
Abstract
Background/Objectives
Self-efficacy is a key component in mental health recovery and improvement in well-being. Mental illness is often resultant of environmental stressors, highlighting the importance of coping skills. Occupational therapists commonly utilise activity-based group therapy to encourage use of activities as coping strategies. However, there has been little research concerning these groups and their role in enhancing self-efficacy in behavioural-based coping skills. This study aimed to explore factors that affect behavioural-based coping self-efficacy during activity-based group therapy in an acute mental health ward. It investigates the relationships between (1) behavioural-based coping self-efficacy with overall mental health self-efficacy and (2) mental health self-efficacy and subjective well-being.
Methods
Immediately after the first group, participants completed a post-group questionnaire. Participation level was also rated. At discharge, the participants were asked to complete the UK Office of National Statistics subjective well-being tool and the Mental Health Self-Efficacy Scale. Descriptive statistics, independent sample t-tests and one-way analysis of variance were done to examine possible covariates and confounders of all outcome variables. General linear models were then conducted.
Results
Post-group questionnaire reflected moderate-high self-efficacy (M = 6.92, SD = 2.48) and positive well-being with higher happiness scores (M = 7.42, SD = 2.20) and lower anxiety scores (M = 3.79, SD = 2.85). Coping self-efficacy significantly predicted overall mental health self-efficacy (p = .014), which in turn significantly predicted positive domains of well-being.
Conclusions
Performing behavioural-based coping strategies in groups can enhance coping self-efficacy and positive well-being, with possible positive influence on mental health self-efficacy and well-being at discharge.
Introduction
In contemporary psychiatric literature, recovery in mental illness is described as an individualized journey of self-discovery and personal empowerment (Jacob, 2015). As such, it is common for recovery-oriented services to focus clients on their own recovery plans and coping strategies. However, it is critical to identify barriers and facilitators in actualizing their recovery plans, as individuals may not persist with their plans if they do not believe they can succeed.
Self-efficacy is the belief that one can successfully carry out specific behaviour in situations that are novel or stressful (Bandura, 1997). This is one of the key factors in facilitating the recovery process (Brenninkmeijer et al., 2019). Higher levels of self-efficacy have also been associated with fewer depressive symptoms (Maciejewski et al., 2000), and less stress and anxiety (Benight & Bandura, 2004). Positive perceptions of individual self-efficacy can influence emotional reactions and associated biological systems that regulate well-being, further improving mental health (Bandura, 1986). Studies on mental health programmes also found intervening on self-efficacy improved subjective well-being (Carpinello et al., 1992; Rosenfield, 1992).
During a relapse, disengagement from pleasurable and challenging activities are common. Disengagement reduces the opportunity to persevere through and succeed in significant life situations, which are critical in maintaining a sense of self-efficacy (Miilanovic et al., 2018). Deteriorated self-efficacy further perpetuate disengagement from daily activities, and contribute to feelings of hopelessness and passivity, which have been reported to negatively influence one’s sense of well-being (Rosenfield, 1992). Therefore, development of self-efficacy may be key, by enabling persons with mental illness to persist in challenging situations, utilising coping strategies and re-engaging in pleasurable and meaningful activities (Bandura, 1997).
Coping strategies are defined as cognitive and/or behavioural efforts to manage external and/or internal demands that are appraised as exceeding the resources of the person (Lazarus & Folkman, 1984). Cognitive coping strategies uses mental activity to manage thoughts or emotions associated with the stressful event, whereas behavioural coping strategies use overt physical or verbal activities. Learning and implementing coping strategies to manage stress can potentially decrease the risks of negative affective states and relapse episodes (Silverman, 2019). Each individual tends to cope in a variety of ways (Thompson et al., 2008), and it has been suggested that no single coping strategy is efficient across all situations for all people (Thoits, 1995). However, people with mental illness often need assistance to identify healthy coping strategies (Silverman, 2019). Regardless of specific coping strategies, interventions designed to increase coping behaviours have been found to be effective (Bradshaw, 1993).
In the study on the effect of stress, self-efficacy has been identified as a coping resource (Pearlin et al., 1981). As self-efficacy is a dynamic construct, it can be modified by interventions focused on the four sources of self-efficacy (Bandura, 1997). The first and most important is the experience of personal mastery, which means one’s own experience in successful completion of tasks. The second is vicarious experience. When others like oneself successfully complete a task, they act as social models and reinforce one’s ability to do likewise. Third is verbal persuasion, when others encourage and reinforce one’s ability. Fourth is physiological factors, when people interpret their ability based on their own physiological and affective states during performance. These factors reflect that self-efficacy can be determined by social factors (Anderson et al., 2014), and the importance of social contextual variables such as modelling and group support (Bandura, 1997) in improving self-efficacy.
