
Abstract
We developed a comprehensive Diet and Lifestyle Quality Index (DLQI) and examined its associations with health status and sociodemographic characteristics in Argentinian adults. The DLQI scores range from 0 to 100 points and comprises 49 indicators across 7 dimensions: diet and eating habits, physical activity, rest and sleeping habits, exposure to sunlight and nature, religiosity, abstinence from tobacco and alcohol, and emotional well-being and relationships. Cross-sectional data from 4215 adults were analyzed to explore links with sociodemographic characteristics and chronic disease prevalence. Participants’ mean age was 35.5±14.6 years and 69% were women. The mean DLQI score was 51.5±10.6. Higher scores were associated with older age, being married, lower financial concern, rural residence, and receipt of social welfare. Elevated DLQI and dimension-specific scores were inversely related to self-reported obesity, diabetes, fatty liver, hypertension, kidney disease, and cancer, while lower scores were positively associated with overweight and obesity. Score distribution and odds ratios supported cut-off points for classifying lifestyle quality. Our evaluation indicates the DLQI is a practical tool for assessing diverse diet and lifestyle factors, with scores reflecting health status in line with existing evidence. Further evaluation in other populations is recommended to confirm its clinical and public health applicability.
“Our evaluation demonstrated that the DLQI is a practical and informative tool for assessing lifestyle quality and estimating chronic disease risk.”
Introduction
Non-communicable diseases represent one of the greatest burdens to human health worldwide, and developing countries are especially affected due to economic and sociocultural disparities.1,2 Emphasis has been placed on the risk factors for the prevention and control of these diseases such as inadequate and unhealthy diet, tobacco use, harmful alcohol consumption, and physical inactivity.3,4 In Argentina, the latest National Risk Factor Survey, a component of the National Strategy for the Prevention and Control of Non-Communicable Diseases, offers information on diet, physical activity, alcohol and tobacco consumption as behavioral risk factors for these diseases. 5
Recognizing that individual lifestyle factors do not act in isolation but contribute collectively to health outcomes, 6 a range of health behaviors began to be systematically evaluated in the mid-20th century to understand their combined effects on health outcomes such as chronic disease, mortality risk and life expectancy. 7 This led to the development of lifestyle indices, such as The Lifestyle and Well-Being Index, 8 the Mediterranean Lifestyle Index, 9 and the Lifestyle Index for iMPROVE Study, 10 among others, which are instruments designed to assess the quality and patterns of individual behaviors and lifestyle choices as a whole.11-13 Lifestyle indices are useful for combining multiple behavioral dimensions into a single score, which facilitates interpretation and comparison in epidemiological research. Unlike full questionnaires, which can be lengthy and complex, indices provide a standardized measure to efficiently assess associations with health outcomes, identify patterns of risk and guide health interventions.14,15
Lifestyle indices typically include the mentioned dimensions, such as diet, physical activity, smoking or alcohol consumption, and are used to identify at-risk populations and inform public health interventions aimed at promoting healthier lifestyles.12,16,17 However, in recent years, research has shown that these traditional risk factors for non-communicable diseases are not the only ones accounting for a comprehensive assessment of lifestyle habits. 18 Current lifestyle medicine evidences indicates that if we only consider habits that have been used in other indices, we may miss relevant information needed to explore associations, establish causality, and design interventions. 19
Other factors, such as rest and sleeping habits,20-23 exposure to sunlight and natural environments,24-27 stress management,28,29 emotional, interpersonal relationships and well-being,18,30,31 religiosity,32,33 and eating habits 34 have been shown to influence morbidity and mortality from non-communicable diseases. For instance, both insufficient and excessive sleep have been associated with an increased risk of cardiovascular disease, while poor sleep quality has been associated with a higher incidence of type 2 diabetes.35,36 Similarly, access to urban green spaces is consistently associated with reduced symptoms of depression and anxiety, supporting their role in mental well-being and stress reduction. 37 Inadequate sun exposure, a common problem in urbanized populations, contributes to vitamin D deficiency, which is associated with musculoskeletal disorders, immune dysfunction and cardiometabolic disease.38,39
Beyond these physiological mechanisms, psychosocial factors have been positively associated with better health outcomes, including lower incidence of cancer, cardiovascular disease and mental disorders, possibly through enhanced social support and stress coping mechanisms.40,41 Psychosocial factors, including disordered mood and low social support, have been associated with cardiovascular disease development and progression. 42 Studies of Blue Zones—regions of exceptional longevity—have highlighted the role of strong social connections and active participation in religious communities, as exemplified by the Seventh-day Adventist cohort from California, as key contributors to increased life expectancy and overall well-being. 43 Given their established influence on health and well-being, these dimensions go beyond traditional diet and physical activity measures to provide a more holistic and comprehensive measure of lifestyle quality. Including them in an index could provide a more nuanced understanding of protective behaviors and risk factors, supporting a more integrative approach to lifestyle-related disease prevention.
To the best of our knowledge, none of the existing health-related lifestyle indices covers all the dimensions mentioned above. Given the need to deepen the understanding of the interaction and synergy between different lifestyle factors with health outcomes, we developed a comprehensive diet and lifestyle quality index and examined if the index scores are associated with the sociodemographic and health characteristics of an Argentinian adult population.
Methods
Study Type and Population
The development of the Diet and Lifestyle Quality Index (DLQI) was carried out as part of the Adventist Health, Lifestyle, and Environmental Study in Argentina (AHLESA), a cross-sectional study that aims to determine the dietary and lifestyle factors associated with health and non-communicable diseases in Argentina. 44 Adults 18 years and older and residing for at least one year in Argentina were recruited for the study via volunteer sampling method both online and in-person from Seventh-day Adventist schools, churches, hospitals, and healthcare clinics, and social networks in every state of Argentina. Data were collected over a period of 19 months using standardized self-administered questionnaires that were completed via the study website (https://ahlesa.uap.edu.ar/) or a mobile phone application developed for the study (can be installed on one’s smart phone or laptop from https://surveyresearch.uap.edu.ar/ahlesa-web/#/).
As of December 2024, a total of 5288 had enrolled in the study. Participants who did not fully complete the questionnaires, those who currently live outside Argentina and those who reported a total energy intake outside the range of 500-6500 kcal 45 were excluded from the analysis.
