
Abstract
Abstract
Mental illness often leads to functional deficits that likely affect one’s driving performance and may even pose threat to other road users. However, having a mental illness does not automatically preclude one from driving which is essential to mobility and productivity. Indeed, evaluating their fitness-to-drive would be of necessary. Despite that, there is still a lack of a local driving evaluation service that specifically addresses the impact of mental illness on driving capacity. This paper discusses the needs to evaluate the fitness-to-drive of people with mental illness. It advocates the development of such specific driver assessment service with a local example as illustration. Lastly, some of the challenges related to the drivers’ responsibility to declare personal health status and large variety of assessment approaches are also discussed.
Introduction
Driving signifies independent community mobility and productivity. It is a complex task requiring a range of skills, such as cognitive, sensorimotor and psychosocial skills (Driver & Vehicle Licensing Agency, 2019). However, drivers with mental illness or those using psychotropic medications often experience functional deficits that would affect their driving performance and may increase risk of traffic accidents (Ménard & Korner-Bitensky, 2008). It is of great concern on how to identify this risky driver group. In this commentary, several issues regarding driver assessment for people with mental illness are examined. Firstly, the impact of mental illness on driving is briefly reviewed. Secondly, the needs for driving assessment are explored. Thirdly, the development of assessment centre for drivers with special needs is advocated and illustrated with a local example in mental health institute. Lastly, some of the challenges ahead are discussed.
Driving and mental illness
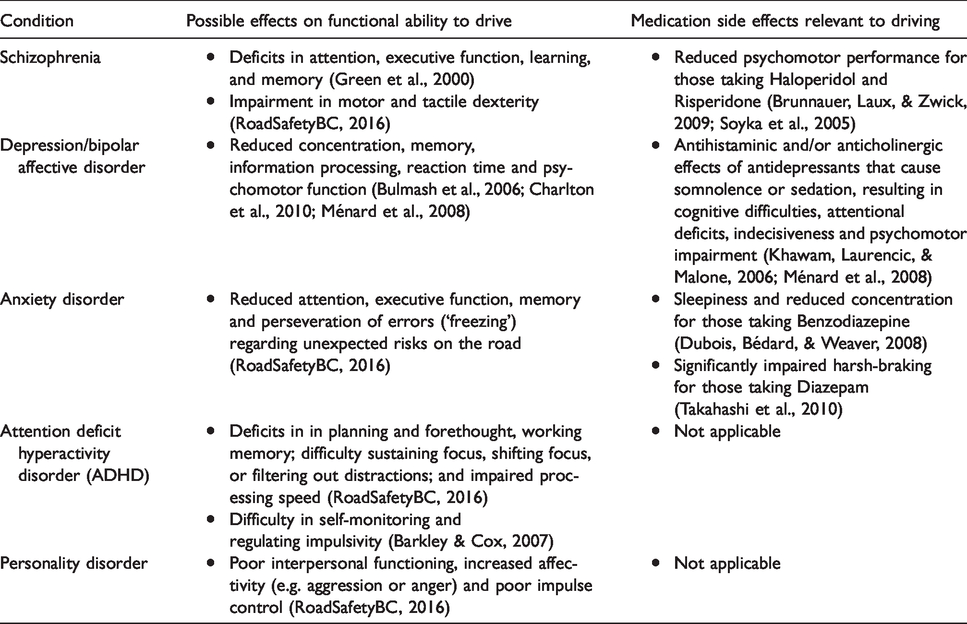
According to the safe driving practice guidelines from different countries, mental illnesses are considered as clinical conditions that would affect one’s fitness-to-drive (Austroads, 2016; RoadSafetyBC, 2016). People with mental illnesses are associated with higher risk of vehicle crashes (Charlton et al., 2010). In particular, drivers with schizophrenia are reported to have a risk of car accidents approximately two times greater than that of age-matched controls (Edlund, Conrad, & Morris, 1989). Their driving capacity is affected by their respective symptoms, including psychomotor impairment (De las Cuevas, Ramallo, & Sanz, 2010), cognitive deficits (Green, Kern, Braff, & Mintz, 2000) and the side effects of medication (Ménard & Korner-Bitensky, 2008) (Table 1). The fluctuating nature of mental illnesses would further complicate their prognosis as well as their fitness-to-drive (Unsworth, 2010).