In mental health settings, group therapy is often a core occupational therapy intervention. These are often activity-based groups (Lloyd et al., 2002), as occupational therapists recognise the therapeutic value of activities in improving overall function, performance, and psychological well-being (Creek, 2014), and found to be beneficial for people living with psychiatric illness (Kirsh, et al., 2019). A wide range of creative activities can be selected for these groups as comparison between different interventions indicate that none is more effective than the other (Kirsh et al., 2019). While the objectives of activity-based groups may vary according to the needs of patients, they often focus on facilitating participants to explore using activities as coping strategies in managing their mental health. These activities form behavioural coping strategies in recovery, leading to better psychosocial functioning. In a study involving music group therapy, inpatients in an acute care mental health ward tended to have more favourable coping self-efficacy as compared to the control group (Silverman, 2019). Eklund (1999) examined the effects of an occupational therapy intervention involving creative activities, and results showed that the intervention group experienced greater improvements in psychological, occupational functions and global mental health.
Although activity-based group therapy is commonly used in acute mental health wards, there has been little research concerning how this type of group interventions may influence coping. Furthermore, while the importance of nurturing self-efficacy in people with mental illness is well-recognised, few studies have investigated using activity-based groups to enhance self-efficacy in behavioural coping strategies.
A domain-specific construct (Bandura, 1994), self-efficacy in this context, termed as coping self-efficacy, is defined as the degree of confidence patients have in their ability to use specific activities performed in the group as coping strategies, in maintaining their mental health. Whereas, general self-efficacy, termed as mental health self-efficacy in our study, refers to confidence in one’s general capacity to handle tasks (Bandura, 1994). Therefore, coping self-efficacy can be conceptualised as a subset of mental health self-efficacy.
Therefore, the purpose of this study was twofold. Firstly, we explore factors that affected coping self-efficacy during activity-based group therapy in an acute mental health ward. Secondly, we investigate the relationships between (a) coping self-efficacy with mental health self-efficacy and (b) mental health self-efficacy and subjective well-being. We hypothesise that there is a positive association between (a) coping self-efficacy and mental health self-efficacy, and between (b) mental health self-efficacy and subjective well-being.
Methods
Study design and setting