Development of Comprehensive Diet and Lifestyle Quality Index
Seven lifestyle dimensions have been considered in the development of the DLQI, based on the pillars of Lifestyle Medicine and existing evidence of their impact on protecting or compromising overall health. These dimensions are: diet and eating habits, physical activity, rest and sleeping habits, exposure to sunlight and natural environments, religiosity, abstinence from alcohol and tobacco, and emotional well-being and interpersonal relationships (see Figure 1). Dimensions considered in the development of the DLQI.
Prior to developing the DLQI, we conducted an exploratory literature search in PubMed (August 2024) including publications from 2004 onwards, in addition to the search for bibliographic support for the incorporation of each relevant dimension. The aim was to identify existing indices and scores related to diet quality, lifestyle, or both, to inform the conceptual framework of our index. We used combinations of keywords such as “lifestyle index,” “diet quality index,” “healthy lifestyle score,” and “composite lifestyle measure,” without restrictions on study design or population. This search yielded 23 publications: 20 presenting lifestyle and/or diet indices and 3 reviews of lifestyle indices. We used the 20 articles (published 2004-2024) for selecting the indicators/items and determining the scoring system and cut-off points for the DLQI (see Supplemental Table 1).
The publications included (1) indices predictive of disease or mortality, (2) indices designed for populations with specific health conditions, and (3) general indices and indices assessing adherence to specific dietary patterns. The full list of articles, along with the items considered and modified for the DLQI, is presented in Supplemental Table 2.
The lifestyle dimensions in the DLQI were measured through 49 indicators/items that were adapted from existing validated instruments that assess the lifestyle factors separately. During the selection of relevant indicators/items from the existing validated instruments, we consulted several systematic reviews on lifestyle factors affecting health,22,26,32,33,37,38 and guidelines/recommendations from the World Health Organization 46 and governmental agencies47,48 for the prevention of non-communicable diseases. A detailed breakdown of each lifestyle dimension, including the component indicators, their corresponding scores, and the references on which they are based, is provided in Supplemental Table 1. The final list of items to include in the DLQI from the existing validated instruments were determined after a review of consulted experts consisting of experts in the areas of nutrition/nutritional epidemiology (4), physiology (2) and psychology (1).
The dimension on diet, which included scores on adequacy, moderation, variety, and overall balance, was evaluated using a validated food frequency questionnaire (FFQ). 49 The eating habits part of this dimension was measured by adding items about meal times, number of meals per day, snacking, eating breakfast every day, and continuing to eat even when being full. From the responses to the FFQ, the average daily consumption of each food group (servings), their percentage contribution to the total daily intake and their diversity were also obtained. In addition, the total daily intake of nutrients, and the diversity of specific nutrient sources were calculated. The structure of this part of the questionnaire, as well as many of its scores, were based on the Diet Quality Index-International. 50 The scoring of the “overall balance” section was based on an adaptation of the Harvard University Healthy Eating Plate by Loma Linda University. 51
The physical activity dimension was measured in metabolic equivalents (METs) 52 and evaluated by the Global Physical Activity Questionnaire (GPAQ). 53 Rest and sleeping habits were assessed using the Pittsburgh Sleep Quality Index (PSQI) 54 along with questions about weekly break, annual rest and screen use during free time. To assess exposure to sunlight and natural environments, participants were asked about frequency per week and times of the day in which they spend time outdoors and under the sun. The religiosity dimension was measured using The Duke University Religion Index (DUREL), 55 which included scores on organizational and non-organizational activities, and subjective components. Abstinence from alcohol and tobacco was determined by the Global Adult Tobacco Survey (GATS) 56 and the Alcohol Use Disorders Identification Test (AUDIT). 57 Emotional well-being and interpersonal relationships dimension included indicators on stress management, forgiveness, gratitude, purpose in life, and interpersonal relationships, measured with items of The Flourishing Scale (FS), 58 The Purpose In Life Test (PIL Test), 59 The Short Form of the Perceived Stress Scale (PSS-4) 60 and, The Gratitude Questionnaire-Six-Item Form (GQ-6). 61
DLQI total scores ranged from 0 to 100 points (diet and eating habits: 36 p.; physical activity: 14 p.; rest and sleeping habits: 10 p.; exposure to sunlight and natural environments: 10 p.; religiosity: 10 p.; abstinence from alcohol and tobacco: 10 p.; emotional health and interpersonal relationships: 10 p.). The scoring system, including the proportion of points assigned to each dimension, was developed iteratively by the research team through review of the scientific literature and comparison with existing dietary and lifestyle indices.62-67 Point allocations were guided by evidence on the associations of each component with non-communicable diseases and their relevance for promoting healthy lifestyles. However, no formal statistical weighting or standardized scoring protocol was applied. For dimensions and indicators/items that were not found to be part of existing lifestyle indices, or whose influence on health and development of chronic diseases was not compared with other habits in the literature, equivalent scores were assigned. See Supplemental Table 2 for details.
Sociodemographic and Health-Related Variables
In addition to the information provided for the calculation of the DLQI, participants also reported sociodemographic characteristics such as gender, age (then categorized as young: 18 to 26 years; young adult: 27 to 39 years; adults: 40 to 59; and older: 60 years and older), educational level (less than elementary, elementary complete, high school complete, and higher education complete), marital status (single, married or cohabiting, separated or divorced, and widowed), main activity (unemployed, student, worker ≤40 hours, worker >40 hours, homemaker or retired), province of residence, access to social welfare and living environment (rural or urban). Items about health status included self-reported diagnosis of chronic non-communicable diseases (obesity, diabetes, arterial hypertension, cancer, fatty liver and chronic kidney disease), and self-reported weight and height measurements. For statistical analysis, people were considered obese if they reported a medical diagnosis of obesity or if their BMI was 30 kg/m2 or higher.
Level of financial concern was rated high or low based on participants’ response to how often they worry about being able to cover their regular living expenses for the month and then was categorized as low (0 to 5 points of worry) and high (6 to 10 points of worry). Province of residence was categorized into the 6 regions of the country (Central, Metropolitan area of Buenos Aires, Northeastern, Northwestern, Southern, and Western). Body mass index (BMI) was calculated as weight (kg)/height-squared (m2). Nutritional status was categorized according to BMI as underweight (<18.5), normal weight (18.5 - 24.9), overweight (25.0 - 29.9) and obese (≥30.0). 68
Statistical Analysis
The total DLQI score for each of the component dimensions were calculated for each participant. Descriptives (means and standard deviations, frequency counts and percentages) were computed for all participants. Comparisons between gender groups (men vs women) on sociodemographic characteristics utilized chi-squared tests for categorical and independent samples t-test for continuous variables. Independent samples t-test or ANOVA were used to compare total DLQI and each component dimension scores across groups stratified by sociodemographic characteristics.
