
Abstract
Group-based lifestyle medicine programs present a promising path to preventing and managing chronic diseases and supporting patient wellbeing. Establishing effective implementation strategies can enhance the scalability of comprehensive lifestyle medicine programs in practice. This convergent mixed methods study aimed to investigate the role of the program deliverer in the feasibility and effectiveness of a group-based program: PAVING the Path to Wellness. Semi-structured qualitative interviews were used to explore differences in perceived feasibility between physician and non-physician practitioners (e.g., allied health professionals) trained to deliver the program. Mixed linear models assessed differences in program effectiveness by type of healthcare practitioner (physician and non-physician practitioner) using the Lifestyle Medicine Health Behavior scale as a pre-/post-measure of self-reported health behaviors (nutrition, physical activity, sleep, social connection, stress, and avoidance of risky substances). Qualitative results supported that the PAVING program was feasible to implement, but that overall feasibility was greatly influenced by billing capabilities and practitioner experience. Quantitative results revealed that the program’s impact differed significantly based on the type of healthcare practitioner; participants in non-physician-led groups saw more improvement in health behaviors following the program. Data integration revealed that training and experience in lifestyle medicine and administrative infrastructure (e.g., billing, recruitment) are crucial to program effectiveness. This study has important implications for practice, including the need to scale practice-based training, promote policies for reimbursing preventive care, and build the administrative infrastructure required to support lifestyle medicine group visits.
Keywords
Introduction
Lifestyle medicine, a medical specialty that uses evidence-based behavioral intervention to prevent and manage chronic disease, addresses the modifiable risk factors for some of the world’s most prevalent chronic diseases including diabetes, cardiovascular disease, and cerebrovascular disease.1,2 The six pillars of lifestyle medicine—nutrition, physical activity, sleep, social connection, stress management, and avoidance of risky substances—have been shown to profoundly impact the risk and severity of disease and the promotion of optimal health.2-4 Despite decades of research supporting the value of lifestyle-based interventions, lifestyle medicine has yet to be adopted as a primary approach to prevent and treat chronic disease.5,6 The widespread adoption and scalability of lifestyle medicine programs depend, in part, on an improved understanding of how to effectively implement and scale lifestyle interventions in practice.1,7
Within the broad spectrum of implementation strategies for chronic disease prevention interventions, group-based lifestyle medicine programs through structured group visits stand out as particularly promising. These programs improve quality of care and health outcomes,8-10 foster psychological and social support, increase engagement, and promote self-management skills.11-13 By fostering peer support and connecting individuals with similar lived experiences, group visits provide a feasible (i.e., practitioners can reach more individuals in less time) and acceptable approach to health promotion.14-16 Despite evidence of the value of group-based programs and group medical visits specifically, it is not yet well understood what implementation strategies enhance the effectiveness of these lifestyle interventions in practice.11,17
Implementation strategies are defined as the methods used to support the integration of evidence-based health interventions into practice.18-20 A better understanding of effective implementation strategies can enhance the scalability of comprehensive lifestyle medicine programs in practice.7,15,21 One key implementation strategy for group-based lifestyle medicine programs is the education and training of program deliverers.20,22 Within dissemination and implementation (D&I) research, a field that focuses on translating research into real-world practice, program deliverers have been identified as critical to health promotion program implementation.23,24 Successful implementation relies on program deliverers who are champions for the intervention, as these individuals are willing to overcome barriers to implementation and disseminate the intervention.20,23,25 Identifying and training champions is a key step in the scaling of health interventions such as group visits. 20 The present study investigates the role of the program deliverer in the feasibility and preliminary effectiveness of the PAVING the Path to Wellness program.
PAVING the Path to Wellness, referred to as the PAVING program, is a promising lifestyle medicine group visit model that has been used in clinical and community settings across the United States and internationally (i.e., Canada, Brazil, Singapore, Greece). 26 The PAVING program has been used as a general chronic disease prevention program, as well as with specific patient populations, such as those experiencing stroke rehabilitation, breast cancer, multiple sclerosis, and perimenopause. Across heterogenous populations, the program has demonstrated high rates of participant and practitioner satisfaction.27-30 In our recent study assessing the preliminary effectiveness of the PAVING program across 19 cohorts in the United States, the program led to significant changes in self-reported participant health behaviors (nutrition, physical activity, sleep, social connection, and substance use), as well as overall lifestyle. 30 These results align with existing literature supporting the program’s preliminary effectiveness in improving patient health and wellbeing.27-29,31 In addition to assessing participant outcomes, our pilot type 1 hybrid effectiveness-implementation study qualitatively investigated implementation outcomes (i.e., acceptability, adoption, feasibility, sustainability) and key contextual factors influencing implementation (i.e., innovation design, setting). 30 The study found that the program was highly acceptable across patients and healthcare practitioners. Despite high program adoption and engagement, potential barriers to program feasibility and sustainability were identified. Barriers to feasibility included time constraints and reimbursement challenges. This work, guided by Proctor’s Implementation Outcomes Framework (IOF) and the Consolidated Framework for Implementation Research (CFIR), 32 focused broadly on implementation outcomes and context. The present mixed methods study expands this work to further investigate the feasibility and effectiveness of a specific implementation strategy: type of healthcare practitioner delivering the PAVING program. Elucidating best practices and implementation strategies for the PAVING program and other group-based lifestyle medicine programs can promote scalability in practice.
To help fill this gap, this study will assess the role of the healthcare practitioner in feasibility and effectiveness of the PAVING program, answering the following research questions: 1. Are there differences in perceived program feasibility based on type of healthcare practitioner (physician vs non-physician) delivering the program? (qualitative) 2. Does the effects of the program on participant-reported health behaviors significantly differ based on the type of healthcare practitioner (physician vs non-physician) delivering the program, controlling for demographic factors? (mixed methods)
Because the healthcare practitioners in this sample self-selected into the PAVING the Path to Wellness community, had backgrounds in lifestyle medicine, and completed the same training to lead PAVING groups, it was hypothesized that there would not be a difference in feasibility or program effects based on the type of healthcare practitioner.