This exploratory cross-sectional observational study was conducted at an acute psychiatric ward in a large tertiary hospital in Singapore. As part of the daily ward milieu, patients were referred for activity-based group therapy if they were able to participate in activities for at least 15 minutes, with minimal to moderate assistance and did not display persistent symptoms that were harmful or disruptive to their peers. Although patients were strongly encouraged to attend group therapy, participation was voluntary.
Activity-based group therapy sessions (Figure 1) were facilitated by an occupational therapist and therapy assistant for 1 hour, every weekday morning. The group format was open, where new participants may join or leave at any time, and the group was structured based on Cole’s seven steps of group interventions, including introduction, main activity, sharing, processing, generalization, application and summary (Cole, 2017). Examples of activities during group therapy.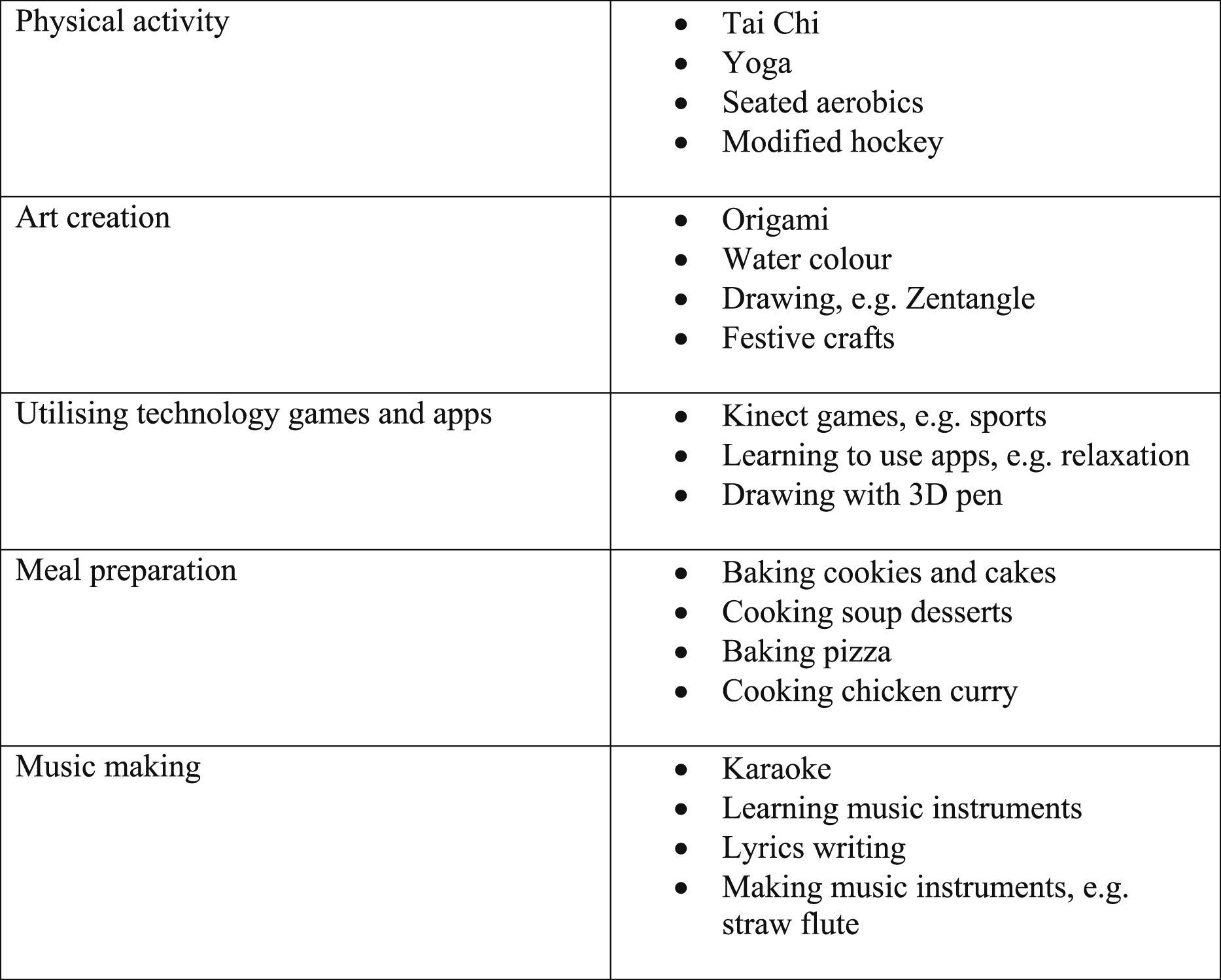
Participants
Fifty participants were recruited via convenience sampling at their first group therapy session. Participants were included if they were at least 21 years old, had a primary diagnosis of a psychiatric disorder, able to read and speak English and able to complete the questionnaires. Written informed consent was obtained from participants. Participants were compensated with a small token sum of cash vouchers for their participation in the study.
Ethical consideration
Ethics approval (number: 2017/00349) was obtained from the National Healthcare Group Domain Specific Research Board (NHG DSRB).
Instruments
Post-group questionnaire
The post-group self-report questionnaire was developed for the purpose of this study. It included a section on sociodemographic information and three questions to measure (1) coping self-efficacy, (2) mood and (3) anxiety after participation in each group (Figure A1). The coping self-efficacy question was based on Bandura’s (2006) recommendation, that there is no all-purpose self-efficacy scale, and scales should be tailored to the specific domain of interest. Questions on mood and anxiety were developed based on the Organisation for Economic Co-operation and Development (2013) recommendation that a minimum of two questions, with one of positive affect, and another of negative affect, should be used to measure subjective well-being. An 11-point Likert scale where 0 is ‘not at all’ and 10 is ‘completely’, was selected as it consistently demonstrated the smallest levels of missing data across multiple surveys in literature (Courser & Lavrakas, 2012). All items were analysed separately.
Pittsburgh rehabilitation participation scale
The Pittsburgh Rehabilitation Participation Scale (PRPS) is an observational clinician-rated measure of patient participation in inpatient rehabilitation sessions. It is a single item measure with a 6-point Likert-type scale (Lenze et al., 2004). The therapist assesses the intensity of participation from 1 to 6, where 1 is ‘None’ and 6 is ‘Excellent’. PRPS is found to be a reliable and valid therapist-rated measure, with high interrater reliability (ICC = 0.91) for occupational therapists (Lenze at al., 2004).