Cronbach’s alpha was calculated to determine internal consistency reliability for the DLQI. To assess the construct validity of the DLQI, independent samples t-tests were used to compare total DLQI and each of its dimensions according to self-reported chronic disease diagnosis (yes/no). Additionally, separate multivariable logistic regression models were fitted to evaluate the association between the total DLQI score and each of its dimensions with chronic disease status (yes/no), adjusting for sex, age, educational level, marital status, level of financial concern, and living environment.
To determine potential cut-off scores to identify low, moderate, and high adherence to healthy dietary and lifestyle habits, the DLQI total score was divided into tertiles (tertile 1: 46.5 points, tertile 2: 56 points). Cut-off values were later adjusted to facilitate interpretability of DLQI scores by individuals: 40 as cut-off point between low and moderate adherence, and 60 as cut-off point between moderate and high adherence. Thus, the category recommendations were: 0-40 points: low diet and lifestyle quality; >40-60 points: moderate diet and lifestyle quality; >60 points: high diet and lifestyle quality. Chi-squared tests were used to assess statistical differences between DLQI score categories and the status of chronic disease diagnosis. Finally, multivariable logistic regression models were used to estimate the odds ratios (OR) and 95% confidence intervals (CI) of each disease according to DLQI score categories.
Results
Distribution of Main Bio-Socio-Cultural Characteristics of Study Participants by Gender.
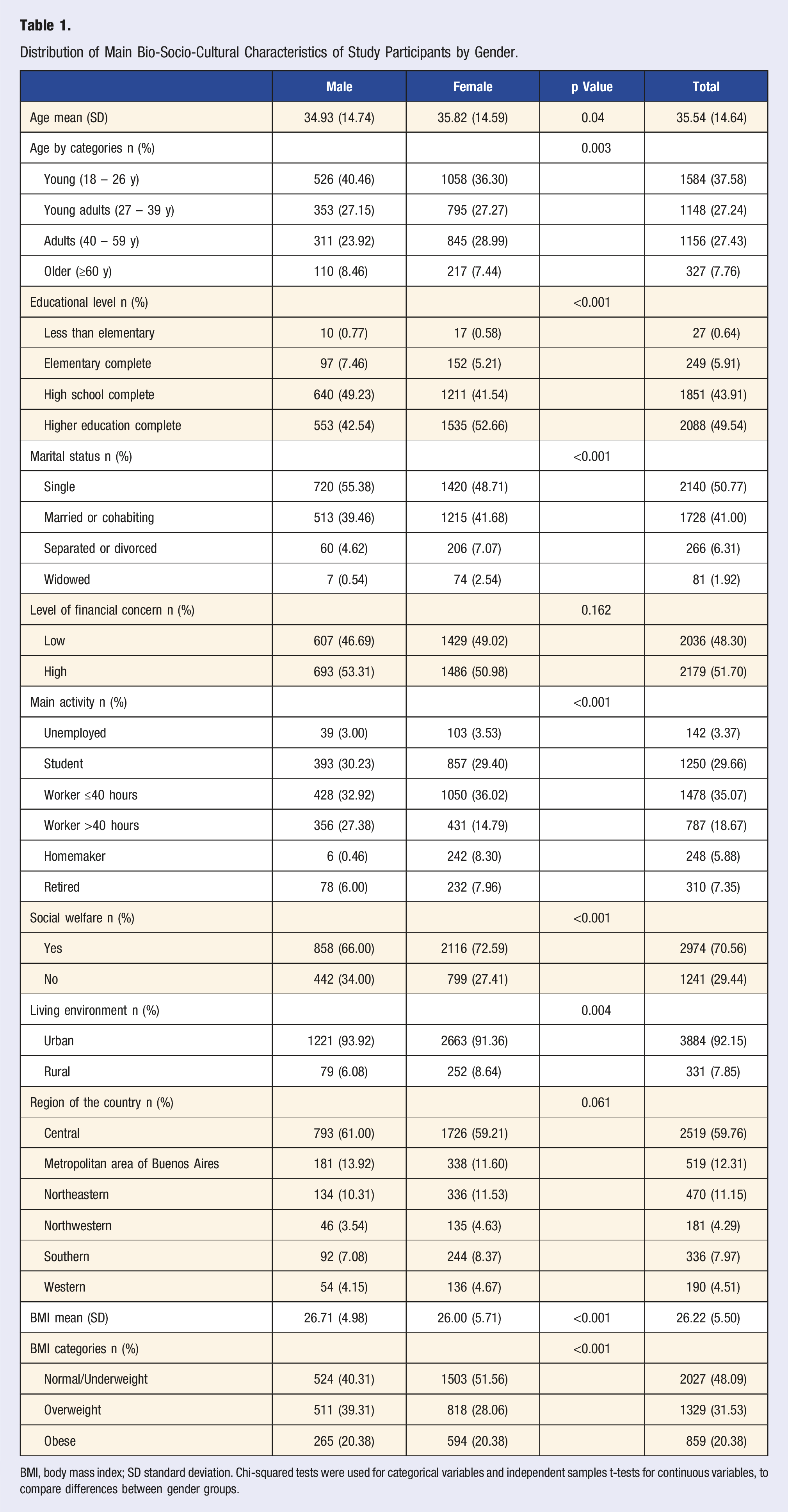
BMI, body mass index; SD standard deviation. Chi-squared tests were used for categorical variables and independent samples t-tests for continuous variables, to compare differences between gender groups.
DLQI and its Component Dimensions and Sociodemographic Characteristics
Mean and Standard Deviation of Lifestyle Index Scores According to Sociodemographic Characteristics.
