
Abstract
Background:
Home health workers are at high risk for musculoskeletal injuries due to the unique nature of their work. This study addressed the lack of evidence on the incidence of musculoskeletal pain in home health workers.
Methods:
A cross-sectional survey design was used to assess work factors and pain prevalence in a sample of home health workers recruited through social media platforms.
Results:
In this sample, the most prevalent work factors were: driving an SUV, using a home health shoulder bag, and documenting on a tablet. Eighty-eight percent of the sample reported experiencing musculoskeletal pain within the last 3 months. Lower back pain was the most prevalent. Inferential analysis showed no statistically significant association between pain and work factors.
Conclusion:
There is a high rate of musculoskeletal pain among home health clinicians. More research is needed to identify root causes of musculoskeletal pain to develop preventative interventions.
Keywords
Introduction
Home health workers are at a greater risk for musculoskeletal injury due to their unique occupational demands.1-4 About 40% to 48% of a home healthcare worker’s time is spent in poor postural positions that do not support optimal musculoskeletal functioning, increasing the risk for shoulder, neck, and back issues. 3 Home healthcare workers’ increased risk may be attributed to the unpredictable and variable work environment, increased isolation, decreased peer support, organizational demands, lack of evidence-based handling aids, and limited space for transfers and handling tasks.2-4 There are many opportunities for investigation and intervention to mediate the risks for this population. Due to the overwhelming individual and structural barriers to musculoskeletal wellness for home health workers, tailored, integrated, and holistic health promotion initiatives must be developed. 1
Few studies have explored the specific ergonomic threats that place home health workers at an increased risk for musculoskeletal disorders. Qualitative studies have explored home health workers’ perceptions of both threats to their health and well-being and how to manage them; however, very little quantitative evidence exists in the realm of ergonomics and the musculoskeletal health of this population.5,6
In terms of viable intervention, the evidence does suggest that secondary prevention interventions, such as workshops, peer-led groups, and goal setting, in addition to conventional delivery of educational content on ergonomics, may prove beneficial for decreasing the rate of injury, pain, and disability among home health workers. 7 There is still a gaping lack of research exploring the rate and prevalence of musculoskeletal disorders among home health workers, especially among occupational and physical therapists; while the profession of nursing provides more clarity related to this topic. 8 It is first important to understand the nature of the problem before developing interventions to solve it. Further quantitative analysis of the ergonomic and musculoskeletal well-being among home health workers will deepen our current understanding of risk factors and subsequently promote the exploration of effective mitigation strategies. 9
The purpose of this study was to determine the prevalence of musculoskeletal injury among home health workers. A survey was conducted among current United States (U.S.) home health workers to determine common work practices and pain prevalence, as well as examine associations between these variables.
Methods
Study Design
This observational study examined work factors and musculoskeletal pain among home health workers in the United States. Data were collected via a self-report cross-sectional survey distributed through social media platforms. The survey was administered through Qualtrics 10 software.
Participants
This study was targeted to home health workers in the United States. Inclusion criteria for this study was being a current home health worker in the United States.
Instrument
A musculoskeletal pain survey targeting home health workers was developed by the authors as there was no existing survey found looking at musculoskeletal factors among home health workers. The primary author is a clinical expert in the field of home health. The survey covered the following factors: demographics, home health work factors, and musculoskeletal pain.
Home health work factors were developed based on factors unique to the home health setting: vehicle, bag, and documentation factors. Patient care activities were excluded from analysis in this study as they are not unique to the home health setting.
All participants were asked if they had experienced musculoskeletal pain within the last 3 months. If a participant responded yes, then a pain survey was presented. If they answered no, the survey was concluded.
