
Abstract
Background/objective
Fixed flexion deformity of the proximal interphalangeal joint can commonly occur following a traumatic injury impacting on hand function and occupational performance. Numerous interventions have been proposed for fixed flexion deformity resolution. This paper investigates the efficacy of static or dynamic orthoses in reducing fixed flexion deformity contracture following traumatic proximal interphalangeal joint injury.
Methods
A multi-database search of three databases (CINAHL, EMBASE, MEDLINE) was conducted. Data extracted for each study were design, patient descriptions, degree of fixed flexion deformity pre- and post-orthoses, and prescribed interventions and exercise programmes.
Results
The search yielded 643 studies, of which eight met the inclusion criteria. Studies used heterogeneous methodologies investigating various orthotic interventions. Meta-analysis or pooling of results was not possible. Dissimilar orthotic wear regimes were noted in all studies and an alternative clinical significance outcome was found.
Conclusion
More research is required to support clinical reasoning in orthotic choice for fixed flexion deformity of the proximal interphalangeal joint post-traumatic injury.
Introduction
The proximal interphalangeal joint (PIPJ) has the largest arc of motion (up to 120°) of the three joints in each digit of the hand. It is estimated that this joint accounts for 85% of the total motion required to grasp an object (Blazar & Steinberg, 2000; Hogan & Nunley, 2006). Unfortunately, the PIPJ is uniquely vulnerable to injury and is inclined to become stiff shortly after trauma or immobilisation. An understanding of the anatomy, the potential for joint instability, and treatment options are essential in the management of these injuries provided by occupational therapists in hand therapy practice (Comer, Clark, & Yao, 2015).
The PIPJ is formed by the head of the proximal phalanx, which is shaped like a short transverse cylinder, and the base of the middle phalanx, which is concave in shape (Skirven, Osterman, Fedorczyk, & Amadio, 2011). The phalangeal head has a sagittally orientated groove and the base has a sagittally oriented ridge. These anatomical features enhance the stability of the joint and ensure that the motion is limited to one degree of freedom (flexion and extension) (Comer et al., 2015). The joint capsule of the PIPJ is reinforced by the volar plate palmarly, the collateral and retinacular ligaments and lateral bands laterally and medially, and the triangular membrane and central bands dorsally. These soft tissue structures contribute to PIPJ stability, however, following injury or trauma can contribute to joint stiffness or deformity (Harrison, 1977).
Fixed flexion deformity (FFD), also known as flexion contracture, is a common complication following traumatic injury to the PIPJ (Hunter, Laverty, Pollock, & Birch, 1999). Although a PIPJ with a FFD may present with a similar pathogenesis, the factors that result in joint stiffness can vary significantly between cases (Yang, McGlinn, & Chung, 2014). Such factors include immobility or poor positioning following the initial acute trauma, post-traumatic shortening or adherence of the soft tissues, and scar and oedema formation of the surrounding structures (Boccolari & Tocco, 2009; Callahan & McEntee, 1986; Hogan & Nunley, 2006; Hunter et al., 1999; Kennedy, Peck, & Stone, 2000; Wu, 1991). The clinical presentation of a FFD typically demonstrates an extension deficit, however, a loss in both flexion and extension range of motion (ROM) may be observed. Reported functional impacts because of this reduction in ROM include difficultly in grasping objects, shaking hands, putting on gloves, completing self-care tasks, and putting the effected hand in a pocket (Hogan & Nunley, 2006; Wollstein, Rodgers, Ogden, Loeffler, & Pearlman, 2012).
The management of chronic FFDs of the PIPJ poses a difficult challenge for hand surgeons and therapists working in hand therapy as outcomes are often unpredictable and poor. Multiple treatment modalities have been described for the management of chronic FFD of the PIPJ, producing limited results. Typically, non-operative treatment using an orthosis or serial casting is trialled prior to open surgical release using two types of orthoses, static and dynamic, which utilise different mechanical principles (Wu, 1991). Static orthoses use a three-point pressure static/inelastic principle, while dynamic orthoses have a static base and a mobilising/elastic element to assist with the force applied to the joint (Glasgow, Tooth, & Fleming, 2008; Li, 1999). The aim for either orthotic design is to enable tissue growth and remodelling by holding the contracted tissue under constant tension that is higher than resting tension (Bell-Krotoski & Figarola, 1995). This process results in the formation of new cells that create a collagen network that can be reoriented to the length required (Brand, 1995).