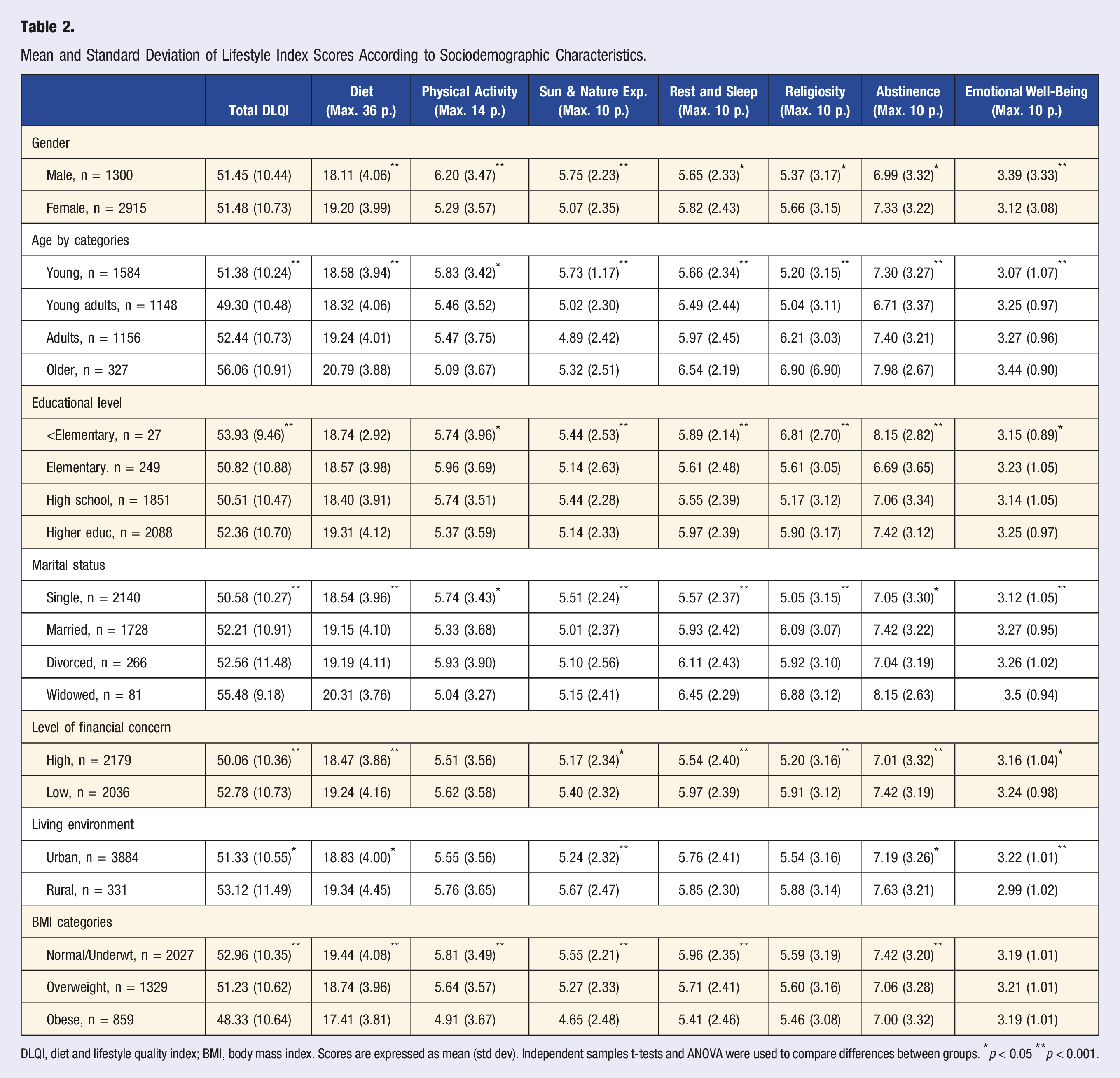
DLQI, diet and lifestyle quality index; BMI, body mass index. Scores are expressed as mean (std dev). Independent samples t-tests and ANOVA were used to compare differences between groups. *p < 0.05 **p < 0.001.
Significant differences (p < 0.05) in the total DLQI score were observed for age, educational level, marital status, level of financial concern, living environment and nutritional status. Older adults and widows had higher scores on the total DLQI, reflecting greater adherence to a healthy lifestyle. In contrast, those with lower educational attainment and with obesity had lower scores on the total DLQI. Men scored best for physical activity and exposure to sunlight and natural environments. Older people scored highest for diet and eating habits, rest and sleeping habits and religiosity. Widowed people scored highest on emotional well-being and interpersonal relationships while those living in rural areas scored lowest. People with the highest BMI scored lowest on diet and eating habits, physical activity, exposure to sunlight and natural environments and rest and sleeping habits. Scores on abstinence from tobacco and alcohol was lowest for those who completed elementary education and highest for those who had lower than elementary education.
Internal Consistency of DLQI
Assessment of internal consistency showed that the DLQI (49 items) had a Cronbach’s alpha of 0.73, with item-deleted alpha values ranging from 0.70 to 0.76. As no single item substantially increased the overall alpha when removed, all 49 items were retained in the final instrument. (See Supplemental Table 3).
DLQI and its Component Dimensions and Self-Reported Health Status
Distribution of Diet and Lifestyle Quality Index DLQI) Scores According to Self-Reported Disease Diagnosis.

Scores are expressed as mean (std dev). Independent samples t-tests were used to compare differences between groups. *p < 0.05 **p < 0.001.