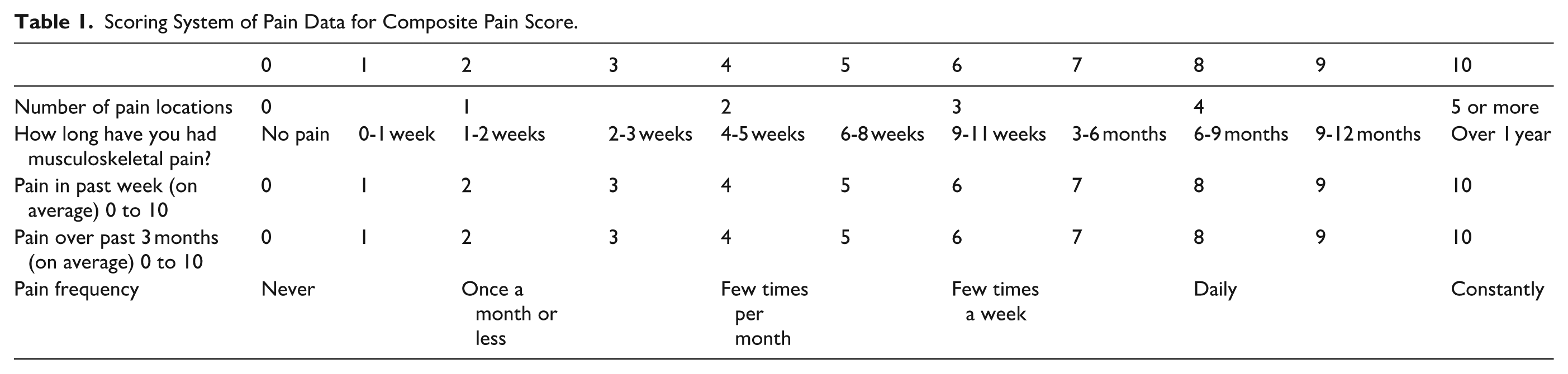
Pain was assessed via 5 questions looking at pain location, duration, frequency, and severity. Pain location has the participants identify specific body parts where they have had musculoskeletal pain. Duration categories were adapted from the Örebro Musculoskeletal Pain Screening Questionnaire. 11 The Örebro Musculoskeletal Pain Questionnaire (OMPQ) is a screening tool designed to predict long-term disability and work absenteeism in individuals with acute and chronic musculoskeletal pain. Pain severity was assessed using a visual analog scale asking for average pain over the past week as well as the past 3 months. Every pain question was scaled to a 10-point scale yielding a potential composite score ranging between 0 and 50 (See Table 1).
Scoring System of Pain Data for Composite Pain Score.
Participants were also asked if they felt being a home health worker put them at risk for musculoskeletal pain overall, as well as specific activities that they felt contributed to their pain.
Content validity for the survey was established by having the survey piloted by a home health clinician who took the survey and provided feedback to ensure it addressed everyday home health work tasks and likely pain elements. This pilot testing did not prompt any amendments to the questionnaire.
Data Collection
The survey was distributed via postings to 6 Facebook 12 groups targeting home health workers and the American Occupational Therapy Association CommunOT 13 forum and was left open for responses for 1 month.
Data Analysis
Data were downloaded and analyzed using Microsoft Office Professional Plus 2019 version of Excel, 14 and inferential analysis was completed using IBM SPSS Version 27. 15
Ethics
The research study was reviewed and approved as exempt from Institutional Review Board under exemption category 2. Informed consent was obtained from all participants through an anonymous online consent form in Qualtrics prior to survey completion.