UK office of national statistics subjective well-being tool
Office of National Statistics (ONS) is a self-report questionnaire which measures subjective well-being, based on the three concepts of well-being: life evaluation, affect and eudemonia. ONS has conducted a range of quantitative and qualitative testing on the measurement of subjective well-being and the four questions has gained National Statistics status (Office of National Statistics, 2015). The questionnaire contains four items that are answered on a scale of 0 to 10, where 0 is ‘not at all’ and 10 is ‘completely’. For the Life Satisfaction, Worthwhile and Happiness questions, scores are categorized as low (0 to 4), medium (5 to 6), high (7 to 8) and very high (9 to 10). For the Anxiety subscale, scores are categorized as very low (0 to 1), low (2 to 3), medium (4 to 5) and high (6 to 10). Scores may be analysed using these threshold categories or raw scores. Scales may be analysed separately.
Mental health self-efficacy scale
Mental Health Self-Efficacy Scale (MHSES) is a self-efficacy scale developed according to the Bandura’s guidelines for constructing self-efficacy questionnaires, specifically for common mental health problems (Clarke et al., 2014). It is unidimensional, with acceptable internal reliability (Cronbach’s alpha = .89) and construct validity (Clarke et al., 2014). It has six items and answered on a 10-point Likert scale, with 1 being ‘not at all confident’ and 10 being ‘totally confident’. Ratings across the six MHSES items for each participant were summed (scores range from 10 to 60) to obtain an overall measure of their mental health self-efficacy, with higher scores indicating greater self-efficacy.
