
Abstract
Objective
Home safety assessment and intervention is a key component in the management of fall risk in elderly people. However, a standardised assessment for home safety has not yet been established in Japan. We developed a Japanese version of the Westmead Home Safety Assessment by partially modifying the original version according to house structures and lifestyles in Japan and examined its inter-rater reliability and content validity.
Methods
Japanese elderly in the community who had fear of falls were recruited to investigate the reliability of the Japanese version of the Westmead Home Safety Assessment. Two occupational therapists simultaneously visited a participant’s home to perform the Japanese version of the Westmead Home Safety Assessment independently. Further, an expert panel of 18 occupational therapists evaluated the relevance of each item of the Japanese version of the Westmead Home Safety Assessment.
Results
Fifty elderly people (aged 78.2 ± 7.1 years) participated in this reliability study. The most frequent hazards were identified as internal steps/stairs, seating, bathroom, bath, and external steps/stairs. Forty-nine items (69%) in the Japanese version of the Westmead Home Safety Assessment were rated to have fair to good (0.40 < κ < 0.75) or excellent (κ ≥ 0.75) reliability as well as excellent validity (item content validity ≥0.78). These items were concerned with basic activities of daily living and some simple instrumental activities of daily living. The scale content validity was 0.78 ± 0.16 but was not excellent (scale content validity index <0.90).
Conclusions
This study suggested that 49 items in the Japanese version of the Westmead Home Safety Assessment were appropriate for home safety assessment for Japanese elderly. Further research is necessary to improve the reliability and validity of the present version of the Japanese version of the Westmead Home Safety Assessment for this population.
Introduction
Prevention of falls is an urgent public health challenge because injuries as a consequence of falls are a leading cause of long-term care among elderly people. Falls are the fifth-ranked cause of living with disability among people aged 80 years and older worldwide (GBD 2015 Disease and Injury Incidence and Prevalence Collaborators, 2016). In Japan, for elderly people certified by municipal governments as needing long-term care, bone fractures or falls accounted for 10.2% of all major causes of long-term care requirement (Ministry of Health, Labour, and Welfare, 2010).
Home safety assessment and intervention can reduce both the rate of falls and risk of falling (Clemson, Mackenzie, Ballinger, Close, & Cumming, 2008; Gillespie et al., 2012). They would be more effective when implemented for high-risk participants and provided by occupational therapists (OTs) (Clemson et al., 2008; Gillespie et al., 2012; Pighills, Torgerson, Sheldon, Drummond, & Bland, 2011). Regarding OTs’ roles in fall prevention, implementing an intensive home safety assessment to take into account the interaction between an individual client and his/her environment (Clemson, Donaldson, Hill, & Day, 2014; Pighills, Ballinger, Pickering, & Chari, 2016) and using problem-solving techniques and including the client in the decision process (Clemson et al., 2014) are beneficial to the aforementioned effectiveness.
A standardised home safety assessment is important to minimise evaluator bias and provide compatibility of evaluation findings about home hazards and is eventually beneficial to provide an accountable and consistent implementation to prevent falls. In Western countries, some assessments originated by OTs with adequate reliability have been developed, such as the Safety Assessment of Function and Environment for Rehabilitation-Health Outcome Measurement and Evaluation (Letts, Scott, Burtney, Marshall, & McKean, 1988), the Westmead Home Safety Assessment (WeHSA) (Clemson, Fitzgerald, Heard, & Cumming, 1999), the Home Falls and Accidents Screening Tool (Mackenzie, Byles, & Higginbotham, 2002; Vu, & Mackenzie, 2012), and the Cougar Home Safety Assessment (Fisher, Coolbaugh, & Rhodes, 2006). However, there is no standardised home safety assessment for fall prevention in the Japanese population.
This study aimed to develop a home safety assessment appropriate to be used by OTs for the elderly with risks of falls in Japan. We modified the WeHSA (Clemson, 1997) that had already been established in Australia to develop a Japanese version for Japanese elderly and examined its inter-rater reliability and content validity.
Methods
Instrument development
From the above-mentioned home safety assessments, the authors selected the WeHSA (Clemson, 1997), which consists of a large number of items to evaluate fall hazards.
The WeHSA consists of 72 items that are rated using a 2-point scale (hazard/no hazard) or ‘not relevant’ according to a home visit by an OT. Hazard options are provided for each item, and the raters also identify the types of hazards.