Results
Participants
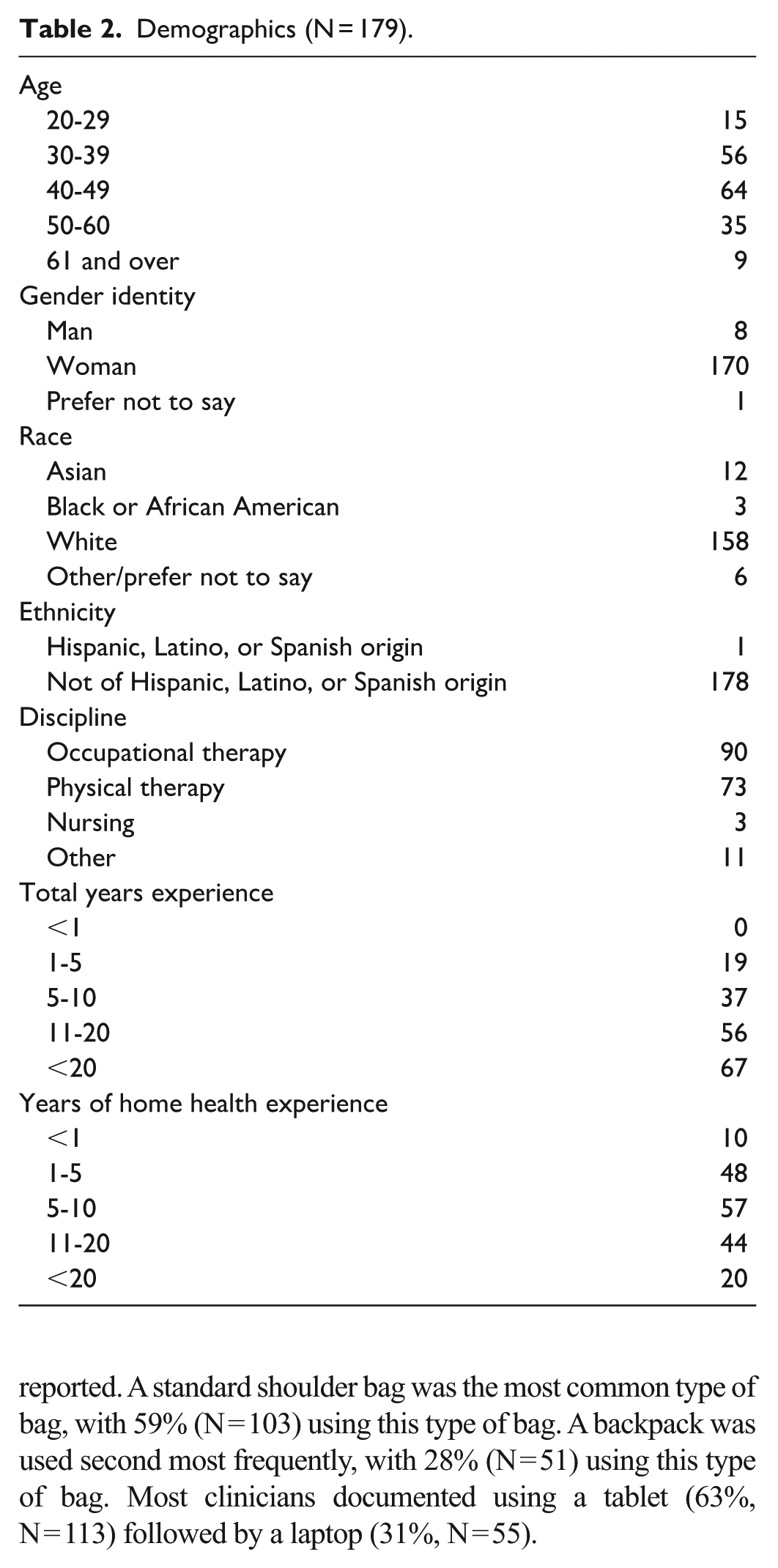
Following recruitment, 192 individuals accessed the screening survey. Four were excluded because they were not current home health workers, and 9 did not provide consent. The remaining 179 participants provided informed consent and completed the survey, yielding a final sample size of 179 home health workers. Participant demographics are presented in Table 2.
Demographics (N = 179).