Impacts of mental illnesses and dedication side effects on driving.
Need for evaluation of drivers with mental illness
Although mental illness likely affects one’s driving capacity, it is estimated that there is a significant portion of drivers with mental illness in community. Rouleau, Mazer, Ménard, and Gautier (2010) and Rowse (2010) have reported that around 30–40% of people with mental illness in Canada and Australia continue to drive. However, as revealed by Rouleau et al. (2010), it is uncertain how often driving assessment was offered to those drivers with mental illness. Other surveys on driver assessment practice have indicated that majority of their clientele are mainly those with physical or aging conditions, such as traumatic brain injury, stroke or mild cognitive impairment, rather than mental illness (Korner-Bitensky, Bitensky, Sofer, Man-Son-Hing, & Gelinas, 2006; Vrkljan, Myers, Crizzle, Blanchard, & Marshall, 2013). Audit reports have also shown that driving and license status of drivers with mental illness is not routinely addressed by clinicians in their case management (Orr & Elworthy, 2008; Yaqub, Ismail, Babiker, & Rao, 2016). Dun, Bull et al. (2015) even explicitly commented that ‘driving is often omitted or ignored during assessment and ongoing work with consumers of mental health services’ (p. 536). This may be due to the low confidence of clinicians in determining client’s fitness-to-drive (Marshall, Demmings, Woolnough, Salim, & Man-Son-Hing, 2012). Inadequate awareness of driving-related legislation or standards; limited resources for the clinicians, clients and families; and insufficient knowledge in driving-related practice are the other challenges that impede the development of driving assessment service for those with mental illness (Curwen & Jebreel, 2012; Dun, Baker, Swan, Vlachou, & Fossey, 2015; Ménard et al., 2012).
Advocacy for driver assessment specific to mental illness and a local example
Until recently, the ‘Drive Safe’ initiatives have emerged in the field of mental health occupational therapy in Australia to improve clinical practice related to safe driving. With the development of relevant policy, practice guidelines and resources, driving assessment for people with mental illness has been advocated and provided by occupational therapists specialised in mental health practice and with recognised training in driving assessment (Dun, Baker et al., 2015; Dun, Bull et al., 2015).
Driving assessment is imbedded in occupational therapy practice. Occupational therapists have conducted study to identify attributes that associated with traffic accidents in Hong Kong. Findings show that impulsivity is associated with risk-taking driving behaviours. Highly impulsive drivers carry out more risk-taking behaviours and are less able to inhibit responses than those with low impulsivity (Cheng & Lee, 2012). Findings also show that driving behaviours are related to how the drivers perceive their vulnerability and causes of road traffic accident (Cheng & Ng, 2012). For those who drive as part of their occupation, they are more prone to drive recklessly and commit traffic offences because of work stress and less sensitive to consequence of risk-taking driving behaviour (Cheng, Ting, Liu, & Ba, 2016). In 2012, the occupational therapy profession in Singapore, the first in Asian countries, was appointed to provide mandatory driving assessment for drivers aged 73 who would like to continue their Taxi Driver’s Vocational Licence for another two years (Sim, 2012). However, driving assessment service specific to people with special need is still scarce in local clinical settings.
In Hong Kong, according to Road Traffic (Driving Licenses) Regulations, Cap 374B (1984), drivers must declare any diseases or conditions that are likely to render them incapable of driving safely and effectively. Medical doctors are usually asked by the Transport Department to comment on the driving capacity of their clients. The Occupational Therapy Department of Castle Peak Hospital has piloted the driver assessment service to clients with mental health in its catchment area since 2015. Four occupational therapists who have extensive experience in psychiatric rehabilitation and completed certified training in driver assessment are currently responsible for service delivery.
Framework of driver assessment was developed to examine the impact of mental conditions on driving capacity (Figure 1) with the following assessment principles that were adopted from the existing safe driving practice guideline (RoadSafetyBC, 2016):
Primary concerns are driving safety and risk to other road users. Functional approach is incorporated for evaluation. Presumed characteristics of particular diagnostic groups are not the solely determining factors on one’s fitness-to-drive. Recommendations on fitness-to-drive are based on the best information gathered during the assessment.