Methods
Study Design
The present study utilized a convergent mixed methods design to explore differences in perceived feasibility and preliminary program effectiveness by type of healthcare practitioner delivering the program (Figure 1). This study is part of a larger pilot type 1 hybrid effectiveness-implementation study, which assessed the preliminary effectiveness and implementation of the PAVING the Path to Wellness program. This study has been certified as exempt from IRB review by the Colorado Multiple Institutional Review Board (IRB#: 23-1296). Flowchart of the convergent mixed methods design procedures (Creswell & Clark, 2017).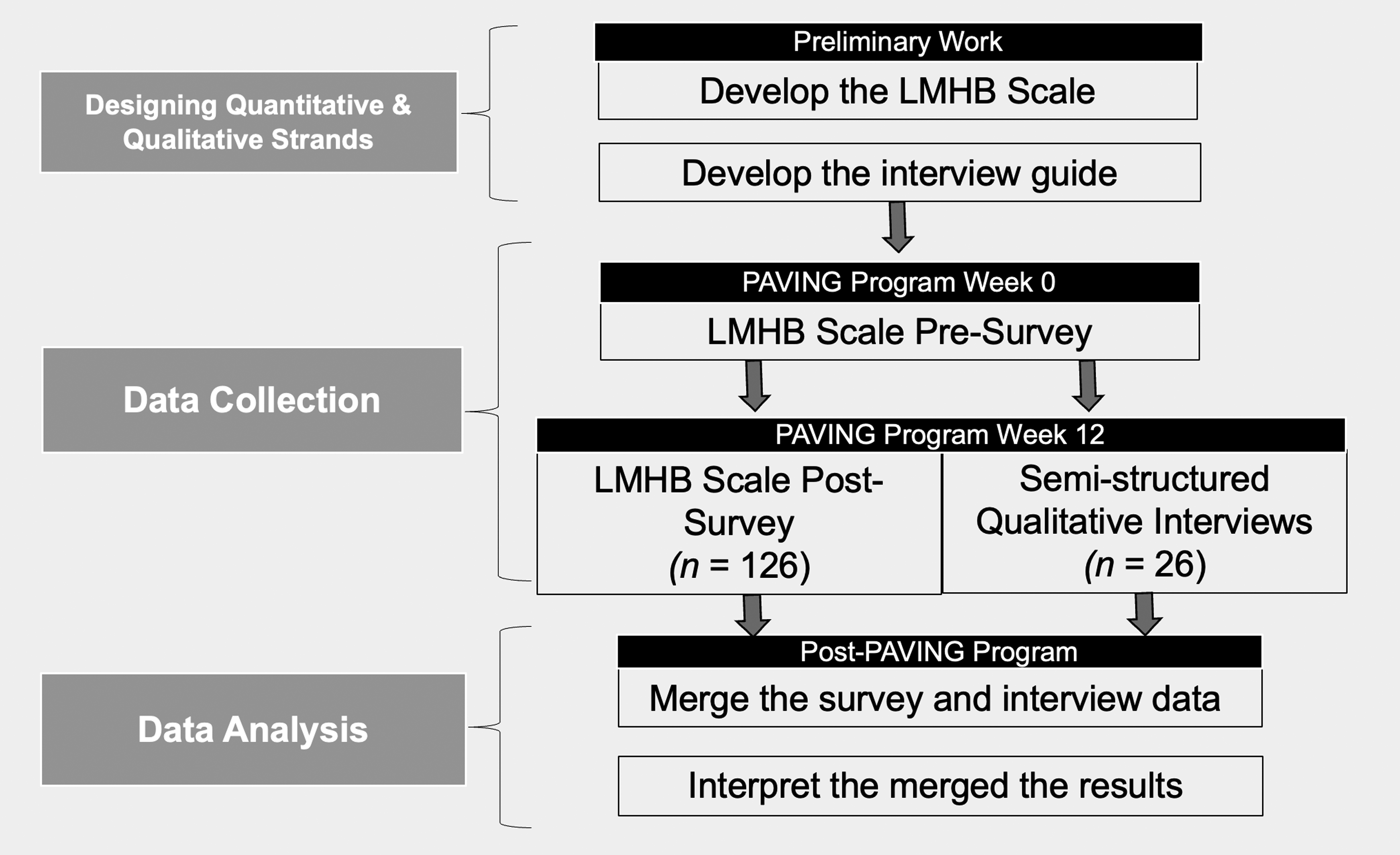
Setting
The PAVING program was delivered to 19 cohorts across the United States between March and June 2024 by trained healthcare practitioners who were recruited from the PAVING the Path to Wellness community by email. Healthcare practitioners completed an application that was reviewed by the lead investigator and PAVING the Path to Wellness executive board; qualified healthcare practitioners (i.e., appropriate credentials and in the United States) were given the opportunity to complete the PAVING Leaders Training as a part of the pilot hybrid study. Sixteen healthcare practitioners completed the training, which was a combination of asynchronous learning and live virtual sessions. Following the completion of the PAVING Leaders Training, twelve of the sixteen (75%) healthcare practitioners who completed the training went on to deliver the program during the study period. Those who did not deliver the program cited administrative or time constraints as reasons for not delivering the program. Of the twelve healthcare practitioners who delivered the program and were a part of the study, half (n = 6) were physicians and half were other qualified healthcare practitioners including a nurse, occupational therapist, physical therapist, physician assistant, health coach, and medical psychologist. Potential program participants were recruited through email, electronic medical records, social media, or flyers based on the practitioner’s network and scope of practice. Healthcare practitioners delivered the program in English in an in-person, hybrid, or virtual format based on preference. Each session involved a check-in to discuss SMART (specific, measurable, attainable, relevant, time-bound) goals, group education, and a facilitated discussion. Healthcare practitioners offered the program to their patient population of interest, which included older adults (4 cohorts), perimenopausal women (3 cohorts), hypertension (3 cohorts), breast cancer survivors (2 cohorts), multiple sclerosis (MS) (2 cohorts), diabetes (1 cohorts), and general prevention (4 cohorts).
Qualitative Strand
Procedures
Semi-structured qualitative interviews were conducted with program deliverers (healthcare practitioners) and participants to elicit in-depth perspectives on program effectiveness and implementation. All healthcare practitioners who delivered the PAVING program were interviewed (n = 12). For program participants, purposive sampling allowed for deliberate sampling of individuals from various strata (i.e., race, education status, age, health conditions, etc.) to ensure variation in sociodemographic and health status characteristics among those interviewed. The lead investigator tracked group-level details on each cohort provided by the healthcare practitioners to ensure the interviewed participants were comparable to the broader sample. Healthcare practitioners aided the research team in recruiting interested participants from various strata (i.e., race, education status, age, health conditions, etc.), and the lead investigator ensured the interviewed participants reflected the distribution of the broader sample. Participant interviews were conducted until thematic saturation was reached (n = 14), which was indicated by consecutive interviews containing no new themes. Interviews were conducted over Zoom and lasted between 30-60 min. Following verbal consent, interviews were recorded on Zoom and transcribed by Microsoft Word. The data were de-identified during data transcription and cleaning to maintain confidentiality. All interviewees were compensated for their time with a $50 electronic gift card sent via email within one week of the interview.
