
Abstract
Objective/Background
Occupational therapists usually assess hand function through standardised tests, however, there is no consensus on how the scores assigned to hand dexterity can accurately measure hand function required for daily activities and few studies evaluate the movement patterns of the upper limbs during hand function tests. This study aimed to evaluate the differences in muscle activation patterns during the performance of three hand dexterity tests.
Methods
Twenty university students underwent a surface electromyographic (sEMG) assessment of eight upper limb muscles during the performance of the box and blocks test (BEST), nine-hole peg test (9HPT), and functional dexterity test (FDT). The description and comparison of each muscle activity during the test performance, gender differences, and the correlation between individual muscles’ sEMG activity were analysed through appropriate statistics.
Results
Increased activity of proximal muscles was found during the performance of BEST (p < .001). While a higher activation of the distal muscles occurred during the FDT and 9HPT performance, no differences were found between them. Comparisons of the sEMG activity revealed a significant increase in the muscle activation among women (p = .05). Strong and positive correlations (r > .5; p < .05) were observed between proximal and distal sEMG activities, suggesting a coordinate pattern of muscle activation during hand function tests.
Conclusion
The results suggested the existence of differences in the muscle activation pattern during the performance of hand function evaluations. Occupational therapists should be aware of unique muscle requirements and its impact on the results of dexterity tests during hand function evaluation.
Keywords
Introduction
Hand and upper extremity function is essential to humans as it allows for the performance of a wide range of self-care, productive, and leisure activities (
Treating patients with hand and upper limb injuries is a common situation for occupational therapists; hand and wrist lesions account for approximately 20% of all cases seen in hospital emergency departments (
Although the cause of injury varies in different countries (
Assessment procedures that allow occupational therapists to obtain accurate and reliable information regarding patients’ hand function are essential for setting realistic goals and measuring patients’ progression during the rehabilitation of upper limb injuries (
Despite focusing on the measurements of body functions and structures, standardised dexterity tests provide valid and reliable data that aids therapists in understanding the impact of hand injuries on patients’ activities of daily life. Commonly used standardised tests have high inter-rater and test-retest reliability, usually with an intraclass correlation coefficient (ICC) greater than 0.85 (
However, given the existence of multiple standardised dexterity tests and an even greater variety of structured tasks involved in each assessment, there is no consensus on which test is more suitable for evaluating the entire function of upper extremities (
The study of muscle activation through surface electromyography (sEMG) allows a real-time, noninvasive assessment of the activation pattern of muscles during the activity performance (
Considering the lack of studies describing the muscle activities of the upper extremities in standardised hand assessments, this study aimed to evaluate and compare the differences in muscle activation patterns during the performance of the box and blocks test (BBT), nine-hole peg test (9HPT), and functional dexterity test (FDT)—the three hand dexterity tests used by occupational therapists during hand function evaluation.
Methods
Participants
A convenience sample of 20 university students, aged 18–30 years, participated in this nonexperimental, descriptive, and cross-sectional study. These students were invited to participate through institutional e-mail or phone call. Participants were undergraduates in mechanical engineering, civil engineering, and occupational therapy, however, undergraduates in physical education and music were excluded because they could have specific upper limb-related skills, like dexterity, that could confound the results. Participants included were exclusively right handed, had no history of pain, discomfort, trauma, or sequelae relating to the upper extremities, and had no familiarity with hand dexterity tests.
Participants who had a body mass index (BMI) of 30 kg/ m2 or more, used medications, or who performed excessive exercise 72 hours before the evaluation were excluded from the study as these factors potentially interfere with the collection of sEMG signals (
The study was approved by the ethics committee of the proposing institutions, and all participants were informed about the experimental procedures and asked to provide a written consent prior to the experiment.
