
Abstract
Introduction
Dry needling has been identified as a potential intervention for a variety of diagnoses. Limited evidence exists to support the use of dry needling following surgical intervention of a distal radius fracture. This case report demonstrates the impact of dry needling in the thumb following a distal radius fracture.
Methods
The patient was a 31-year-old healthy female who sustained a distal radius fracture and required surgical intervention. The patient required a volar plate removal and extensor tenolysis. The patient attended traditional occupational therapy with one session of dry needling to assist in improving range of motion and decreasing pain.
Results
The patient benefited from the use of dry needling. The patient had no pain with functional grasping and pinching following dry needling and improved on the Kapandji score from eight to nine out of ten. The patient also reported a decrease in overall pain, from seven to two on the Numeric Pain Rating Scale.
Discussion
The patient benefited from dry needling in the thumb to improve both range of motion and pain symptoms. While the evidence is limited, dry needling may be an appropriate intervention to assist in recovery and reduce thumb pain following distal radius fractures.
Introduction
Distal radius fractures are the most common injuries of the musculoskeletal system, and consequently, hand and wrist fractures account for nearly 2.5% of all emergency room visits (Medoff, 2011; Nellans et al., 2012). Falling on an outstretched limb is the primary cause of distal radius fractures, and although there is no standard treatment associated with distal radius fractures, many are treated in a non-operative fashion (Medoff, 2011). Nevertheless, parameters do exist for surgical intervention in severe fractures that pose functional consequences without repair (Bamford & Walker, 2010; Obert et al., 2013). Over the past decade, open reduction with internal fixation (ORIF) surgery has gained popularity for treating this condition (Medoff, 2011). ORIF involves an open reduction to set the bone and internal fixation using screws, plates, rods, and/or pins to hold the bone in place while it heals. Following wrist fracture fixation, hardware removal is sometimes necessary due to a variety of reasons, including pain, tendon dysfunction, complex regional pain syndrome, and bone malunion (Medoff, 2011; Snoddy et al., 2015). In these cases, physical and occupational therapy after the ORIF hardware removal can be beneficial to help restore normal mobility, function and contribute to satisfactory outcomes (Snoddy et al., 2015). While distal radius fracture recovery time can vary following surgical intervention, more positive outcomes have been found in patients who have higher perceived outcomes, improved grip strength, and radiographic evidence of restored anatomy (Medoff, 2011).
Dry needling is a procedure performed by a physical or occupational therapist to reduce pain and muscle tightness. Dry needling involves inserting a monofilament needle into the skin and muscle in an identified myofascial trigger point (MTrP), with the removal of the needle occurring once the trigger point is no longer active, eliciting a physiologic response (Kietrys et al., 2013). MTrPs have been identified as a source of pain and contributor to functional deficits including range of motion (ROM) limitations and decreased strength (Travell & Simons, 1999; Unverzagt et al., 2015). Active trigger points are described as hyperirritable spots in a taut band of skeletal muscle/fascia that possess electrical characteristics similar to a strong muscle contraction (Ge et al., 2011). MTrPs are identified through palpation and the identification of taut bands in the skeletal muscle (Unverzagt et al., 2015). These taut bands are composed of skeletal muscle and fascia and can cause localized tenderness and referred pain (Celik & Mutlu, 2013). The mechanism of action behind dry needling is unclear, but it is believed that it may elicit an analgesic effect, relax the actin–myosin bonds, and improve muscle blood flow in the area surrounding the tissues (Cagnie et al., 2013; Dunning et al., 2014; Kietrys et al., 2013; Unverzagt et al., 2015). Previous research supports the use of dry needling to decrease pain and improve ROM (Gerber et al., 2015; Kaljić et al., 2018; Kietrys et al., 2013; Liu et al., 2015; Ziaeifar et al., 2014). However, a systematic literature has identified low-quality evidence to support the use of dry needling compared to no intervention or a sham intervention (Gattie et al., 2017). Evidence to support the use of dry needling in the hand is minimal, with one preliminary study demonstrating an improvement in both pain and perceived outcome following one treatment session (Azizian et al., 2019). To increase the body of evidence supporting the use of dry needling in the hand, we present a case report exploring the use of dry needling in conjunction with occupational therapy following a severe fracture with ongoing post-surgical pain and ROM deficits. The following case report aims to address the clinical question: “Does dry needling assist in the treatment of thumb pain following a volar plating removal and tenolysis?”