Interview Guide
D&I Constructs and Sample Interview Guide Questions for PAVING Leaders.
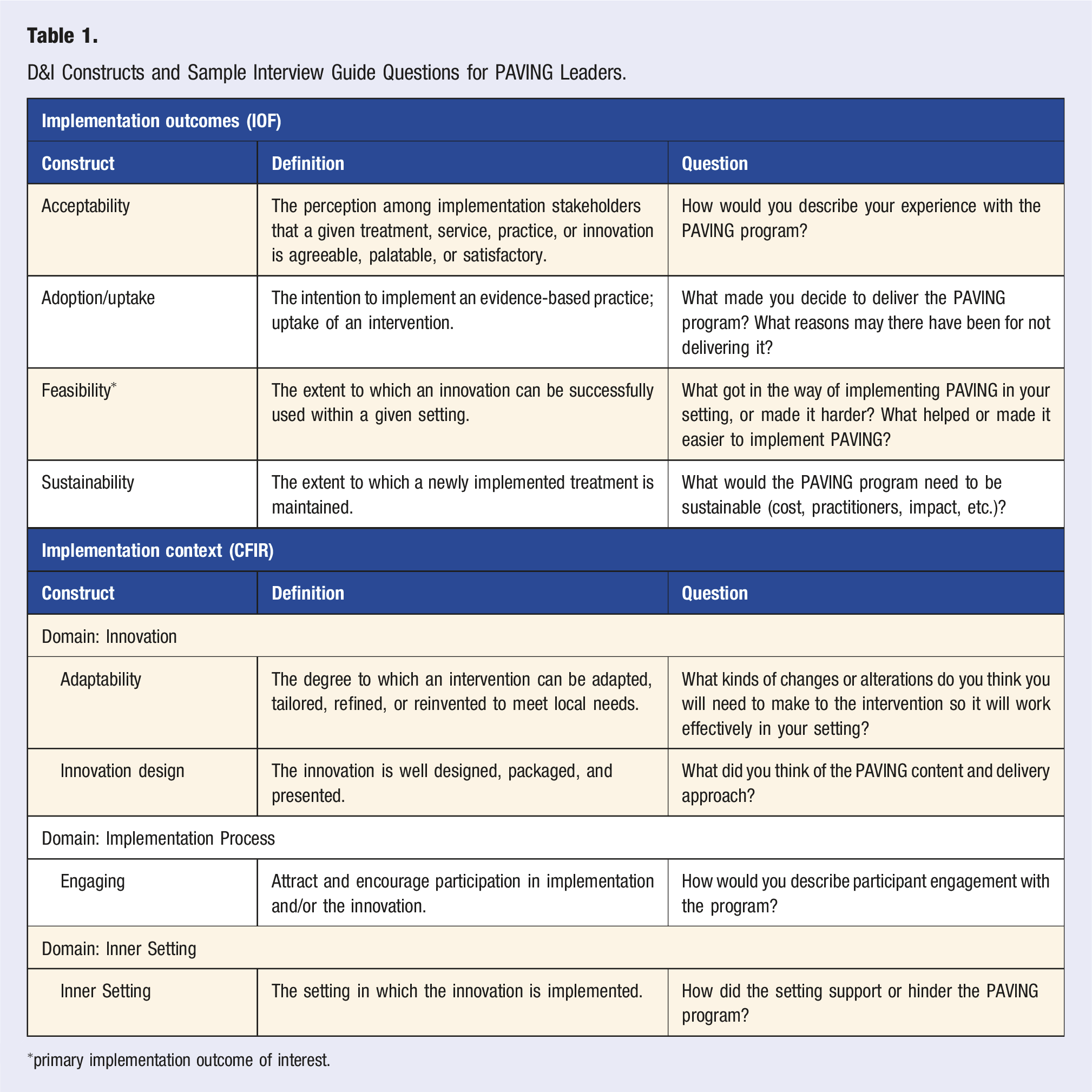
∗primary implementation outcome of interest.
Data Analysis
A phenomenological approach was used to investigate differences in perceived program feasibility based on type of healthcare practitioner (physician vs non-physician). Five transcripts were first coded independently by two researchers and compared for inter-rater reliability, with coding adjustments for consistency via discussion and consensus. The two researchers then met at regular intervals to review and ensure consensus on subsequent coding. Following coding, NVivo15 was used for data analysis. 35 A deductive, theory-driven approach based on CFIR and IOF was used alongside an inductive, data-driven approach to capture novel themes in program implementation. An iterative thematic analysis was used to draw meaning from the data broadly36,37 before framework analysis was used. The framework analysis interpreted patterns in the data based on the pre-selected D&I frameworks.38,39 Lastly, taxonomic analysis was used to systematically identify barriers and facilitators to feasibility. 40
Quantitative Strand
Procedures
Pre- and post-surveys were administered to program participants prior to the first PAVING session and again after the final session. Healthcare practitioners were responsible for sharing the survey with participants through an online link or printed copies. Both versions of the survey included an initial informed consent section that covered the study’s purpose, participation requirements, potential risks and benefits, confidentiality protocol, and contract information for the study investigators and the Colorado Institutional Review Board. Qualtrics, a secure electronic application for collecting and storing data, was used to administer the online survey. 41 Following both pre- and post-survey completion, participants were sent a $25 e-gift card to compensate them for their time. For participants who were not able to complete the survey online due to accessibility issues, a paper version of the survey was administered following the same consent procedure and physical gift cards were provided following survey completion. Physical copies of the data were stored in secure locations (e.g., a locked filing cabinet). Participants who did not complete the survey were given 1-2 reminders by their healthcare practitioner. All data were collected between June 2024 and April 2025.
Measures
This study utilized the Lifestyle Medicine Health Behavior (LMHB) scale, which assesses self-reported health behaviors across the six pillars of lifestyle medicine (nutrition, physical activity, sleep, social connection, stress, and avoidance of risky substances). 42 The LMHB scale assesses the six lifestyle medicine pillars using 3-5 items per pillar (23 items in total). Sample items for sleep and physical activity include, “Do you sleep between 6 and 8 hours per day?” with Likert response options including, “Never, Rarely, Sometimes, Usually, and Always” and “On a typical week, how much time do you spend in total on moderate and vigorous physical activities where your heartbeat increases and you breathe faster (e.g., brisk walking, cycling as means of transport or as exercise, heavy gardening, running or recreational sports)? Only include activities that lasted at least 10 min at a time.” Response options included, “Less than ½ hour, ½ an hour - 1 ½ hour, 1 ½ hour - 2 ½ hour, 2 ½ hour - 5 hour, and More than 5 hours.” The survey also included demographic items (age, employment status, sex, race, education level).
