
Abstract
Background
Occupational therapists are optimally positioned to screen, assess, consult, and support driving among medically at-risk populations (College of Occupational Therapists of Ontario [COTO], 2021; World Federation of Occupational Therapy, 2019). In fact, recent changes to provincial legislation recognize the importance and relevance of occupational therapy in addressing driving. In 2018, the government in the Canadian province of Ontario amended the Highway Traffic Act to grant occupational therapists the discretionary authority to report any person who has a condition or impairment that may make it unsafe to operate a motor vehicle to the Ministry of Transportation (Highway Traffic Act, 1990, subsection 203[2]). Given this increased responsibility for Ontario occupational therapists, there is an opportunity to understand the current practices of occupational therapists and how equipped they feel to fulfill this recently expanded role for driving practice.
A body of research has examined the role and practice of occupational therapists in addressing driving across different practice contexts (Cammarata et al., 2017; Korner-Bitensky et al., 2010; Petzold et al., 2010; Unsworth, 2011; Unsworth et al., 2015; Vrkljan et al., 2013, 2015). For example, prior to the legislative changes, Korner-Bitensky et al. (2010) conducted a Canada-wide survey of occupational therapists (n = 147) to identify the capacity-building needs for different “knowledge areas” related to older driver screening/assessment, 1 intervention, and advanced practice. This study surveyed therapists working in community settings (n = 65), rehabilitation centres (n = 34), acute care hospitals (n = 34) and driving assessment centres (n = 6) to explore which driving-related practices they engaged in, their self-reported competence for knowledge areas relevant to driving, and the perceived importance and likelihood of undertaking driving-related continuing education (Korner-Bitensky et al., 2010). Results from this survey suggested that while therapists report competence for knowledge areas related to driver screening, few had experience providing older driver retraining or discussing and supporting clients in driver cessation and alternative community mobility. Moreover, 60% of the therapists surveyed did not feel competent regarding legal issues and liabilities related to driver screening, assessment, and retraining (Korner-Bitensky et al., 2010). These findings are similar to those reported in a recent study undertaken shortly after the introduction of discretionary reporting 2 for Ontario occupational therapists. From their interviews, Sangrar et al. (2018) found that therapists remain uncertain of legislation and licensing policies and procedures for medically at-risk drivers and their role in medical fitness to drive. Occupational therapists also expressed concern that addressing driving can jeopardize the therapeutic relationship and even fear clients may seek legal action against the therapist for reporting a driver to the ministry (Sangrar et al., 2018).
Occupational therapists also reported professional tensions within interdisciplinary teams when addressing driving (Sangrar et al., 2018). Therapists shared the challenges experienced when navigating differences in opinion for fitness to drive with physicians. They also described one-sided approaches in which a physician deferred the decision solely to the occupational therapist to “clear the [client] to drive” (Sangrar et al., 2018, p. 278). Furthermore, occupational therapists expressed concern regarding physicians using occupational therapy assessment results outside of their intended purpose to justify a report to licensing authorities. For example, a client may have consented to a cognitive assessment without the knowledge that the physician could use the results to initiate a report to the ministry (Sangrar et al., 2018). These findings underscore the practical, ethical, and professional challenges for addressing driving and highlight the need for more research to support competency development of occupational therapists in this area.
Given the breadth of settings in which occupational therapists are employed, it is a priority to understand driving within specific practice areas and contexts (Sangrar et al., 2018). Acute care hospitals pose a unique challenge for addressing driving. First, acute care settings provide treatment for the most medically complex clients with medical conditions associated with increased risk of motor vehicle collision, such as stroke, traumatic brain injury, diabetes, and dementia (Canadian Council of Motor Transport Administrators [CMTA], 2020). Second, acute care settings are fast-paced, stressful work environments. With the rising costs of inpatient care, acute care hospitals have increasing pressures to discharge clients as quickly as possible (Britton et al., 2015). Due to these practice demands, occupational therapists feel pressure to focus on interventions that directly relate to discharge, such that therapy is typically restricted to self-care activities, with little attention to participation in other domains (Britton et al., 2015, p. 16, Murray et al., 2021). Driving is an example of an occupation that therapists may not have time to address in acute care, yet lengthy waitlists to access community occupational therapists render acute care a possible “last stop” to address driving for many clients. If risks are identified in acute care regarding driving ability, this may prompt the team to broach driving with the client to ensure appropriate next steps. Thus, the barriers to addressing driving in general may be amplified in the medically complex and discharge-focused acute care setting.
In summary, despite new legislation granting increased driver reporting responsibilities to occupational therapists, addressing driving in occupational therapy practice can be met with uncertainty and challenges, which may be further complicated in acute care settings. To support the professional development of occupational therapists and client-centred care in this evolving area of practice, more research is needed to understand the role, current practices, and competencies of acute care occupational therapists regarding driving. This study sets the stage for such research by examining the practice needs of acute care occupational therapists in the Canadian province of Ontario.
Building upon the work of Korner-Bitensky et al. (2010) and Sangrar et al. (2018), the objectives of the present study were to identify (1) what knowledge areas are relevant to driving practice specifically in acute care settings as rated by occupational therapists, (2) self-reported competence for knowledge areas among acute care occupational therapists, (3) knowledge areas encountered the most and least in practice, and (4) which resources acute care occupational therapists access to gain competency for addressing driving. The term “knowledge area” utilized by Korner-Bitensky et al. (2010) is defined in the current study as the specific skills and knowledge related to driving within clinical practice (e.g., “screening for physical impairments” and “information on driving cessation and its impact”). Competence is operationalized as the self-reported level of knowledge, judgment or skill related to addressing driving in the acute care setting (i.e., the ability to perform the skill and/or possessing specific knowledge for each driving-related knowledge area). In this conceptualization, knowledge is a component of competence, such that occupational therapists must gain knowledge to develop competency for driving-related knowledge areas.
Methods
The present study employed a cross-sectional survey design to examine driving practice within acute care occupational therapy. Western University's Health Science Research Ethics Board, in London, Ontario approved this study (Project ID: 120353). Manuscript reporting follows recommendations per the Checklist for Reporting Of Survey Studies (CROSS; Sharma et al., 2021), presented in Appendix A.