Total DLQI score and for each dimension were also assessed for possible association with self-reported disease diagnosis. High scores for total DLQI, diet and eating habits, physical activity, exposure to sunlight and natural environments, rest and sleep habits, religiosity and abstinence from alcohol and tobacco showed lower odds of presenting obesity or diabetes. The odds of arterial hypertension decreased with higher scores for total DLQI, diet and eating habits and abstinence from tobacco and alcohol. The odds of cancer decreased with higher scores for abstinence from tobacco and alcohol, and odds of chronic kidney disease decreased with higher scores for religiosity. The odds of fatty liver decreased with higher scores for total DLQI, diet and eating habits, physical activity, exposure to sunlight and natural environments, and rest and sleeping habits (Figure 2). Dimensions of DLQI and Odds of Disease. Odds ratio values and their confidence intervals are estimated for the presence of obesity, diabetes, arterial hypertension, cancer, chronic kidney disease and fatty liver, in relation to the total DLQI score and score on each of the dimensions of the DLQI, adjusted for sex, age, educational level, marital status, level of financial concern and living environment. P values are also shown.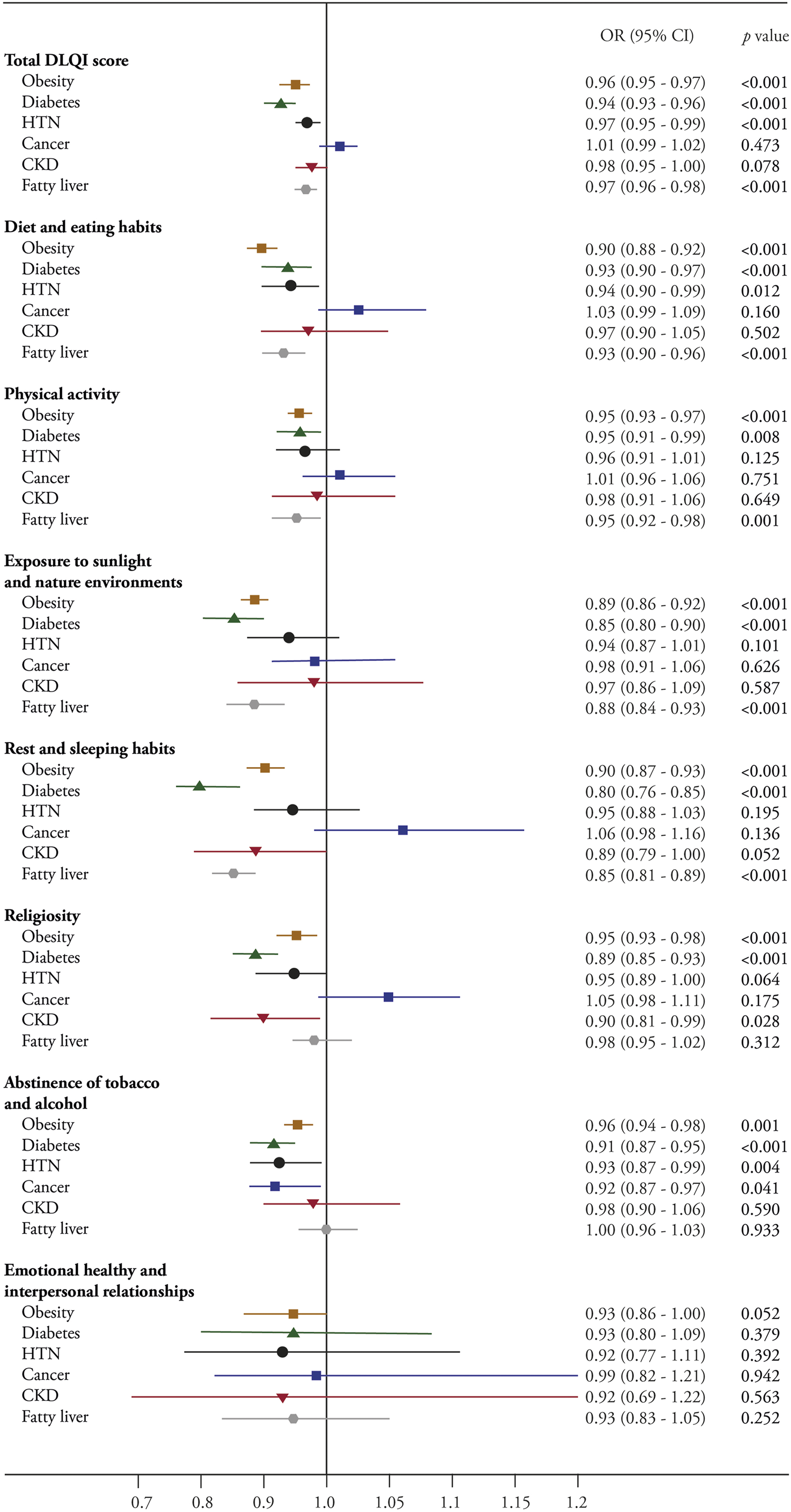
Distribution of the Sample According to Scoring Categories.
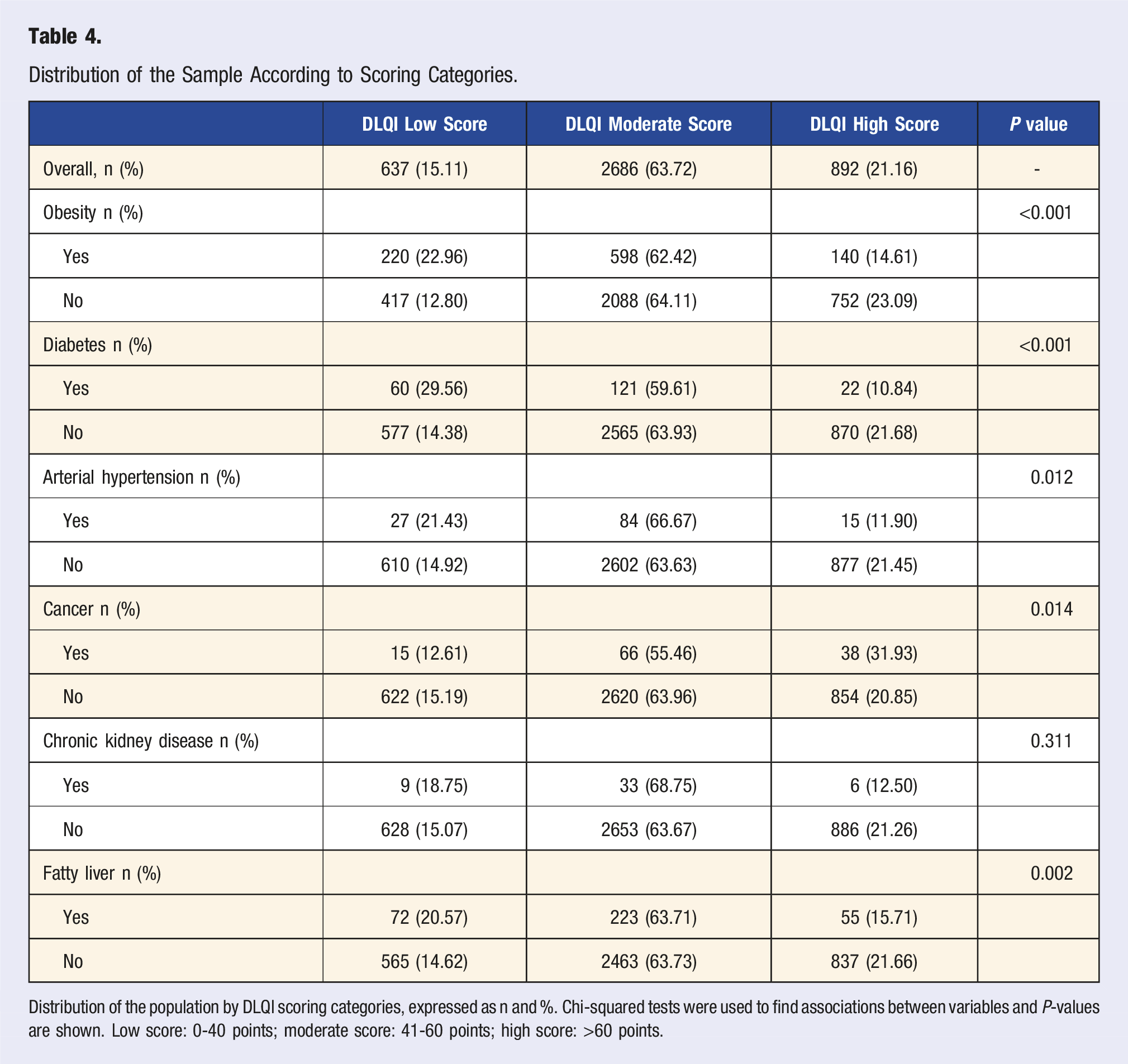
Distribution of the population by DLQI scoring categories, expressed as n and %. Chi-squared tests were used to find associations between variables and P-values are shown. Low score: 0-40 points; moderate score: 41-60 points; high score: >60 points.