Patient description
The patient was a 31-year-old pleasant female, who suffered a fall on ice resulting in a right distal radius intra-articular fracture. The distal radius was fractured into three separate pieces, and surgical intervention was deemed necessary. The patient underwent an ORIF of the distal radius 5 days postinjury in conjunction with a posterior interosseous neurectomy and extensor pollicis longus debridement. After the surgical procedure, the patient was placed in a soft dressing and a sugartong splint, including a thumb spica component.
Functional measurements at three time points.
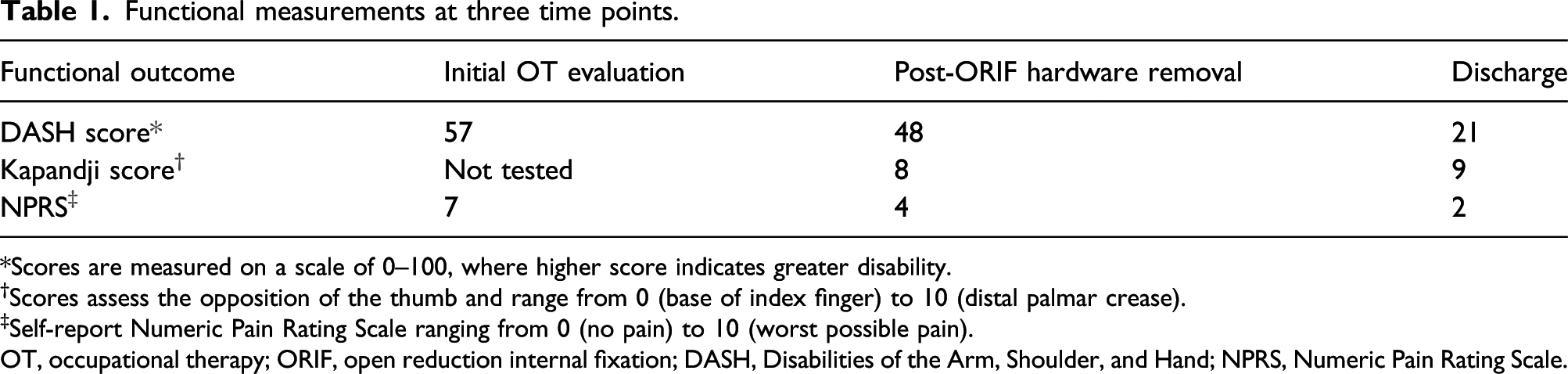
*Scores are measured on a scale of 0–100, where higher score indicates greater disability.
†Scores assess the opposition of the thumb and range from 0 (base of index finger) to 10 (distal palmar crease).
‡Self-report Numeric Pain Rating Scale ranging from 0 (no pain) to 10 (worst possible pain).
OT, occupational therapy; ORIF, open reduction internal fixation; DASH, Disabilities of the Arm, Shoulder, and Hand; NPRS, Numeric Pain Rating Scale.
An extensor tenolysis with hardware removal was completed 15 weeks following the ORIF of the distal radius fracture. The third and fourth extensor compartment and the extensor pollicis longus were transposed with scarring evident. The pronator quadratus was found to have been scarred as well. A tenolysis was performed to release the above-listed scar adhesion, in addition to the plate removal.
