
Abstract
Objective
This study explored factors which predict stroke survivors who could achieve “clinically significant functional gain” and return home when being discharged from a local hospital after in-patient stroke rehabilitation programme.
Methods
This study included 562 inpatients with stroke who were residing at community dwellings before onset of stroke, and transferred to a convalescent hospital for rehabilitation from four acute hospitals over one year. The main outcome variables of prediction were (a) achieving “clinically significant functional gain” as measured by (a1) achievement of “minimal clinically important difference” (MCID) of improvement in Functional Independence Measure Motor Measure (FIM-MM)”, (a2) one or more level(s) of improvement in function group according to the patients’ FIM-MM, and (b) discharge to home. Sixteen predictor variables were identified and studied firstly with univariate binary logistic regression and those significant variables were then put into multivariate binary logistic regression.
Results
Based on multivariate regression, the significant predictors for “clinically significant functional gain” were: younger age <75 years old, higher Glasgow Coma Scale score at admission, with haemorrhagic stroke, intermediate FIM-MM function group. Those significant predictors for “discharge to home” were: living with family/caregivers before stroke, higher FIM score at admission, and one or more level(s) of improvement in FIM-MM function group.
Conclusions
This study identified findings consistent with overseas studies in additional to some new interesting findings. Early prediction of stroke discharge outcomes helps rehabilitation professionals and occupational therapists to focus on the use of appropriate intervention strategies and pre-discharge preparation.
Introduction
Stroke is a major cause of disability with an indication for long term rehabilitation, which includes an in-patient phase as well as a community phase (Feigin et al., 2003). Despite the incidence rate of stroke in Hong Kong has decreased, the number of stroke survivors remains large due to reduction in mortality rate and population aging (Woo et al., 2014). That implies there is an increasing demand for stroke rehabilitation services. Early and accurate prediction of rehabilitation outcomes, such as discharge destinations, better functional improvement, etc. can facilitate the rehabilitation team to customize their plans of care (e.g. triage to different wards, intensive training versus reinforcing skills of care-givers, etc.) and allow more time for liaison and/or making referrals between transitions of care. Subsequently, it may improve patients’ outcomes, decrease length of stay, lower costs, and, improve utilization of resources (Summers et al., 2009).
Outcomes of stroke are associated with various factors including sociodemographic characteristics, clinical characteristics of the stroke incident, comorbid conditions, functional performance at the beginning of the treatment and rehabilitation process. Previous studies and systematic reviews reported that age, marital status, time from stroke onset to rehabilitation, aphasia, neglect, stroke severity presented in National Institutes of Health Stroke Scale, cognitive function, and motor function such as walking distance were associated with the gain score in Functional Independence Measure (FIM) after stroke rehabilitation (Brown et al., 2015; Fung, 2004; Leung et al., 2010; Meyer et al., 2015; Scrutinio et al., 2015). On the other hand among these variables it was found that functional independence was the most determinant factor of discharge destination in majority of studies (Mees et al., 2016). Furthermore, stroke survivors were more prone to institutional care if they had the characteristics of older age, living alone, having pre-existing comorbidities such as atrial fibrillation, severe stroke, dysphagia, cognitive, motor or functional impairment (Brown et al., 2015; Itaya et al., 2017; Mees et al., 2016; Nguyen et al., 2015). This study aimed to explore if these predictor variables of different aspects stated above showed similar positive association with achievement of clinically significant functional gain and discharge to home for stroke patients in a local rehabilitation hospital.
Methods
This was a retrospective cohort study of which the variables of interest – both the outcome and predictor variables, were retrieved from various information systems of the Hong Kong Hospital Authority, i.e. Clinical Data Analysis & Reporting System (CDARS), Clinical Management System (CMS), the Functional Independence Measure Module (CMS-FIM) under CMS and patients’ medical records. All the data were independently retrieved and reviewed by two persons – the principle investigator and the 2nd co-investigator in order to ensure accurate and valid information before analysis. All personal data was kept in strict confidentiality and was handled in line with hospital’s policy in handling, storage and destruction of patients’ medical records. This study was approved by the Research Ethics Committee (Kowloon Central/Kowloon East) [Ref: KC/KE-17-0231/ER-1].