Procedures
Immediately after the first group therapy session, participants were administered with a post-group questionnaire. Only a single session was selected as it is more congruent with the rapid turnover of patients typically found in the acute mental health ward. Instead of two measures at pre and postgroup, only a single measure at postgroup was utilised. This was designed to minimise measurement fatigue within the temporal parameters of a single group session. The therapist also rated participants’ participation in the group session using PRPS. At discharge, participants were asked to complete the ONS subjective well-being tool and the MHSES.
Data analysis
All descriptive and inferential analysis were done using IBM SPSS Statistics (Version 26.0, IBM Corp.). Descriptive statistics, independent sample t-tests and one-way analysis of variance (ANOVA), were done to examine possible covariates and confounders of all outcome variables. To examine predictors of (1) coping self-efficacy after group therapy and (2) overall mental health self-efficacy at discharge, full linear regression models were conducted using Enter Method, including possible covariates and confounders. Subsequently, to test if mental health self-efficacy predicted subjective well-being, general linear models were conducted. For all models, final models only included significant interactions and covariates if they affected the dependent variable.
Results
Participants demographics
Demographic of participants (N = 50).
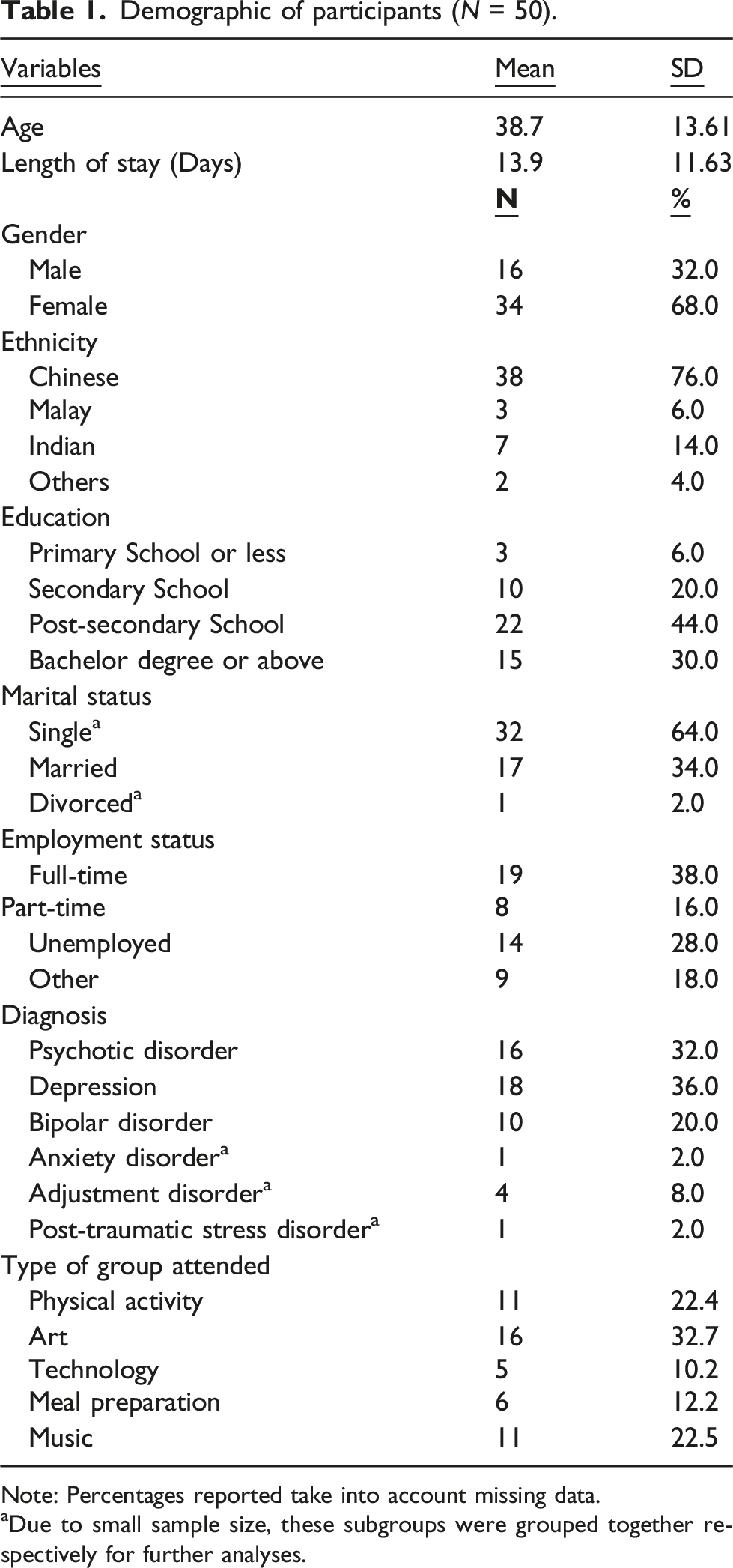
Note: Percentages reported take into account missing data.
aDue to small sample size, these subgroups were grouped together respectively for further analyses.
Group intervention and coping self-efficacy
Post-group questionnaires scores showed that patients rated themselves as having moderate to high self-efficacy (M = 6.92, SD = 2.48) to use the activity they participated in as a coping strategy. Overall, participants also experienced positive feelings with higher happiness scores (M = 7.42, SD = 2.20) and lower anxiety scores (M = 3.79, SD = 2.85). Therapists also rated patients as having a ‘good’ level of participation (M = 4.47, SD = 1.00), indicating that they finished most activities and followed directions.
T-test results of gender and marital status to outcome variables.
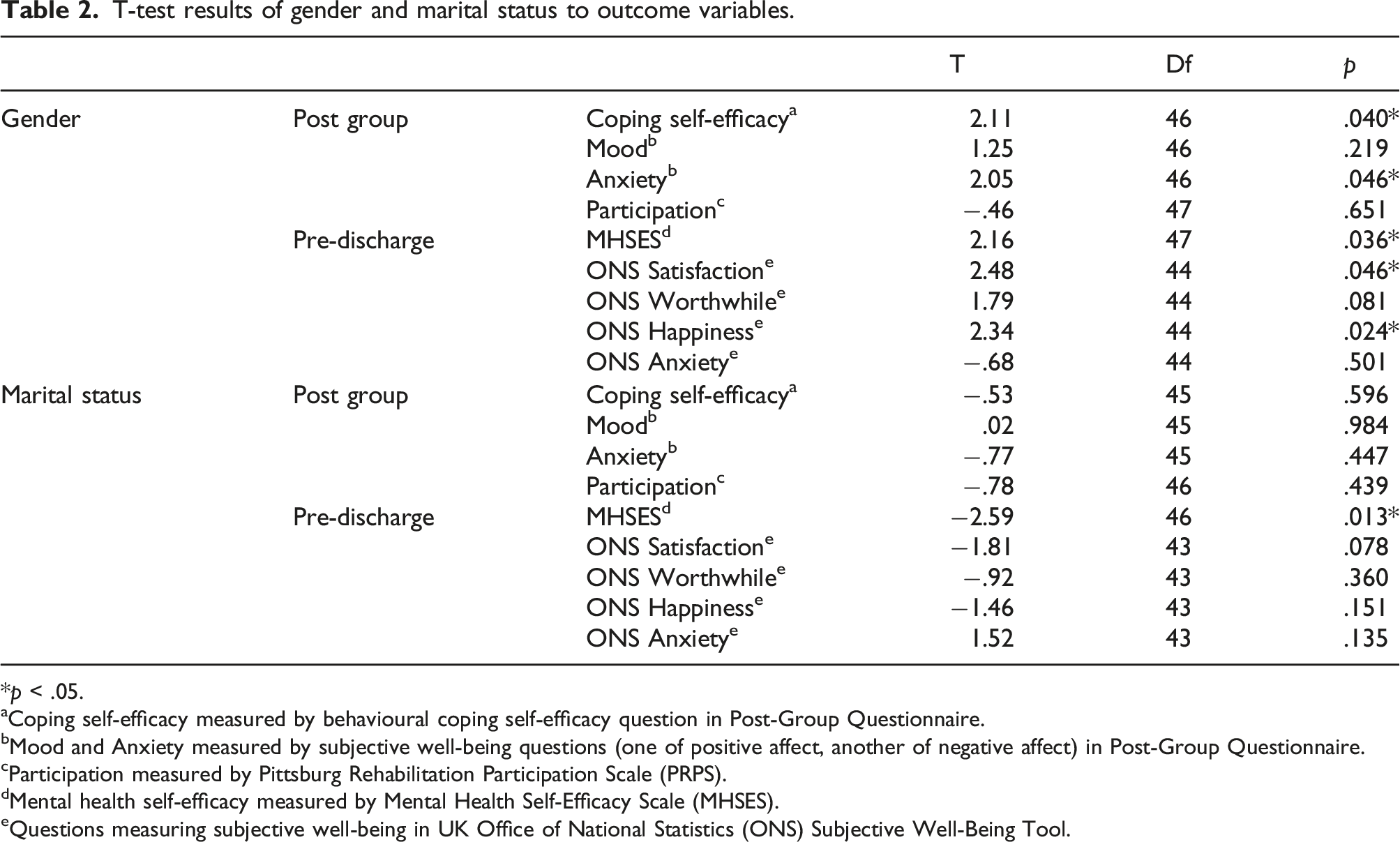
*p < .05.
aCoping self-efficacy measured by behavioural coping self-efficacy question in Post-Group Questionnaire.
bMood and Anxiety measured by subjective well-being questions (one of positive affect, another of negative affect) in Post-Group Questionnaire.
cParticipation measured by Pittsburg Rehabilitation Participation Scale (PRPS).
dMental health self-efficacy measured by Mental Health Self-Efficacy Scale (MHSES).
eQuestions measuring subjective well-being in UK Office of National Statistics (ONS) Subjective Well-Being Tool.
Summary of general linear regression models.
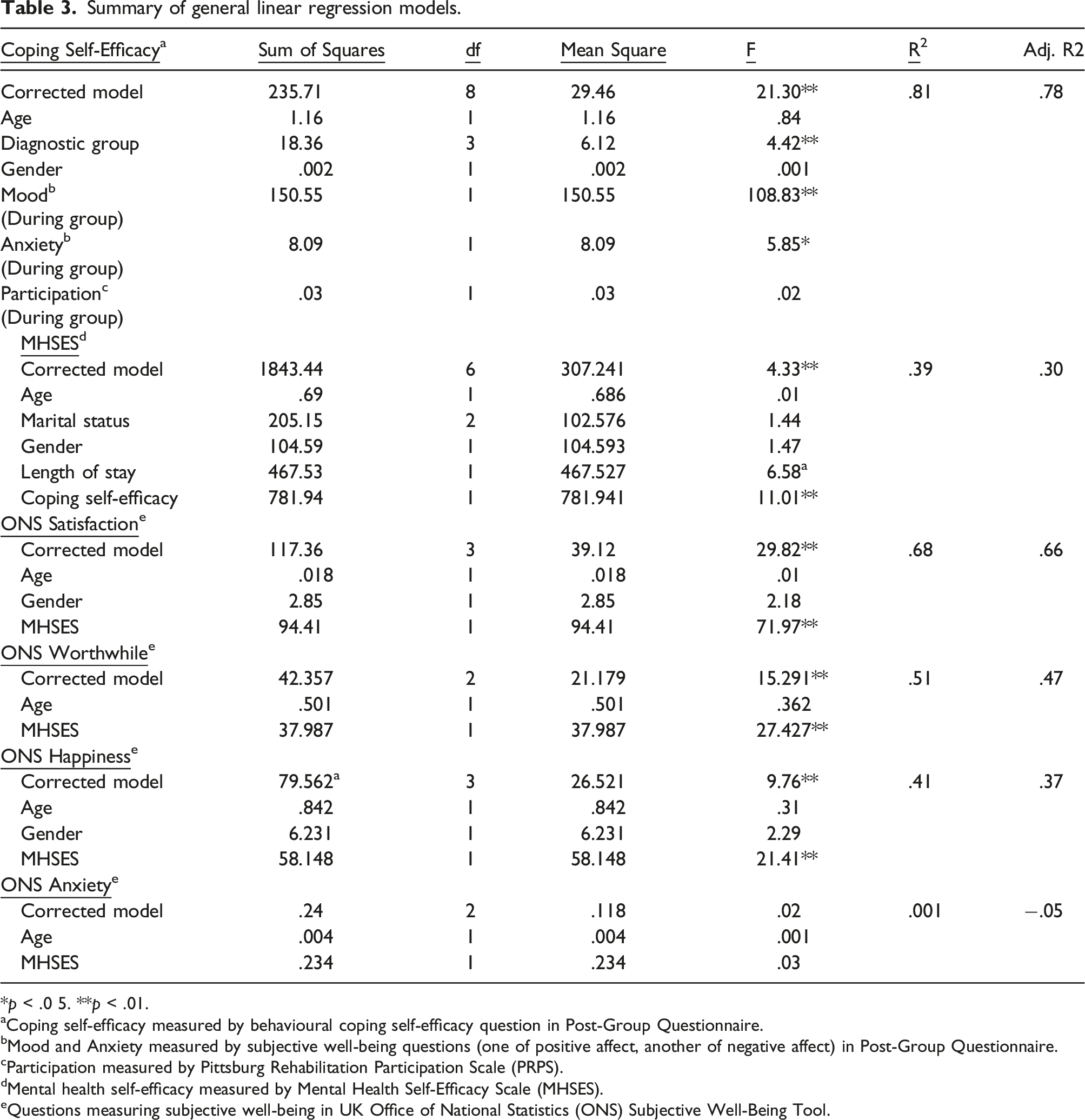
*p < .0 5. **p < .01.