The LMHB scale has undergone psychometric evaluation to assess content validity, construct validity, convergent validity, content validity, face validity and internal consistency reliability in a sample of 399 adults. Content validity was established by review from five experts with experience in lifestyle medicine and survey methods. The scale was shown to have appropriate construct validity fit with a five-factor model (χ2 [224] = 502.48, P < .001, CFI = .91, TLI = .90, RMSEA = .06, SRMR = .07). Convergent validity was demonstrated through correlations between items selected for each pillar and the full scales that the items were derived from (nutrition r = 0.69, P < 0.001; sleep r = 0.72, P < 0.001; P < 0.001; social connectedness r = 0.82, P < 0.001; avoidance of risky substances r = 0.693, P < 0.001). Face validity was demonstrated through participant feedback; participants reported that the items were clear and that the scale was easy to complete. Lastly, internal consistency reliability was established (α = 0.84). The scale has also been validated to assess cardiovascular disease risk using the UK Biobank sample, with a higher LMHB score associated with lower cardiovascular disease risk. 43
Data Analysis
After data collection was concluded, data were exported into SPSS Version 28.0 for analyses. Pre- and post-data were matched, yielding a total of 126 participants for the final analytic sample. The demographics of the matched pairs (n = 126) were compared to those who only completed the pre-survey (n = 176) or post-survey (n = 141) to ensure there were no notable differences, and none were found. Following data cleaning and matching, we investigated patterns of missingness in the final analytic sample. The data were missing completely at random (Little’s MCAR = 401.34, df = 391, P = .348), with missing data ranging from 0 to 4%. Frequencies and descriptives were run to explore all variables of interest. Listwise deletion was used since data were missing at random.
Multiple mixed linear models were run to determine if the effects of the program on reported health behaviors significantly differed based on the type of healthcare practitioner (physician vs non-physician) leading the PAVING group, controlling for demographic factors. The models included time (pre-/post-PAVING program) as a fixed effect, practitioner type (physician vs non-physician), the interaction between time and practitioner type, and participant demographic variables (sex, race, education, work status). An unstructured covariance structure was used to model within-subject variability across timepoints. Compound symmetry was also considered for parsimony, but the unstructured covariance displayed a better model fit based on AIC and BIC values. The unstructured structure approach was confirmed to be stable using the covariance estimates; this approach was used across all models.
Mixed Methods
To better visualize differences in program impact on reported health behaviors between participants in physician vs non-physician-led groups, the estimated marginal means (pre-program to post-program) were plotted for each of the six lifestyle medicine health behaviors (nutrition, physical activity, sleep, social connection, stress, avoidance of risky substances). The data were then triangulated with qualitative interview data on program impact across each of the six lifestyle medicine health behaviors.
Results
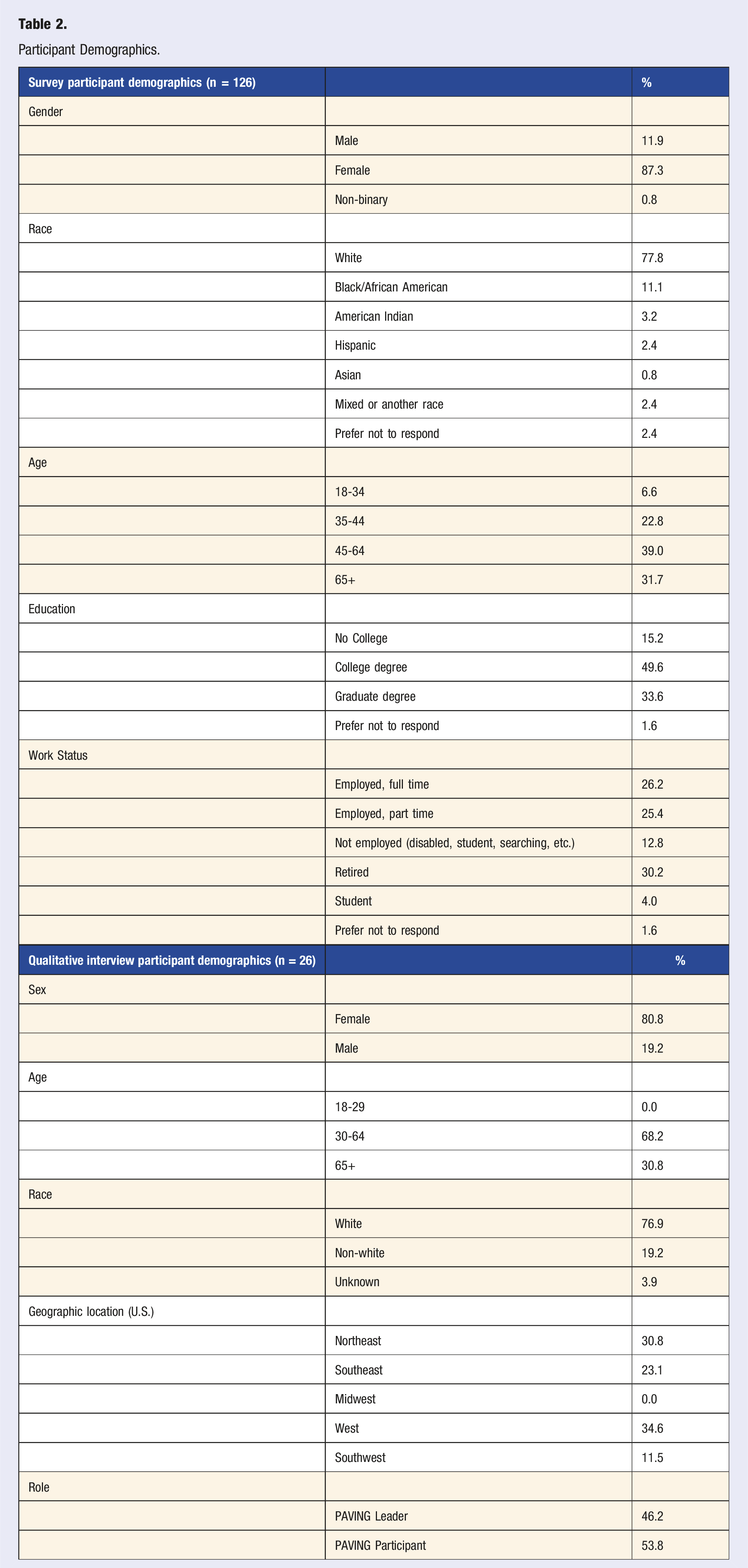
Participant Demographics.
