
Abstract
Objective
While musculoskeletal disorders (MSD) and physical strength have been extensively studied in health care professionals, little attention has been paid to health care support staff, such as patient care assistants and operation patient assistants, whose jobs are physically demanding. The purpose of this paper was to examine the musculoskeletal symptoms and physical strength of newly recruited health care support staff.
Method
Convenience sampling was conducted on 111 newly employed health care support staff in a public hospital. A custom-made pre-placement examination was performed. Data were analysed using descriptive, correlation, and regression analyses.
Results
Nearly one-third (32%) of the newly recruited health care support staff had experienced musculoskeletal symptoms in at least one body part during the preceding 12 months. Two-thirds (68%) of subjects were physically inactive, and sixty percent was overweight or obese. Handgrip strength was weaker than the local norm. The subjects’ dominant handgrip strength, bilateral lifting, pushing, and pulling force were significantly correlated. Only bilateral lifting was significantly associated with MSD among the newly recruited health care workers.
Conclusions
This study reports the baseline prevalence of MSD symptoms in the newly recruited health care support staff. Their sedentary lifestyle and suboptimal physical strength may render them susceptible to occupational injuries and disease. An effective occupational health programme that provides periodic health surveillance should be considered for high-risk health care workers to allow proper interventions in a timely manner.
Keywords
Introduction
Musculoskeletal complaints are commonly reported by health care workers. As suggested by the literature, musculoskeletal injury contributes to absenteeism at work (Hafner et al., 2018), work restrictions (de Fernandes & Burdorf, 2016), and disabilities (van Duijn et al., 2004), impacting the health care workers' productivity and quality of life (Lopes et al., 2019; McPhail et al., 2014). Such injuries also affect an organization's capacity to meet the care needs of patients. Among health care workers, the support staff, such as patient care assistants, operation patient assistants, and health care assistants, is one of the groups at high risk of developing such complaints, given the heavy demands of their jobs. In particular, patient care assistants and health care assistants are responsible for various patient care activities including changing diapers, bathing, and transferring patients, whereas operation patient assistants are accountable for transporting hospital beds, equipment, and linens; they also prepare and deliver meals to patients. These health care support staff are involved in direct patient care and other roles that are physically demanding. While the health care support staff is vulnerable to sustaining work-related musculoskeletal disorders (WMSD), little research has been conducted to examine the level of musculoskeletal complaints in the newly recruited support staff. Previous studies focused on health care professionals, such as physicians, dentists, and nurses, who suffer from WMSD (Tinubu et al., 2010; Yasobant & Rajkumar, 2014). Non-health care professionals, such as the health care support staff, tend to be under-served by the research community. As support staff plays a vital role in meeting the care needs of the patients, understanding whether they can cope with the physical demand of the job and whether accommodations and training are needed to support them is crucial. This is particularly the case for newly recruited health care support staff who may not be aware of the implications of the physical demands of the job. Since health care workers were found to experience more musculoskeletal complaints as their work experiences increase (Tinubu et al., 2010), studying newly recruited health care support staff is significant so that strategies can be developed by the organizations to help them prevent occupational injury, particularly musculoskeletal disorders (MSD), and to maintain a good quality of life. Preventive measures may allow organizations to focus their efforts to effectively reduce the prevalence of MSD for this vulnerable population.
MSD have been widely studied in different occupational groups, especially in hospital and home care workers. Anderson and Oakman (2016) conducted a systematic review of 26 articles to understand the prevalence and risk factors for WMSD in allied health professionals. The review showed that WMSD prevalence rates ranged from 28% to 96% over a one-year time frame, with the lower back being the most affected area. Lower back pain was reported as the most common MSD in Japanese nurses (Smith et al., 2006), Chinese nurses (Smith et al., 2004), Taiwanese nursing aids (Feng et al., 2007), and from Hong Kong nurses (Yip, 2002), followed by shoulder pain (Smith et al., 2006, 2004), and knee pain in nurses in Greece and Iran (Alexopoulos et al., 2011; Mehrdad et al., 2010). Despite the abundant literature on MSD, no local study was found on the prevalence of musculoskeletal complaints in newly recruited health care support staff.