Static orthoses can be stratified into two types: static progressive and serial static (Glasgow et al., 2008). Static progressive orthoses consist of a stable base and an element of mobility using an inelastic material such as nylon monofilament, cord, or Velcro strap which holds the PIPJ at the end range of available passive extension. Serial static orthoses hold the PIPJ at the available end range of passive extension. Both static progressive and serial static orthoses require regular review and adjustment to ensure adequate extension force is applied as the contracture of soft tissues decreases and growth occurs. Dynamic orthoses are known to provide gentle, controlled, persistent force to the joint, which can also reduce pain and discomfort (Callahan & McEntee, 1986; Li, 1999).
To date, there is no consensus on the best orthotic treatment for FFD following a traumatic PIPJ injury. This article systematically reviews all literature investigating conservative management of chronic FFDs of the PIPJ following a trauma using orthotic intervention. Our objectives were to:
Describe and critique the study designs, methodologies, and intervention protocols used in the international literature, Compare the outcomes of static and dynamic orthoses used to manage post-traumatic FFD of the PIPJ, Provide recommendations for future research in this area.
This review was registered on Prospero; International Register for systematic reviews, in September 2014 (Registration number: CRD42014013838).
Methodology
Search strategy
Relevant articles were identified from a search of MEDLINE Complete (1946–May 2017), EMBASE (1974–May 2017), and CINHAL (1937–May 2017). A combination of search terms relating to FFD of the PIPJ and orthotic intervention was developed in consultation with a medical librarian (see Appendix 1). The search was restricted to publications in English with the following selection criteria applied:
The study was confined to conservative management of chronic FFD resulting from a trauma. Studies that reported participants who were receiving acute management; had undergone surgery for deformity in the previous 12 months; or had a confirmed diagnosis of acute concomitant injuries, infections, systemic diseases, or previous neurological spasticity or pathology were excluded. The study reported use of one or more conservative orthotic management interventions. The study used a Level IV (Case series) or higher study design as per the NHMRC Evidence Hierarchy (Coleman et al., 2005). The study was published in a peer-reviewed journal. Abstracts presented at conferences and editorials were excluded. Theses and dissertations were also excluded.
The reference lists of included articles were also screened to identify additional articles suitable for inclusion.
Data extraction and quality assessment
The data was extracted independently by one reviewer (NY) using a standardised form, which contained characteristics of subjects (including trauma type), degree (°) of pre-intervention FFD, duration of time FFD had been present prior to treatment, orthoses description and regime, prescribed exercise programme, and results. A second reviewer (LSR) checked the data for accuracy.
The study design and analytical methods were also recorded for quality appraisal using the PEDro Scale (Moseley, Herbert, Sherrington, & Maher, 2002), a checklist that evaluates the quality of randomised control trials of physical therapy interventions. Studies were rated according to the PEDro classification criteria where a score of 6–10 indicates high quality, a score of 4–5 indicates fair quality, and a score of ≤3 indicates poor quality.
Data synthesis
Synthesis of data was primarily narrative due to the heterogeneity of studies (differing study design, methodologies, and outcome measures), inadequate statistical data, and methodological limitations.
Results
Description of included studies
The initial search strategy yielded a total of 738 articles, with 643 non-duplicate citations identified. After screening of titles and abstracts by two reviewers (NY and NT), the full text of 24 articles was assessed for eligibility. Sixteen articles were excluded during full-text screening. Eight studies involving 190 (range 4–46) individuals with 214 FFDs of the PIPJ published over a 17-year period (1995–2012) were deemed suitable for inclusion in this review. The detailed PRISMA flow chart of the search process is summarised in Figure 1. Study settings included Australia, United States of America, and Italy.