Qualitative Results
A total of 26 interviews were conducted with healthcare practitioners (n = 12) and program participants (n = 14). The majority of the samples were females between the ages of 30 and 64, which aligns with broader study sample (Table 2).
Feasibility
Overall, qualitative analyses revealed that the program had high perceived feasibility. When asked about their experience offering the PAVING program, one practitioner said, “It was pretty easy, I would say. 8 on [out of] 10, maybe 9 even.” To better understand the feasibility of program implementation, the qualitative data were analyzed to examine differences in feasibility based on the type of healthcare practitioner (physician vs non-physician) delivering the program. In general, physicians reported more barriers and fewer facilitators to program implementation compared to non-physicians. However, given the qualitative nature of this analysis and the small sample size, these results should be interpreted with caution.
Taxonomic analysis was then used to identify and categorize key considerations related to the feasibility of program implementation and provide an understanding of how these considerations converged or diverged across physicians and non-physician program deliverers (Figure 2). It is important to note that these are the barriers and facilitators reported by individual healthcare practitioners; not all barriers and facilitators were reported by every provider, so this list is not representative of the group as a whole. They are instead reflective of the unique experience of each practitioner, which was influenced by the organization, delivery modality (in-person, virtual, hybrid), previous experience with group-based lifestyle medicine programs, and other contextual factors. Key barriers and facilitators to program implementation are further described below. Taxonomic analysis of the barriers and facilitators influencing feasibility reported by healthcare practitioners (physicians vs non-physicians).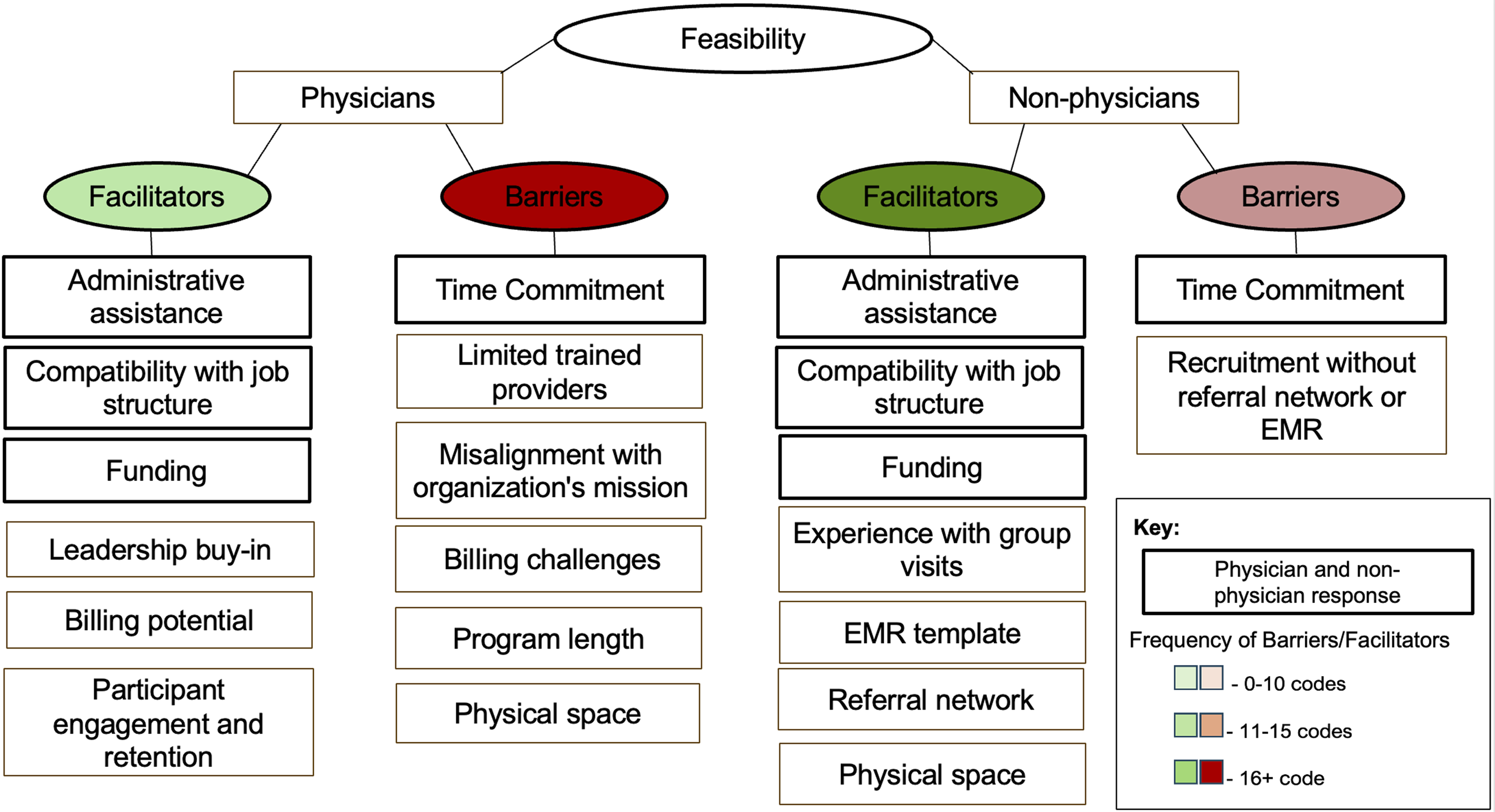
Funding and Billing Challenges
Some considerations were reported across multiple physician and non-physician program deliverers and were categorized as cross-role themes. Uncertainty and challenges around funding the program and practitioner reimbursement emerged as critical to program feasibility: We need to understand better what the billing model is gonna look like. So, talking about American healthcare like which insurances are gonna allow this or.. understanding the cost model better.. figuring out who does that.. So we need to know how much it's gonna cost and figure out what that would look like. - Leader
While some practitioners had the opportunity to bill the program as a group visit, many lacked the administrative support or capacity to establish the infrastructure needed to bill patients in the context of this pilot: We don't have, like, a billing and compliance department that would help me figure that part out. It would be a lot of just finding those steps on my own. - Leader
Program deliverers described varying levels of compatibility between their current job structure and program implementation, which significantly influenced perceived feasibility. Across physician and non-physician program deliverers, being able to be paid through their current job structure was a key facilitator when possible: I'm in a lucky situation because this is my job. I get paid to do this.. I think it's good for the healthcare system to say that they're offering it.. And I'm super happy doing it. I love it. - Leader
Another said, “I just kind of added it and I still counted it as work time but like I was allowed to do that. It was just additional stuff.” Regardless of whether practitioners were able to be reimbursed for implementing the program for this pilot, the general consensus was that financial support (e.g., billing, reimbursement) would need to be streamlined to sustain the program. Part of establishing the billing process involves modifying the program structure to meet billing requirements. The PAVING program is very adaptable, allowing program deliverers to modify the program's length and format (e.g., virtual versus in person) to bill as needed based on their practice. Most practitioners agreed that to support the billing potential of the program as a shared medical appointment or out of pocket, the program duration would need to be eight weeks or less. As one practitioner said, “My only thing is I think for me in a clinical practice or private practice, it would have to be cut down to at least eight weeks.” These comments provided critical quality improvement and best practice insights for the PAVING program, as the standard model is weekly meetings over twelve consecutive weeks.