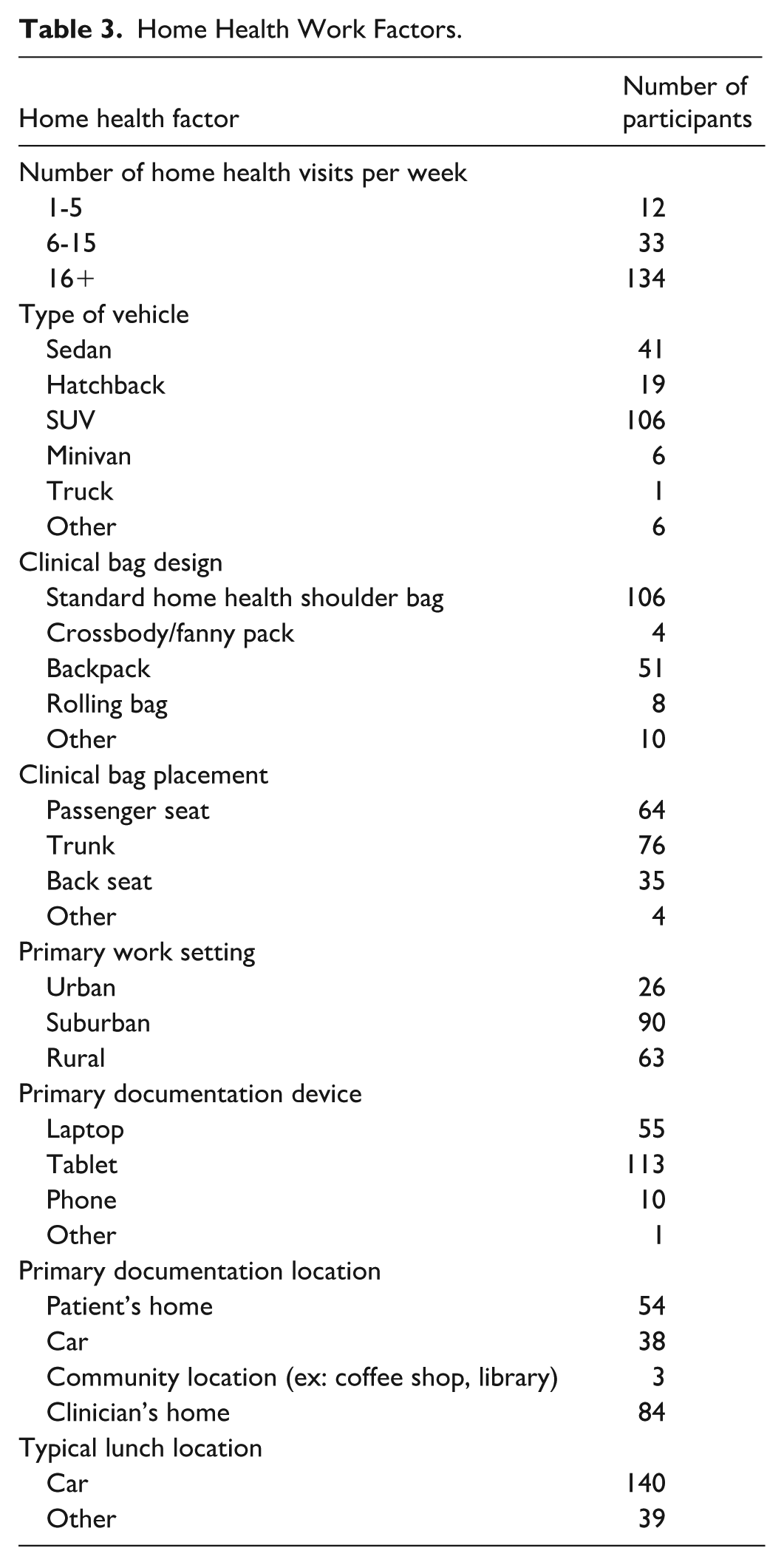
Home Health Work Factors
Data were collected on home health work factors (Table 3). A sport utility vehicle (SUV) was the most common mode of transportation, with 59% (N = 103) of respondents driving one. Sedans were the second most frequent transportation option (23%, N = 41) and some people used hatchbacks (11%, N = 19) while using a minivan, truck, or other transportation was rarely reported. A standard shoulder bag was the most common type of bag, with 59% (N = 103) using this type of bag. A backpack was used second most frequently, with 28% (N = 51) using this type of bag. Most clinicians documented using a tablet (63%, N = 113) followed by a laptop (31%, N = 55).
Home Health Work Factors.
Pain
Of the home health workers surveyed, 77% felt that working in home health put them at risk for musculoskeletal pain (Figure 1).