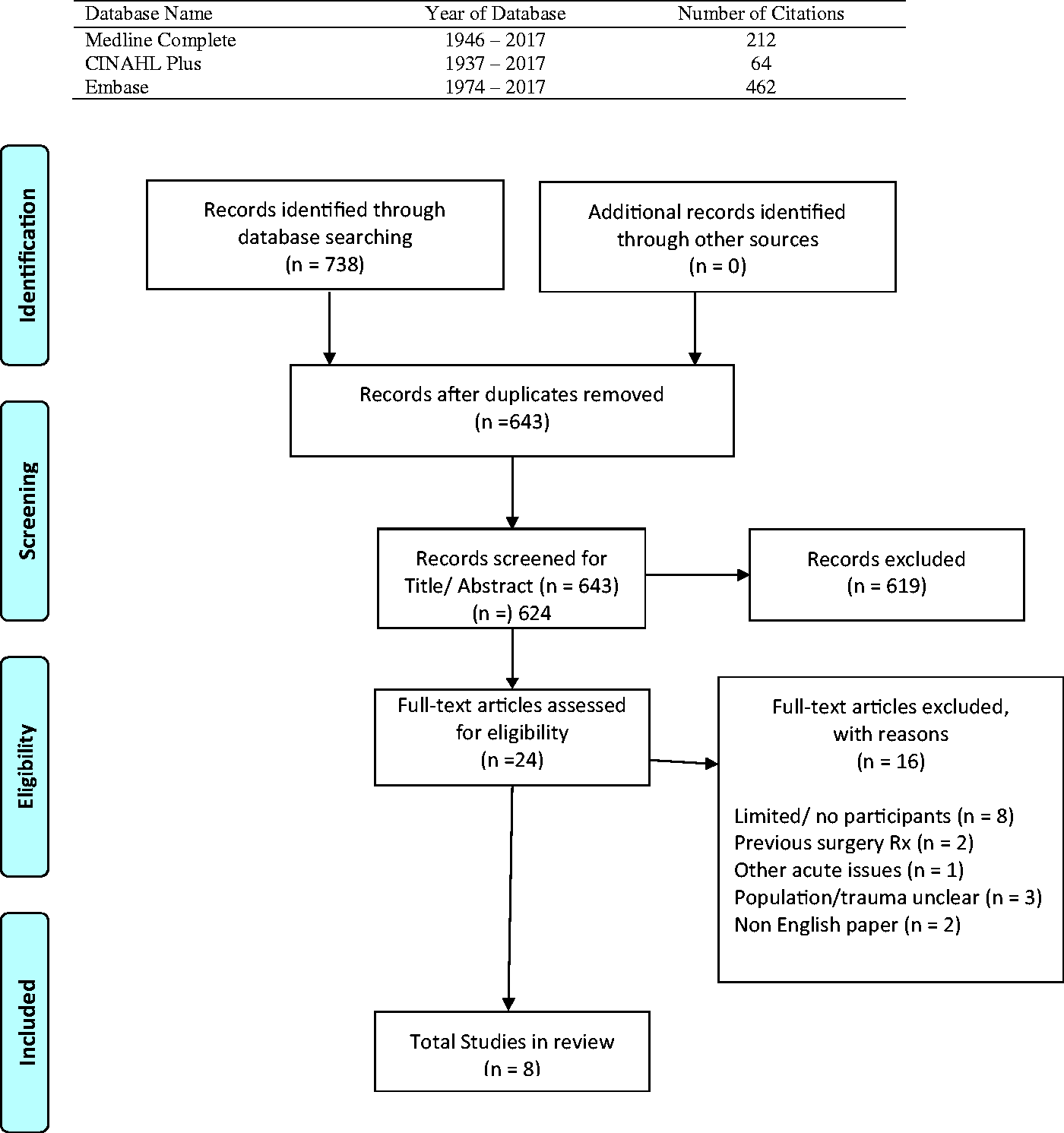
PRIMSA flow diagram of study selection.
Classification of selected studies
The eight included studies consisted of varying levels of research quality as demonstrated by PEDro scores (range 2–10; mean 5.87) as reported in Table 1. The study designs included three randomised controlled trials (RCTs) (Level II Evidence) and five case series studies (Level IV Evidence). No included study compared the use of both static and dynamic orthoses. Three of the included studies investigated multiple joints or deficit types and four did not provide baseline FFD ROM measures.
PEDro scoring.