The patient was evaluated by occupational therapy 3 days following the surgical intervention of tenolysis and hardware removal. At the time of occupational therapy evaluation, the patient’s major complaints involved limited thumb motion. As shown in Table 1, the patient had a DASH score of 48 out of 100, with higher scores indicating a greater level of disability (Beaton et al., 2001). The Kapandji score was utilized to assess the opposition of the thumb (Jha et al., 2016). At the evaluation, the patient could not achieve small finger (SF) opposition to the base of the SF and had a Kapandji score of eight out of ten (Table 1) (Jha et al., 2016). The patient agreed to attend therapy two times per week with an emphasis on restoring thumb ROM to aid in meeting her stated goal of improving functional grasping. The patient was educated on wrist and thumb active and passive ROM as part of her home exercise program. Occupational therapy interventions consisted of active and passive ROM, heat modalities, and ultrasound over the course of 11 visits over 7 weeks. The patient consistently had a Kapandji score of eight out of ten actively following each treatment session, with no additional improvement in active range of motion (Jha et al., 2016). The patient continued to have complaints of pain in the musculature in the thenar eminence, with the pain in the extensor region of the thumb resolved. At this point, it was determined the patient may benefit from the addition of dry needling of the thenar eminence to her plan of care. Before the dry needling intervention, the patient had a deficit of 0.5 cm to oppose to the base of the SF and a Kapandji score of eight out of ten (Jha et al., 2016). The patient also had consistent complaints of pain of a four out of ten on a Numeric Pain Rating Scale (NPRS) with a score of ten being the worst (Table 1) (Hawker et al., 2011).
Methods
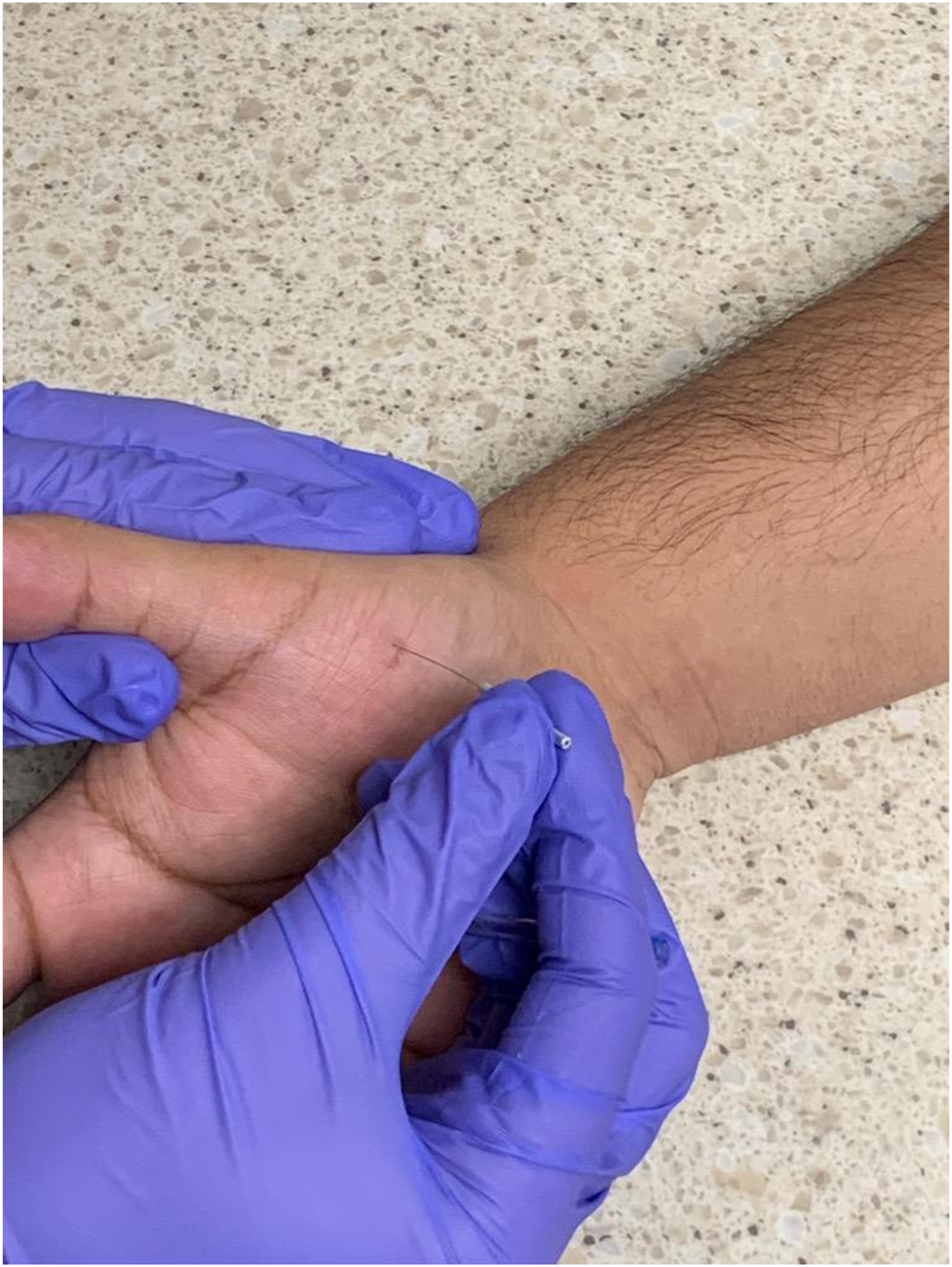