The Japanese version of the Westmead Home Safety Assessment (WeHSA-J) was developed according to the following steps: forward translation of the evaluation form and its manual, back translation of the form and manual, a pilot test conducted with two elderly persons, and cultural adaptation. Although new evaluation items were not added to the WeHSA-J, minor changes to the names of 10 items in the original WeHSA were made to suit the structural features of Japanese homes (Appendix 1). For example, a typical Japanese bathroom area consists of a dressing room adjacent to a bathroom and components in a bathroom such as a bath, washing place, and shower (Figure 1); therefore, we modified the evaluation items in the category of ‘bathroom’ of the original WeHSA. Additionally, because a typical Japanese house has tatami rooms for sitting on a cushion on the floor and sleeping on a futon on the floor (Figure 2), these cases were also evaluated using the WeHSA-J items ‘seating’ and ‘bed’ of the WeHSA. All the changes and cultural adaptations in the WeHSA-J were approved by the original author of the WeHSA.
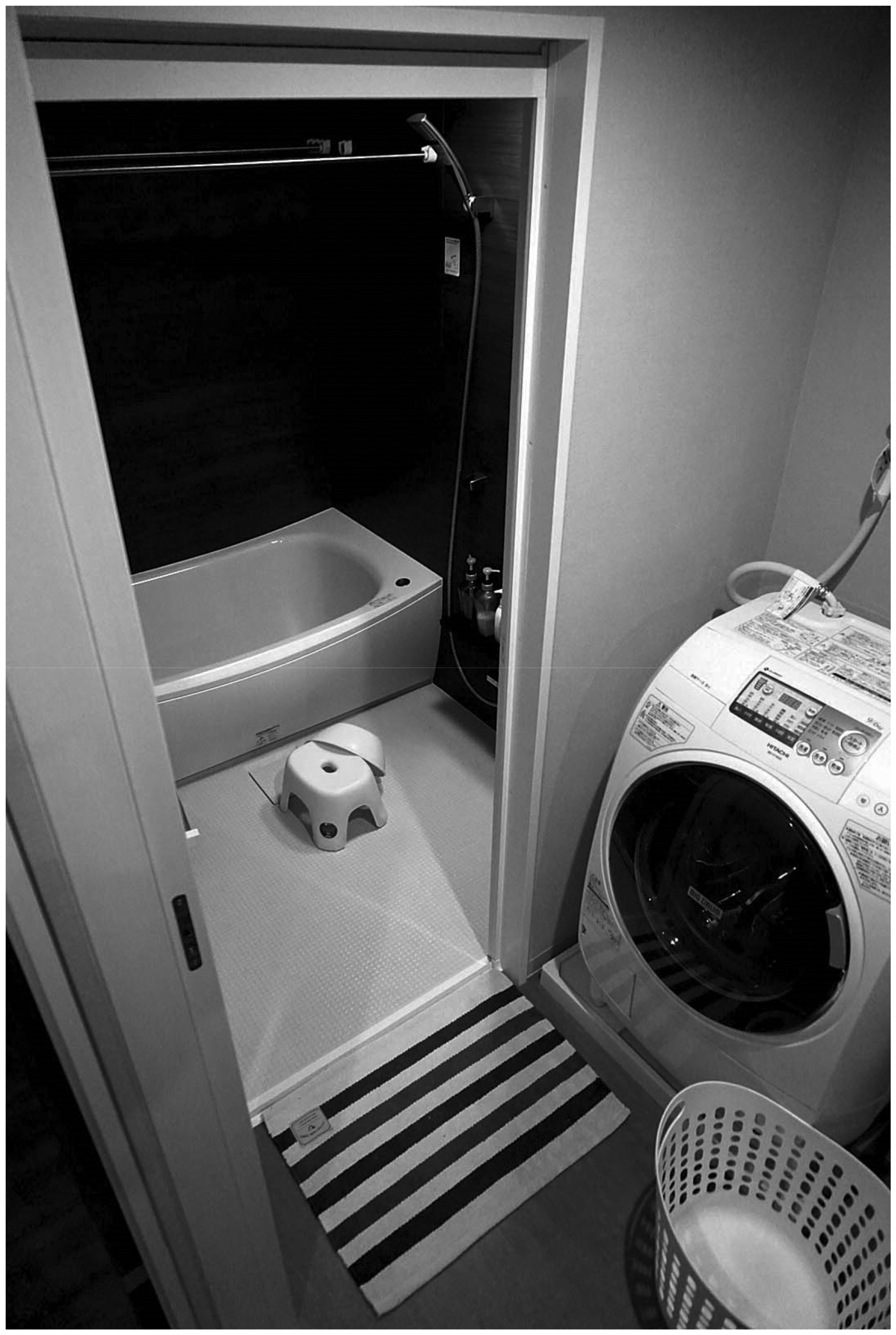
A Japanese bathroom and a dressing room. A typical Japanese bathroom area consists of a bathroom and a dressing room adjacent to a bathroom.