Participants
Patients with principal diagnosis of stroke who were residing at community dwellings before the onset of stroke being transferred from the acute hospitals, Caritas Medical Centre, Kwong Wah Hospital, Queen Elizabeth Hospital and United Christian Hospital to Kowloon Hospital (KH) within a 12-month period from 1st April, 2015 to 31st March, 2016 were included in the study. Patients with the following criteria would be excluded: i) residents of old age home (OAH) before the stroke incident, ii) drop-out from the rehabilitation programme, e.g. episodic death, being transferred back to acute hospitals due to deterioration in medical conditions and not returning to KH, etc., iii) missing data in major parameters which cannot be retrieved.
Outcome variables
The research team made reference to previous studies (Brown et al., 2015; Fung, 2004; Itaya et al., 2017; Leung et al., 2010; Mees et al., 2016; Meyer et al., 2015; Nguyen et al., 2015; Scrutinio et al., 2015) and the consensus-based core recommendations from the Stroke Recovery and Rehabilitation Roundtable in identifying outcome measures and potential predictor variables (Kwakkel et al., 2017). The two outcome variables being studied in this research were (a) achieving “clinically significant functional gain”, and, (b) discharge to home; not requiring institutional care. The “clinically significant functional gain” was operationally defined in two ways. They are (a1) achievement of “minimal clinically important difference” (MCID) of improvement in FIM Motor Measure (FIM-MM), and, (a2) one or more level(s) of improvement in function group as classified by KH according to patients’ FIM-MM. “Clinically significant functional gain” referred to any change in levels between the time of admission and the time of discharge in positive direction. MCID was defined as “the smallest difference in score in the domain of interest which patients perceive as beneficial and which would mandate” (Jaeschke et al., 1989). According to Beninato et al. (2006) a change of 17 points in FIM-MM was defined as the MCID for stroke rehabilitation. For “clinically significant functional gain” in our research, that meant an increase of at least 17 in FIM-MM when discharged from KH comparing that at admission to KH. The other operational definition for “clinically significant functional gain” was “one or more level(s) of improvement in KH FIM-MM function group” when discharged from KH when comparing that at admission to KH. In KH stroke patients were classified into three groups based on their FIM-MM: i) FIM-MM ≤26 – “lower” function group whose activities of daily living (ADL) function was dependent and/or required maximal assistance, ii) FIM-MM 27 to 52 – “immediate” function group whose ADL function required minimal to moderate assistance, &, iii) FIM-MM ≥ 53 – “higher” function group whose ADL function was independent with/without supervision) (Stroke Rehabilitation Triage Form, 2017). This classification facilitated KH medical team members to have an easy and quick interpretation of patients’ functional level. The second outcome variable was “discharge to home”. It referred to those stroke patients discharged back home immediately after the completion of KH stroke rehabilitation programme; those who were discharged to OAH either temporarily or for long term care were not counted.
Predictor variables
Emphasis was put on the following two criteria in the selection process: i) these variables were reliably and routinely recorded in various information systems of the Kowloon Hospital, and, ii) these variables would be easily understood and interpreted by members of the rehabilitation team. Finally, sixteen predictor variables were selected and grouped into four groups namely: i) demographic characteristics, ii) clinical characteristics, iii) neurological impairment at the time of admission to the KH rehabilitation programme, and, iv) process characteristics of the rehabilitation programme. The demographic characteristics included age, gender and premorbid living situation. The clinical characteristics included stroke type, prompt thrombolysis treatment at the onset of ischaemic stroke, comorbid conditions including atrial fibrillation, hypertension, type II diabetes mellitus (uncomplicated), hyperlipidemia and, pneumonia complication. The clinical parameters adopted for illustrating the levels of “neurological impairment” at admission to KH included Glasgow Coma Scale (GCS), Mini-Mental State Examination (MMSE), performance in ADL in terms of FIM score, FIM-MM, the KH FIM-MM function groups, and, the presence of dysphagia with the need of nasogastric tube feeding. The process characteristics of the rehabilitation programme included the time from stroke onset to rehabilitation at KH, programme interruption at KH, i.e. being transferred momentarily back to the acute hospital and then returning to Kowloon Hospital to continue their rehabilitation programme and the length of stay at KH. For predicting “discharge to home”, the two parameters defining “clinically significant functional gain” based on FIM-MM were in return being evaluated for their potential predictive ability.