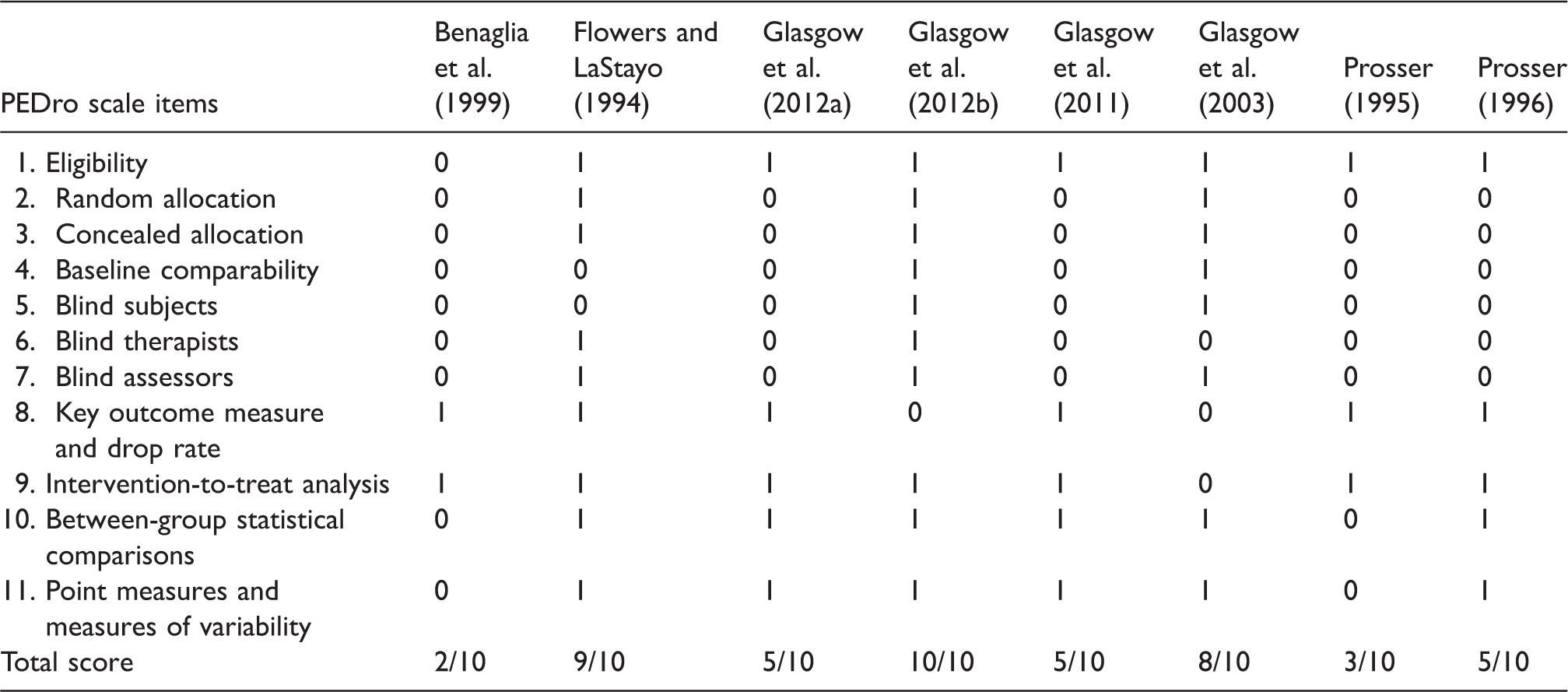
PEDro: Physiotherapy Evidence Database Scale; Yes = 1, No = 0.
Population
The demographic and baseline data of the participants recruited for the included eight studies are summarised in Table 2. The median number of participants recruited to each study was 21 (IQR 13.75–34.25). The mean age of participants, which was reported in five studies, was comparable between studies (range 35–40 years). All studies included participants who had developed a FFD because of a traumatic injury, with six of the studies specifying trauma type which included damage to the joint capsule, joint capsule damage and fracture, dislocation with soft tissue injuries including volar plate and sprain of the collateral ligaments, flexor and extensor tendon injuries, and distal radius fractures.
Summary of characteristics of the included studies.

ADL: Activities of Daily Living; AROM: active arnge of motion; CI: confidence interval; DIP: distal interphalangeal joint; FFD: fixed flexion deformity; MCP: metacarpal phalangeal; PIP: proximal interphalangeal; PIPJ: proximal interphalangeal joint; PROM: passive range of motion; QID: quater in die/ 4 times daily; ROM: range of motion; SD: standard deviation; TERT: total end range time; TROM: total range of motion.