Instrumentation
Hand Dexterity Tests
Three hand dexterity tests were selected for this study, BBT (
BBT consists of repeatedly moving 2.5-cm wooden cubes from one box to another when the boxes are placed side by side (
FDT involves the grasping and manipulation of 16 wooden pegs, measuring 2.2 cm in diameter and 4 cm in length, that are placed in a 21 cm2 shardwood board (
Similar to FDT, 9HPT measures hand dexterity by placing wooden pegs in a pegboard as fast as possible. The test uses thin, 7-mm diameter pegs, and also considers the removal of pegs as a part of the evaluation (
The selection of the three tests was based on the type of motor tasks required by each instrument to measure hand dexterity, in accordance with the categorisation proposed by
We selected BBT based on its use in studies investigating hand and upper extremity function in acute and chronic conditions (
Despite being classified as pegboard tests, FDT and 9HPT require different movement patterns during test performance (
Electromyography Equipment
The New MioTool Wireless® (Miotec Biometric Equipment –Porto Alegre, Rio Grande do Sul, Brazil), an 8-channel system with a common mode rejection of 126 db and amplification to a gain of 1000, was used to collect the sEMG data. Signals were conditioned with a digital band-pass filter between 10–500 Hz and a 60-Hz notch, with a 14-bit analog to digital conversion at a sampling frequency of 1000 Hz, and sensors with entry impedance of 1010 Ω.
Disposable, bipolar Ag/AgCl surface electrodes with a 15 mm diameter and 20 mm inter-electrode distance (3M Healthcare, Sumaré, SP, Brazil) were used. Electrodes were fixed to the skin of participants with Micropore (3M Healthcare, Sumaré, SP, Brazil) and custom-made, low-compression elastic tape, to reduce the signal interference caused by the movement of sensors.
Anthropometric data was obtained through a digital scale with 150 kg capacity and a 100-g interval (Filizola —Sao Paulo, SP, Brazil). A vertical stadiometer was fixed to the scale to measure participants’ height in centimetres. Additionally, the JAMAR Hydraulic Hand Dynamometer (Patterson Medical Holdings, Inc., — Warrenville, IL - USA) was used to measure the flexor digitorum superficialis’ (FDS) maximum voluntary contraction.
Electronic placement
Muscles selected for this study were located by palpation during voluntary contraction. Portions of each participant's skin directly over the muscle bellies of the muscles were shaved and carefully cleaned to reduce the contact impedance (
Muscle selections were based on the actions of proximal and distal muscles during upper extremity movement (
Selected Muscles and Electrode Positioning.
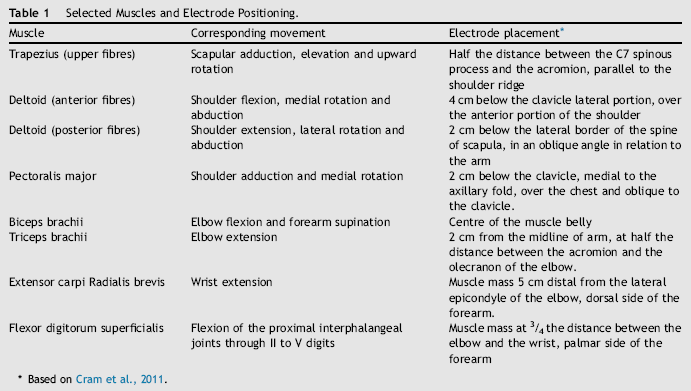
Based on
Distal muscles, the Extensor Carpi Radialis Brevis (ECRB) and the Flexor Digitorum Superficialis (FDS), were selected according to their functions in wrist and finger movements and due to their functions in wrist positioning (
Procedures
We selected a convenience sample of 10 male and 10 female students from undergraduate and graduate courses at a public university in Brazil. They were invited to participate through an institutional e-mail address or phone call. Participants were contacted before data collection to explain the research requirements (no exercise and use of medications 72 hours before the experimental procedure). All the procedures necessary for data acquisition were conducted on the same day, in an acclimatised environment, with sessions scheduled to allow the use of natural light to reduce the interference of electrical equipment with the sEMG signal.