Physical strength is an important characteristic of workers who perform physically demanding jobs. Handgrip strength has been reported as the best predictor of the capacity to carry weight (Von, 2000) and of general muscle strength (Wind et al., 2010), thus handgrip strength is used as an estimation of a worker’s overall physical capacity. Some studies reported that strong grip strength may reduce the risk of musculoskeletal injury or accident (Chaffin et al., 1978; Waters et al., 1993).
The association between MSD and lifting, pushing, and pulling force had been documented in the literature (Anap et al., 2013; Hoozemans et al., 2002). In a systematic review of longitudinal studies, da Costa and Vieira (2010) identified heavy lifting as a risk factor contributing to MSD. Hoozemans et al. (2002) suggested a strong relationship between pushing and pulling and shoulder complaints. Health care support staff are required to perform frequent patient transfers that require lifting as well as pushing and pulling stretchers or wheelchairs. Therefore, isometric grip strength, bilateral lifting, pushing, and pulling force are captured in this study in job-specific physical examinations, echoing the literature's suggestion of a connection with MSD.
Musculoskeletal injuries, a leading cause of worker disability, occur more frequently when the physical demands of a job exceed the worker's physical capabilities (Blue, 1993). Furthermore, workers who adopt unusual or restricted postures appear to be at higher risk of developing musculoskeletal complaints and often exhibit reduced strength and lifting capacity (Gallagher, 2005). Therefore, physical strength and musculoskeletal disorders were selected in this study to screen for pre-existing conditions that may place workers at additional risk.
Health care workers who are unable to meet the physical demands of their jobs are considered to be at risk for musculoskeletal injury. As a result, those who work in high risk service jobs, such as hospital orderlies, are commonly given post offer, pre-placement physical examinations. Various studies have reported on the effectiveness of pre-employment examinations at preventing occupational injury and disease in workers (Laflin et al., 1997; Legge et al., 2013). Physical ability tests have been used as an effective means of improving the quality of matches between job demands and worker abilities, thereby enhancing work performance and reducing the risk of injury. Anderson (2006) reported a 57% reduction in back injuries and a 41% reduction in overall injuries, on average, as a result of the implementation of such a testing program. The overall value of pre-placement examinations is acknowledged by the research community, and custom-made pre-placement examinations geared towards the specific needs of various jobs in terms of equipment/process utilized, routine, and workload are additionally promoted by Shrivastava et al. (2014).
While there is a tremendous amount of available literature that discusses MSD and overall physical strength of health care professionals (Burdorf et al., 2013; Fang et al., 2013; Feng et al., 2007), a notable gap exists in understanding the specific risks for newly recruited support staff who are at high risk of developing MSD due to their demanding jobs. This study aimed to address this gap by examining the musculoskeletal complaints and overall physical strength of the newly recruited health care support staff through the use of a custom-made pre-placement examinations. Another purpose of this study was to screen for pre-existing conditions that may place workers at additional risk, especially considering the staffing shortages and aging workforce in public hospitals. The goal of gathering the baseline information on their musculoskeletal complaints and overall physical strength was to determine if they were capable of performing the essential functions of their jobs and whether accommodations and training are required to better support them. This baseline information would also guide the organization in the development of preventive measures to promote occupational health and increase productivity of health care support staff.
Methods
This study adopted convenience sampling. A total of 111 health care support staff at the Hong Kong West Cluster Hospitals were recruited from April 2013 to December 2013. All participants were involved in direct patient care and support that required heavy lifting and transfer. This study was approved by the Ethical Committee of the Institutional Review Board of the University of Hong Kong and the Hospital Authority Hong Kong West Cluster (Reference Number: UW 14-065).
Study design and measures
A custom-made pre-placement examinations was conducted by the occupational physician and two occupational therapists who are core members of the Occupational Medicine team in addition to the standard pre-employment health check. The process included a clinical examination, a self-reported questionnaire, an assessment of bilateral handgrip strength, lifting, pushing and pulling, and measurement of body weight and height. The occupational therapists were also responsible for providing work assessment and work capacity evaluations, which were within the scope of their expertise. The adoption of a custom-made pre-placement examinations aligned with the recommendations of Shrivastava et al. (2014).