During the dry needling session, a taut band of tissue within the thenar eminence was identified by the therapist (Figure 1-Palpation). The taut band of tissue was correlated with a pain response from the patient, and it became the focus of treatment due to the reproduction of symptoms with palpation. Multiple areas of pain were identified and utilized for the dry needling application, as the taut band was the length of the abductor pollicis brevis. The area was swabbed with a 70% alcohol swab. A pre-sterilized, disposable solid filament needled was utilized for the dry needling application. The therapist donned disposable gloves prior to the dry needling application. A pistoning technique was used to complete the treatment with three 0.25 mm × 30 mm needles placed into the abductor pollicis brevis (Figure 2—Pistoning). The needle shaft was maintained in a sterile state throughout the duration of treatment, and the therapist did not identify any blood or drainage from the needling sites. The patient was educated to use ice or heat as needed for pain control following the appointment. Palpation. Pistoning.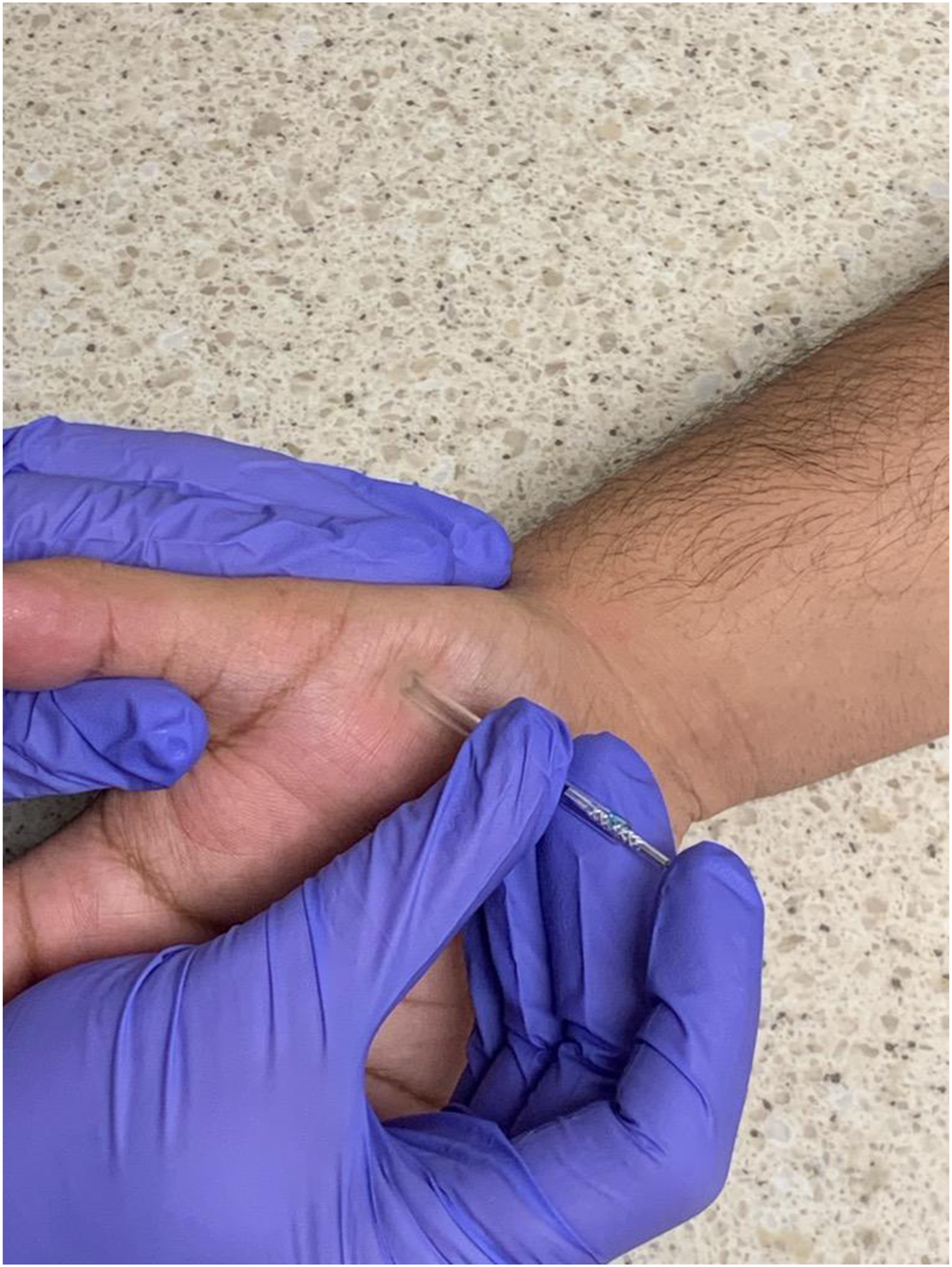
Results
The patient completed one dry needling session, followed by three subsequent occupational therapy visits, totaling 14 occupational therapy visits over 7 weeks. The patient tolerated the dry needling treatment without any adverse effects. Following the dry needling intervention, the patient demonstrated the ability to fully oppose to the base of the SF, with a Kapandji score of nine out of ten. The patient demonstrated a consistent improvement following the dry needling intervention, which continued for the next three occupational therapy visits. The patient was discharged with continued ability to oppose to the base of the SF and a Kapandji score of nine out of ten (Table 1) (Jha et al., 2016). The patient also reported pain of two out of ten on a numeric rating scale and a DASH score of 21 (Table 1). At the time of discharge, the patient was restored to full function and had minimal reported limitations with daily activities.
Discussion
The evidence supporting the use of dry needling continues to grow (Azizian et al., 2019; Dunning et al., 2014; Kietrys et al., 2013); however, current literature is lacking demonstrating the effectiveness of dry needling in the hand, specifically the thumb. The results of this upper extremity case report are consistent with the current body of evidence evaluating