First, 1 hour prior to the data acquisition, the electrodes were placed and the maximum voluntary contraction (MVC) of each muscle was obtained. For each muscle, participants were asked to perform three repetitions of maximum isometric contraction under manual resistance for 10 seconds, with a 2-minute interval between each attempt. To obtain the MVC of the FDS, we used the JAMAR hydraulic hand dynamometer (Patterson Medical — Warrenville, Illinois, United States of America), in accordance with the American Society of Hand Therapists guidelines (
The arithmetic mean of the three attempts, expressed in microvolts, was calculated and used as a reference representing 100% of the muscle sEGM activity (
After obtaining the MCV, participants were instructed to perform the hand dexterity tests. The order of the tests was randomised by drawing pieces of paper with the test names from an opaque paper bag. The hand dexterity tests were placed on a wooden desk (120 cm x 60 cm) at a height of 100 cm (

Experimental setting. (A) Box and blocks test; (B) Nine-hole peg test; (C) functional dexterity test.
Each test was performed five times, with a 30-second rest between each repetition. A chronometer was used to record the 60 seconds of each BBT repetition and the time required for participants to complete the 9HPT and FDT. The arithmetic mean of the sEMG signal obtained during the five repetitions for each test was calculated, and a final value expressed in microvolts was obtained for each muscle. The values were normalised according to the MVC obtained previously, and the final data regarding the muscle activation pattern was expressed as a percentage of the MVC.
Data analysis
Descriptive statistics were used to calculate participants’ mean age, BMI, and the mean percentage of the MVCs for each muscle during performances of the BBT, 9HPT, and FDT.
Data was assessed for normality through the Shapiro–Wilk test, which showed a non-normal distribution for the sEMG activity of the selected muscles between participants. The Friedman test was used to compare the normalised muscle activity patterns observed in each test and a post hoc analysis was conducted using individual Wilcoxon signed rank test with a Bonferroni-adjusted alpha value.
To investigate the existence of differences in sEMG activity between male and female participants, the Mann–Whitney test was used to compare the MVC percentage of the eight muscles during the performance of the three hand function tests between sexes. Additionally, the relationship between the activation patterns of the evaluated muscles during the hand dexterity tests were investigated using the Spearman rank order correlation. The SPSS software version 20.0 was used for all data analysis, with a significance level set at .05.
Results
Participants’ demographics
Participants’ mean age was 24.2 (± 3.4) years and average BMI was 23.6 (± 2.8). The mean anthropometric data for female participants was a height of 1.6 m (± 5 cm) and a weight of 60.3 kg (± 7.56 kg), with the average height of 1.75 m (± 5 cm) and 72.6 kg (± 9.6 kg) amongst male participants (
Participants’ Demographic Data.
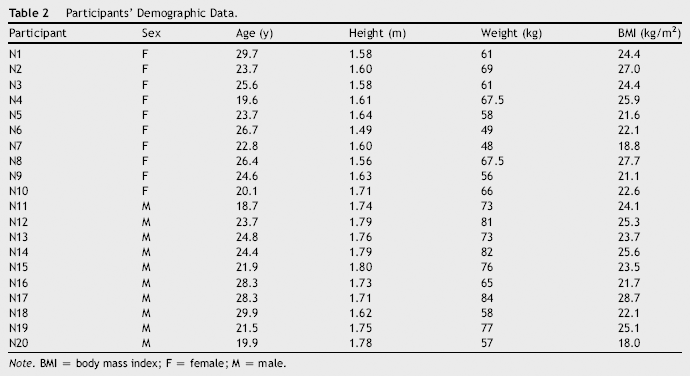
Note. BMI = body mass index; F = female; M = male.
sEMG activity during hand function tests
Changes in the muscle activation were observed when comparing the mean sEMG activity of the three tests (
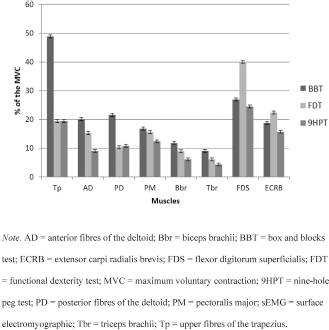
sEMG activity during the performance of the three hand dexterity tests.