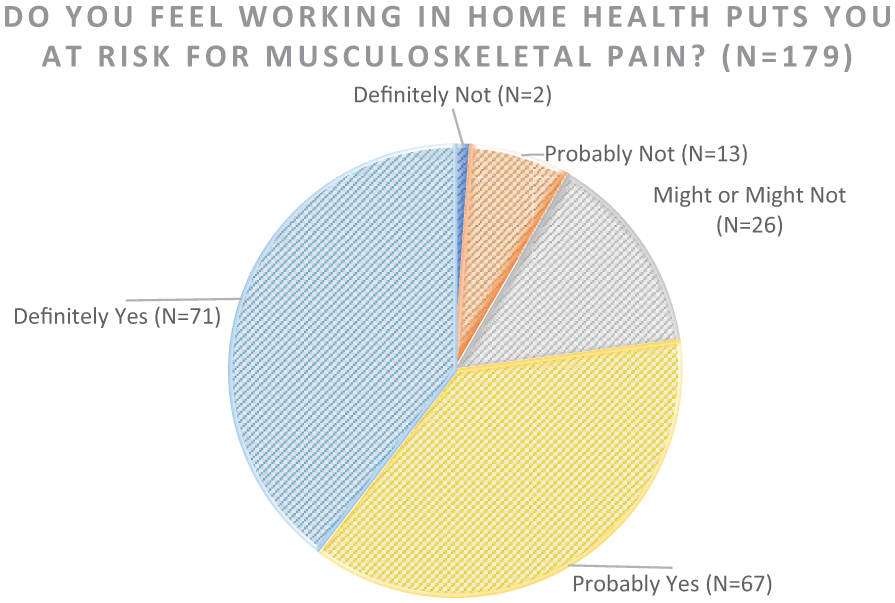
Home health worker perceived pain risk (N = 179).
Of the clinicians who responded to the survey, 88% (N = 157) reported musculoskeletal pain in the last 3 months. Of the respondents, 150 completed the pain questionnaire. Of those, 71 (48%) reported their pain had been present over a year. Lower back pain was the most common, with 65% of those reporting pain reporting lower back pain. Neck, Shoulder, upper back, and wrist and hand pain were also prevalent (see Table 4). On the 10-point pain scale, average pain score was 3.50 during the last week (SD 1.80) and 4.03 over the last 3 months (SD 1.90).
Pain Location (N = 150).

Clinicians were also asked during which tasks they experienced pain, and which tasks they felt contributed to their pain. Driving, providing direct patient care, and documenting were listed as the highest pain tasks in both domains (Figure 2).
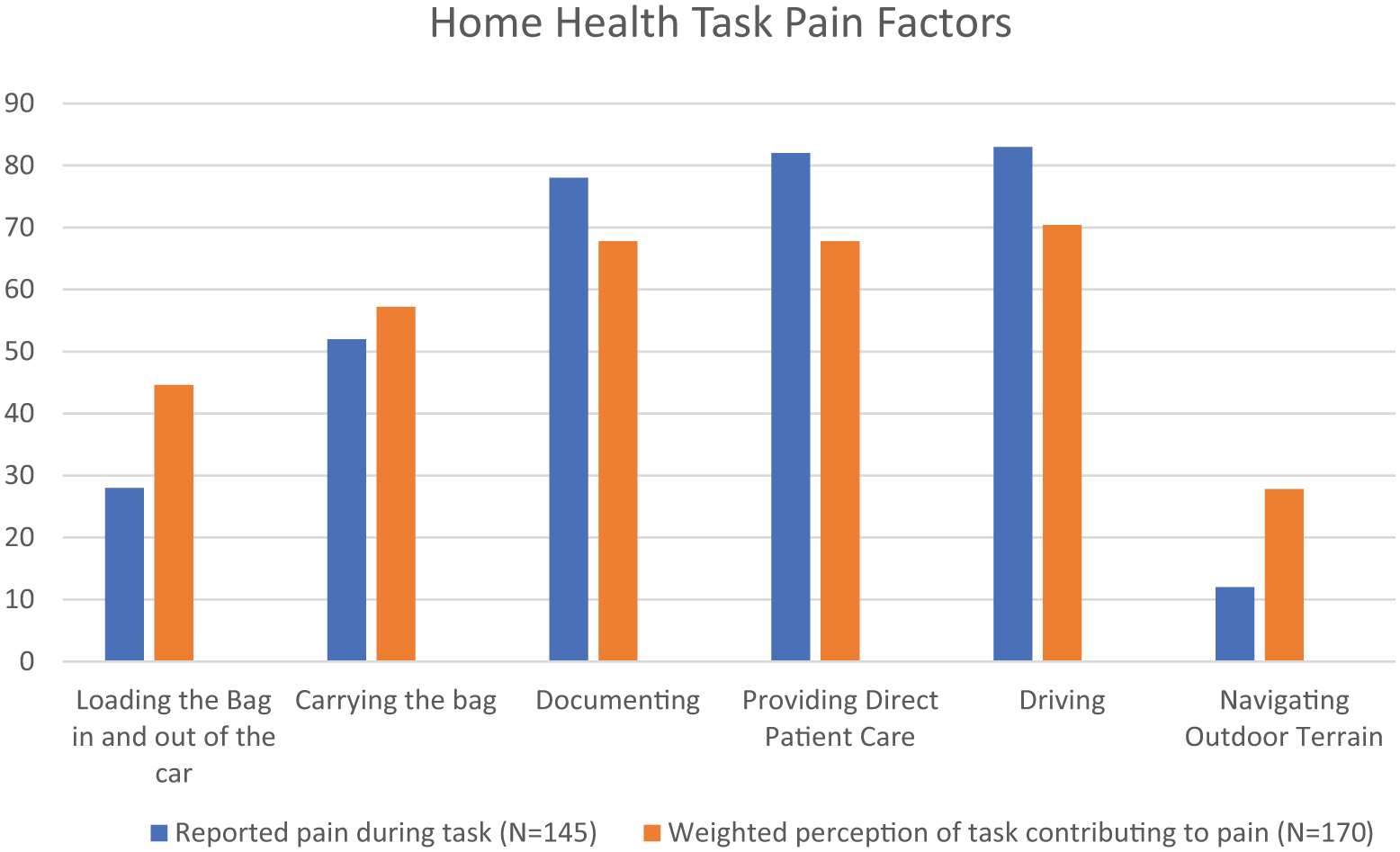
Home health task pain factors.
Inferential Analysis
Inferential analysis was completed to look for statistically significant differences among groups based on the home health work factors. For this analysis, in addition to a 0 to 10 pain scores, a composite pain score was calculated from the pain variables that included frequency and duration of pain (Table 1).
A series of chi-square tests were conducted to examine the relationships between home health work factors (including geography, vehicle type, bag type, bag storage location, documentation location, documentation device, and lunch location) and pain locations (low back, upper back, neck, shoulder, and wrist and