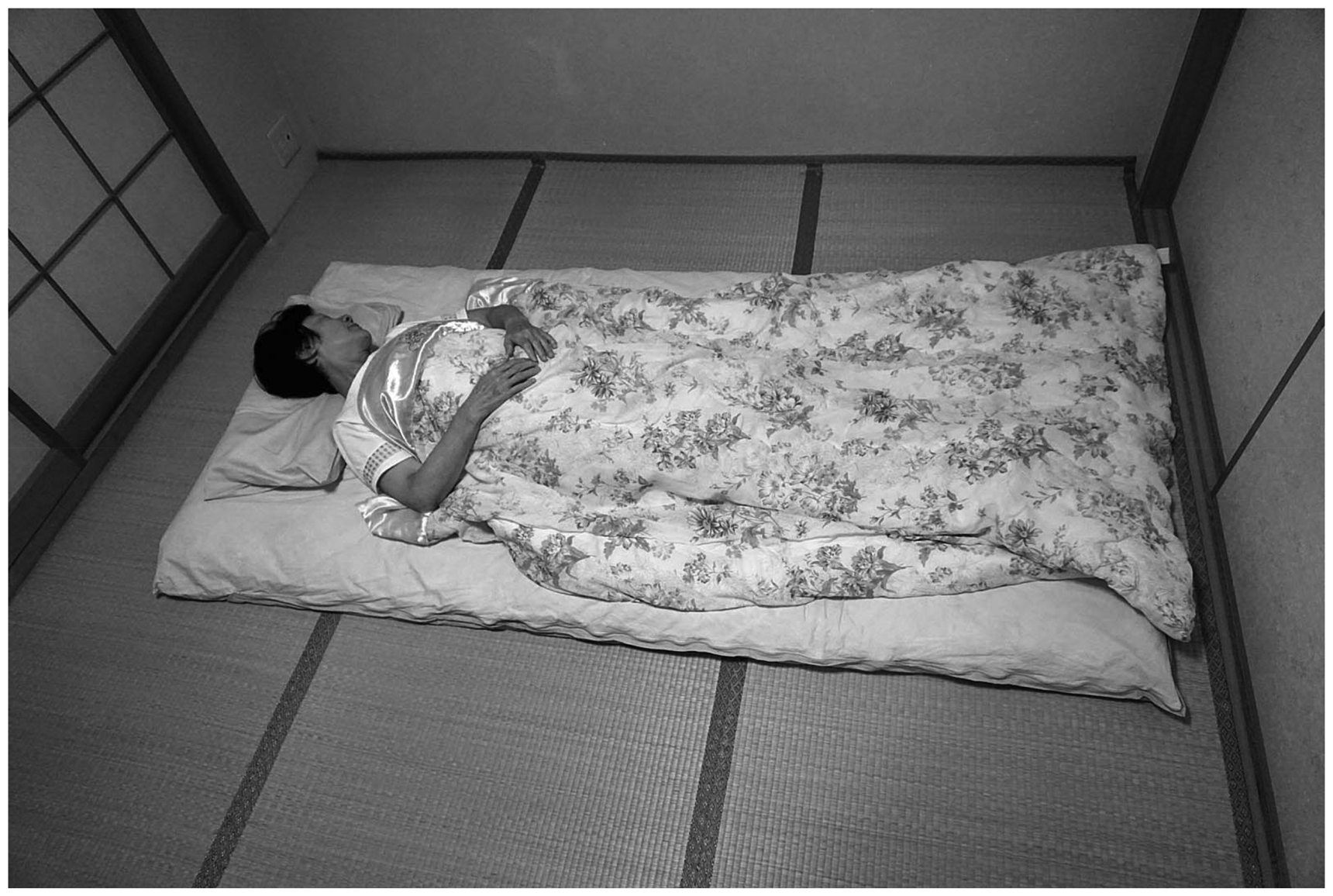
Sleeping on a futon in a tatami room. A typical Japanese house has tatami rooms for sleeping on a futon and sitting on a cushion on the floor (tatami).
Reliability and validity
This study examined both the inter-rater reliability and content validity of the WeHSA-J. The authors gave OTs workshops to administer the WeHSA-J, including two lectures (4 hours in total). The OTs implemented the WeHSA-J at their own clinical sites, reported the results, and then received feedback. To assess the inter-rater reliability of each rating for the 71 items in the WeHSA-J, some OTs who had completed our workshop recruited participants under the following two conditions: (1) elderly people who either lived at home or were planning to be discharged from the hospital, and (2) were able to walk indoors with or without assistance but had risks of falls as determined by OTs and family members or fear of falls by the elderly themselves.