Participants
Occupational therapists working in Ontario acute care hospitals were eligible to participate in the study if they practice in an inpatient acute care unit with adults 18 years of age or older. Occupational therapists who were not currently practicing (e.g., parental, medical, or education leave) but have practiced in acute care in the last 2 years were also eligible to participate. Occupational therapists not practicing in acute care, or with populations younger than 18 years of age were excluded. An advertisement was posted on two professional association websites, the Ontario Society for Occupational Therapists (OSOT) and Canadian Association of Occupational Therapists, in addition to being shared on their respective emailing lists. Occupational therapists were also invited via social media platforms (Facebook, Twitter), the i-Mobile Driving Research Lab website, and professional networks via pre-existing email lists (OSOT Hospital Sector Community of Practice and the Clinical Preceptor Network at Western University). Online survey links were provided within the advertisements/emails.
Additionally, occupational therapists were invited via telephone. To reduce risk of bias, a randomized call list was created from the public register of occupational therapists available on the College of Occupational Therapists of Ontario (COTO) website. The search filters “acute care,” “adults 18 to 65 plus” and “general hospital” were utilized to develop the list. Occupational therapists were contacted via the workplace telephone number listed on the public register. Occupational therapists who expressed consent to participate in the study over the phone were provided with a follow-up email including the link to participate in the study.
Survey Development
An online survey was utilized as it is a cost-efficient strategy to reach as many participants as possible within the data collection period (Dillman et al., 2014).
The survey was adapted from Korner-Bitensky et al. (2010) utilizing the tailored design method for online surveys (Dillman et al., 2014). The original survey in Korner-Bitensky et al. (2010), was also developed using the tailored-design method and was validated by five experts, including researchers, occupational therapists, and driver rehabilitation specialists, and was further piloted with an additional four occupational therapists.
To adapt the survey to the acute care setting and to reflect the current responsibilities for fitness to drive in Ontario, additional knowledge areas were added, as well as new questions related to the existing knowledge areas. Specifically, in addition to new knowledge areas, the survey in Korner-Bitensky et al. (2010) was expanded to identify the knowledge areas encountered the most and least in practice, how relevant each knowledge area is to acute care occupational therapy, and how occupational therapists gain competency in driving-related knowledge areas. Development of 10 new knowledge areas was achieved via three methods, (1) reflexivity on the first author's practice as an acute care occupational therapist with more than 10 years of clinical experience, (2) a literature search of relevant studies pertaining to driving and occupational therapy, and acute care occupational therapy, and (3) through consultation with the fourth author who is an occupational therapist with a program of research focused on driving and community mobility across the life span.
For preliminary validation, the survey was shared with a panel of acute care occupational therapists to review the survey for clarity, completeness, and relevancy. To represent a wide range of possible respondents, a preview of the survey was sent to a convenience sample of three occupational therapists with different practice experience and employment statuses. The survey was shared with a part-time novice occupational therapist with less than 2 years of practice, a full-time occupational therapist with 9 years of experience in acute care, and a full-time professional practice leader in occupational therapy at a regional hospital, who has practiced for 15 years. The panel provided feedback to clarify some knowledge areas, made suggestions for readability, and recommendations for areas of repetition that could be removed. The revised survey was shared again with the same panel of occupational therapists who agreed that the revisions addressed the suggested changes, and the content reflected the area of practice.
Survey
The survey was comprised of six sections and is presented in Appendix B. In Section 1, participants completed eligibility screening and provided demographic information including the number of years of practice, number of years of practice specifically in acute care, the area of practice within acute care (i.e., medicine, surgery, neurology, etc.), and employment status (full-time, part-time, or casual) utilizing multiple choice and open text fields.
Sections 2, 3 and 4 included 29 knowledge areas in the practice domains of screening and assessment (8 items), intervention (8 items), and advanced practice (13 items). Sections 2, 3 and 4 presented the respective domains followed by the same two Likert-type questions. The questions asked respondents to (1) rate the relevance of each knowledge area to the occupational therapist role in acute care, and (2) rate their self-reported competence for each knowledge area. Section 5 presented the knowledge areas organized by the domains of screening and assessment, intervention, and advanced practice and asked participants to identify the three most encountered and three least encountered knowledge areas within each domain respectively. Section 6 asked the respondents to reflect on the previously presented knowledge areas and indicate which resources they have accessed (if any) to gain competence in this area. Section 6 included multiple choice and open-text fields. At the end of the survey, respondents were provided with an optional open-text field to enter any further comments to the researchers.
Data Collection
The online survey platform QualtricsXM was utilized to administer the survey which has both browser and mobile optimized versions for survey completion and allows participants to pause the survey and resume later to maximize response rates (Dillman et al., 2014). Occupational therapists who expressed interest in participating were directed to the survey link including the letter of information and consent form. The survey required a response for the screening eligibility questions, but all other survey questions could be skipped. Any prospective participant that did not meet the eligibility criteria was not presented the survey and was thanked for their interest in the study. Data was collected for a period of 3.5 months. All responses to the survey were anonymous and confidential and stored in a secured server network, and via the QualtricsXM platform.
Data Analysis
SPSS was used to analyze the survey results. As the study was exploratory in nature, all survey responses, including incomplete surveys, were included in the analysis to capture as much data as possible. Descriptive statistics were calculated for occupational therapist demographic variables. Means and standard deviations (SD) were calculated for number of years of practice (in total) and number of years of practice specifically in acute care. Frequencies and percentages were calculated for area of practice within acute care. Data from each knowledge area in terms of relevance, how often employed, and self-reported competence were analyzed to report the frequency and percentages of each response. Frequency and percentages were also calculated to report the resources therapists have accessed to gain competency in the knowledge areas. All open-text data were organized into groupings of similar responses and percentages were calculated to express the proportion of relevant respondents for each (Bengtsson, 2016).