aCoping self-efficacy measured by behavioural coping self-efficacy question in Post-Group Questionnaire.
bMood and Anxiety measured by subjective well-being questions (one of positive affect, another of negative affect) in Post-Group Questionnaire.
cParticipation measured by Pittsburg Rehabilitation Participation Scale (PRPS).
Mental health self-efficacy measured by Mental Health Self-Efficacy Scale (MHSES).
Questions measuring subjective well-being in UK Office of National Statistics (ONS) Subjective Well-Being Tool.
Factors affecting mental health self-efficacy
There was a significant difference in mental health self-efficacy scores between gender, and between singles and married individuals (Table 2). Other sociodemographic variables were not significantly related to mental health self-efficacy.
Full linear modelling was conducted to examine if post-group coping self-efficacy predicted mental health self-efficacy. Controlling for covariates (age, marital status, gender and length of stay), coping self-efficacy significantly predicted overall mental health self-efficacy (Table 3).
Factors affecting subjective well-being
In ONS subjective well-being tool, scores indicated high life satisfaction (M = 6.89, SD = 1.96), worthwhile (M = 7.04, SD = 1.51) and happiness scores (M = 7.09, SD = 2.07) and low–medium anxiety (M = 3.46, SD = 2.70). There was a significant difference in life satisfaction and happiness scores between males and females (Table 2). Full linear models were conducted for all aspects of well-being controlling for the covariates identified. While controlling for covariates, mental health self-efficacy significantly predicted life satisfaction, happiness and worthwhile domains of well-being but did not predict anxiety scores (Table 3).
Discussion
As predicted, participants after participation in their first activity-based group, tended to have high task-specific self-efficacy, indicating that participants felt confident in using the activity done during groups as a coping strategy. This resonates with existing research that regardless of specific coping strategies, interventions designed to increase coping behaviours have been found to be effective (Bradshaw, 1993).
There are numerous implications on how the group process can enhance self-efficacy. The social learning theory and four sources of self-efficacy – performance attainments, vicarious experience, verbal persuasion and physiologic arousal – could provide a basis for understanding (Bandura, 1997). Firstly, participants in an activity-based group had to complete an activity. As they worked to overcome obstacles to complete the activity, they gained information about their sense of efficacy. This was enhanced by the occupational therapist ensuring that activities given to participants were at the just-right challenge (Cole, 2017), enabling personal mastery and opportunity to develop skills and confidence. However, results from PRPS indicated that the art of participating alone is not sufficient in influencing self-efficacy. Developing competence through mastery experiences represents a key source of self-efficacy (Bandura, 1986). An individual who perceives a relationship between personal effort and success at an activity will then have a higher sense of task-specific self-efficacy (Carpinello et al., 2000).
Secondly, vicarious experience in a group setting enhances an individual’s feelings of self-efficacy. Many studies support the notion that individuals’ thoughts and actions are influenced by their observations of other people (Rosenthal & Bandura, 1978). The impact on self-efficacy is more evident when role models are similar to the individual (Carpinello et al., 2000). The role of vicarious experience may be an important and positive influence in activity-based groups, especially when group members observe other members with mental illness, put in efforts in participation and succeeding. This may be an advantage of group interventions over individual interventions, and reason behind various group interventions shown to improve self-efficacy and well-being (Kukla et al., 2017; Silverman, 2019).