Statistical analysis
All predictor (or independent) variables were compared for patients discharged home and those discharged to OAH or other facilities. For each analysis, p values were obtained using Pearson chi-square tests for categorical variables and Wilcoxon Signed-Rank Test for continuous/ordinal variables. Logistic regression is the most appropriate method for binary outcomes and for considering confounding effects of multiple variables (Armitage et al., 2002). Predictor variables were put into univariate binary logistic regression with (a) “clinically significant functional gain” and (b) “discharge to home” as the outcome (or dependent) variables respectively. Predictors with p < 0.1 in univariate analysis were then put into multivariate binary logistic regression. Events per variable value of 10 was suggested for the multivariate regression (Peduzzi et al., 1996). If the Spearman rank correlation for the predictor variables was >0.5, one of the variables was chosen for the next step based on clinical relevance. Statistical analysis was performed with Statistical Products and Service Solutions version 23.
Results
Seven hundred and two (i.e. 702) stroke patients were initially identified from CDARS and CMS-FIM-module but 140 of them were excluded according to our listed exclusion criteria (55 residents of old age home before the stroke incident; drop-out from the rehabilitation programme included 19 episodic deaths, 56 being transferred back to acute hospitals due to deterioration in medical conditions and not returning to KH, 10 with missing data in major parameters including FIM or GCS scores which cannot be retrieved. The characteristics of the remaining 562 stroke patients were shown in Table 1. Among this group of patients, 279 (49.6%) were age <75, 268 (47.7%) were female, 373 (66.4%) suffered from ischemic stroke, 136 (24.2%) suffered from haemorrhagic stroke, and, 66 (11.7%) were premorbid living alone. Table 2 summarized the rehabilitation outcomes of patients: 138 (24.6%) achieved MCID of improvement in FIM-MM, 164 (29.2%) had one or more level(s) of improvement in KH FIM-MM function group, and, 304 (54.1%) were discharged home. The results of univariate and multivariate binary logistic regression analysis between the predictor variables and the outcome variables (a1) “achievement of MCID of improvement in FIM-MM”, (a2) “one or more level(s) of improvement in KH FIM-MM function group”, and, (b) “discharge to home” were showed in Tables 3 to 5 respectively.
Characteristics of the 562 stroke patients included in this cohort.
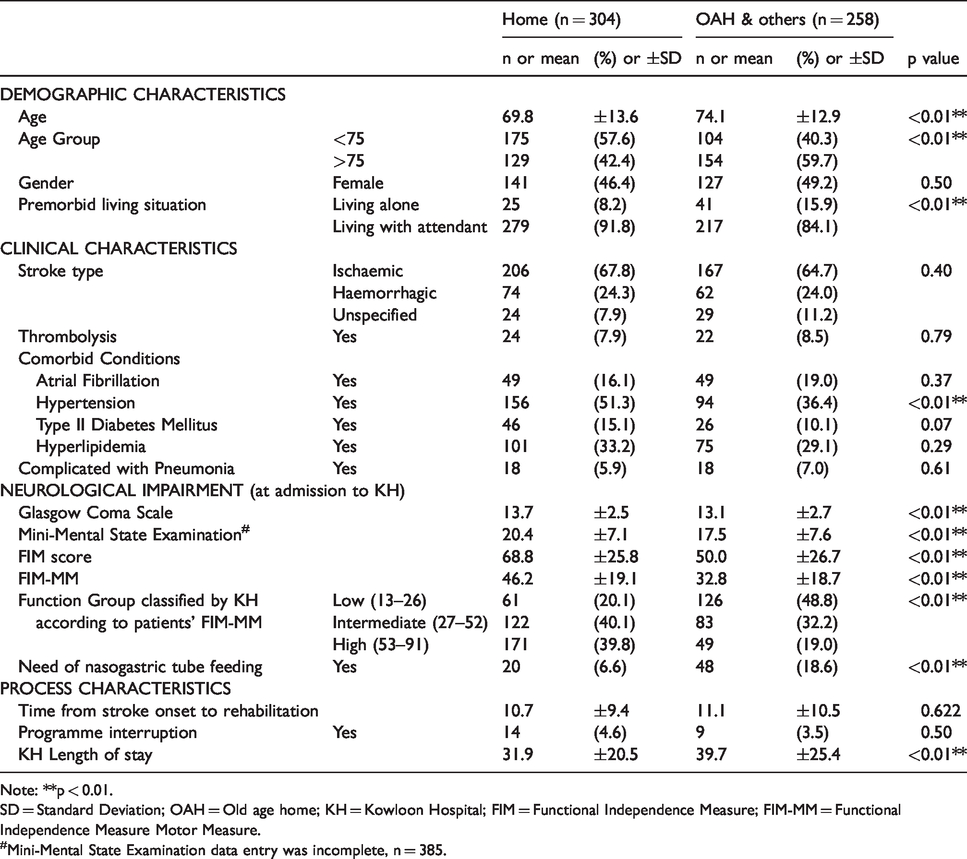
Note: **p < 0.01.