Post hoc analyses of muscle activation patterns obtained using individual Wilcoxon signed rank test revealed a significant increase in the activation of the Tp, AD, PD, PM, and Tbr sEMG activity during the performance of BBT when compared to FDT and 9HPT (p < .001), indicating an increase in the activation of proximal muscles during BBT.
Despite the similarities between the two pegboard tests, no differences were observed in muscle activation when comparing FDT with 9HPT, suggesting that the muscle recruitment pattern and the motor strategies involved in the performance of both tests may be similar.
Comparisons of the sEMG activity between the sexes revealed significant differences in muscle recruitment. During the BBT performance, female participants presented an increased activity of the AD, PM, Bbr, Tbr, and ECRB muscles. Increased muscle activation was also observed in the PD, PM, Bbr, Tbr, and ECRB among female participants performing the 9HPT, with a similar activation pattern observed with the FDT results (
Comparison of Mean sEMG Activity—Female and Male Participants.
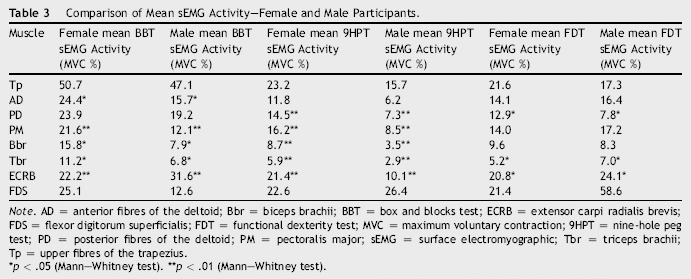
Note. AD = anterior fibres of the deltoid; Bbr = biceps brachii; BBT = box and blocks test; ECRB = extensor carpi radialis brevis; FDS = flexor digitorum superficialis; FDT = functional dexterity test; MVC = maximum voluntary contraction; 9HPT = nine-hole peg test; PD = posterior fibres of the deltoid; PM = pectoralis major; sEMG = surface electromyographic; Tbr = triceps brachii; Tp = upper fibres of the trapezius.
p < .05 (Mann–Whitney test).
p < .01 (Mann–Whitney test).
Correlation between the sEMG activities of the selected muscles suggests different patterns for each test. During BBT, a significant, strong, and positive correlation (p < .05; r > .5) was observed between the recruitment of the AD, PM, and TBr. The same correlation was observed between the PM, TBr, and FDS muscles, suggesting a coordinated function of these muscles during the reaching activities required by the test (
Spearman Correlation Coefficient (rho) for the sEMG Activity of Selected Muscles during Hand Dexterity Tests.
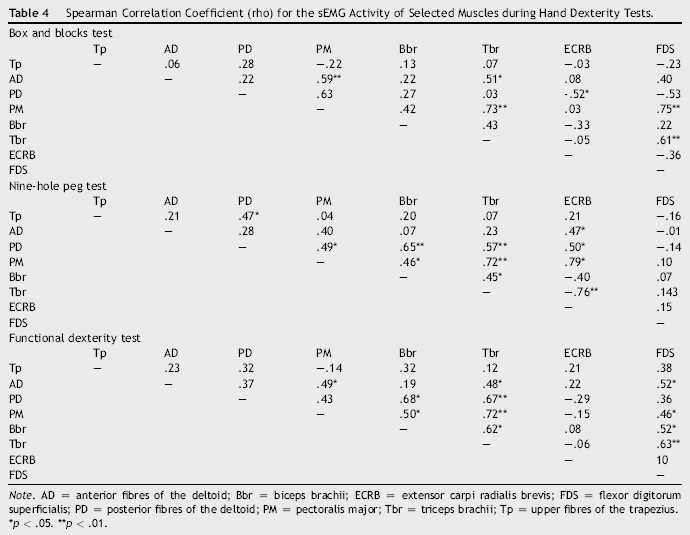
Note. AD = anterior fibres of the deltoid; Bbr = biceps brachii; ECRB = extensor carpi radialis brevis; FDS = flexor digitorum superficialis; PD = posterior fibres of the deltoid; PM = pectoralis major; Tbr = triceps brachii; Tp = upper fibres of the trapezius.