Disease modeling based on DLQI categories indicated that moderate and high DLQI scores were associated with lower odds of obesity and diabetes across all groups. Compared with the low DLQI category, being in the moderate or high DLQI category was significantly associated with lower odds of hypertension in women and in the overall population. High DLQI scores were also associated with lower odds of chronic kidney disease while moderate and high scores were associated with reduced odds for fatty liver disease across all groups. Figure 3 shows the odds ratios (ORs) and 95% confidence intervals (CIs) for each DLQI category (moderate and high relative to low) in relation to the presence of each disease. DLQI Scores and Odds of Disease. Odds ratio values and their confidence intervals are estimated for categories of DLQI score on the presence of obesity, type 2 diabetes, arterial hypertension (HTN), cancer, chronic kidney disease (CKD), and fatty liver for all participants (A), men (M), and women (W). Low DLQI score was taken as the reference category, adjusted for sex, age, educational level, marital status, level of financial concern, and living environment.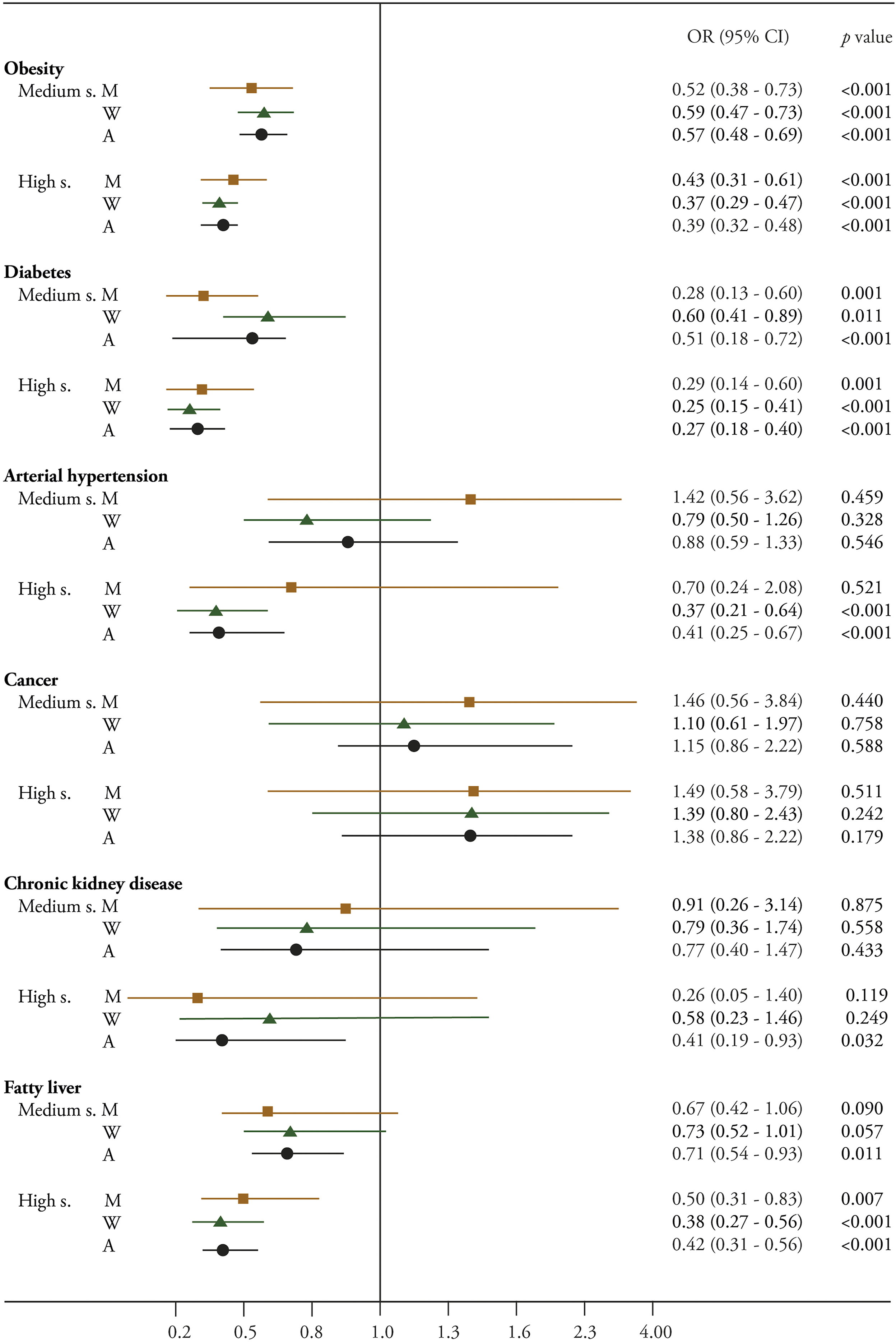
Discussion
The DLQI was developed based on robust evidence linking lifestyle habits to health and disease outcomes, and it encompasses dimensions that comprehensively address dietary and lifestyle factors known to influence health. Despite adapting items from existing validated instruments for use in the DLQI, our assessment confirmed the reliability of the resulting instrument, as demonstrated by acceptable internal consistency. In addition, DLQI scores demonstrated the ability to discriminate between individuals with self-reported medical condition—obesity, diabetes, hypertension, cancer, chronic kidney disease, and fatty liver—and those without any reported disease, thereby providing evidence of construct validity.