SD = Standard Deviation; OAH = Old age home; KH = Kowloon Hospital; FIM = Functional Independence Measure; FIM-MM = Functional Independence Measure Motor Measure.
#Mini-Mental State Examination data entry was incomplete, n = 385.
Rehabilitation Outcomes of the 562 stroke patients included in this cohort.
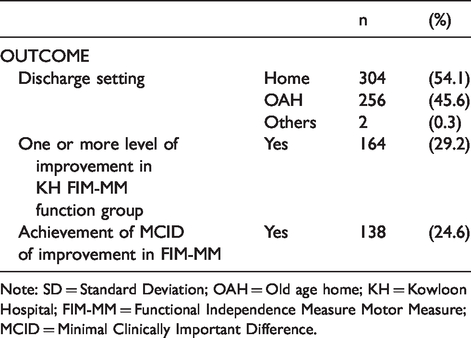
Note: SD = Standard Deviation; OAH = Old age home; KH = Kowloon Hospital; FIM-MM = Functional Independence Measure Motor Measure; MCID = Minimal Clinically Important Difference.
Binary logistic regression of factors associated with (a1) “clinically significant functional gain” – “achievement of MCID of improvement in FIM-MM”.
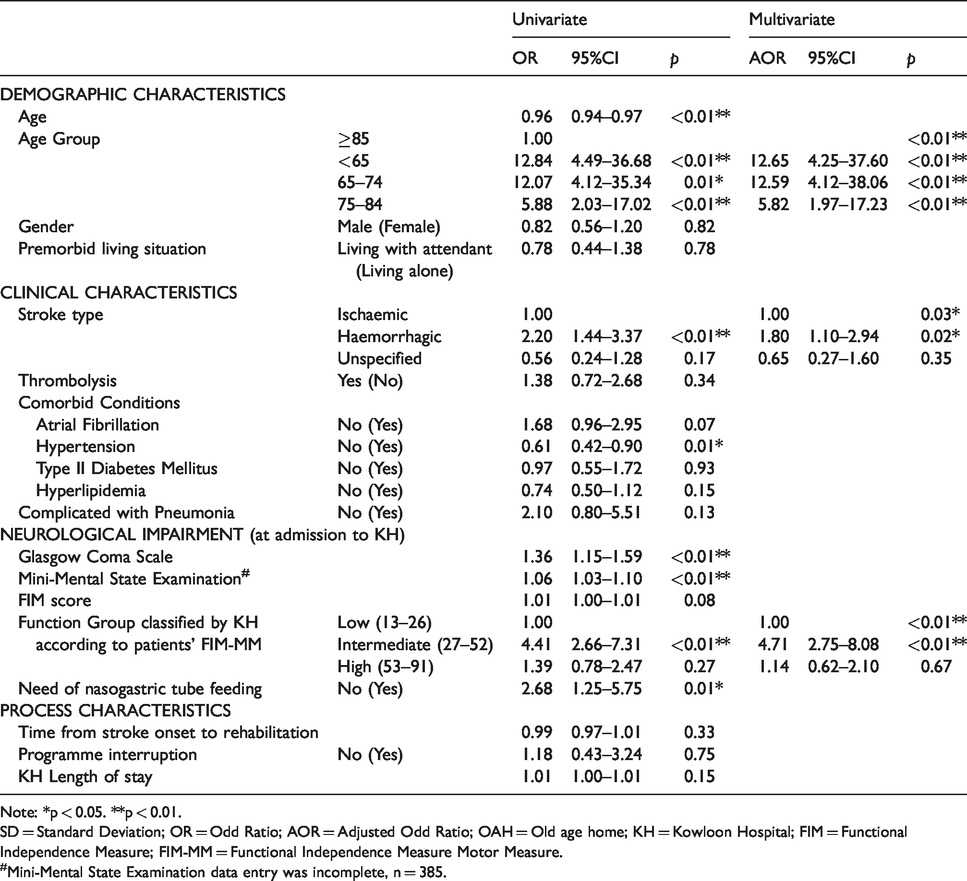
Note: *p < 0.05. **p < 0.01.