Adequate funding was not only critical for the program deliverer, but also to provide valuable support that enhanced program feasibility. The most reported support was administrative assistance: “I did have an administrative assistant, which was critical.” Another program deliverer said, “I had like a support person who was calling them, told them about the program, and kind of she got them to come. That was huge. Again, it's a rural community so.. I don't live in the community, so having someone there from the community, who knows everybody, that was really huge.”
Healthcare Practitioner Experience and Training
Another theme that emerged across practitioners was previous healthcare experience. Those who had offered group visits before felt more prepared to deliver PAVING and, therefore, described higher perceived feasibility. And then I the fact that I had done group medical visits before, so I kind of already had that that template piece already in there. I already knew how to do. - Leader
Regardless of previous experience, several leaders felt that the PAVING Leaders Training equipped them to deliver lifestyle medicine programming and provided a structure to successfully implement group visits that they would not otherwise have access to. I feel like the [PAVING] training prepared me really well for what I wanted to convey and how I wanted to present the information with a good clear picture and a solid background. - Leader
Quantitative Results
The quantitative results on program effectiveness were analyzed from the pre-/post-survey given to program participants. The final analytic sample (n = 126) was predominantly white (78.4%) and female (87.3%), which was reflective of the overall sample (Table 2). Most of the sample were 45 years old or older (70.7%), with 22.8% aged 35-44 and 6.6% 35 or less. Half of the participants had a college degree as their highest degree (49.6%), 32.8% had completed a graduate degree (i.e., master’s, doctorate), and 15.2% of participants did not have a college degree.
Type III Tests of Fixed Effects for Interaction Effect of Time x Practitioner Type Across Health Behavior Outcomes.
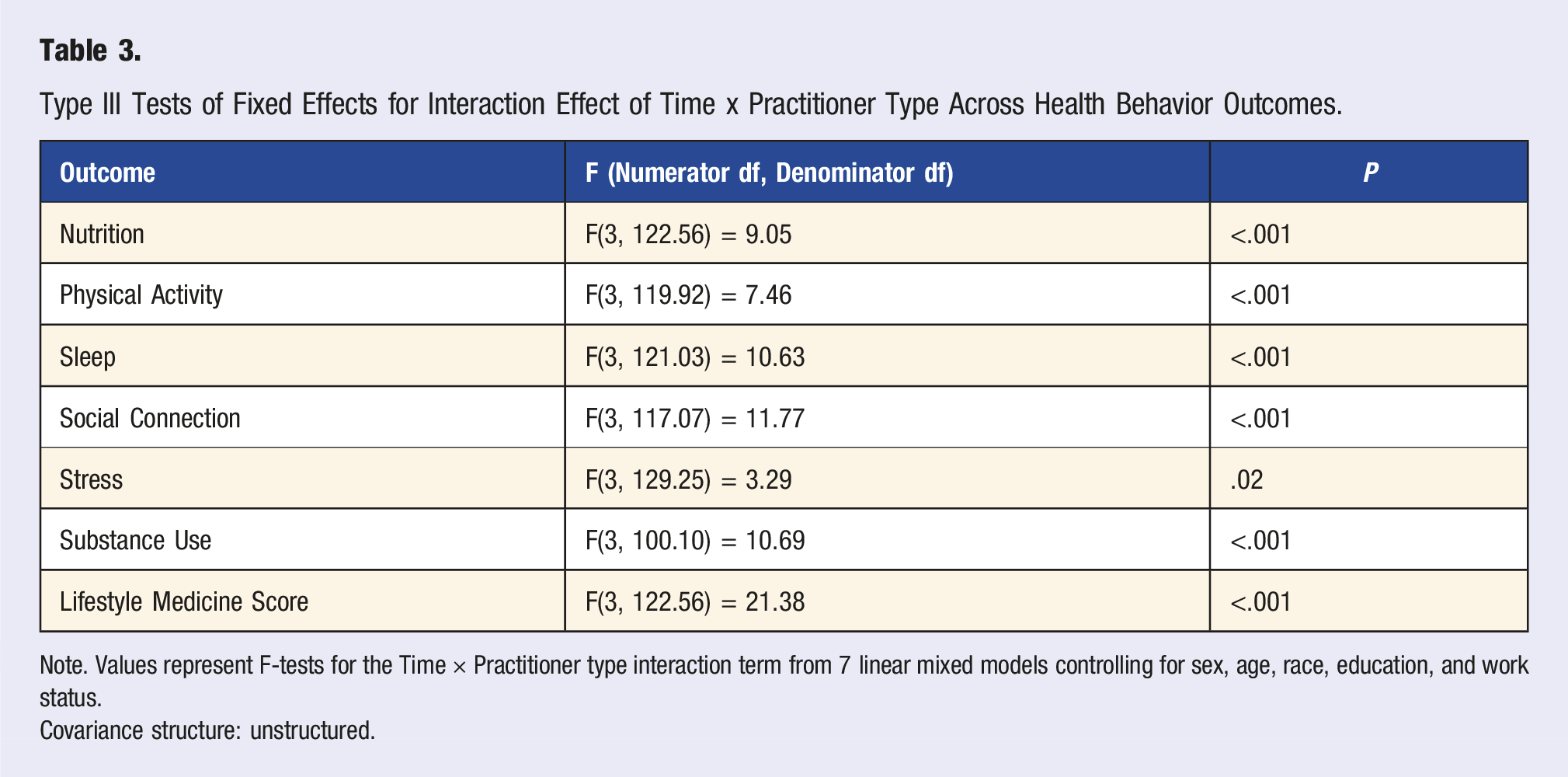
Note. Values represent F-tests for the Time × Practitioner type interaction term from 7 linear mixed models controlling for sex, age, race, education, and work status.