Musculoskeletal complaints
Musculoskeletal complaints were identified through clinical examination and a self-reported questionnaire. While the self-reported questionnaire offers a subjective evaluation of the symptoms, clinical examination provides an objective lens. The questionnaire was divided into two parts. The first part contained questions regarding demographics and physical activity patterns, hobbies, work history, occupational safety and health training record, as well as a request for a record of sick days taken as a result of musculoskeletal disorder or injuries. The second part of the questionnaire was symptom recording as stipulated in the Nordic Musculoskeletal Questionnaire (NMQ). The NMQ is widely used for reporting musculoskeletal symptoms and has high reliability and validity (Barros & Alexandre, 2003; Fang et al., 2013). The questions included an anatomical diagram with labels on nine body parts. These included the neck, shoulder, elbow, wrist and hand, upper back, lower back, hip and thigh, knee, ankle, and foot regions. Respondents were asked if they experienced pain in each of the above body parts in the past 12 months. If so, they were then asked if the pain interfered with their normal work in the past 12 months. The response was scored on a dichotomous scale. The use of a 12-month recall period to analyze the prevalence of musculoskeletal disorders aligns with the Asian studies’ practice (Feng et al., 2007; Smith et al., 2006; Yip, 2002). After the questionnaire was completed, the subject was assessed by a clinical examination performed by the occupational physician, followed by the physical strength assessment performed by occupational therapists.
Grip strength
Grip strength was measured using a Jamar Plus+ hand dynamometer. The second grip handle and the standard testing position approved by the American Society of Hand Therapists (Fess, 1992; Innes, 1999) were utilized. Subjects were asked to sit in a straight-backed chair with their feet flat on the floor, shoulder adducted and neutrally rotated, elbow flexed at 90 degrees, forearm in a neutral position, wrist at between 0 and 30 degrees extension and between 0 and 15 degrees ulnar deviation. Both hands were measured three times, with 15–20 seconds of rest between measurements. The mean of three trials in kilogram force was used as the handgrip strength.
Bilateral lifting, pushing and pulling
The Baltimore Therapeutic Equipment (BTE) Primus tool 181 (BTE Technologies, Inc., USA) was used to measure isometric lifting capacities. Subjects were instructed to lift the tool with maximum effort at waist level under the supervision of an occupational therapist. A standard position with the elbow flexed at 90 degrees and feet in an even stance was advised. The mean of three trials in kilogram force was used as the lifting force and the coefficient of variation was calculated.
Bilateral push and pull was measured with the Chatillon DFE series digital force gauge in standing position. Isometric push and pull at waist level was measured, and the mean of three trials in kilogram force was used as the pushing and pulling force.
Data analysis
The results were analysed using PASW version 18. Risk factors were analysed using logistic regression and expressed as adjusted odds ratios (OR) with 95% confidence intervals (95% CI). MSD was used as the dependent variable, with demographic items, grip strength, bilateral lifting, pushing and pulling force, body mass index, physical activity patterns, occupational safety and health training used as the independent variables or predicting factors. The Pearson Correlation was used to assess the correlation between dominant grip strength, bilateral lifting and pushing and pulling. The Pearson Chi-Square test was used to assess the link between weak grip strength and reported MSD symptoms and gender and MSD symptoms. For assessing group difference in MSD, the t-test was used for continuous data (including handgrip strength, bilateral lifting, pushing and pulling force and body mass index), and the Mann Whitney U test was used for ordinal data (physical activity pattern) comparison. In all tests, p ≤ .05 was considered significant at a 95% confidence interval.
Results
A total of 111 health care support workers were recruited with a mean (SD) age of 46.9 (8.4) years. Demographic and baseline characteristics are summarised in Table 1. The mean (SD) body mass index was 24.4 (3.8), ranging from 16.4 to 40.4. Sixty percent of the subjects were overweight or obese. Sixty-eight percent of the subjects seldom exercise or exercise with a frequency of less than once per week. Furthermore, 73% of subjects had not received occupational safety and health training in the previous year, and 67% of subjects were new to the health care field.
Baseline characteristics of the newly recruited health care workers (n = 111).