the use of dry needling in other various body regions to reduce pain and improve ROM (Dunning et al., 2014; Gattie et al., 2017; Gerber et al., 2015; Kietrys et al., 2013; Liu et al., 2015; Ziaeifar et al., 2014). The patient’s response to dry needling treatment was favorable with a noticeable ROM improvement and overall decreased pain at rest and with function. The ROM improvement was achieved in a relatively short time with minimal complications, further providing support for the use of dry needling on MTrPs, specifically in the thumb. The results of this case report are important because they help to support the use of dry needling in hand injuries with ongoing ROM deficits and pain complaints and may provide options for clinicians to consider in practice to facilitate better outcomes in a relatively timely manner.
This case report does present with some limitations. While there was an improvement that was maintained following the dry needling intervention, the patient completed occupational therapy sessions in conjunction with dry needling. Therefore, ROM increases cannot be solely attributed to the dry needling intervention. Further studies evaluating the use and efficacy of dry needling interventions on ROM in the thumb are warranted to increase the evidence supporting the use of the treatment.
Although evidence substantiating the use of dry needling continues to grow, current literature exploring the effectiveness of dry needling in the thumb and hand is lacking. The results of this case report support the adjunctive use of dry needling in the management of ROM limitations and ongoing post-surgical thumb pain following a severe fracture. The pain decreased in the thenar eminence with a decrease in taut tissue also noted following the dry needling intervention. Nevertheless, additional studies are warranted to evaluate the use of dry needling in the thumb and hand to further support the use of the intervention for the hand and upper extremity rehabilitation. Additional studies could also help to identify the variances in outcomes with traditional acupuncture and dry needling within the hand and thenar eminence.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.