Findings
Participants
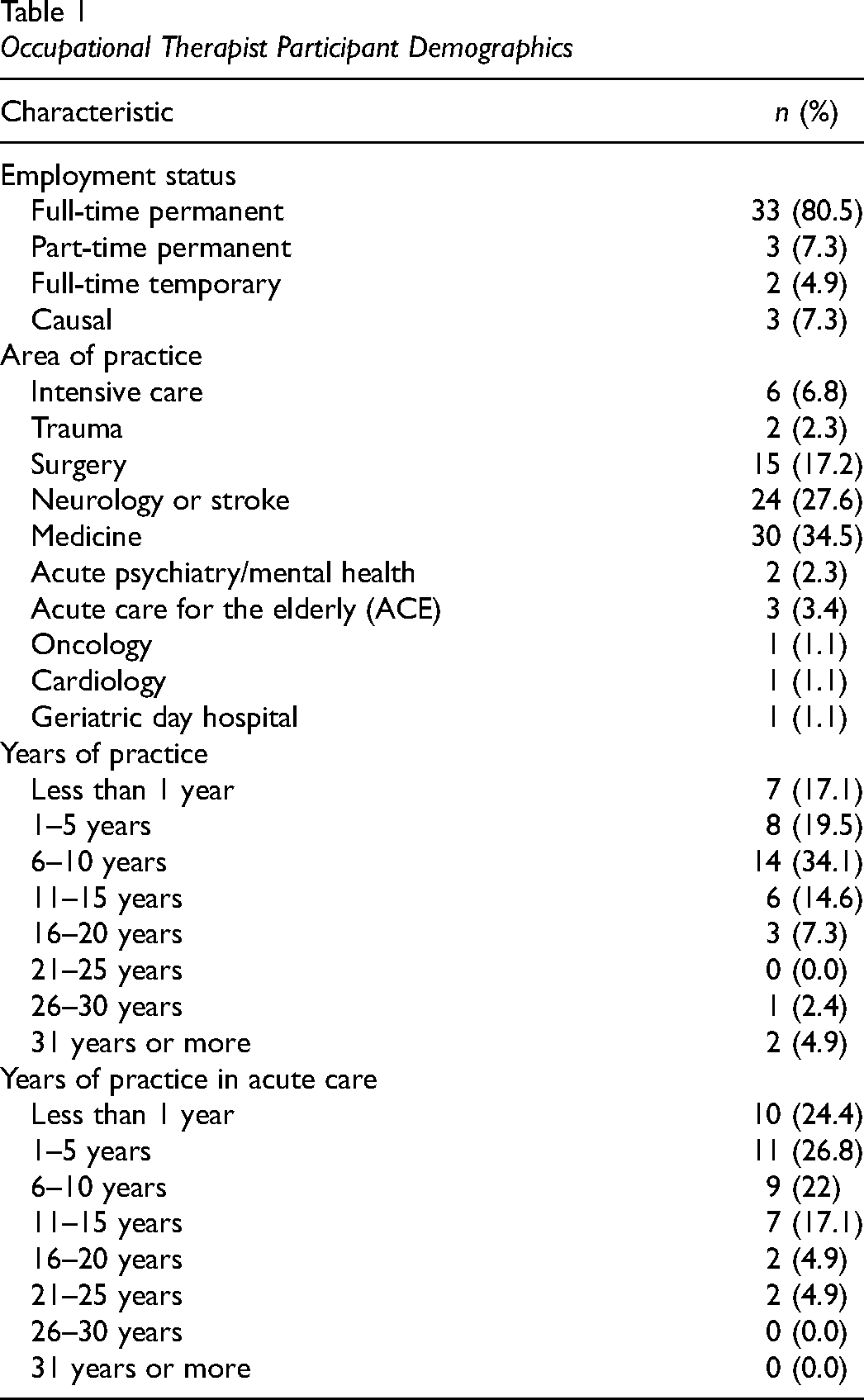
A total of 59 prospective respondents accessed the survey, 9 (15%) were ineligible, 9 (15%) were eligible but did not complete the survey and 41 (70%) were eligible and completed the survey. As the survey was administered via an anonymous link, reasons why eligible prospective participants did not complete the survey are unknown. Of the 41 study participants, 39 (95%) completed the survey in its entirety, and two participant surveys were incomplete (18% and 20% complete, respectively). A search of the public register of all occupational therapists in Ontario using filters to identify eligible therapists revealed an estimated population size of N = 415. As such, the sample size corresponds to an estimated 10% (41/415) of the population. Respondents ranged from 1 to 38 years since graduation from occupational therapy school (M = 9.7, SD = 8.7). Additional participant demographics are presented in Table 1.
Occupational Therapist Participant Demographics
Relevance, Competence, and Frequency
Across knowledge areas, occupational therapists’ ratings of relevance regarding the knowledge areas identified were higher than their own ratings of competence for such areas. The reported relevance and competence for each driving-related knowledge area is presented in Tables 2 and 3, respectively. Each table presents the knowledge areas chronologically by the number of “very” or “somewhat” responses from most to least. Overall, ratings of relevance exceeded the competency ratings an average of 29.3%. However, in the top nine knowledge areas of greatest discrepancy, ratings of relevance exceeded self-ratings of competence an average of 45.3%. Figure 1 presents nine knowledge areas with the greatest discrepancies between ratings of relevance and self-competence.
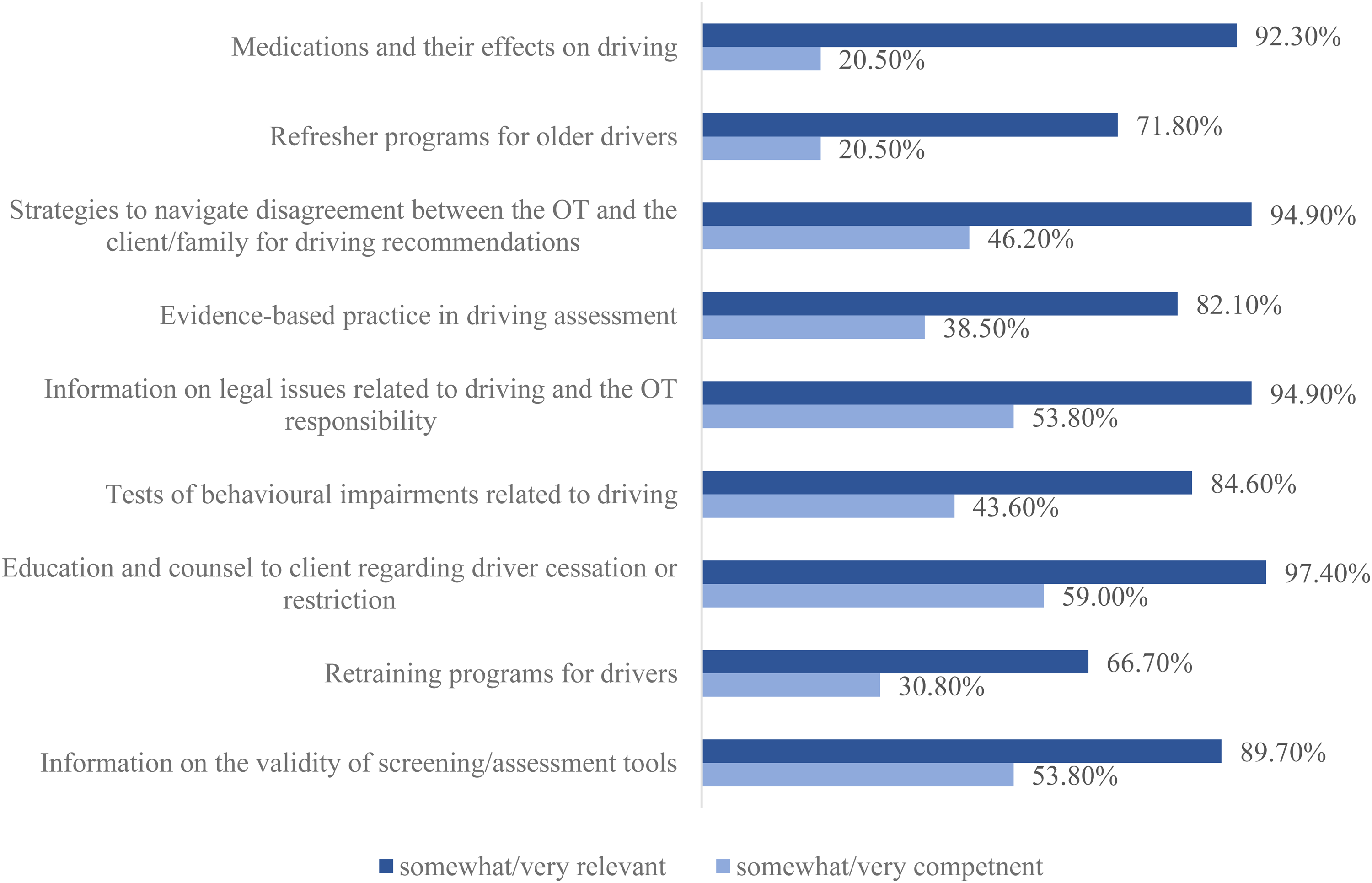
Knowledge areas with the largest differences between self-reported relevance and competence.