The first part of assessment includes screening assessments on sensorimotor, cognitive and psychosocial functions to identify deficits related to driving. Another core component is functional assessment with the use of simulator. In the simulated road assessment, clients would drive a standardised route with common road situations such as roundabouts, unmarked lanes, different speed limit, etc. Basic driving skills and road hazard handling were evaluated throughout the driving simulation. Mental condition and driving behaviour such as impulsivity or risk-taking are also taken into account when concluding their driving capacity. Most importantly, drivers’ responsibility to report to the Transport Department on their health conditions is educated to clients. Report including test results of the driving assessment and recommendations on driving fitness of clients would be compiled to the case psychiatrist.
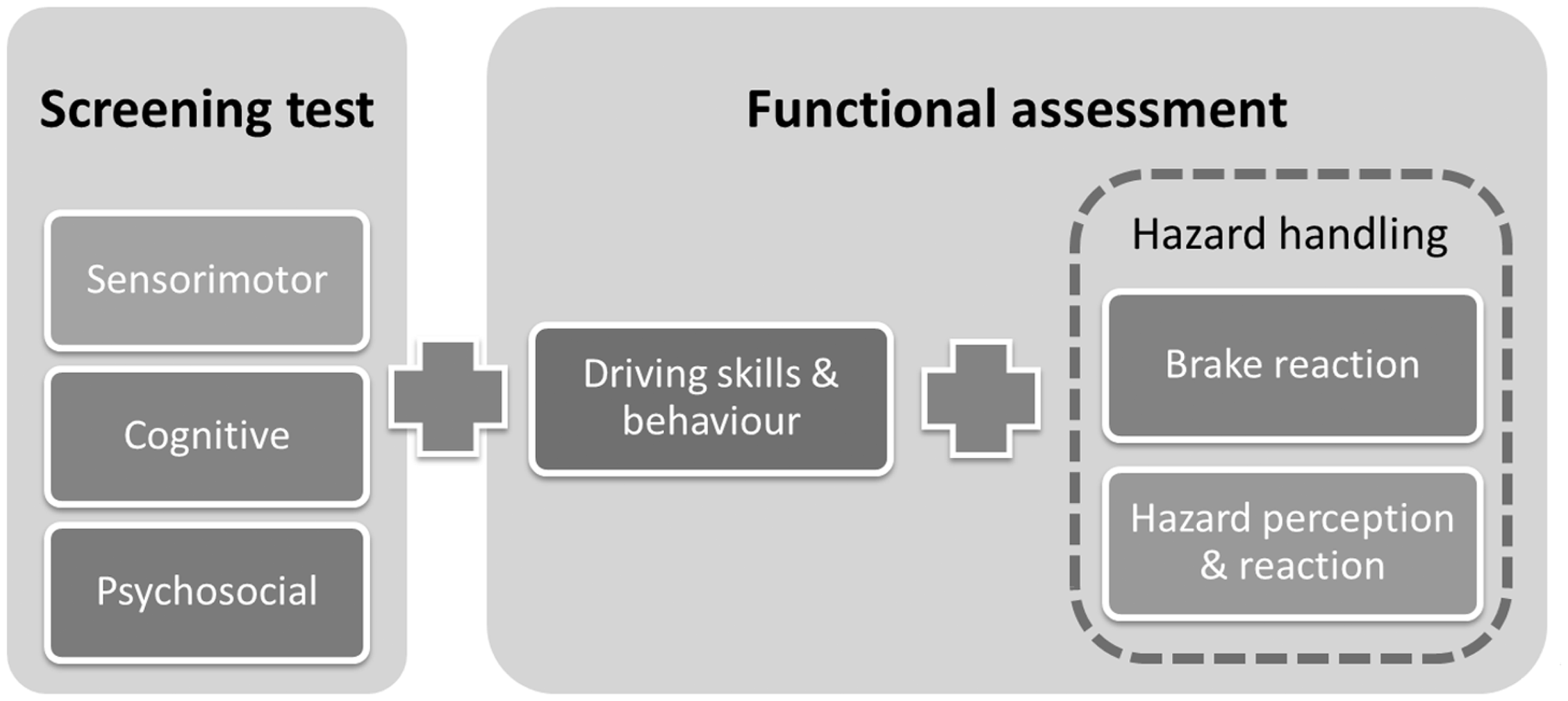
Framework of driver assessment for people with mental illness.
