlery or with a spoon or fork in one hand while the other hand provides assistance without the use of cutlery. Nevertheless, some respondents seemed to understand the questions and responded accordingly, and the reliability scores for these items were fair. One suggestion to solve this discrepancy with cultural relevance is to replace the items while retaining the same intended meaning (Beaton et al., 2000), which was done, for example, in the Arabic version of the SF-36 (Meidany et al., 2003). However, we are unaware of any culturally relevant substitute daily life activity that can replace the use of a knife and fork while retaining the challenge that lies within the task. Hence, this discrepancy between eating habits needs to be taken in consideration in clinical use of the CHEQ in similar contexts. Despite a high comprehension rate, the cultural relevance was reported as low for playing cards. This might be because of religious influences in the Arabic culture forbidding gambling, which was not the intention with the item. Thus, we suggest adding an example of a family card game, such as UNO, to increase the cultural relevance of the item.
Another concern was the comprehension of the response option ‘Get help’ in the opening question. The explanation of this response, ‘how does it work if you try for yourself?’ may not suffice in the Arabic version, as extensive explanations may be needed in Arabic-speaking cultures to be understandable. Hence, an extended explanation is suggested to be added to the Arabic CHEQ.
Limitations and future suggestions
A potential limitation of the study was that the Arabic CHEQ was only tested in Jordan, and reliability of an instrument in one country does not necessarily mean that the instrument is reliable in other countries speaking the same language. The cultural context in Jordan is considerably close to other Arabic-speaking countries in the Middle East; hence, the results are likely to be generalizable to other countries in this region, but this needs to be confirmed in future studies that include other Arabic speaking countries. Another limitation was that the sample size was too small for investigating test-retest reliability in the two age versions separately, resulting in wide confidence intervals for ICCs and kappa-values. Future studies should investigate test-retest reliability of the Arabic CHEQ versions using a larger sample allowing for separate analyses of each version.
The results of using the CHEQ with younger children are reported here for the first time. Through the suggested adaptations, the Arabic version of the CHEQ will be comprehensible and reliable for assessing children with unilateral hand dysfunction in Jordan. Further studies are needed to investigate other psychometric properties of the Arabic CHEQ in more depth, including, but not limited to, validity evidence such as response patterns, sensitivity to change, and differential item functioning across patient groups, different Arabic-speaking countries and other cultures.
Footnotes
Acknowledgements
We would like to thank the children and their parents who participated in this study. We also thank the participating units (Rehabilitation departments at King Hussein Medical Centre and Al Bashir Hospital, Cerebral Palsy Foundation, The University of Jordan and King Abdullah University Hospital). Special thanks to members of the back-translation team for their valuable participation and input in the back-translation process. We would like to thank Dr. Nihad Almasri for the logistic support for data collection and Hadeel Al-Hadidi for her help with data collection.
Data availability statement
The data that support the findings of this study are available on request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Norrbacka-Eugeniastiftelsen [grant 803/18]; Riksförbundet för Rörelsehindrade Barn och Ungdomar; Folke Bernadotte stiftelsen; The research committee, Region Örebro County; and, Örebro University under Strategic Grants 2019 (awarded for REAL research environment). The investigation was partially supported by the Faculty Scientific Research at Jordan University of Science and Technology, Irbid, Jordan, [grant number MA 84/2017].