Occupational Therapist Reported Relevancy for Fitness to Drive Knowledge Areas
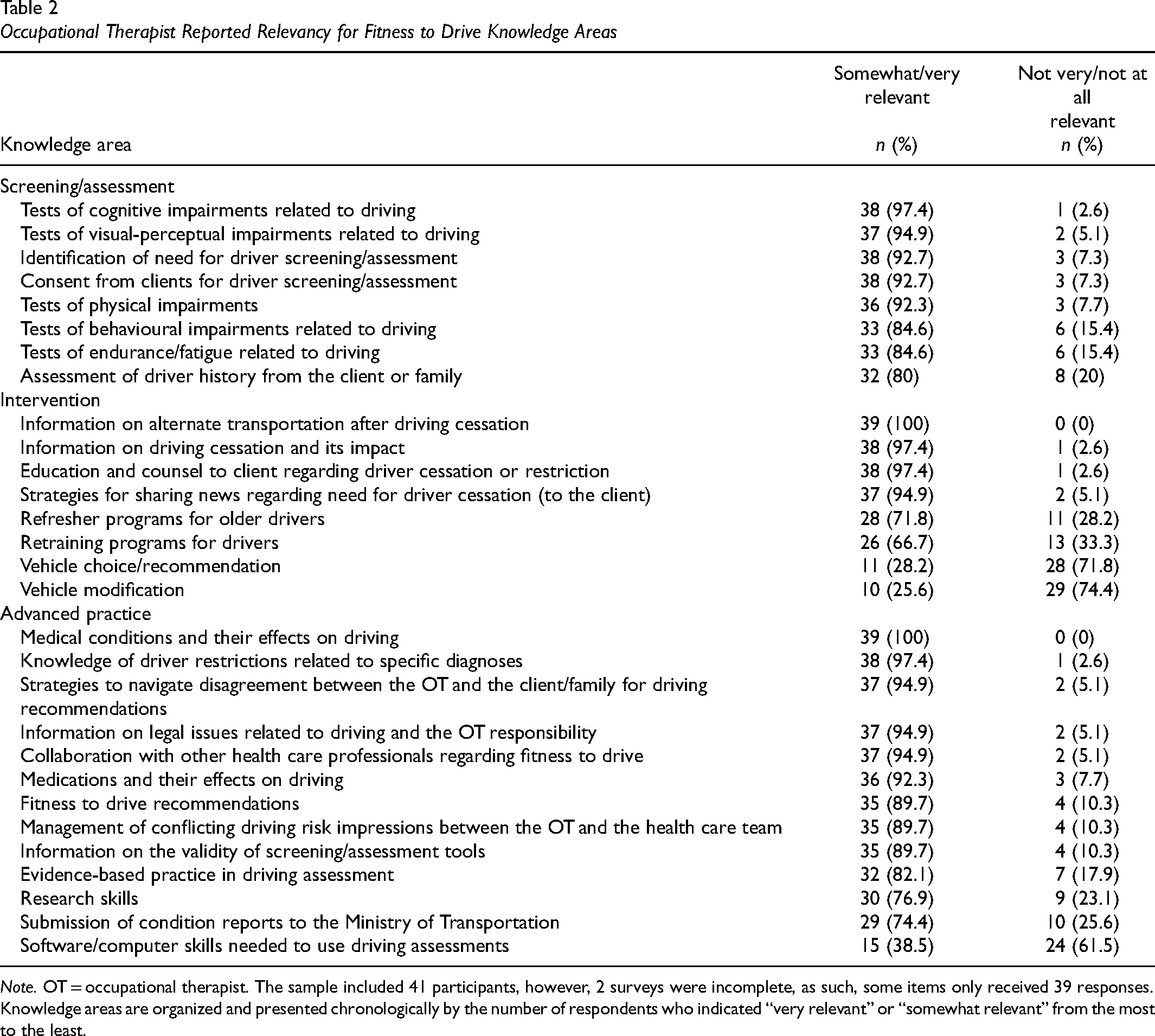
Note. OT = occupational therapist. The sample included 41 participants, however, 2 surveys were incomplete, as such, some items only received 39 responses. Knowledge areas are organized and presented chronologically by the number of respondents who indicated “very relevant” or “somewhat relevant” from the most to the least.