Thirdly, verbal persuasion reinforces beliefs that individuals can perform and use the activity to cope with stressful events. That is, self-efficacy improves when one is exposed to sustained and genuine encouragement from respected others (Bandura, 1986). This applies to both verbal support from therapists and fellow participants. Qualities of therapists are commonly considered essential to a good therapeutic relationship, and facilitative therapist attitudes and behaviours are universally applicable (Bachelor & Horvath, 1999). Effective professionals had been described in terms of their ability to develop positive relationships through active listening, understanding, support and warmth (Mancini, 2007). Similarly, connection with others in social relationships has been identified as a key factor promoting recovery and improved mental health (Tew et al., 2012). This may be why being married, which suggest the presence of a supportive significant other, appear to be important in determining perceived mental health self-efficacy. In addition, supportive social environment in group settings have been identified by several studies to be one of the key therapeutic factors of groups (Carpinello et al., 1992; Eklund, 1997; Rebeiro & Cook, 1999).
Lastly, physiologic arousal indicates that approaches that help individuals to interpret emotional reactions positively may enhance coping efficacy and improve performance (Bandura, 1997). Consequently, when participants enjoy the activities that they are doing in the group, they are more likely to interpret their emotional and physiological states positively. They may also experience flow, defined as the mental state when one is totally involved in an activity (Csikszentmihalyi, 1975). This includes the focussing of attention on a clear goal, a loss of self-consciousness, and a sense that the activity in itself is rewarding (Emerson, 1998), enhancing an individual’s sense of well-being and self-efficacy. The results support that the emotional experience during the group activity appeared to be stronger predictors than completion of the task itself.
Therefore, self-efficacy in using specific activities performed in the group as coping strategies may be enhanced through appropriate support in an activity-based group. Previous research indicates health outcomes can be improved and sustained when self-efficacy is involved in behavioural change strategies (O’Hare & Shen, 2013). This affirms that behavioural coping strategies which play an important role in mental health recovery can be reinforced via activity-based group therapy. Improvement of self-efficacy could be an explicit goal in mental health recovery groups and intervention strategies.
In relation to the second objective, our results suggested that higher self-efficacy in using specific activities as coping strategies postgroup, has a strong positive relationship with general mental health self-efficacy, which in turn contributes to overall well-being. These findings are in accordance with existing literature on self-efficacy. For example, Suzuki et al. (2011) found that individuals with high general self-efficacy are likely to score high on specific self-efficacy, and that self-efficacy can be important to subjective well-being (Anderson et al., 2014; Carpinello et al., 1992; Rosenfield, 1992). Carpinello et al. (1992) also found that improvement in well-being may occur by increasing one’s sense of self-efficacy.
Participants in our study who had higher specific coping self-efficacy during their first group had higher mental health self-efficacy at discharge. This lends support to evidence that regardless of the specific coping skill, coping is an essential component of recovery in mental health (Silverman, 2019). It also suggests the importance of this personal resource as it was found to be related to other positive outcomes both in our study and past studies.
Limitations in the studies’ design include, firstly, a small sample size affecting the strength of the results. Nevertheless, it is a pilot exploratory study to examine possible relationships of important variables, within the context of activity-based group therapy in acute mental health ward. As self-efficacy was not measured at baseline in our study, this may also have had a significant influence in predicting outcomes for people with mental illness, given the significance of self-efficacy on recovery. It would be necessary to replicate this study to confirm whether the relationships observed are also found in larger samples and explore the inclusion of further outcomes.
Secondly, all participants in our study could also attend a variety of group and/or individual therapy conducted by other healthcare professionals as part of their usual routine care, determined by the treating physician. These treatments may have impacted on patient’s mental health self-efficacy and subjective well-being at discharge. Because of a cross-sectional design, no causal relationships can be inferred. Longitudinal studies and broader investigations into the factors related to coping self-efficacy are needed to understand how best to enhance it. Future studies need to also examine the differences between general mental health self-efficacy and self-efficacy specific to behavioural-based coping.
Conclusion
This study suggests that performing behavioural coping strategies in groups has positive associations with behavioural coping self-efficacy and positive well-being postgroup. In addition, it was strongly associated to high mental health self-efficacy at discharge. Overall, the results support the use of activity-based group therapy by occupational therapists in an acute mental health ward, and self-efficacy should be a key element in interventions to elicit a process of empowerment that may improve recovery and well-being.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Appendix
Please answer the following questions on a scale of 0 to 10, 0 being ‘not at all’ and 10 is 'completely'.