Covariance structure: unstructured.
The estimated marginal means for each pillar were plotted to visualize the interaction effect between type of practitioner and examine patterns of change in outcomes for physician and non-physician-led groups (Figure 3). The plots demonstrated that health behavior outcomes across both groups generally improved following the program. However, the magnitude of change varied depending on the outcome and type of practitioner. For nutrition and physical activity behaviors, the non-physician-led groups saw more improvements compared to the physician-led groups. This trend was also true of sleep, social connection, and stress, though the improvements were more modest. Substance use improved (higher score = lower substance use) in the non-physician-led group but remained fairly stable in the physician-led group. Non-physician-led groups saw a greater improvement in overall lifestyle medicine score compared to the physician-led groups. Joint display of participant and practitioner quotations and estimated marginal means of pre-/post reported behavior changes between non-physician and physician-led groups.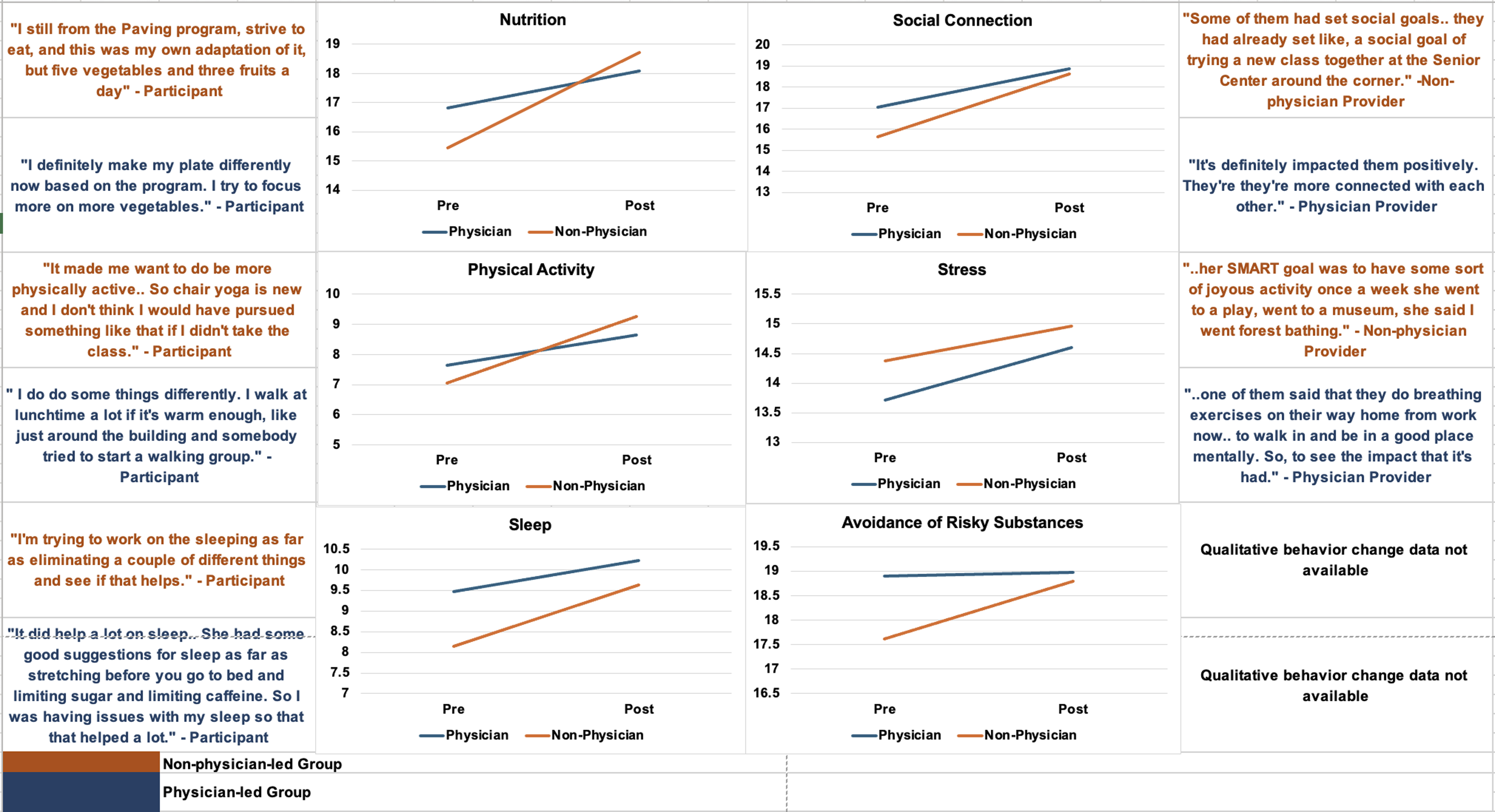
Mixed Methods Results
Data triangulation between the quantitative results and qualitative interviews provided more insight into the program’s impact on lifestyle medicine health behaviors. Qualitative data from physician and non-physician practitioners as well as program participants were integrated to contextualize the quantitative results; Figure 3 illustrates this integration in a joint display. The qualitative results put the quantitative results to expand on how the program influenced each lifestyle medicine pillar.