Occupational Therapist Self-Reported Competency for Fitness to Drive Knowledge Areas
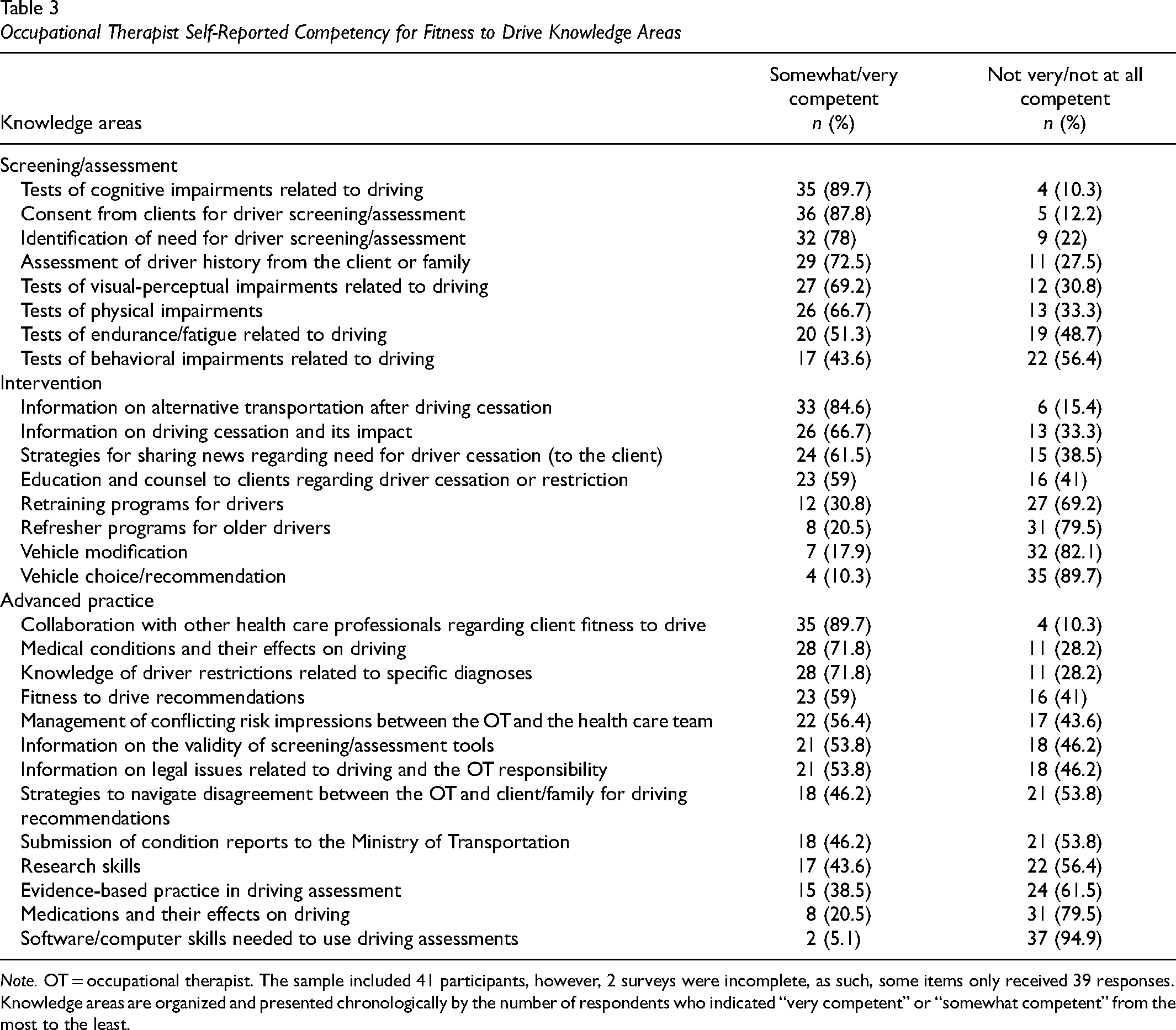
Note. OT = occupational therapist. The sample included 41 participants, however, 2 surveys were incomplete, as such, some items only received 39 responses. Knowledge areas are organized and presented chronologically by the number of respondents who indicated “very competent” or “somewhat competent” from the most to the least.
Information about alternative transportation after driving cessation, and cognitive clinical testing were knowledge areas most often used in their clinical practice, with nearly a third of respondents rating these areas in the top three. In contrast, advice regarding vehicle choice or vehicle modifications were among the least often offered to clients in acute care settings. Table 4 presents the most and least encountered knowledge areas in practice across all domains.
The Most and Least Frequently Employed Knowledge Areas in Practice
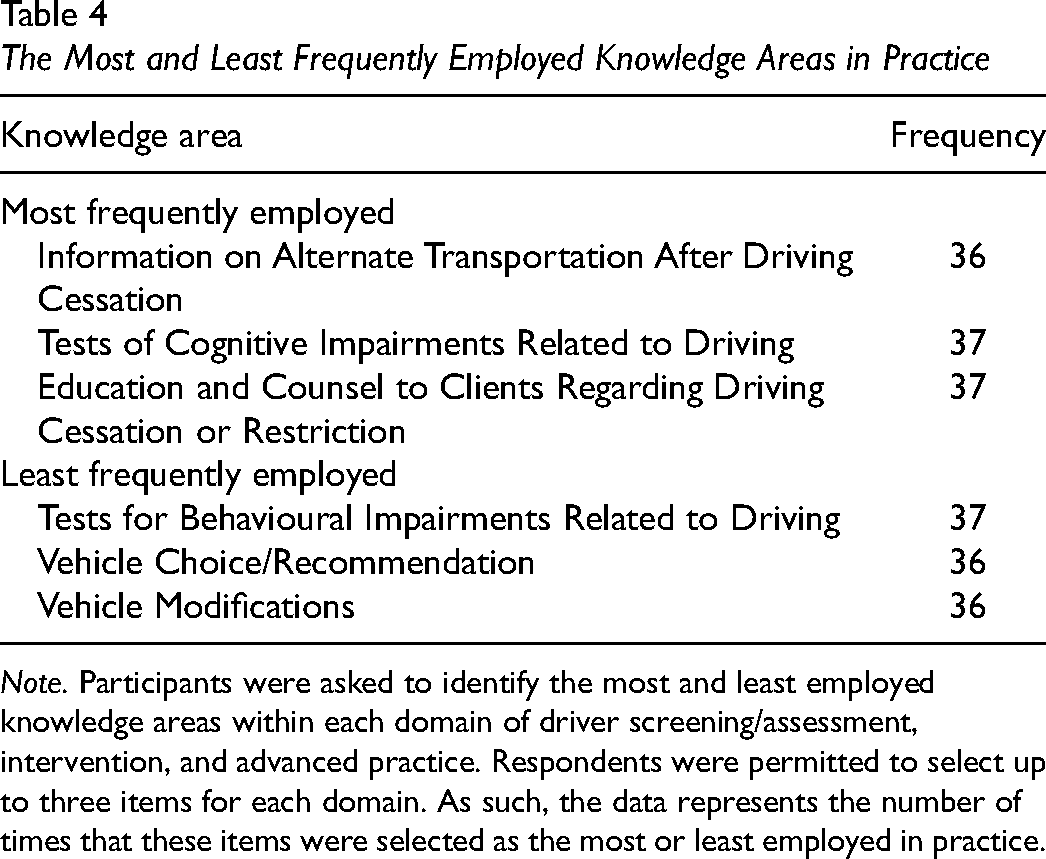
Note. Participants were asked to identify the most and least employed knowledge areas within each domain of driver screening/assessment, intervention, and advanced practice. Respondents were permitted to select up to three items for each domain. As such, the data represents the number of times that these items were selected as the most or least employed in practice.