To examine the reliability, two raters simultaneously visited the participants’ homes and performed independent assessments. One rater was the OT (the therapist rater) who recruited the participants for this study, and the other rater was the second author (the expert rater) who developed the WeHSA-J. We also collected information regarding the participants’ ages, genders, living conditions, primary diagnoses, indoor locomotion methods, Berg Balance Scale (BBS) scores (Berg, Wood-Dauphinee, Williams, & Maki, 1992), and the number of falls in the prior year. The BBS is widely used to observationally measure balance and assess the risk of falls in elderly people, with scores ranging from 0 to 56. The risk of multiple falls is supposed to increase with a score below 45 and increase significantly with a score below 40 (Muir, Berg, Chesworth, & Speechley, 2008).
The content validity of the WeHSA-J was examined by an expert panel. We mailed the questionnaire about its validity to 24 OTs who did not participate in the WeHSA-J workshop and had 10 or more years of clinical experience including the implementation and/or education of home modification. Each expert was asked whether each item of the WeHSA-J was relevant as an evaluation item for identifying fall hazards at home in Japanese elderly using a 4-point scale (1 = not relevant, 2 = somewhat relevant, 3 = quite relevant, and 4 = highly relevant).
This research protocol was approved by the Ethical Committee of School of Medicine, Shinshu University. Written informed consent to participate in this study was obtained from all the participants.
Data analysis
Cohen’s kappa (κ) coefficient was used to examine the reliability, and the item content validity index (I-CVI) and the scale content validity index (S-CVI) were used to examine the validity.
As reported in the reliability study by the original authors of the WeHSA (Clemson et al., 1999), the results of the hazard rating were analysed using a binary variable: ‘hazard’ and either ‘no hazard’ or ‘not relevant’. According to the criteria proposed by Fleiss, Levin, and Paik (2003), a range of κ ≦ 0.4 was defined as poor, a range of 0.4 < κ < 0.75 was defined as fair to good, and a range of 0.75 ≦ κ was defined as excellent. The statistical significance level was set at P < 0.05.
The I-CVI score was calculated by dividing the number of experts who gave a rating of 3 (quite relevant) or 4 (highly relevant) by the total number of experts. The S-CVI score was the average of the 71 I-CVI scores. According to the criteria proposed by Polit and Beck (2015), I-CVIs of 0.78 or higher were excellent, and S-CVIs of 0.90 or higher were excellent.