Our evaluation demonstrated that the DLQI is a practical and informative tool for assessing lifestyle quality and estimating chronic disease risk. The use of structured cut-off points enabled the classification of diet and lifestyle quality adherence to low, moderate, and high levels which can potentially offer meaningful guidance or actionable information for individuals and enhance its utility in epidemiological research. Potentially, this tool can be used for self-assessment to determine adherence to healthy lifestyle practices, aid in goal setting to improve current behaviors or act as a motivational tool for setting lifestyle goals. In the right context, health professionals may use the index for personalized advice. More importantly, researchers can utilize the DLQI to further determine the synergy among the dietary and lifestyle practices and their associations with health and disease outcomes and facilitate more targeted interventions for a study population.
The DLQI includes comprehensive dietary and lifestyle indicators, and covers dimensions not included in most other indices in Argentina and worldwide. While there is well-established data that diet and physical activity contribute to the development of chronic diseases such as obesity,69,70 related metabolic conditions, and cancer, 62 evidence for the other factors is still emerging.
Considered as one of the most comprehensive indices, the Lifestyle and Well-Being Index 8 includes the dimensions of adiposity, smoking, family history of disease, dietary data, physical activity and insomnia. However, only 4 of these dimensions can be considered lifestyle, while 2 relate to personal or family health. The Mediterranean Lifestyle Index (MEDLIFE) integrates food consumption patterns, traditional Mediterranean habits, physical activity, rest and social interaction in the index, 9 while the Lifestyle Index and Work Ability focuses on non-smoking, maintaining a healthy weight, daily fiber intake and regular physical activity. 71 Similarly, a China-US healthy lifestyle comparison index assessed diet quality, physical activity, smoking and alcohol consumption. 67
Most existing indices were designed to estimate the risk of mortality, life expectancy,16,66,72 or the likelihood of developing diseases such as cancer, 12 obesity62,73 or cardiovascular disease. 64 Some, although not predictive, have been used in specific health situations.10,13,71,74 In contrast, the DLQI was designed to focus on those factors described in the literature as protective against non-communicable diseases. Our paradigm has been shaped by the health principles espoused by Seventh-day Adventists, and can be represented by the acronym NEWSTART—Nutrition-Exercise-Water-Sunshine-Temperance-Air-Rest-Trust in God. 75 These principles are not only similar but confirmed by the 6 interconnected pillars that the American College of Lifestyle Medicine considers as the basis for the treatment, reversal, and prevention of chronic diseases: Optimal Nutrition-Physical Activity-Stress Management-Restorative Sleep-Connectedness-Risky Substance Avoidance (https://lifestylemedicine.org/about-lifestyle-medicine/).
A systematic review highlighted the importance of green spaces in preventing lifestyle diseases such as depression, diabetes, and obesity. 26 Sun exposure is crucial for the production of vitamin D and its metabolic pathways, which are essential for mental health, osteomyoarticular integrity, immunity and prevention of non-communicable diseases.27,76,77 For their part, the Duke University Religion Index 55 has been largely used in different health studies worldwide. High scores on this scale are usually associated with faster-time disease recovery, lower rates of depression, and slower progression of disability, among other positive health outcomes. 78
Our results showed significant associations between sociodemographic characteristics and DQLI dimensions. Men had higher scores for physical activity, exposure to sunlight and natural environments and emotional well-being and interpersonal relationships than women. This aligns with the observation that men have higher physical activity while women have higher perceived stress due to multifactorial responsibilities. 79 On the other hand, women scored higher on diet and eating habits, rest and sleeping habits, religiosity and abstinence from alcohol and tobacco. This is consistent with previous studies reporting that women placed a higher priority on diet quality,80,81 religiosity 82 and overall health care than men. 83
Age was also an important factor strongly associated with lifestyle scores. Younger people reported better physical activity level and exposure to sun and natural environments, whereas older adults had higher averages on total DLQI score, and particularly in diet and eating habits, rest and sleeping habits, religiosity, abstinence from alcohol and tobacco, and emotional well-being and interpersonal relationships. These results are in line with existing evidence on health behavior trends across age groups, with older adults often adopting healthier lifestyles, including religiosity. 84
Financial worries were associated with lower lifestyle scores, particularly in the dimensions of diet and eating habits, exposure to sunlight and natural environments, religiosity, abstinence from alcohol and tobacco and emotional well-being and interpersonal relationships. These are consistent with other research which points to mental stress for financial insecurity as a barrier to healthy lifestyle choices. 85 Urbanization also played a role. Those living in urban areas had lower scores on total DLQI, diet and eating habits, exposure to sunlight and natural environments, abstinence of tobacco and alcohol and emotional well-being and interpersonal relationships, consistent with studies showing the negative effects of urban environments on stress and lifestyle behaviors. 86 These findings highlight the importance of tailoring health promotion interventions to the sociodemographic characteristics of the population.
The results of this cross-sectional study indicate that obesity, diabetes, arterial hypertension, chronic kidney disease and fatty liver are associated with lower lifestyle total scores on the DLQI, as well as several of its dimensions, consistent with previous research.29,87 Individuals with metabolically unhealthy phenotypes were more likely to report less favorable dietary and physical activity habits, which are known risk factors for poorer metabolic and cardiovascular outcomes.88-90 While causality cannot be inferred, existing evidence suggests that adopting a balanced diet and engaging in regular physical activity are key strategies for improving metabolic health and may support transitions toward healthier phenotypes. 91 These findings highlight the critical role of lifestyle factors in the context of chronic disease prevention and management, and suggest that the DLQI could be useful for identifying individual lifestyle domains in need of improvement.