Resources Accessed to Gain Competency
Occupational Therapy Practice guidelines, toolkits, assessment batteries and similar practice resources, and scientific literature are the among the most frequently accessed resources to gain competence in driving-related practice knowledge. The percentage of respondents who accessed each resource is presented in Figure 2. Of the occupational therapists who reported using practice resources from other professions (n = 12; 30.8%), the guidelines accessed were for physicians (n = 11) and optometrists (n = 1).
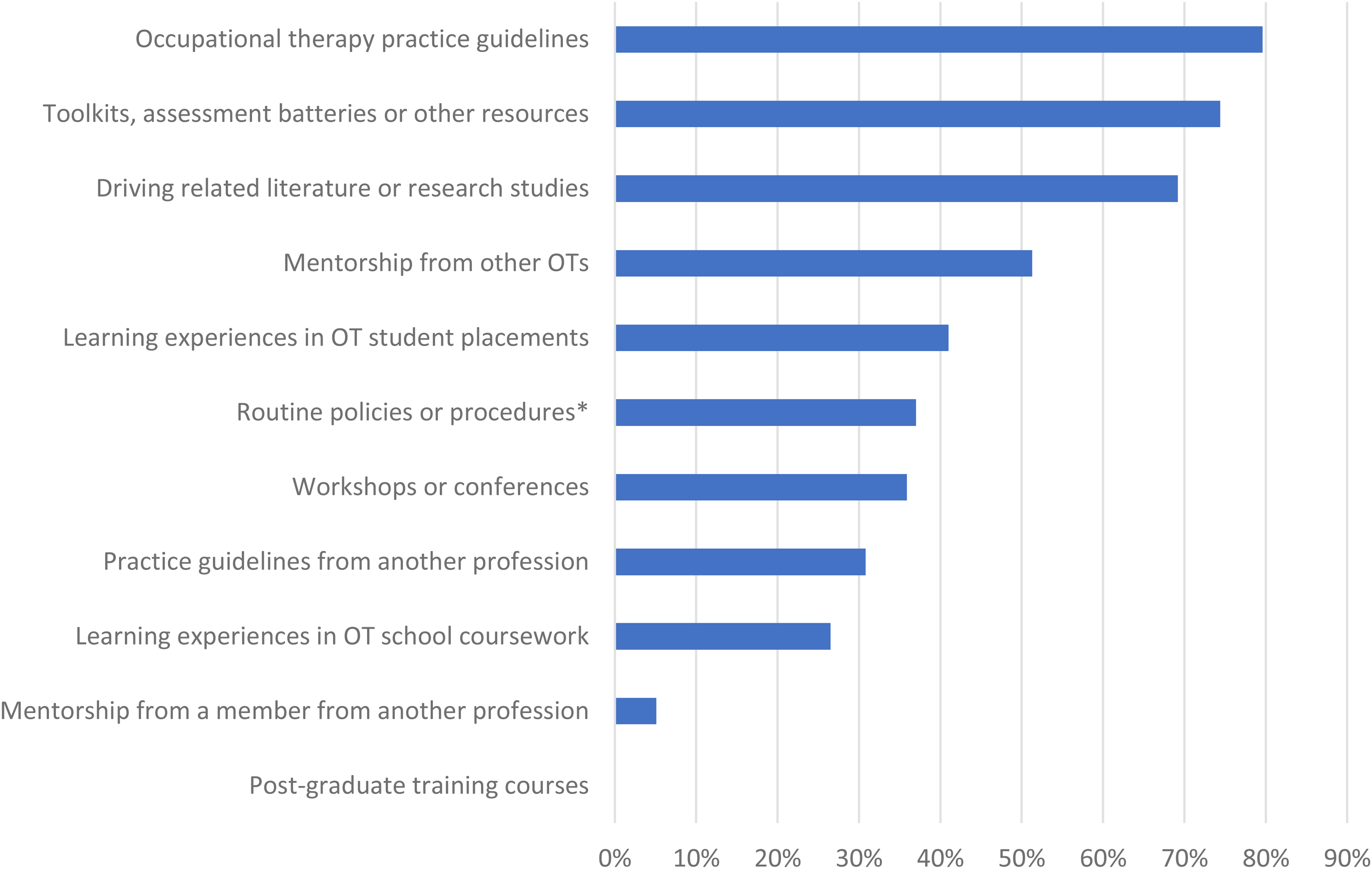
Resources accessed by occupational therapists to gain competency in fitness to drive practice.
Open-Text Responses
A total of 8 (19.5%) respondents provided optional feedback at the end of the questionnaire. Although the open-text responses are from a small proportion of participants, there are some responses that discuss the challenges of addressing driving in acute care settings. For example, some respondents (n = 5; 62.5%) indicated that driving is either not addressed, or is not a priority due to time constraints in this setting, “driving is not the physician's priority to get the [client] home” (Participant [P]15)). Another respondent also shared, “there is not enough time to complete assessments/identify risks/needs before a [client] is discharged the majority of the time” (P2). Other respondents (n = 3; 37.5%) discussed the medical acuity of clients as a barrier to addressing fitness to drive in hospital, for example, “[clients] are “sicker than ever” (P11), at “their worst moments” (P4), and are “too ill to determine their fitness to drive” (P19). Most respondents in this group (n = 6; 75%) also highlighted the importance of the physician's role in driving, and three (37.5%) participants reported they defer to the physician to address driving and notify the ministry of transportation, “If there is a concern, it falls to the most responsible physician to send the information to the Ministry” (P6) and “we leave this responsibility to the physicians” (P19).
Despite the concerns raised regarding the role of occupational therapy and driving practice in acute care, half of the participants who provided responses to the open-text question (n = 4; 50%) discussed the importance of ongoing education, “I am eager to learn and advance my knowledge and practice with respect to driving” (P34). Another participant reported participating in a “working group and developed an algorithm to help inform [occupational therapists] in their clinical reasoning [regarding] reporting medically at risk drivers” (P21).
Discussion
The goal of the present study was to describe the practice of driving for Ontario occupational therapists working in acute care. The results suggest that despite the notoriously fast-paced, discharge-focused setting of acute care occupational therapists report driving is important for acute care practice. Specifically, 20 out of 29 knowledge areas were rated as very relevant or somewhat relevant by ≥80% of respondents. Knowledge areas related to driver screening/assessment (specifically screening) had higher ratings of relevance compared to intervention or advanced practice. Occupational therapists also report spending the most time providing information on alternate transportation, completing screening tests, and providing education and counsel to clients regarding driving cessation and restriction.