SPSS version 23.0J was used for the data analysis.
Results
Participants
Fifty elderly people (aged 78.2 ± 7.1 years, 29 males (58%) and 21 females (42%)) participated in this reliability study (Table 1). Most of the participants lived with other individuals (n = 41; 82%). The participants’ diagnoses included cardiovascular disease, osteoarthritis, cancer, etc. Regarding indoor locomotion methods, 26 participants (52%) walked independently without a walking aid, 11 (22%) walked independently with a walking aid, and 13 (26%) walked with assistance. The BBS score of all participants ranged from 5 to 50, and 30 (60%) were below 40; eight (16%) were between 41 and 44; and 12 (24%) were 45 and over. The self-reported number of falls in the past year was as follows: 23 participants (46%) reported none, 7 (14%) reported one fall, 19 (38%) reported two or more falls, and one (2%) reported ‘unknown’. None of the participants demonstrated impaired visual performance. The reasons for conducting the WeHSA-J on each participant were as follows: a home visit before discharge from the hospital for 22 participants (44%), consultation on fall prevention for 17 (34%), and community-based OT services for 11 (22%). A total of 13 OTs participated in this reliability study as therapist raters.
Characteristics of the participants in the reliability study (n = 50).
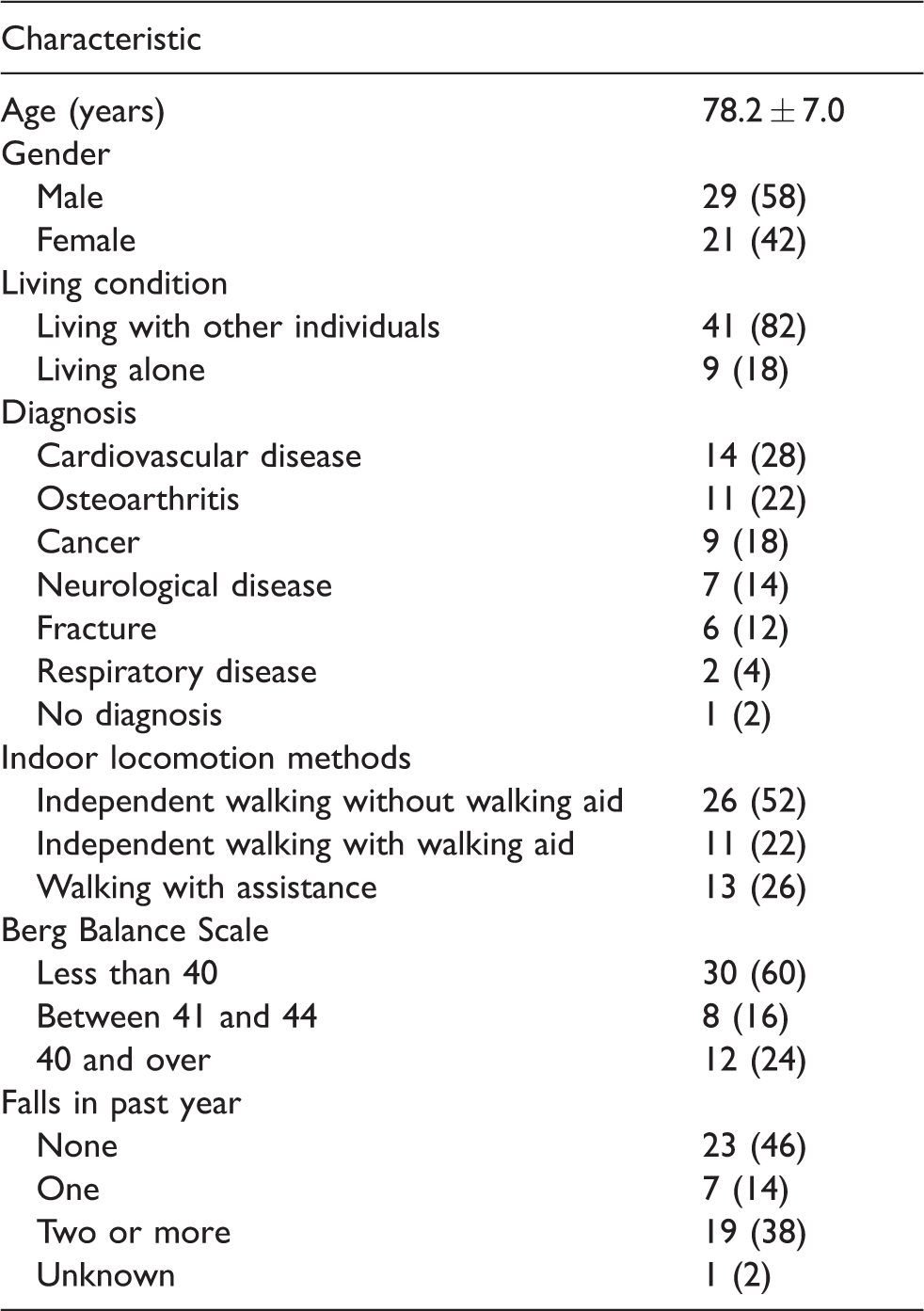
Data are presented as n (%) or mean ± standard deviation.
In the validity study, 18 OTs (seven males and 11 females) responded (a 75% response rate). The years of clinical experience of the 14 OTs (78%) ranged from 10 to 20 years, and the remaining four OTs (22%) each had more than 20 years’ experience. Eleven OTs (61%) worked in hospitals, 4 (22%) worked at a university, and 3 (17%) worked for the local government.
Hazards in the home
The most frequent hazards were identified as internal steps/stairs (n = 32; 64% identified by the therapist raters), seating (n = 32; 64%), bathroom (n = 26; 52%), bath (n = 24; 48%), external steps/stairs (n = 22; 44%), toilet location (n = 21; 42%), footwear (n = 20; 40%), internal steps/stairs handrails (n = 20; 40%), floormats (n = 18; 36%), and pathways/driveways (n = 18; 36%) (Table 2). No hazards were identified for the following five items: ironing area, internal stairs/elevator/approach, hot plates, dishwasher, and drier.
Most frequent hazards in the home identified by the raters of Japanese elderly.
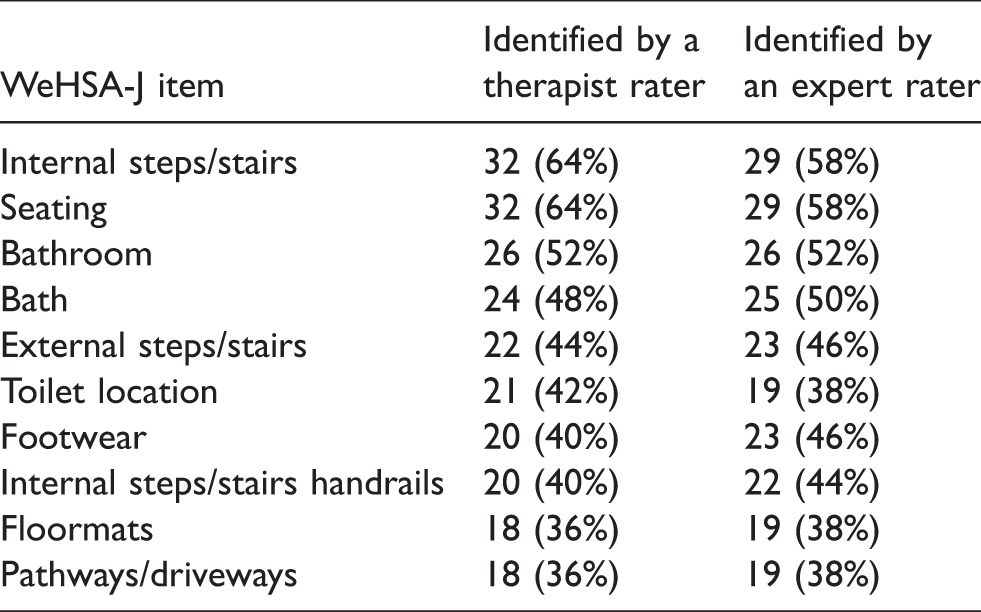
WeHSA-J: Japanese version of the Westmead Home Safety Assessment.