Baseline measures of the degree of FFD deficit (using ROM goniometry) were reported in half of the reviewed studies, with results varying between studies. The reported mean FFD deficit measurements were 27° (Benaglia, Sartorio, & Franchignoni, 1999), 31° (Prosser, 1995), and 39° (Prosser, 1996), while one study reported a range of 15°–60° (Flowers, 2002). Six studies provided details regarding the time since injury or deformity. All included studies provided intervention to deficits that were no more than six months old. No paper included in this review used a standardised assessment or classification criteria to determine severity of injury.
Intervention
Table 2 shows the interventions, orthotic regime, and exercise programmes used in each study. More than half of the included studies investigated the effectiveness of dynamic orthoses using a custom-made capener orthosis. One study compared two different dynamic orthoses designs: a custom-made capener and a dynamic low-profile hand-based outrigger orthosis (Prosser, 1996). Three studies investigated the effectiveness of static orthoses using three different designs: serial casting (Flowers & LaStayo, 1994), modified belly orthotic (Glasgow, Wilton, & Tooth, 2003), and static progressive hand-based orthotic (Benaglia et al., 1999; Flowers & LaStayo, 1994).
The amount of force used was consistent for six of the included studies reporting the application of 200–250 g. One study reported an application of 800 g of force using serial casting (Flowers & LaStayo, 1994). One study which used a hand-based static progressive orthosis did not report a measure of force applied, instead using subjective discomfort reported by the participant as a clinical indication for excessive force (Benaglia et al., 1999). All studies reported regular monitoring of the amount of force applied by the orthosis, with follow-up appointments every one to two weeks during the intervention time frame.
Orthotic wear regime was clearly defined in all studies. Prosser (1996) investigated dynamic orthotic wear of 8–12 hours per day/night for eight weeks. The final mean total end range time (TERT) wear reported was 10 hours (SD: 3). In her second study, Prosser (1995) describes an orthotic regime of 6–12 hours of dynamic orthotic wear per day over an eight-week period, with final mean TERT wear of 11 h. Glasgow, Fleming, Tooth, and Hockey (2012a) investigated the use of a custom-made capener orthosis for a minimum of 6–12 hours per day. A TERT wear of 10.8 hours (SD: 2.1) was reported. Glasgow, Fleming, Tooth, and Peters (2012b) randomly allocated daily TERT wear of a dynamic capener orthotic regimen as either 6–12 or 12–16 hours. A daily mean TERT of 9.5 hours for the first group and 11.5 hours for the 12–16 hours group was reported (Glasgow et al., 2012b). In their second study, Glasgow, Tooth, Fleming, & Peters (2011) reviewed dynamic orthotic wear over a minimum of 6–12 hours per day. Separate data were not available for this study between flexion and extension deficits and TERT outcomes were not reported (Glasgow et al., 2011).
Glasgow, Wilton, and Tooth (2003) reviewed a four-week static orthotic programme, with a modified belly orthotic, reviewing a daily TERT wear programme of less than 6 hours compared to 6–12 hours. Separate data were not available for the actual TERT-modified belly orthotic regime. A case review of four participants by Bengalia, Sartorio, and Franchignoni (1999) applied a static progressive orthosis for 1 hour TERT wear followed by 1 hour rest, six times per day until contracture resolution was achieved. During the rest period, participants completed AROM exercises.
Daily TERT wear reported in two studies was left to the discretion of the participants as they could select continuous or intermittent wear of their orthosis. Five studies did not specify if the TERT wear time was continuous or intermittent (see Table 1).
Flowers and LaStayo (1994) compared 3–6 days of consecutive serial casting. The aim of the study was to examine the association between length of time in cast and final extension ROM of the PIPJ. The results demonstrated that six days of TERT wear were clinically significant in achieving a greater increase in PROM compared to three-daywear (60° (
In addition to the orthotic wear, a home exercise programme was described in seven of the eight studies. Exercise programmes consisted of Active ROM, Active and Assisted ROM, Oedema Management, and Functional Hand Use. A detailed description of the exercise programmes for all studies is reported in Table 1.
Outcome
Due to the limited available data and findings in the included eight studies, no conclusive evidence to support one orthotic design as being superior in FFD contracture resolution was found.
All included studies of dynamic and static orthoses regime reported an improvement in FFD following application of an orthoses over varied lengths of TERT wear. A full description of the reported FFD, AROM, PROM, and total range of motion improvements following intervention is reported in Table 2. In addition to different orthotic regimens, the TERT wear for all studies varied. Daily TERT wear reported to achieve a reduction in FFD varied from 9 to 11.5 h in four studies (Glasgow et al., 2012a, 2012b; Prosser, 1995, 1996).