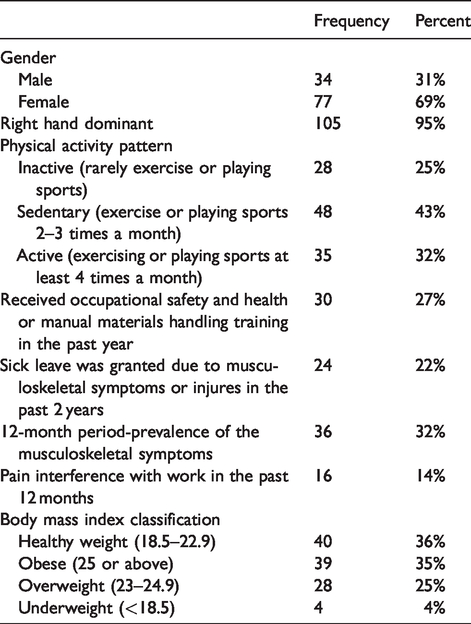
The results indicated that 32% of the newly recruited support staff had experienced musculoskeletal symptoms in at least one body part during the preceding 12 months. Fourteen percent of subjects reported that their musculoskeletal symptoms interfered with work, meaning that they had taken at least one day of sick leave in the past 12 months. The most commonly affected body part was the knee at 15%, followed by the elbow at 12% and the foot at 11% (Table 2).
Pattern of 12-month prevalence of musculoskeletal symptoms and physical strength by gender (n = 111).
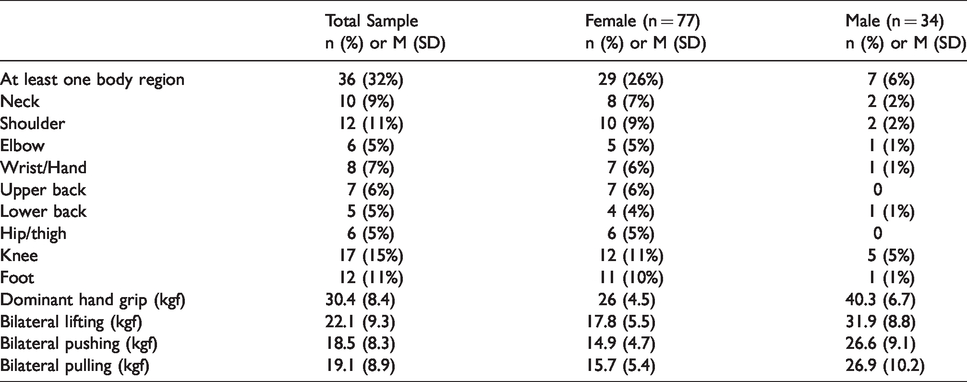
Mean scores of handgrip strength, bilateral lifting, pushing and pulling force in both genders are depicted in Table 2. There was a positive correlation found between dominant handgrip and bilateral lifting (r = .69, p < .01), dominant handgrip and bilateral pushing (r = .68, p < =.01) and dominant handgrip and bilateral pulling (r = .64, p < .01) (Table 3). Weak handgrip was identified in 10% of subjects, though 80% of the weak grip subjects were new to the health care service, and therefore may not have been familiar with the biomechanics involved in force exertion in health care.
Correlation coefficient of dominant hand grip strength, bilateral lifting, pushing and pulling force (n = 111).

**Correlation is significant at the 0.01 level (2-tailed).
With reference to Grobler (2013), weak handgrip was identified if a subject’s average handgrip minus 2 kg was lower than the normative mean value for their age and gender minus two standard deviations. There was no statistically significant association between weak grip and MSD symptoms (X2(1) = .09, p = .77) nor between gender and MSD symptoms (X2 (1) = .08, p=.08) (Table 4).
Association between weak grip and musculoskeletal symptoms, gender and musculoskeletal symptoms (n = 111).
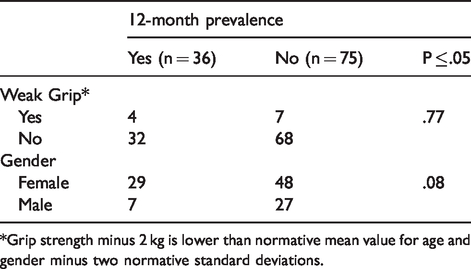
*Grip strength minus 2 kg is lower than normative mean value for age and gender minus two normative standard deviations.