Reliability and validity
For the inter-rater reliability of the WeHSA-J, 48 items were rated excellent (68%; P < 0.01) and 18 were rated fair to good (25%; P < 0.01); none were rated poor. The above-mentioned five items (7%) that did not present an identified hazard could not be calculated using Cohen’s kappa (κ) coefficient.
Regarding the content validity, the I-CVIs of 50 items (70%) were rated as excellent, whereas the S-CVI was 0.78 ± 0.16, which was not rated as excellent (less than 0.90).
Forty-nine items (69%) in the WeHSA-J were rated as fair to good or excellent for inter-rater reliability as well as for excellent content validity (Table 3). The 49 items included those concerned with basic activities of daily living, such as locomotion, seating, sleeping, bathing, and going to the toilet, as well as those concerning simple instrumental activities of daily living (IADL), such as preparing a simple meal and going to a washing machine. The other items (31%) were mostly concerned with IADL, such as cleaning, telephone call, ironing, cooking, doing laundry, taking medication, and safety calls (Table 4). All these items except for ‘internal stairs/elevator/approach’ were unaccepted due to the shortage of I-CVI score.
The 49 items of the WeHSA-J with adequate inter-rater reliability and content validity.
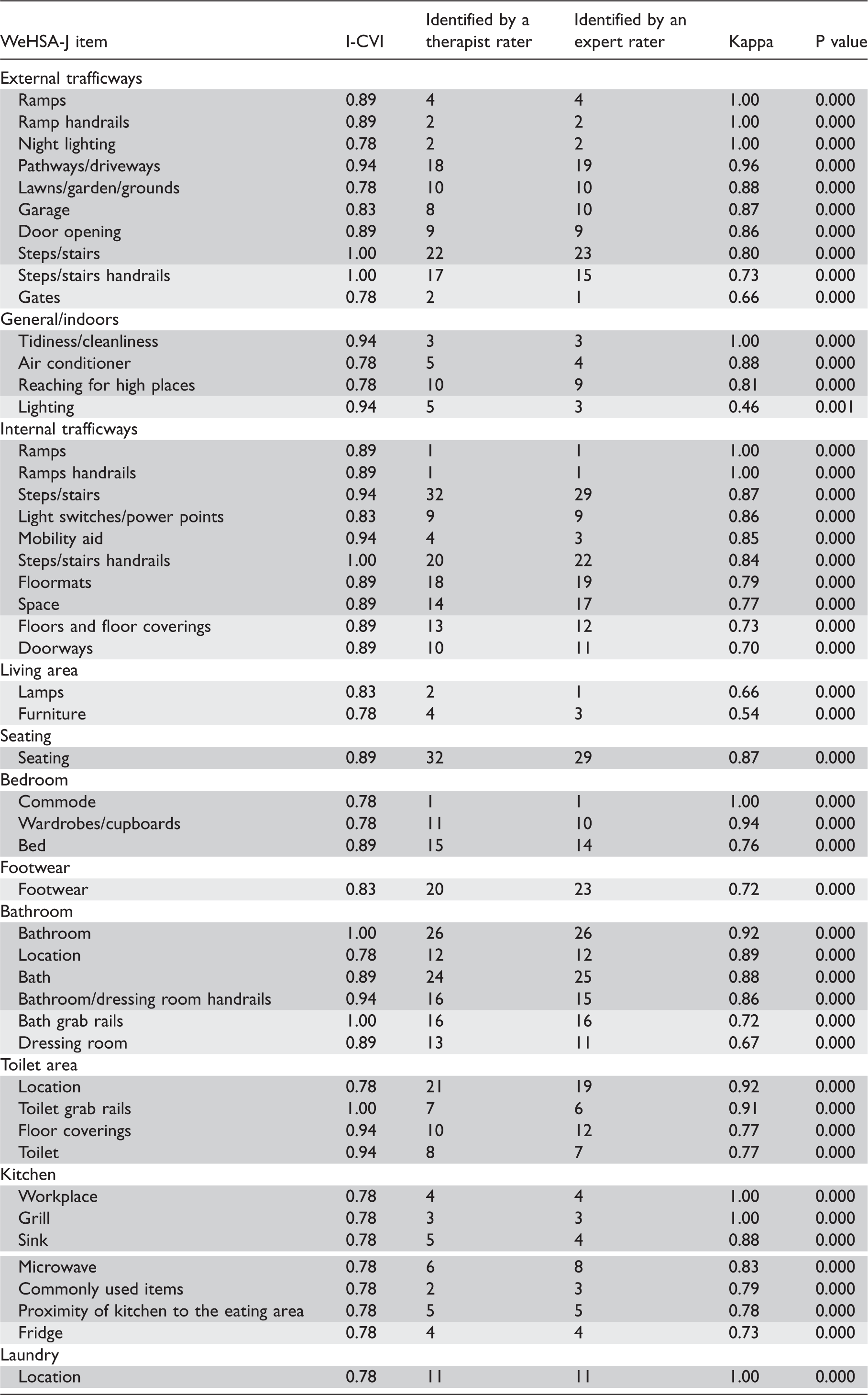
I-CVI: the item content validity index; WeHSA-J: Japanese version of the Westmead Home Safety Assessment.