Discussion
Despite FFD of the PIPJ joint being a common clinical problem following traumatic injury, we identified only eight studies that investigated conservative management using static or dynamic orthoses. A significant portion of fully reviewed papers did not fulfil the selection criteria as they presented as a literature review, a case study, consisted of other conditions or joints, involved previous surgical intervention, were published in languages other than English or did not clearly define conditions under examination. Included studies utilised heterogeneous methodologies with differing study designs, orthotic types, levels of force applied, home exercise programmes, and orthosis wear time. Pre-intervention FFD measurements and trauma types were not provided for all studies.
Included studies were mostly conducted in Australia, highlighting a gap in the available literature for Africa, Asia, the Americas, and Europe. One explanation for the lack of published studies in some of these geographical regions is that notion that different cultures may have different approaches to hand therapy or treatment priorities. A recent investigation of the experiences of Australian volunteer therapists in Bangladesh to provide recommendations for future therapy capacity building projects identified cultural differences such as learning styles, knowledge, skillset, clinical reasoning, and referral differences between surgeons and therapists which may delay intervention (O’Brien & Hardman, 2014). In addition, the authors of this study report that Western practices were often a poor fit owing to the fact that there was a mismatch between theoretical knowledge and clinical reasoning skills, or simply a disparity between knowing and doing. Another explanation for a lack of published studies in Africa and Asia may be the availability, feasibility, and financial sustainability of sourcing materials such as thermoplastic and Velcro.
The quality of the included studies was varied. Five out of the eight studies were rated fair to poor quality for the lack of random allocation; blinding of participants, therapists, and assessors; and baseline comparability. However, it should be noted that blinding of participants or therapists in these studies is not considered feasible given the nature of the intervention itself. It is therefore recommended that random allocation and blinded assessors should be considered by researchers in future study design. Limitations of the included studies included small sample sizes, which impact on the generalisability of results, and the lack of direct comparison between the use of dynamic and static orthosis.
No standardised measure or classification of the severity of injury was utilised in any included study, instead relying on improvements in pre- and/or post-intervention ROM measures. The Hand Injury Severity Scoring (HISS) system, which is useful measure of severity and guide to likely outcome, is a suitable measure which should be considered in the development of future studies to provide a quantitative measurement of trauma severity beyond ROM (Campbell & Kay, 1996). Further, no included study utilised a standardised functional outcome measure, such as the Canadian Occupational Performance Measure (COPM) (Law et al., 1998), or hand-specific outcome measure, such as the Disability of the Arm, Shoulder, and Hand (DASH) (Hudak et al., 1996), to quantify intervention outcome. This is a major limitation of the reviewed studies as an individual may regain significant ROM following intervention, but still experience functional limitations which may challenge their competency and ability to carry out their chosen occupations (Robinson, Brown, & O’Brien, 2016).
Use of a dynamic orthosis, which provides gentle, controlled, persistent force to the joint, was the most investigated intervention regime in all reviewed papers (Hooper & North, 1982; Li, 1999). The amount of force applied for orthoses under investigation was consistent across most studies (200–250 g of force), except for one study investigating serial casting (800 g of force) (Flowers & LaStayo, 1994). The level of force applied in the included studies is consistent with research on tissue remodelling that uses a low-load prolonged stretch to promote tissue growth and avoiding forceful stretch that may result in tissue damage (Bell Krotoski, 2011; Brand, 1995).
All five studies that investigated the use of dynamic orthoses fabricated a custom-made orthosis, with no studies utilising a pre-fabricated orthotic option. Therefore, from the reviewed literature it is not possible to comment on the efficacy or outcome of pre-fabricated dynamic orthoses in the management of traumatic FFD of the PIPJ. While it is acknowledged that custom-made orthoses can be time consuming for beginners, the findings of this review suggest that a custom-made dynamic orthosis should be the preferred approach used by therapists (Boccolari & Tocco, 2009). Additionally to our findings, this design is also known to be cheaper and more comfortable when compared to pre-fabricated orthoses (Boccolari & Tocco, 2009; Callahan & McEntee, 1986).