SD = Standard Deviation; OR = Odd Ratio; AOR = Adjusted Odd Ratio; OAH = Old age home; KH = Kowloon Hospital; FIM = Functional Independence Measure; FIM-MM = Functional Independence Measure Motor Measure.
#Mini-Mental State Examination data entry was incomplete, n = 385.
In multivariate logistic regression, the significant predictors for (a1) “achievement of MCID of improvement in FIM-MM” were “age groups < 85” (Compared with reference ≥85; < 65 AOR 12.65, 95% CI 4.25–37.60, 65–74 AOR 12.59, 95% CI 4.16–38.06, 75–84 AOR 5.82 CI 1.97–17.23), “haemorrhagic stroke” (Compared with reference “ischemic stroke”; AOR 1.80, 95% CI 1.10–2.94), “Intermediate KH FIM-MM function group” (Compared with reference “Low KH FIM-MM function group”; AOR 4.71, 95% CI 2.75–8.08) (Table 3). The significant predictors for (a2) “one or more level(s) of improvement in KH FIM-MM function group” were “age groups <75” (Compared with reference ≥85; <65 AOR 2.87, 95% CI 1.52–5.63, 65–74 AOR 2.41, 95% CI 1.15–4.61), “with one more mark in GCS at admission” (AOR 1.56, 95% CI 1.27–1.80) and “with one less mark in FIM score at admission” (AOR 0.97, 95% CI 0.96–0.82) (Table 4). The significant predictors for (b) “discharge to home” were “premorbid living with family or with attendant” (Compared with reference “premorbid living alone”; AOR 2.88, 95% CI 2.06–30.07), “with one more mark in FIM score at admission” (AOR 1.03, 95% CI 1.02–1.05), and “one or more level(s)of improvement in KH FIM-MM function group” (Compared with reference “no change in KH FIM-MM function group”; AOR 1.81, 95% CI 1.22–2.68) (Table 5).
Binary logistic regression of factors associated with (a2) “clinically significant functional gain” – “one or more level(s) of improvement in function groups as classified by KH according to the patients’ FIM-MM”.