 Items with excellent reliability.
Items with excellent reliability.
 Items with fair to good reliability.
Items with fair to good reliability.
The 22 items of the WeHSA-J without calculated inter-rater reliability and/or without adequate content validity.
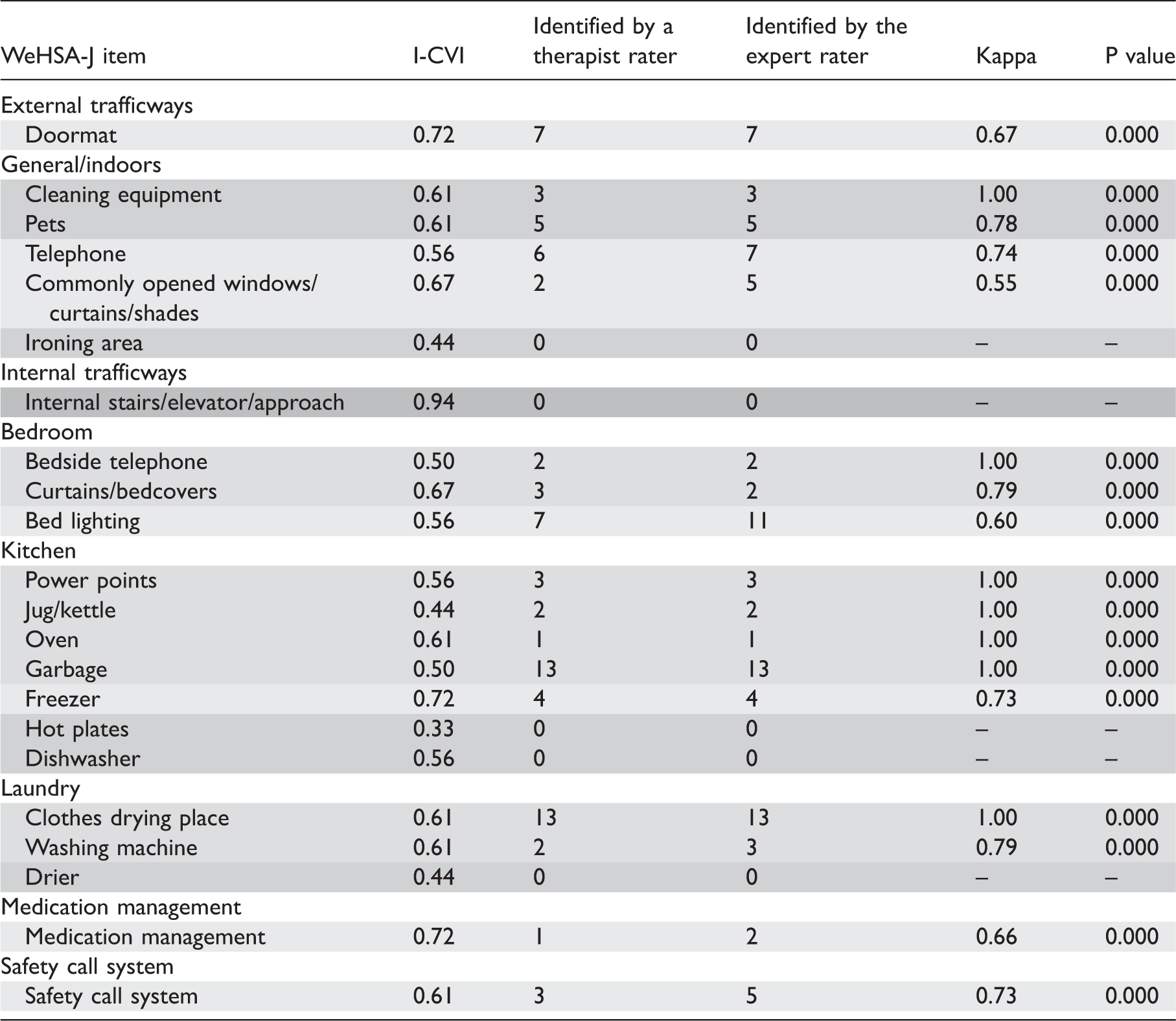
I-CVI; the item content validity index; WeHSA-J: Japanese version of the Westmead Home Safety Assessment.