Discussion
The results of this study contribute to the growing body of literature on group-based lifestyle medicine programs, highlighting key implementation considerations for program effectiveness and feasibility. The qualitative results emphasized the challenge of reimbursement, highlighting the need for increased policy-level and programmatic support for billing group visits. 44 This theme builds on our prior findings about implementation of the PAVING program, which found that aspects of the CFIR-defined Inner Setting (organizational infrastructure, funding and resources, compatibility, and mission alignment) were key to successful group visit implementation. 30 These findings also echo the broader literature on group visits, emphasizing the challenges that billing presents across various settings and types of healthcare practitioners.6,45-47 Reimbursement in traditional fee-for-service payment models has historically hindered the expansion of chronic disease prevention efforts, specifically when it involves group visits and team-based care.6,48 While the expansion of payment models to support group-based lifestyle interventions is promising,49,50 it is also complex and dependent on the type of health care practitioner and setting51,52 Future research and policy development should aim to streamline reimbursement processes for chronic disease prevention49,52
The quantitative results from the mixed linear models demonstrated that the PAVING program positively impacted participant-reported health behaviors, and that program effectiveness significantly differed based on type of practitioner. Compared to those in groups facilitated by physicians, participants in groups that were facilitated by non-physician healthcare practitioners (primarily allied health professionals) saw greater improvement in self-reported health behaviors following the PAVING program. This may be because allied health professionals are more likely to have positive attitudes towards preventive health promotion approaches compared to physicians.53-56 Many primary care practitioners feel ill-equipped to offer lifestyle medicine programming despite recognizing the value of this type of preventive care.7,57,58 One study of physicians found that most physicians did not feel confident and their ability to change patient health behaviors. Adequate training was found to be the only significant predictor of high self-efficacy for counseling patients on lifestyle behaviors. 57 A separate qualitative study found that physicians identified lack of confidence, knowledge, and skills as barriers to providing lifestyle counseling to patients. 58 While existing literature helps to explain the finding that physician-led groups saw less improvement in health behaviors, all the health professionals in this study volunteered to lead the PAVING program and had a vested interest in lifestyle medicine. As such, the physicians that self-selected into this study likely have more knowledge of lifestyle counseling and are not representative of the average practitioner. For this reason, it was hypothesized that there would not be a statistically significant difference in program effectiveness based on type of healthcare practitioner. However, the results indicated that there was a difference in program effectiveness based on practitioner type, with participants in the non-physician-led groups reporting greater behavior change. When considering this result, it is valuable to note that participants in the non-physician-led groups typically scored lower at baseline, which indicates these participants had a greater potential for behavior change. For instance, the physician-led group had a near perfect score (19/20) on avoidance of risky substances and had a very limited opportunity for improvement (i.e., ceiling effect).
Outside of training, time constraints have historically made it challenging for physicians to prioritize preventive care.59-61 In this study, physicians reported more barriers to implementing the PAVNG program compared to non-physician providers, further suggesting that contextual factors may have differentially influenced implementation by physician and non-physician providers, as well as program effects in groups led by each type of provider. Greater physician-reported barriers along with differences in baseline health status between groups may have influenced the quantitative results.
Integrating qualitative data on the feasibility of implementation strategies added critical context to the quantitative findings. Healthcare practitioners (physicians and non-physicians) who delivered the PAVING program felt that the PAVING training, a background in lifestyle medicine, and experience with group visits were key facilitators to program feasibility. These results emphasize the need for standardization and expansion of training for group-based health promotion interventions.17,62 Well-defined and organized group programs paired with high quality training for providers may be especially valuable to improve physician self-efficacy and attitudes towards delivering lifestyle medicine interventions and navigating implementation barriers.62-64 Enhancing opportunities for all types of healthcare practitioners to engage in practice-based training can promote lifestyle medicine intervention adoption and effectiveness,17,65,66 which can support the widespread implementation of lifestyle medicine group programs in clinical and community practice.6,45,46
Existing literature supports that the PAVING program demonstrates promise for effectively improving health behaviors.27-30 This study adds to the evidence by highlighting healthcare practitioner training as a key implementation strategy. It also calls attention to potential differences in training and preparedness between types healthcare practitioners, with non-physician practitioners (e.g., occupational therapists, physical therapists, nurses, physician assistant) potentially facing fewer barriers to lifestyle medicine program implementation. Further investigation should be done to understand what types of healthcare practitioners and settings are best suited for implementing the PAVING program.
Furthermore, continuing to standardize and scale the PAVING Leaders Training could provide a practical opportunity to equip healthcare practitioners with varying experience in lifestyle medicine to deliver group-based programming, enhancing the adoption and sustained delivery of PAVING the Path to Wellness and other lifestyle medicine interventions.7,20,67 Future iterations of the PAVING Leaders Training should be segmented based on the type of practitioner and experience in lifestyle counseling. The study also underscores the need for streamlined billing and reimbursement processes for lifestyle medicine group visits. Lastly, it highlights the value of integrating D&I science and evidence-based frameworks into lifestyle medicine evaluation to enhance the scalability of lifestyle medicine in real-world practice.66,68-70
Limitations
While this study provided practical insights for lifestyle medicine program implementation, it is not without limitations. First, the program deliverers were a self-selected group of healthcare practitioners with a vested interest in lifestyle medicine. They are not representative of healthcare practitioners as a whole and may have potentially biased the results towards more favorable outcomes. For instance, a more representative group of healthcare practitioners may have reported lower overall feasibility. Second, the absence of a control group of participants restricts the ability to conclude that the health behavior impacts were a result of the intervention and not external factors. It is also important to note that participants in the non-physician-led groups scored lower at baseline for many of the health behaviors compared to participants in the physician-led group. This lower baseline score may indicate that these participants had greater potential for behavior change. Third, health behavior change was assessed via participant report rather than by objective and observational measures. The measure used to assess health behaviors, however, has demonstrated good psychometric properties compared to other instruments and has the advantage of being pragmatic and low-burden, important requirements in research conducted in “real world” contexts. Future work should include a large and diverse sample and random assignment to reduce bias and promote generalizability of the results. 71 To further investigate the role of the healthcare practitioner, randomized controlled trials should assign participants to the practitioner and account for participant’s baseline health.
Conclusion
This study provided insights to help establish best practices for group visit implementation and evaluation to support the integration of lifestyle medicine interventions in practice. While the PAVING program generally led to reported health behavior improvements across all groups, participants in non-physician-led groups (e.g., allied health professionals) reported greater improvements in participant-reported health behaviors than those in physician-led groups. The mixed methods findings emphasized that systemic and individual practitioner-level factors influence the feasibility and effectiveness of the PAVING program. Billing opportunities and reimbursement procedures emerged as essential to program feasibility, highlighting a need for payors and healthcare systems to streamline procedures and administrative support for billing group visits and preventive are. Further investigation highlighted ample training and experience in health coaching and lifestyle medicine programming as crucial to program delivery. Medical education and healthcare organizations should consider adopting practice-based training for lifestyle medicine interventions. Future efforts should focus on policy advocacy for reimbursement, training standardization, and infrastructure development to facilitate the effectiveness, adoption, and sustainability of group-based lifestyle medicine interventions in practice.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Two authors serve on the executive board of the PAVING the Path to Wellness non-profit. This is not a paid position. Their involvement providded strategic insight in alignment with the organization's mission. To avoid any potential conflict of interest, these individuals were not involved in the research activities.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Ardmore Institute of Health.
Data Availability Statement
Data is available from the authors upon request.