There are several service characteristics that could further illustrate the driving issues and service need of people with mental illness. Concerning the driving status, around 94% of them were holding a valid driving license and more than half of them were commercial vehicle drivers at the time of assessment (Figure 2). They were either driving or on sick-leave but planned to resume driving afterwards, indicating an imminent need to assess their fitness-to-drive. When it comes to client’s characteristics, the major diagnosis was mood disorder, followed by Schizophrenia. There were around 42% of clients deemed to have inadequate driving capacity, in which the presence of significant cognitive deficits was far more prevalent than physical impairments. The most prevalent driving skill deficit identified during the simulated road assessment was hazard handling, followed by observation, planning and judgment, and vehicle positioning, while the deficits in physical control of vehicle and reaction time were relatively less common. These certainly show the importance to have a comprehensive assessment on various domains of clients’ functional status, driving skills and behaviours. Lastly, our recommendations on clients’ driving capacity were found consistent with that of their medical reports submitted by the psychiatrists to the Transport Department. All the above illustration elucidates some particular features of driver assessment for people with mental illness, but it is also limited to the experience of a single psychiatric hospital only and may not fully represent the entire population in Hong Kong. Indeed, such driver assessment service should be expanded locally to benefit more clients, and further studies should be conducted to advance our understanding in driving-related practice.
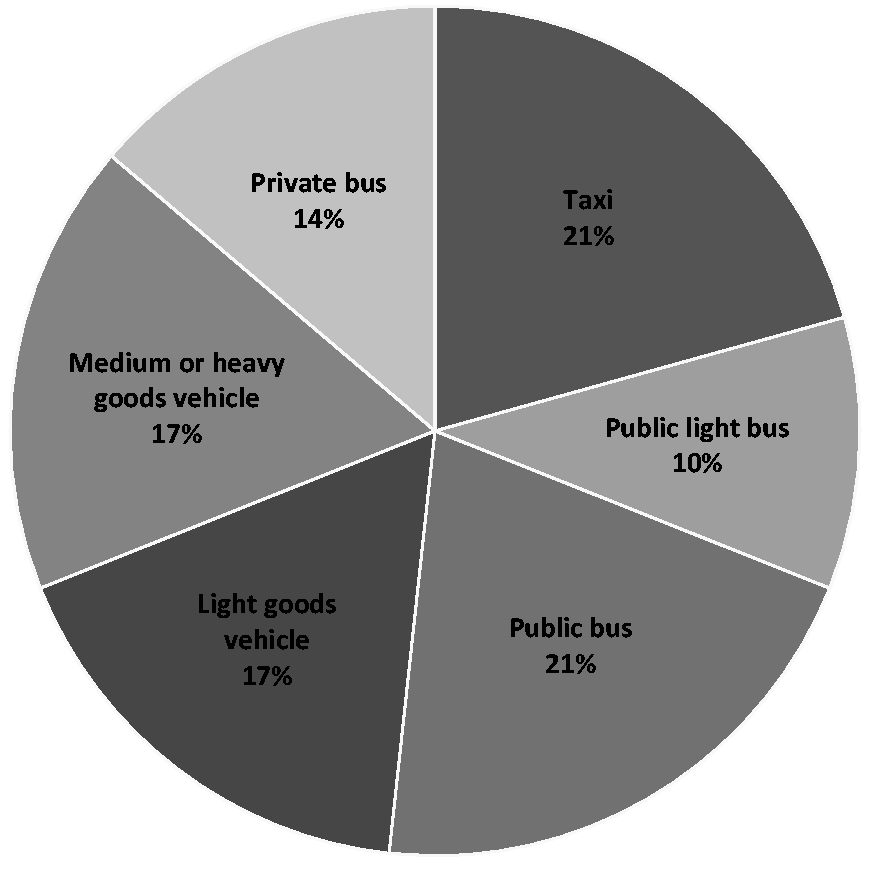
Distribution of job posts among those participants who were commercial vehicle drivers.