Items with excellent reliability but without excellent validity.
Items with fair to good reliability but without excellent validity.
 Items without calculated reliability and without excellent validity.
Items without calculated reliability and without excellent validity.
 Items without calculated reliability but with excellent validity.
Items without calculated reliability but with excellent validity.
Discussion
The results of this study suggested that the 49 items (69%) in the WeHSA-J were reliable and relevant for identifying fall hazards in the homes of elderly Japanese. In contrast, the other items were mostly concerned with IADL and were not always applicable to all seniors.
According to a report by the Tokyo Fire Department, one of the few statistical records of accidental falls in Japanese elderly, 27,253 seniors living in Tokyo were taken by ambulance in 2015 due to falls at home. The sites of occurrence were the living room and bedroom (68%), entrance (10%), hallway and veranda (7%), toilet area and washroom (3%), kitchen (3%), stairs (2%), bathroom (2%), and garden and pond (2%), among others. The 49 items in this study broadly covered the sites of accidental elderly falls at home.
The WeHSA-J generally had adequate inter-rater reliability, similar to the original WeHSA. The number of items with excellent or fair to good reliability was as follows: 65 items (92%) in the original version (Clemson et al., 1999) and 66 (93%) in the Japanese version. There was no item with poor reliability in both versions. A possible reason for this result was that the collected data in this study, as well as in Clemson et al.’s research (1999), warranted specific training for the raters of the assessments to maximise reliability and consistency.
The results of this study also clarified some frequent fall hazards in the homes of Japanese elderly. It is generally known that Japanese houses commonly have many steps indoors and high bathtubs; both are fall hazards for seniors. However, there were few reports citing substantive evidence of these risks. To our knowledge, this study is the first to report that internal steps and bathtubs are the most frequent fall hazards specifically for Japanese seniors. According to a study of 257 Australian elderly (Clemson, Roland, & Cumming, 1997), the following items of the WeHSA were indicated as the most frequent hazards: floormats (n = 76; 30%), pets (n = 71; 28%), pathways/driveways (n = 51; 20%), bathroom floor surfaces (n = 47; 18%), toilet floor surfaces (n = 46; 18%), bathmats (n = 45; 18%), seating (n = 36; 14%), footwear (n = 32; 12%), external steps (n = 31; 12%), and lighting (n = 31; 12%). Conversely, only 13 cases (5%) of internal step/stair hazards and 11 cases (4%) of bath hazards were found by Clemson et al. (1997), whereas 29 cases (58%) and 24 cases (48%) were found, respectively, in our study.
The present study had several limitations. First, convenience samples were used, and the sample size was small. This resulted in selection bias, that is the majority of samples for the reliability study were patients who received a home visit before hospital discharge and with low BBS scores (less than 45). Further, the majority of the raters in the validity study were OT hospital employees. Thus, the evaluation items accepted in this study might be appropriate for the impaired elderly rather than the elderly in general. Second, there were factors that might influence the results of the evaluation process for both studies of validity and reliability. In the validity study, the evaluators were asked about the relevance of each evaluation item of the WeHSA-J but were not asked about its scope. Therefore, we did not investigate whether there were omissions in the evaluation items for identifying fall hazards in the homes of Japanese elderly. In the reliability study, one rater (the therapist rater) was trained by the other rater (the expert rater and second author), thereby creating the potential for bias, as the expert rater could know the results evaluated by the therapist rater. Third, the question about the participants’ one-year fall histories might create recall bias in the reliability study. In addition, since the participants’ cognitive status was not evaluated, this might increase recall bias. Considering the above-mentioned limitations, further research is needed to determine other psychometric properties such as construct validity in order to refine the evaluation items whether they are well fitted for identifying fall hazards in the homes of the elderly with risks of falls in Japan.
Conclusions
Although the framework of the WeHSA-J in its entirety was not adequate in the home safety construct for falls prevention of the Japanese elderly, the 49 items were reliable and relevant for identifying fall hazards in their homes. Further research is necessary to improve the reliability and validity of the present version of the WeHSA-J for this population.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.