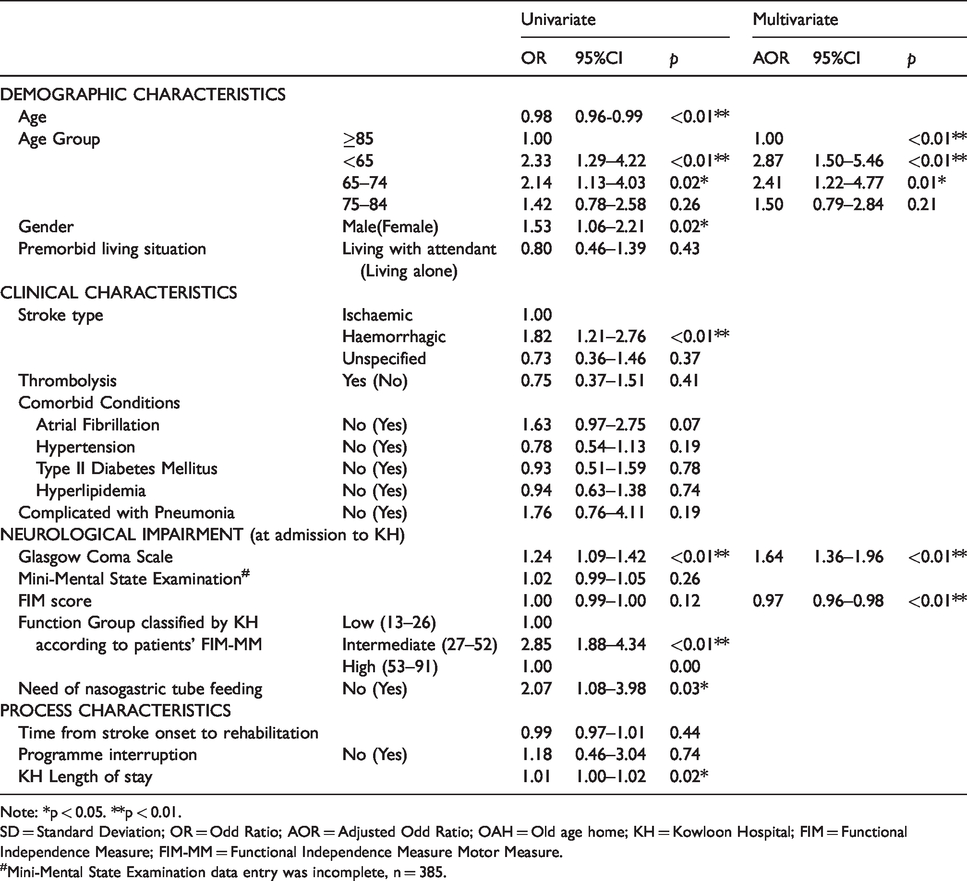
Note: *p < 0.05. **p < 0.01.
SD = Standard Deviation; OR = Odd Ratio; AOR = Adjusted Odd Ratio; OAH = Old age home; KH = Kowloon Hospital; FIM = Functional Independence Measure; FIM-MM = Functional Independence Measure Motor Measure.
#Mini-Mental State Examination data entry was incomplete, n = 385.
Binary logistic regression of factors associated with (b) “discharge to home”.
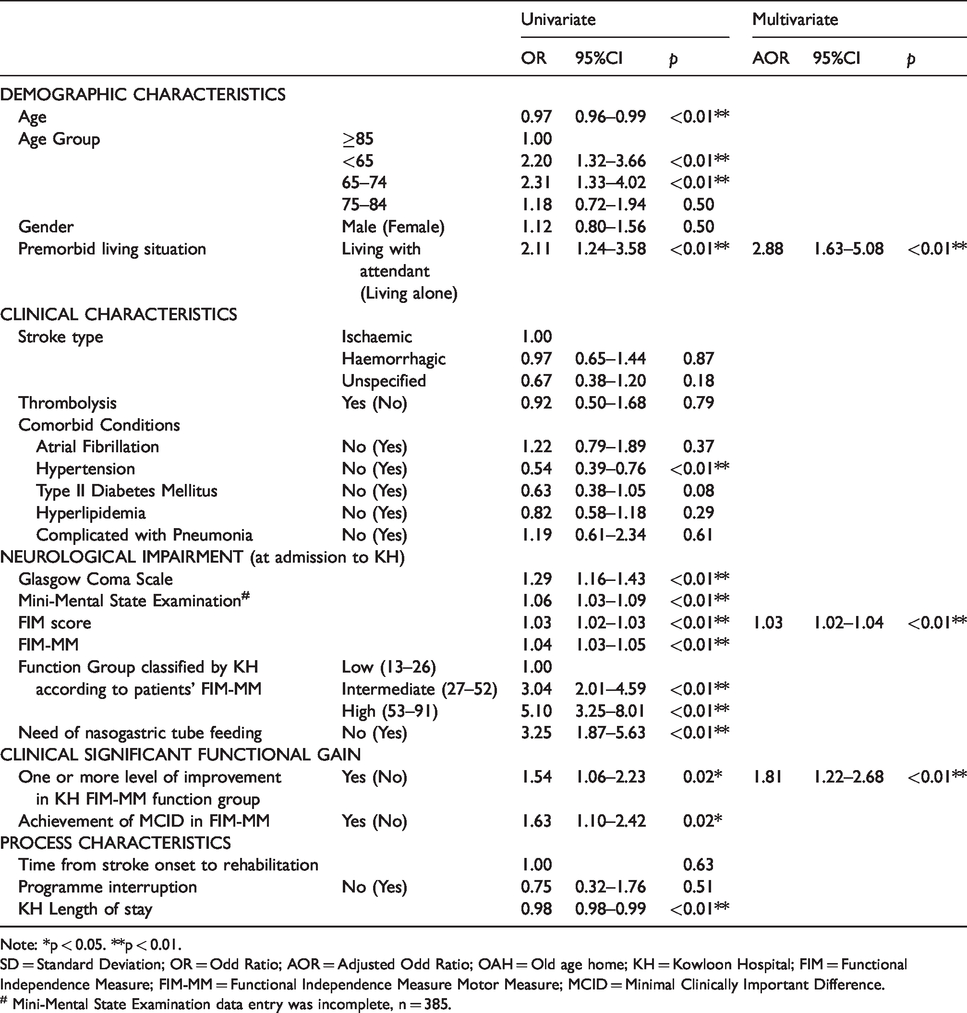
Note: *p < 0.05. **p < 0.01.
SD = Standard Deviation; OR = Odd Ratio; AOR = Adjusted Odd Ratio; OAH = Old age home; KH = Kowloon Hospital; FIM = Functional Independence Measure; FIM-MM = Functional Independence Measure Motor Measure; MCID = Minimal Clinically Important Difference.
# Mini-Mental State Examination data entry was incomplete, n = 385.
Discussion
This study identified factors independently associated with achieving “clinically significant functional gain” and returning home when being discharged after in-patient stroke rehabilitation programme. Some findings were consistent with previous overseas studies while some findings were conflicting or new. These findings provided us with more clues for identifying stroke patients with higher possibility of discharge to home so that we could start the discharge planning well in advance and accordingly; for instance, providing support for pre-discharge preparation such as caregiver training by nurses and therapists, exploration of home environmental barrier by occupational therapist, referral to community support.
It was coherent with previous studies that younger age was associated with better functional gain in both univariate and multivariate analysis (Brown et al., 2015; Fung, 2004; Scrutinio et al., 2015). However, in our findings it was identified that the age group 65–74 years old were obviously not yet too old to be labelled with limited rehabilitation potential; this age group was associated with better functional gain when being compared with age group 75–84 years old and age group >85 years old. On the other hand, age was commonly reported as a significant predictor of discharge to home (Itaya et al., 2017; Mees et al., 2016; Nguyen et al., 2015). However, the factor age was eliminated in the multivariate logistic regression model for predicting discharge to home. Significant correlation (Pearson coefficient −0.25) between age and initial FIM scores revealed the confounding effect.
Premorbid living with relative/attendant was not found to have a strong association with functional gain but found to be the strongest predictor for discharge to home regardless of their age, cognitive and motor function. The result was congruent with a previous report (Mees et al., 2016). It was similar to marital status which was reported to be a significant predictor (Nguyen et al., 2015) but premorbid living with relative/attendant represent better the possible availability of care giver from other family members. The association was even stronger for stroke survivors who were not independent in self-care.