Challenges ahead
De las Cuevas and Sanz (2008) studied the driving capacity of 208 stable outpatients with mental illness, of which 80% scored below the required standard to obtain a driving license. However, none of the subjects who actually held a driving license and drove daily had reported their mental conditions to relevant traffic authority. These ‘hidden’ at-risk drivers undoubtedly pose a threat to other road users. Such under-reporting was also observed in our service as around 80% of clients did not report to the Transport Department regarding their health status. The majority of them explained that they were not aware of the responsibility to declare. Another possible reason would be the lack of mandatory driver evaluation and reporting system to the authority after the onset of mental illness. However, given the concerns of breaching confidentiality and resulting into legal conviction, it would be a dilemma for a medical professional to take initiative to report to Transport Department on risky drivers for the sake of public safety without the consent from them. Also, the consequence of reporting might contribute to the under-reporting. Around 60% of our clients were commercial vehicle drivers and their employment or even livelihood would be seriously affected in case of the suspension of their driving licenses. Worries about the license removal after reporting would likely reduce their motivation to declare their health status or to sit for a driving assessment. Lastly, the fact that some people with mental illness are likely to have inadequate insight on their mental illnesses would further prevent them from taking initiative to declare. Therefore, education on the legal responsibility to report is extremely important and should be the key focus of a driver assessment. The possibility of unemployment arising from driving license removal should also be addressed. Work resettlement service should be considered as a follow-up for exploring other employment opportunities and facilitating changes in their worker role.
Another challenge concerns with the choice of assessment tools for determining driving fitness. In fact, driving assessment practices vary greatly and there is no universally accepted guidance on what exactly constitutes a ‘suitable’ or the ‘best’ assessment (Korner-Bitensky et al., 2006; Vrkljan et al., 2013). There exist different types of tests to measure driving capacity across diagnostic groups, including standardised batteries (Unsworth et al., 2012) or domain-specific assessments (Kay, Bundy, & Clemson, 2009; Myers, Ball, Kalina, Roth, & Goode, 2000). Also, the context of assessment might utilise on-road situation (Kay, Bundy, Clemson, & Jolly, 2008), off-road situation (Unsworth, Lovell, Terrington, & Thomas, 2005) or a simulated road environment (Bédard, Parkkari, Weaver, Riendeau, & Dahlquist, 2010). There are also assessments for specific drivers’ attributes or driving behaviour, namely impulsivity or risk taking (Cheng, Ng, & Lee, 2012; Cheng et al., 2016).
Among these, simulated driving test seems to be an emerging evaluation method being applied to different conditions such as Alzheimer’s disease (Frittelli et al., 2009), traumatic brain injury (Lew et al., 2005), stroke (Akinwuntan, Wachtel, & Rosen, 2012), attention deficit hyperactivity disorder and autism spectrum disorder (Classen, Monahan, & Wang, 2013) and mental illness (Brunnauer et al., 2009). There are a number of advantages of using simulator to evaluate driving capacity. Firstly, it provides situational assessment to assess clients’ ability to handle traffic under a safe and controlled environment. It seems to be particularly suitable for assessing the driving fitness of people with mental illness, in which driving-related cognitive deficits are quite prevalent among them. Another longitudinal study on elderly at-risk drivers (Lee & Lee, 2005) and a comparison study using on-road tests (Lee, Cameron, & Lee, 2003) have demonstrated that a simulator seems to be a reliable, valid and practical tool for identifying at-risk drivers. Secondly, real-life traffic and specific road conditions can be simulated, and this is especially useful to assess clients’ behaviour in hazardous situations (Underwood, Crundall, & Chapman, 2011) which cannot be controlled during on-road evaluation. Thirdly, instant feedback could be provided to clients, allowing them to ‘visualise’ their driving ability and improving insight into their driving capacity.
Conclusion
Having mental illness is not necessarily equal to absolute inability to drive. Instead, fitness-to-drive of individuals with mental illness should be examined carefully before they drive. A specialised driver assessment that addresses the unique characteristics of mental illnesses is certainly needed. However, such service is scarce locally and it requires specially trained professionals. Occupational therapists specialised in both mental health practice and driver assessment does play a vital role in this emerging area. Such driving assessment service should definitely be expanded in the psychiatric field to address the needs of clients, and more studies are recommended to further enhance driving-related practice in Hong Kong.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.