Subjects who reported no MSD symptoms demonstrated significantly better bilateral lifting force (M = 23.5, SD = 9.5) than those with MSD symptoms (M = 19.2, SD = 8.2), t(106) = 2.29, p = .02. No significant difference was found between MSD symptoms and body mass index (t(109) = .16, p = .87), handgrip strength (t(109) = 1.1, p = .278), bilateral pushing force (t(106) = 1.27, p = .21), pulling force (t(106) = .85, p = .40), or exercise frequency (U = 1183, p = .26).
Logistic regression analyses revealed that only bilateral lifting was significantly associated with MSD among the newly recruited health care support staff (OR .893, CI = .82–.98, p = .01). The other predictors including age, gender, body mass index, grip strength, and physical activity patterns were not significantly correlated with MSD.
Discussion
This study reported the baseline prevalence of MSD in newly recruited health care support staff. Most of the subjects were physically inactive, obese, or overweight, and also lacked occupational safety and health training. Their handgrip strength was weaker than the local norm. The findings in this study serve as very valuable baseline information that will assist the organization in developing robust preventive strategies to aid this vulnerable population in maintaining a low prevalence rate of MSD and assuring a high quality of life for years to come. Specifically, since their job demands heavy lifting, which puts them at risk of developing MSD, personal and occupational health education should be offered and recommended, especially to those who are new to the health care field. Refresher courses or workshops should be made available on a regular basis to this underserved group that does not have the professional background to meet the heavy work demands. A buddy system that involves pairing the newly recruited support staff with a seasoned support staff and access to an occupational therapist would help to ensure both technical and psychological support are available to enforce proper practice in ergonomics, safety measures, and patient lifting techniques.
MSD prevalence
This study found a relatively low prevalence of MSD symptoms in health care support staff. The 12-month prevalence of MSD symptoms found in this study was 36%, as compared to 70% with Chinese nurses (Smith et al., 2004), 85.5% with Japanese nurses (Smith et al., 2006), 66% with female Taiwanese nursing aides (Feng et al., 2007), and 66% with patient care associates in the United States (Sembajwe et al., 2013). One of the major reasons for this could be that the subjects were newly recruited health care workers and therefore did not have the impact of years of experience, psychosocial, and workplace issues. While this finding may not be unexpected, it does serve as a crucial database for the organization to understand the needs of the support staff who tend to receive minimal attention and support given their low status in the organizational hierarchy. In particular, it helps the organization better identify employees who may have a pre-existing conditions that puts them at additional risk. For example, 60% of the subjects were obese and 68% of subjects exercise less than once per week. This implies that the sedentary lifestyle of the support staff may place them at additional risk for developing MSD. Preventive measures such as providing education on diet and exercise and fitness programmes should be considered to help the support staff remain fit for their jobs. Also, the database information can help the organization develop a customized strategic plan that focuses on vigorous preventive measures to reduce and prevent the occurrence of MSD among the support staff. For example, two-thirds of the newly recruited health care support staff are new to the health care service and did not receive occupational safety and health training. This creates an inherently high-risk group for developing MSD. Prevention is always better than treatment. Monitoring programmes should also be provided by the organization to prevent burnt out. The impact of long term exposure to physically demanding jobs of this nature increases the risk of developing more musculoskeletal complaints and should be on the watch list.
Different patterns of musculoskeletal complaint were noted despite the overall low prevalence. The newly recruited health care support staff in this study had a low prevalence of musculoskeletal complaints in the low back (5%), neck (9%), and shoulder (11%) regions. This finding deviates from what was reported in the literature. Low back pain, for example, is very common in health care workers due to the nature of their jobs, with prevalence at 56%–71%, while neck and shoulder pain at 40%–72% (Smith et al., 2006, 2004). Such substantial discrepancy between the newly recruited and experienced health care workers could be explained by years of experience working in these environments, and the psychological impact thereof. Interestingly, this study found that the knee (15%), elbow (12%) and foot (11%) were the top three problem areas that the newly recruited health care workers experienced trouble with as far as musculoskeletal complaints were concerned. This could be explained by a high percentage of subjects with obesity which increases the burden on weight-bearing joints like the knee and foot.