FIM-MM was commonly reported as a powerful predictor for discharge to home (Itaya et al., 2017; Mees et al., 2016; Nguyen et al., 2015). Likewise, the association was even stronger for stroke patients premorbid living alone as showed in univariate analysis. However, this study showed FIM score to be the significant predictor instead of FIM-MM in multivariate logistic regression. It echoed that the cognitive measure although may not be a powerful predictor as FIM-MM, also contributed to discharge to home (Itaya et al., 2017; Nguyen et al., 2015). Healthcare professional should consider patients’ cognitive function as it was related to compliance to training, coping skill when discharged home, etc.(Fong et al., 2001). On the other hand, stroke patients in the Intermediate KH FIM-MM function group generally had the best FIM-MM gain. This was coherent with the large scale linear regression study by Brown et al. (2015). It was suggested that the relationship between initial FIM score and FIM-MM gain was not linear and we did not simply interpret that the lower the FIM score the better the FIM-MM gain. There was a ceiling effect in using FIM which was also stated in a previous report (Scrutinio et al., 2015). The ceiling effect was more obvious in using the outcome variable one or more level(s) of improvement in KH FIM-MM function group. This outcome variable had a major drawback of masked functional gain by stroke patients in high FIM-MM group as it was impossible for them to have one or more level(s) of improvement in the triage system. Therefore, we recommended the use of “achievement of MCID of improvement in FIM-MM” in our related review in the future. Moreover, using IADL and higher performance measure can be considered in regard to the limitation of FIM.
There were four new but interesting findings. Despite the fact that GCS is readily available in many settings, GCS had not been explored in prediction of functional gain and discharge destination. In this study, “with one more mark in GCS at admission to KH” showed significant association with functional gain. On the contrary persistent low conscious level implied limited participation in rehabilitation or even self care activities such as oral intake (Ikenaga et al., 2017). Secondly, stroke patients with hemorrhagic stroke were about 2 times more likely to achieve MCID of improvement in FIM-MM in this study. This appeared to be a conflicting finding as hemorrhagic stroke was generally more severe than ischemic stroke (Meyer et al., 2015; Sheedy et al., 2014). In this study, only survived hemorrhagic cases were transferred to KH and many of the patients at KH included were from rehabilitation ward instead of general or geriatric ward. This may imply that hemorrhagic stroke patients at KH were of less severity with better potential when compared with the total hemorrhagic stroke population. Thirdly, prediction of returning home using FIM progression instead of functional independence, clinical characteristics or social support has not been studied sufficiently (Mees et al., 2016). The new finding one or more level(s)of improvement in KH FIM-MM function group being a predictor in multivariate regression although could not help early prediction on admission, it was possible to study the use of interim FIM progression for prediction of discharge destination and evaluation of discharge plan in the future. Fourthly, having diagnosis of hypertension was about 2 times more likely to be discharged home in univariate analysis. This factor has been explored but no conclusive result was found (Mees et al., 2016). Diagnosis of hypertension being advantageous for stroke survivors was not clinically plausible as it was a risk factor for further complication and mortality (Yuan et al., 2018). After further review of the data set, it was found that larger proportion of the stroke patients without hypertension diagnosis were of unspecified stroke type and were of lower initial FIM score. Further study should be conducted to clarify if the result was due to error such as underdiagnosis of hypertension at admission for severe or complicated cases.
Several limitations of this study should be addressed. First, the sample size was relatively small when compared with previous comprehensive studies on different variables. It could lead to reduced chance of detecting true effect of variables especially the less common ones such as programme interruption. The limited event per variable also did not allow further multivariate analysis in specific group such as stroke survivors premorbid living alone. Future study with longer period of review and larger sample size could increase the statistical power and allow investigation of long term outcomes. Second, this was a single-centre study. Although this ensured the uniformity of data collection and rehabilitation process, it limited the generalizability of the results so the sample represented certain proportion but not overall stroke population in Hong Kong. Third, this study was limited by the retrospective data from the electronic database. Although manual data collection error could be minimized, the predictor variety was limited by the source. Some variables such as walking distance and economic status which were suggested to be associated with discharge destination by Brown et al. (2015) and Mees et al. (2016) were not available. Most treatment process such as acute stroke unit care versus general medical care, surgical, thrombolytic or endovascular treatment versus conservative treatment, need of mechanical ventilation or intensive care were not also investigated. Fourth, some data for instance, MMSE was incomplete which might lead to biased result.
Conclusion
This study shows that age, FIM and premorbid living with attendant remain as powerful predictors for “clinically significant functional gain” and “discharge to home” for stroke survivors. Other predictors including GCS and one or more level(s)of improvement in KH FIM-MM function group are newly identified. Early prediction of stroke discharge outcome helps medical and rehabilitation professionals to focus on the use of appropriate intervention strategies and pre-discharge preparation.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.