Similar to ratings of relevance, occupational therapists reported higher competence for knowledge areas related to driver screening when compared to providing interventions and other areas more reflective of advanced practice (e.g., vehicle modifications). However, across all domains, only in 6 (21%) of the examined knowledge areas did >25% of respondents indicate perceiving themselves as very competent. Overall, occupational therapists consistently rated the relevance for driving-related knowledge areas more highly than their own ratings of competence in such areas. This mismatch between perceptions of relevance and competence signals a gap between desired competence and current competence when it comes to addressing driving in this setting. Some therapists acknowledged they should be addressing driving-related knowledge areas in their practice yet did not perceive themselves as competent to address these areas.
There were two knowledge areas that were perceived as highly relevant by respondents yet were not similarly rated for competence. Among 37 (94.9%) respondents, the knowledge area “strategies to navigate disagreement between the occupational therapist and the client/family for driving recommendations” was rated as very relevant or somewhat relevant. However, only 18 (46.2%) respondents felt very competent or somewhat competent to address this area. Similarly, 37 (94.9%) respondents indicated that the “information on legal issues related to driving and the occupational therapist responsibility” is very relevant or somewhat relevant, but only 21 (53.8%) report feeling very competent or somewhat competent. These findings are similar to those reported in prior research conducted both before and after the legislative changes for reporting medically at-risk drivers in Ontario. Previous studies found that occupational therapists report considerable stress and challenges with addressing driving in their clinical practice and that more training and education regarding the legal implications with respect to their role and responsibilities is warranted (Korner-Bitensky et al., 2010; Sangrar et al., 2018).
When the ratings of relevance and competence are considered together, the knowledge areas occupational therapists reported are most relevant and feel most competent to address in acute care were as follows: driver screening especially for cognitive impairments, being aware of specific diagnoses/conditions and implications for fitness to drive, and addressing driver cessation with clients, including providing options for alternate transportation. These findings are consistent with a “generalist” tier of expertise in the field of driving and community mobility. In this tier, occupational therapists are described as possessing the skill and knowledge to complete driver screening and providing information to support community mobility (Korner-Bitensky et al., 2007).
As found in the survey conducted by Korner-Bitensky et al. (2010), there is little focus on driver retraining or refresher programs within occupational therapy practice, which also appears to be the case in acute care. Interestingly, many therapists (n = 28; 71.7%) reported that referrals to driver refresher programs are relevant (somewhat or very) to acute care occupational therapy, yet this intervention is among the least often employed in practice.
When it comes to acute care and occupational therapy practice, literature describing the discharge planning focus in acute care may provide an explanation for the limited attention to driver intervention. Within acute care settings, only the highest priority occupational therapy assessments and interventions are completed, usually with the view of “safe” discharge (Britton et al., 2015, 2016). Thus, driving may only become a priority when it is a safety issue, such as when the team expresses concern a client can no longer drive. Addressing driving in acute care, according to respondents in this study can, but does not always involve, the occupational therapist undertaking screening of the individual in question as well as providing counselling for driving cessation and alternatives for transportation. However, interventions to maintain driving status are not usually addressed due to complexities of care in this setting. The priority in acute care may be addressing current risks for driving, rather than preventative actions to ameliorate future risk, such as referring to driver refresher programs. In this way, the focus of driving in acute care is consistent with the overall goal for “safe discharge,” such that occupational therapists are more likely to screen for specific deficits that can affect driving rather than providing interventions that address such deficits, which might support continued driving.
In acute care settings specifically, occupational therapists must balance competing priorities. Therapists must consider intersecting threats to client and public safety together with the potential negative consequences to client community mobility if driver status is jeopardized. Given the pervasiveness of “car culture,” and the ongoing prioritization of car travel over other transport alternatives, (Mattioli et al., 2020) clients not only risk restrictions to community mobility if their license is suspended following driver screening, but also threats to identity, autonomy, and independence (Vander Veen & Rudman, 2022). Indeed, some open text responses raised concerns related to addressing driving in acute care when individuals may be at their “worst moments.” With decreasing availability of community occupational therapy services, however, acute care often becomes the only opportunity to discuss driving, despite the barriers which preclude in-depth assessment and intervention in hospital settings. Occupational therapists need to be attuned to the ways opposing risks transact with each other and the practical realities of the health care system when addressing driving in acute care settings (Vander Veen & Rudman, 2022).
Despite the challenges to addressing driving, results from the current study provide some evidence that occupational therapist competency for fitness to drive may be improving. For example, therapists in the current study had higher reports of competence (very competent or somewhat competent) for legal issues (53.8%), compared to respondents in the Korner-Bitensky et al. (2010) survey (39.8%). Furthermore, many respondents from the 2010 survey (Korner-Bitensky et al., 2010) expressed the desire to gain competency in providing alternative transportation options. In the current study, 33 (84.6%) respondents reported competence (very competent or somewhat competent) regarding sharing alternative transportation solutions, which may demonstrate increased competency in this domain as well. While there are differences in their respective respondent demographics, occupational therapists in the current study may have higher self-competence for awareness of legal implications and providing resources for alternate transportation.
In terms of how occupational therapists might gain competence for addressing medical fitness to drive, the most commonly reported resource accessed was occupational therapy practice guidelines. The findings of the present study suggest the current resources therapists are utilizing are not meeting the demand for further competency development for driving practice. Consistently, occupational therapist ratings of self-competence were lower than ratings of relevance for every knowledge area, suggesting that therapists view driving as relevant, but do not perceive themselves as having the matching competence to address it. Previous research has also suggested there are opportunities for competency building for driving practice across many contexts (Korner-Bitensky et al., 2010; Sangrar et al., 2018). Consequently, these findings are consistent with prior research, and signal that acute care therapists may need to explore additional avenues for competency development.
Competency development, as described by a sample of 317 occupational therapists in Quebec, is affected by both personal (knowledge/skills, motivation, etc.) and organizational factors (context/resources, climate/culture of organization, stressors/pressures from the working environment, etc.) (Rochette et al., 2020). While personal factors are perceived as modifiable, organizational factors are perceived to be less so (Rochette et al., 2020). These same organizational barriers to competency development also exist in the acute care occupational therapy setting including space, resources, culture, and time pressures (Britton et al., 2015, 2016; Murray et al., 2021). As such, these less modifiable organizational barriers to general competency development may also specifically impact capacity building for fitness to drive within acute care settings.