p < .05.
p p < .01.
The correlation of the muscle activation during the 9HPT indicated a coordinate activation of the PD, Bbr, TBr, and ECRB. Although a similar pattern of strong and positive correlations between proximal muscles was observed when analysing the sEMG activity of the FDT, significant correlations were also found between FDS and the AD, PM, Bbr, and Tbr.
This muscle activation pattern could be explained by the finger motions required for the FDT performance, in addition to the reaching movements.
Discussion
The present study measured the sEMG activities of eight muscles in the upper extremities during three hand function tests. Although the three tests selected for this study aimed to measure the hand dexterity and function, important differences in the muscle activity were observed. An increased activity of proximal muscles was found during the performance of BBT, whereas a significantly higher activation of the distal muscles occurred during FDT and 9HPT, with no differences between them.
The results indicate the varying influence that different tasks have on muscle activity, which based on the objectives of clinical assessment, can impact test selections. As previously presented by
In contrast to the muscle activity observed during the BBT performance, 9HPT and FDT did not show significant activation of the proximal muscles. In both the tests, the Tp, AD, PD, PM, BBr, and TBr showed an activation of less than 20% of the MCV, suggesting a stabilising action of the proximal muscles during the performance of FDT and 9HPT (
Similar results were observed in studies that aimed to analyse fine motor skills using sEMG.
Differences in the sEMG activity of male and female participants were also reported by other studies.
Although not significant, an increased sEMG activity, expressed in a higher percentage of the MVC, was observed in women during a hand stabilisation test (
A positive correlation between the activation of individual muscles was observed in the three hand function tests. A similar pattern of activation of the Tp, AD, and TBr was observed by
In addition, significant correlations in the range of motion of the upper extremity joints were also found during reaching and grasping tasks by using kinematic analysis (
This study had several limitations. A small sample size can influence the generalisation of the results. Although there were only 20 participants, this number of participants conforms to the studies using electromyography as an evaluation method. In this study, we did not evaluate the sEMG activity of the intrinsic hand muscles. Although the thenar and lumbricalis muscles have a fundamental role in fine hand movements, the authors believe that the presence of electrodes and the materials necessary for its proper fixation at the palm of the hand would influence the movements used to complete the hand function assessment. The sEMG activity of intrinsic hand muscles and its relation with proximal muscles should be investigated in future studies.
Conclusion
The results of the sEMG of the eight muscle groups, measured during three standardised functional tests, indicated that the proximal muscles were more active during BBT, whereas FDT and NHPT activated more distal muscles and had no significant statistical differences between them.
Women showed a higher percentage of muscle activation than men; this result may be justified by different neural activation strategies used by each sex. The research may contribute to the evaluation processes used in occupational therapy and strengthens the recommendation to use such tests to evaluate the functions of the upper limbs.
The results suggest the existence of differences in the muscle activation pattern during the performance of hand function evaluations. Occupational therapists should be aware of unique muscle requirements and its impact on the results of dexterity tests during evaluation.
Footnotes
Acknowledgments
This research received financial support from CAPES (Coordenação de Aperfeiçoamento de Pessoal de Nível Superior).