The subjects’ demographics shed light on the profile of the health care support staff. The sick leave prevalence in this study (14%) is slightly higher than that in Taiwan (11%) (Feng et al., 2007). In addition, this study reported a higher mean age of 46.9 as compared to other studies. For example, the mean age of the patient care associates in the United States was 41 (Reme et al., 2012), 43.3 with Taiwanese nursing aides (Feng et al., 2007), 34 with Chinese nurses (Smith et al., 2004), and 32.9 with Japanese nurses (Smith et al., 2006). The finding of this study showed a more mature group of health care workers. Okunribido et al. (2011) posited that older workers aged 50 and above were at a higher risk of developing MSD than the young workers aged 25 or below. It has implications for the organization in terms of developing preventive strategies to maintain a low MSD prevalence. For example, occupational health education and on the job training may need to take into account the supporting staff’s ability to use technology and equipment as the older workforce may not be tech-savvy. Also, the organization’s should be aware of the need and ready to accommodate the older workforce through methods such as providing alternatives to change jobs to match their changing physical capacity as the need arises.
Grip strength
In this study, the average dominant handgrip strength in females and males was 26 kgf and 40.3 kgf, respectively, which is lower than the norm, 28.5 kgf and 43.8 kgf, respectively (Tsang, 2005). This finding is in line with the findings of Wong and Kwok (2012), showing that the health care support staff with the highest physical job demands had the lowest level of handgrip strength. Similar findings have been reported in other studies (Grobler, 2013; Harbin & Olson, 2005). Conversely, high handgrip strength does not necessarily mean that a person is good at manual material handling, which is essential in the day to day operations of health care workers. Therefore, improvements in occupational safety awareness and the practice of proper posture in functional tasks of pulling, pushing, and lifting could be beneficial for newly recruited health care workers.
Regarding physical strength in the pre-placement examinations, only bilateral lifting force showed a significant association with musculoskeletal disease and it also had a strong correlation with dominant handgrip, bilateral pushing and pulling force. Therefore, bilateral lifting could be selected in the specific pre-placement examinations for the health care support staff and further study to better explore the cut off score is warranted.
Limitations
One of the major limitations of the study was sampling. The small sample size and recruitment of subjects from a non-probability sampling methodology undermined the ability to generalize the findings to a larger population. Recall bias also could not be excluded despite the adoption of a one-year prevalence measure, which is less susceptible to the influence of recall bias as compared to career prevalence (Anderson & Oakman, 2016). Given that all the subjects in this study were new employees and some were new to the health care field in general, the possibility of the subjects reporting their musculoskeletal complaints as WMSD could not be ruled out. As indicated by Adegoke et al. (2008), it might be hard to differentiate WMSD from musculoskeletal complaints and vice versa as they share similar presentation in the ways they respond to work demands. Since all the subjects in this study were new to their jobs, the impact of years of experience, work, and psychosocial factors on musculoskeletal complaints was not studied. Future studies could create a prospective design with a larger sample size studying the causal relationship of musculoskeletal complaints and years of experience or physical strength. Moreover, a longitudinal study is warranted to study risk factors such as age, high body mass index, psychosocial work demands, and heavy lifting that are associated with WMSD. A follow-up study on the presence of musculoskeletal symptoms and the subsequent sick leave granted would be warranted.
Conclusion
This study reports the baseline prevalence of musculoskeletal disease in the newly recruited health care support staff. Their sedentary lifestyle and suboptimal physical strength may make them susceptible to occupational injuries and disease. An effective occupational health programme that provides periodic health surveillance should be considered for high-risk health care workers to allow proper interventions in a timely manner.
Footnotes
Acknowledgements
The author is grateful to all the participants in this study as well as the generous support from the human resources service centre of Queen Mary Hospital. Furthermore, a special thank you to Henry Kwok for his exemplary guidance and constant support throughout the project. I am also grateful to Henry Fung and Mary Chu for the support in this project. Last but not the least, I would like to extend the deepest gratitude to Sincere Wong for her invaluable input and assistance that greatly improved the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.