Going beyond barriers to identify solutions, primary strategies identified by therapists for developing competency include reflexive practice, reviewing evidence, collaborating with peers/colleagues, participating in continuing education, and supervising occupational therapy students (Rochette et al., 2020). Interestingly, while 27 (69.2%) respondents in the present study reported reviewing driving-related literature, only 20 (51.3%) reported seeking mentorship from other occupational therapists to gain competency. As such, it warrants further exploration to identify why peer mentorship and collaboration was only pursued by half of the respondents (n = 20) in the current study.
A study conducted in Australia that assessed the adherence of occupational therapist driver assessors to competency standards illustrates further strategies for enhancing competence. Fields et al. (2022) investigated the efficacy of providing individualized education using the Australian Competency Standards for Occupational Therapy Driver Assessors. Following individual sessions including education, personalized feedback from a practice audit, and encouraging reflection on how the session may affect their practice, occupational therapist adherence to competency standards increased (Fields et al., 2022). This research provides evidence that well-informed practice guidelines can be supplemented with such feedback to increase competency.
Implications for Occupational Therapy Practice and Education
Reflecting on results of the current study and extant research regarding competency development, there are several recommendations for supporting acute care driving practice. First, the Ontario occupational therapy practice guidelines could be utilized as a framework to provide focused education, to formulate feedback on therapist practice, and guide reflexive practice to support competency development (Fields et al., 2022). Second, providing more opportunities for occupational therapists to review driving literature and discuss with other therapists may prove to be a useful strategy to bolster competency in this practice area (Rochette et al., 2020). Fact sheets that include summarized research, practice recommendations, and case studies could be developed and shared during occupational therapy practice meetings to provide an opportunity for peer mentorship and discussion. Annual professional development education mandated by the regulatory colleges, such as the COTO, could be an avenue to support education to therapists about driving. Finally, further education could prioritize topics related to areas with the largest gaps in relevance and competence (i.e., legal implications and occupational therapist responsibility and strategies to navigate disagreement between the occupational therapist and client/family for driving recommendations). Occupational therapists cite considerable stress when approaching driving with clients, and identifying effective strategies to support competency development could potentially alleviate negative experiences and bolster job satisfaction. In fact, in a study investigating job satisfaction and retention of allied health professionals, competency was highly rated by participants as a determinant of job satisfaction and significantly predicted job retention in hospital settings (Wilson, 2015).
In terms of occupational therapy education, there may be an opportunity to consider how driving is addressed within the occupational therapy curriculum. Only 10 (25.6%) respondents reported learning about driving practice within occupational therapy curriculum, and 16 (41%) within clinical placements. Interestingly, it is only among those therapists with less than 10 years of practice experience who encountered any teaching about driving in the occupational therapy curriculum. However, among all participants with less than 10 years of experience, only 10 (32.3%) reported drawing upon learning experiences in occupational therapy school coursework to gain competency in driving. Based upon these findings, there is opportunity to enhance the competency for driving practice of entry level acute care clinicians. As time constraints are significant when therapists join practice, particularly in acute care, addressing driving more comprehensively in occupational therapy curriculum may be warranted. Previous research examining Canadian occupational therapy program curricula similarly supports enhanced training and development for driving-related competencies for students (Zur & Vrkljan, 2014).
Directions for Future Research
Further research is warranted to obtain deeper understandings of driving as a practice area in acute occupational therapy. Specifically, qualitative methods (interviews or focus groups) would serve to contextualize the data from the current study and identify key learning priorities and optimal strategies to gain competency for fitness to drive. Moreover, understanding some of the ethical and professional tensions that occupational therapists experience in addressing driving (Sangrar et al., 2018) and how they manifest in the acute care setting, would be valuable to inform how to best support therapists in this practice area fraught with barriers to an occupation-based practice (Murray et al., 2021). Future research is also warranted to develop and evaluate specific acute care occupational therapy practice resources to support driving-related competency development. Furthermore, as only therapists trained in the last 10 years reported receiving education in driving practice within their entry level occupational therapy program, it warrants exploring if there is an association between occupational therapy education and competence for driving. Finally, given the variability in occupational therapist reporting requirements to licensing authorities, examining driving practice across different jurisdictions could investigate if reporting responsibility influences self-reported competency.
Limitations
The present study aimed to include as many respondents as possible, however, the final sample size is modest. Furthermore, while some participants were selected at random from a purposive sample of the public register of occupational therapists, other methods involved using professional networks and associations, which may exclude occupational therapists who do not belong to these groups. Moreover, as with all survey data, there is a risk of selection bias, such that those with less time or interest in the topic, for example, may be less likely to participate, which may exclude important perspectives.
Conclusion
Occupational therapists report a discrepancy between perceived relevance and competence for knowledge areas related to driving such that ratings of competence were consistently lower than self-ratings of relevance. This discrepancy suggests that while occupational therapists consider driving knowledge areas to be relevant to acute care, therapists do not perceive they possess matching levels of competency to address them. Our findings support the need for further research into the feasibility and efficacy of strategies for competency development to advance occupational therapy practice that support driving and community mobility.
Key Messages
Acute care therapists report driving-related knowledge areas are relevant to practice, yet do not perceive they possess the competence to address such areas.
Acute care occupational therapists are invited to reflect upon their role with addressing driving within their setting and seek resources and mentorship to support any learning needs.
Further examination of the role of occupational therapists in addressing driving is warranted within and beyond the acute care setting to inform occupational therapy education, fieldwork, continuing education, and the development and evaluation of practice resources.
Supplemental Material
sj-docx-1-cjo-10.1177_00084174231182898 - Supplemental material for Addressing Driving in Acute Care: Perceived Relevance and Competence
Supplemental material, sj-docx-1-cjo-10.1177_00084174231182898 for Addressing Driving in Acute Care: Perceived Relevance and Competence by April Vander Veen, Jeffrey Holmes, Patricia Tucker and Liliana Alvarez in Canadian Journal of Occupational Therapy
Supplemental Material
sj-docx-2-cjo-10.1177_00084174231182898 - Supplemental material for Addressing Driving in Acute Care: Perceived Relevance and Competence
Supplemental material, sj-docx-2-cjo-10.1177_00084174231182898 for Addressing Driving in Acute Care: Perceived Relevance and Competence by April Vander Veen, Jeffrey Holmes, Patricia Tucker and Liliana Alvarez in Canadian Journal of Occupational Therapy
Footnotes
Ethics Board
Western University Health Science Research Ethics Board, in London, Ontario (Project ID: 120353).
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
Notes
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.