hand). No statistically significant associations were found across the analyses (all P > .05). Three results were approaching significance with p value of less than 0.10: the result of bag type and upper back pain was χ²(4, N = 147) = 9.42, P = .052; the result of bag type and wrist and hand pain was χ²(4, N = 147) = 8.04, P = .090; and the result of the documentation device and upper back pain was χ²(2, N = 147) = 5.15, P = .076.
Inferential analysis using an ANOVA was completed for home health work factors (including geography, vehicle type, bag type, bag storage location, documentation location, documentation device, and lunch location) and pain factors (pain within the last week, pain within the last 3 months, and the composite pain score). The composite pain score was developed based on the pain variables (Table 4).
A one-way ANOVA revealed a significant effect of bag storage location within car on pain within the last week, F(4,142) = 4.19, P = .003. Post-hoc comparisons using Games-Howell test revealed no significant difference by group indicating the result is statistically detectable in aggregate (ANOVA), but not large enough between any 2 specific groups to be significant after correction. Additionally, there was an effect approaching significance of effect of bag storage location within car on composite pain score, F(4, 142) = 2.02, P = .095.
A one-way ANOVA revealed no significant differences (all P > .05) in composite pain score among groups based on home health factors, including geography, vehicle type, bag type, bag storage location, documentation location, documentation device, and lunch location.