Serial casting has been reported to be easy to fabricate, in addition to having low fabrication costs and a low profile, decreasing the functional and financial impact on the individual (Callahan & McEntee, 1986). Despite these factors, only one study included in this review investigated serial casting (Flowers & LaStayo, 1994). In this study, individuals were provided serial casts for either a three- or six-day period to establish if TERT wear time impacted on contracture resolution. The authors reported findings that six days of TERT wear were clinically significant in achieving greater PROM compared to three days wear. Such findings are promising for therapists; however, due to the limited evidence available it is difficult to generalise these findings.
Although a clinical reduction in the FFD severity, as measured by changes in ROM, was observed in all included studies, it remains unclear if one type of orthosis is more superior in contracture resolution. The frequency of review appointments during intervention time frames was consistent, with most studies completing weekly reviews, suggesting that close monitoring is clinically relevant for therapists to assess, adjust the amount of force, review home exercise programmes, and track clinical outcomes. It was also observed that an increase in TERT wear was more likely to lead to clinically significant outcomes in changes of ROM; however, changes in functional outcomes were not established.
Limitations of this review
The findings of this study may be limited by examining studies only published in English. It is possible that a wider search of additional databases and grey literature may have uncovered additional studies.
Summary of evidence
The consensus of the best orthosis for contracture resolution of a traumatic PIPJ FFD is unclear. There is no evidence available to indicate if the use of dynamic or static orthoses results in superior clinical outcomes. It was found that positive improvements in FFD severity have been reported for both orthotic types.
The limited evidence identified from this systematic review is that six days of TERT, using serial casting, demonstrated a statistically significant improvement in PROM compared to three days of TERT. A secondary finding identified by this review was that daily TERT does not necessarily need to be continuous splint wear. In future application, the therapist should educate the client to wear the splint as much as possible over the day as this has been seen to be more superior in contracture resolution compared to shorter periods of time.
Clinical implications
Despite limited evidence, some findings in this review can be utilised in daily clinical practice. Both static and dynamic orthoses can be used in conjunction with a number of home exercise programmes, which may include AROM, PROM, daily functional use, and appear to result in a positive outcome. A major consideration when using either orthotic type is the prescribed TERT, with increased daily wear time more likely to lead to a timely and successful outcome.
Experienced therapists should consider fabricating a dynamic capener orthosis with approximately 250–500 g of force, which encourages tissue remodelling and attempts to avoid tissue damage. Static options, such as serial casting, can be considered as a cheaper option within a clinical setting.
Overall, both dynamic and static orthoses appear to be safe and effective in contracture resolution for the post-traumatic FFD of the PIPJ. It is recommended that occupational therapists address functional limitations and activity restrictions, in addition to changes in body structures and functions, in order to achieve a return to meaningful occupations (Robinson et al., 2016). Ultimately, professional reasoning of the therapist should be used due to the lack of evidence-based findings keeping the occupational needs of the client in mind.
Future research recommendations
Given that the aim of this systematic review was to establish if there is evidence highlighting whether static, static progressive or dynamic orthoses use was more effective in contracture resolution for the traumatic injuries of the PIPJ, the evidence available does not provide an answer. Ultimately, a RCT with sufficient power and a stringent methodology that compares static and dynamic orthosis outcomes is required. It is suggested that future studies ensure that the assessor is blinded, and appropriate baseline measures and summary of prescribed home exercise programme are clearly documented. Suggested outcome measures that should be considered in study design include TERT, ROM, HISS, DASH, COPM, pain scale, functional limitations reported by the client whilst wearing the orthosis, and time to achieve contracture resolution. Overall, more research could help establish a preferred, evidence-based intervention for a commonly seen hand deformity which is known to have large functional implications.
Conclusion
This review identified few studies that have attempted to examine the efficacy of interventions for the resolution of FFD of the PIPJ. Both static and dynamic orthosis have been found to provide a clinical improvement in FFD, however, a lack of statically significant results means a consensus for best practice cannot be established. Based on the findings of this review, therapists treating FFD of the PIPJ should consider using a custom-made dynamic capener orthoses using professional reasoning to determine TERT wear. Further research using stringent methodology and a consensus of outcome variables could provide therapists with guidance on best practice management of FFD of the PIPJ.
Footnotes
Acknowledgements
Occupational Therapy Department, Eastern Health, Victoria, Australia
Allied Health Research Department, Eastern Health, Victoria, Australia
Library Staff, Eastern Health, Victoria, Australia
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.