Our findings are consistent with previous research showing that abstinence from tobacco and alcohol is associated with lower likelihood of cancer (see Figure 2). However, no protective association was observed between the total DLQI score and self-reported cancer diagnosis. This may reflect “reverse causation” as it is well documented that individuals diagnosed with cancer often adopt healthier lifestyle behaviors after diagnosis. Motivated by increased health awareness and a desire to improve treatment outcomes and overall well-being. Studies have further shown that cancer survivors who adopt healthier lifestyles experience lower mortality rates and improved health-related quality of life. 92
Interestingly, higher religiosity scores were associated with a lower likelihood of diabetes and chronic kidney disease in our study. This association may be partly explained by healthier behaviors often positively associated with religiosity, such as reduced tobacco and alcohol use, healthier dietary choices, and stronger social support networks, all of which contribute to reduce disease risk. 93 For example, one study reported that spirituality was inversely associated with obesity and chronic disease risk among African-American adolescents, suggesting a potential protective factor in weight control. 94 Other evidence indicates that religious practices, such as prayer and reading sacred texts, may support diabetes management by enhancing adherence to treatment and psychological well-being. 95 However, the relationship between religiosity and health varies across contexts. For instance, among Indian immigrants, certain religious practices were associated with higher body mass index, underscoring the cultural and behavioral complexity of this relationship. 96 Overall, our findings emphasize the importance of considering religiosity and spirituality in public health research and interventions aimed at preventing and managing diabetes, obesity and other chronic conditions.
Our study sample showed the following prevalence rates: obesity (22.7%), diabetes (4.8%), arterial hypertension (3.0%), cancer (2.8%), chronic kidney disease (1.1%), and fatty liver disease (8.3%). Compared to national-level data, our sample appears to be healthier in several respects. For instance, last national data indicate that approximately 32.4% of Argentine adults are obese, and of those who have ever had their blood pressure measured, 34.7% reported that a health professional told them they had high blood pressure. 5 Regarding diabetes, the International Diabetes Federation estimates a prevalence of around 14% among Argentine adults. 97 These comparisons suggest that our study may underrepresent the true burden of several chronic conditions in Argentina. This discrepancy should be taken into account when generalizing our findings and underscores the potential influence of selection bias or sampling characteristics, such as recruitment methods, sociodemographic composition, or health awareness of participants.
Strengths and Limitations
This study has several notable strengths. To our knowledge, the DLQI is currently the most comprehensive multidimensional lifestyle assessment tool that captures both dietary and non-dietary lifestyle factors simultaneously, allowing for a more integrative perspective. A key strength of the DLQI is the inclusion of lifestyle dimensions that, despite their collective influence on overall health, are often overlooked in similar indexes. In addition, the index allows for the establishment of absolute cut-off points to classify individuals into 3 levels of healthy lifestyle adherence. This classification not only facilitates participant feedback in research, but also serves as a practical tool for raising awareness of chronic disease prevention. The relatively large study sample enhances the generalizability of the findings to our sample population, while the consistency of our findings with existing evidence supports the construct validity of the DLQI. By highlighting both its utility at the population level and its potential for individual lifestyle assessment, this study adds novel evidence to the growing literature on comprehensive lifestyle indices.
This study has several limitations that should be acknowledged. Although items in the DLQI were adapted from previously validated instruments, reliance on self-reported data for both lifestyle behaviors and disease diagnoses may have introduced recall bias or misclassification. In the case of our population which included students and health-oriented populations 98 such as health professionals, the self-report may have led to over- or underestimation. 99 Although we covered every state of Argentina, our study sample did not proportionally represent the Argentinian demographic since our participants were mostly from Seventh-day Adventist schools, churches, hospitals, and healthcare clinics. This limits the generalizability of our findings. Finally, although our assessment indicates that the DLQI is useful for classifying diet and lifestyle quality and may help distinguish individuals based on health status, its sensitivity and specificity for accurately identifying those at risk of chronic disease or differentiating between risk categories may be limited, especially in clinical and general population settings. 100 Despite these limitations, the DLQI remains a valuable tool that offers a practical and accessible resource for researchers in epidemiology and public health.
More research is needed to examine the applicability of the DLQI in other populations and settings, to establish its utility for assessing diet and lifestyle quality, and to investigate the combined effects of dietary and lifestyle factors on health and disease outcomes. Future studies should also explore the use of DLQI in relation to additional health indicators, including inflammatory markers, metabolic profiles and gut microbiota composition. Such research would provide a deeper understanding of the links between lifestyle, well-being and overall health.
Conclusions
The DLQI, a comprehensive dietary and lifestyle tool composed of 49 indicators grouped into 7 dimensions, can be a useful tool for assessing dietary and lifestyle behaviors associated with reduced chronic disease risk. The dimensions unique to the DLQI—religiosity and exposure to sunlight and nature—extend the usefulness of this index to a more inclusive lifestyle assessment. By capturing the multidimensional nature of healthy behaviors, the DLQI is potentially informative for identifying areas for lifestyle improvement. Future research should expand its use across diverse populations and settings to validate its utility and predictive capacity.
Supplemental Material
Supplemental Material - Development and Assessment of a Comprehensive Diet and Lifestyle Quality Index in an Argentinian Adult Population
Supplemental Material for Development and Assessment of a Comprehensive Diet and Lifestyle Quality Index in an Argentinian Adult Population by Belén Carlino, Camila Niclis, Sara Leeson, Rocio Victoria Gili, Ismael Alejandro Contreras-Guillén, Laura Rosana Aballay, Martín Leonardo Mayta, Marcia Cristina Teixeira Martins, Fabio Juliano Pacheco, and Gina Segovia-Siapco, Sandaly Oliveira da Silva Pacheco in American Journal of Lifestyle Medicine
Footnotes
Acknowledgments
Appreciation is expressed to the subjects who participated in this study.
Author Contributions
SOSP, FJP, GS-S and BC participated in the design of the study. IAC-G participated in the programming and development of the tool for data collection. SL, RVG, IAC-G, SOSP, FJP and BC participated in development of the tool and in data collection. SOSP, CN, LRA, FJP, GS-S and BC analyzed and interpreted the data and drafted the manuscript. BC, GS-S, SOSP, FJP, CN, LA, MLM and MCTM provided critical comments and worked in manuscript preparation. All authors reviewed the content of the manuscript and approved the final version.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was partially funded by a research grant from the Adventist University of River Plate, Argentina, and by the Grants for Research and School Partnership International (GRASP-Intl. resolution ##2190339) from Loma Linda University Health, USA. Belén Carlino is funded on a doctoral scholarship by the National Scientific and Technical Council (CONICET), Argentina, RESOL-2021-154-APN-DIR#CONICET.
Ethical Considerations
The study was evaluated and approved by the Ethics Committee of the Adventist University of River Plate School of Medicine (resolution #1.5/2020). Participants were enrolled in this study by invitation and electronic informed consent, and all procedures were conducted following the international ethical standards proposed by the Declaration of Helsinki.
ORCID iDs
Data Availability Statement
The authors may consider the availability of data upon request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.