Discussion
This study reveals a high pain prevalence among home health workers. No significant relationships emerged between work factors and pain. However, analysis may have been limited by the high levels of pain present throughout the sample.
These findings parallel previous work examining the incidence of injuries in health care workers. Previous cross-sectional, observational studies suggested high rates of lower back, shoulder, and neck pain among home health care workers. 16 Similar to previous work examining workers compensation claims among long term care healthcare workers, 17 our study found lower back pain to be the most prevalent. However, in long-term care, shoulder and other upper extremity injuries were second most common, whereas neck pain was the second highest. 12 This may be due to lack of a formal workstation and high rates of tablet use for documentation. Furthermore, up to 89% of injuries sustained by long term healthcare workers were chronic in nature. 17 This aligns with previous assertions that the musculoskeletal injury risk profile was different for home healthcare workers because of their lower patient-handling hours and increased participation in transportation-related activities. 9 Therefore, the risk profile of home health workers may significantly differ from other healthcare worker populations.
Qualitative analysis of home health worker perspectives revealed that the autonomy home health workers experiences may also impact their risk profile. 5 Home health workers have greater independence and therefore may complete more administrative tasks, including scheduling, ordering equipment, and triaging medical issues. Additionally, because home health care workers are alone in the home, without access to physical assist or lifting aides, they may feel pressure to mobilize clients without assistance, thus increasing their risk of musculoskeletal injury. Future research should investigate if pain rates are associated with time distribution of driving, treatment, and administrative tasks.
Although inferential analyses were conducted to explore potential relationships between various home health work factors and pain outcomes, the results did not reveal any statistically significant associations. However, a few findings approached significance, suggesting possible trends worth further investigation. Specifically, relationships between bag type and both upper back and wrist/hand pain, as well as between documentation device and upper back pain, showed P-values below .10. Additionally, a significant effect was found for bag storage location within the car on pain experienced in the past week, though post-hoc comparisons did not identify significant differences between specific groups. These findings may indicate subtle patterns that could become more evident with a larger sample or refined pain measures.
Given the high pain prevalence among home health workers found in the present study, home health organizations should develop proactive interventions to combat potential pain-risk factors including assessing documentation tools and bag types and providing ergonomics education. This study has some limitations. The most significant limitation of this survey is the distribution method. The recruitment methodology only targeted home health workers who engaged in social media. As the authors are occupational therapists, they had more access to occupational therapy forums, so the profession of occupational therapy may be over-represented in this survey. Another possible limitation is that the type of social media chosen (Facebook) may lend to certain age groups. Others who use other types of social media besides Facebook may not have seen it. Additionally, the survey recruitment flyer mentioned pain, so there may have been a recruitment bias favoring people with pain. Finally, the survey asked about musculoskeletal pain but it did not address all potential causes or tasks associated with musculoskeletal pain. The composite pain scale used in this study was exploratory and may not have been sensitive enough to reflect differences among groups. Based on the observational nature of this study, causal relationships are not established.
Recommendations for future research include repeating this study with an even larger sample of individuals and examining how specific patient-care tasks and work-week time allotment impact pain presence. Additionally, kinematic analysis of home health work tasks may reveal causes of high levels of pain.
Conclusion
There is a high incidence of musculoskeletal pain in this sample of home health workers. Driving, providing direct patient care, and documentation were observed to be the most painful work tasks. Lower back pain was most common. More research is needed to identify root causes of musculoskeletal pain to develop preventive interventions.
Footnotes
Acknowledgements
The authors have no acknowledgments on this project.
Ethical Considerations
This project, Application # F2024_001, was reviewed by the Widener University Institute for Occupational Therapy Education Human Subjects Ethics Committee and was determined to be “not human subjects research” and thus was exempt from Institutional Review Board review.
Consent to Participate
Participants gave consent electronically prior to participating in this study.
Author Contributions
Sara Kate Frye participated in ethical approval, developing the survey, data collection, data analysis, and manuscript preparation and Kristen Kelly participated in the ethical approval, developing the survey, literature review, and manuscript preparation.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.