
Abstract
Polycystic ovary syndrome (PCOS) is a common endocrine disorder in women of reproductive age. Most patients present insulin resistance (IR) and impaired VO2max associated with cardiovascular mortality. While exercise is recommended as the first-line treatment, there is a lack of certainty of the exercise intensity effect on improvement of pathogenic factors. The aim of the study was to determine the effect of MICT on VO2max and HOMA-IR compared to other exercise intensities in women with PCOS. Search was performed on PubMed, Scopus and Web of Science during February 2025. Eligible studies included RTCs, women with PCOS diagnosis, moderate-intensity training and/or other intensities intervention lasting ≥8 weeks, and VO2max measured by direct method. Meta-analyses included 10 studies involving 289 participants. MICT improved cardiorespiratory capacity as follows: 4.65 mL/kg/min, 95% CI: 3.07-6.23 P < 0.001, I2 = 84% n = 9; and HIIT: 3.55 mL/kg/min, 95% CI: 1.84-5.26, P < 0.001, I2 = 0% n = 4. No effect was seen on HOMA-IR with MICT: 0.06, 95% CI: −0.67-0.78 P < 0.88, I2 = 0% n = 3; or HIIT: −0.20, 95% CI: −0.70-0.31, P < 0.44, I2 = 0% n = 3. In conclusion, MICT appears to promote greater changes of VO2max than HIIT and none of those exercises had a significant impact on IR.
“In addition to the androgen excess, the high prevalence of IR and its association with cardiopulmonary impairment could increase the risk for cardiometabolic disease.”
Introduction
Polycystic ovary syndrome (PCOS) is the most common endocrine disorder among women of reproductive age. Its global prevalence of 9.2% differs according to Rotterdam diagnosis criteria.1,2 Clinical presentation is heterogeneous and can be categorized in several phenotypes involving symptoms such as hirsutism, alopecia, acne, irregular menstrual cycles and reduced fertility. 3 Although PCOS is mainly a hyperandrogenic disorder, evidence suggests a strong association to insulin resistance (IR) and its compensatory hyperinsulinemia.4,5 IR affects adipose tissue and skeletal muscle, favoring adipocyte dysfunction with low grade of inflammation and impaired muscle mitochondrial function compared to their counterparts without PCOS. 6 While IR is not a diagnosis criteria, 37.5% of women with PCOS present this condition. 7 Metabolic dysfunction along with other health-related issues like abdominal obesity, sedentary lifestyle and poor diet facilitates androgen secretion in a vicious circle that worsens the underlying hormonal disturbances. 8 Therefore, insulin sensitivity not only plays a crucial role in the pathophysiology of PCOS but also in its treatment.9,10
PCOS is a significant concern in women’s health. Patients are at a higher risk of developing metabolic syndrome, diabetes mellitus, cardiovascular diseases and cancer compared with age-matched and Body Mass Index-matched controls.11,12 Evidence indicates that overweight/obese PCOS women usually present an impaired cardiorespiratory capacity measured as maximal aerobic capacity (VO2max). VO2max is a very important indicator of the patient’s ability to sustain physical activity and impacts not only on exercise adherence, but also on quality of life. Some studies had observed an inverse correlation between IR and VO2max in overweight and obese women with PCOS 13 which could be associated with mitochondrial dysfunction.14,15 Low levels of VO2max may be related to an increase in autonomic sympathetic tone, decrease vagal tone 16 and could be linked to the androgenic pattern in PCOS patients. 17 Moreover, diminished functional capacity may perpetuate IR over time and increase cardiovascular mortality risk. 18
While no universal therapy for PCOS is available, lifestyle modifications (including dietary changes, physical activity or both) are considered as the first line of intervention. 19 Exercise has been shown to reduce adipose tissue and IR, which contributes to reducing hyperandrogenism. Promoting normal endocrine and adrenal functions may result in a complete recovery from the clinical characteristics of PCOS.20,21 Studies have reported that exercise training can substantially improve VO2max and other metabolic markers including insulin sensitivity measured by homeostatic model assessment of insulin resistance (HOMA-IR). 22 The improvement in physical conditioning leads to increased tissue sensitivity to insulin and reduces cardiovascular risk factors in persons with IR. 23
The international evidence-based guidelines for the assessment and management of PCOS recommends 150 min/week of moderate intensity or 75 min/week of vigorous intensity exercise for all women with PCOS. 19 In addition, results from a systematic review advised women with PCOS to engage at least 90 min of moderate intensity continuous training (MICT) at 60%–70% of VO2max per week to reduce cardiometabolic problems. 20 Nonetheless, authors suggest that higher intensities may offer superior metabolic health benefits and serve as a more time-efficient alternative to traditional endurance training.24-26 Therefore, the aim of the present study was to determine the effect of MICT on VO2max and HOMA-IR in comparison to other exercise intensities in women with PCOS.
Methods
Protocol and Registration
This meta-analysis was approved and registered on Prospero International Prospective Register of Systematic Reviews (CRD42024623712).
Search Strategy, Study Selection and Data Extraction
We performed a systematic search of all publications up to February 2025 using Pubmed, Scopus and Web Of Science databases. This review was carried out in accordance with the guidelines on Cochrane Handbook for Systematic Reviews of Interventions and with PRISMA statements for the reporting of systematic reviews.
27
Figure 1 shows the PRISMA flow diagram for study selection. MeSH terms and free-text were used to perform the search (Appendix A), and the reference lists of other review articles were explored using snowballing methods to identify other potential eligible studies. The search was restricted to full text available articles in English or Spanish. PRISMA flow diagram for study selection.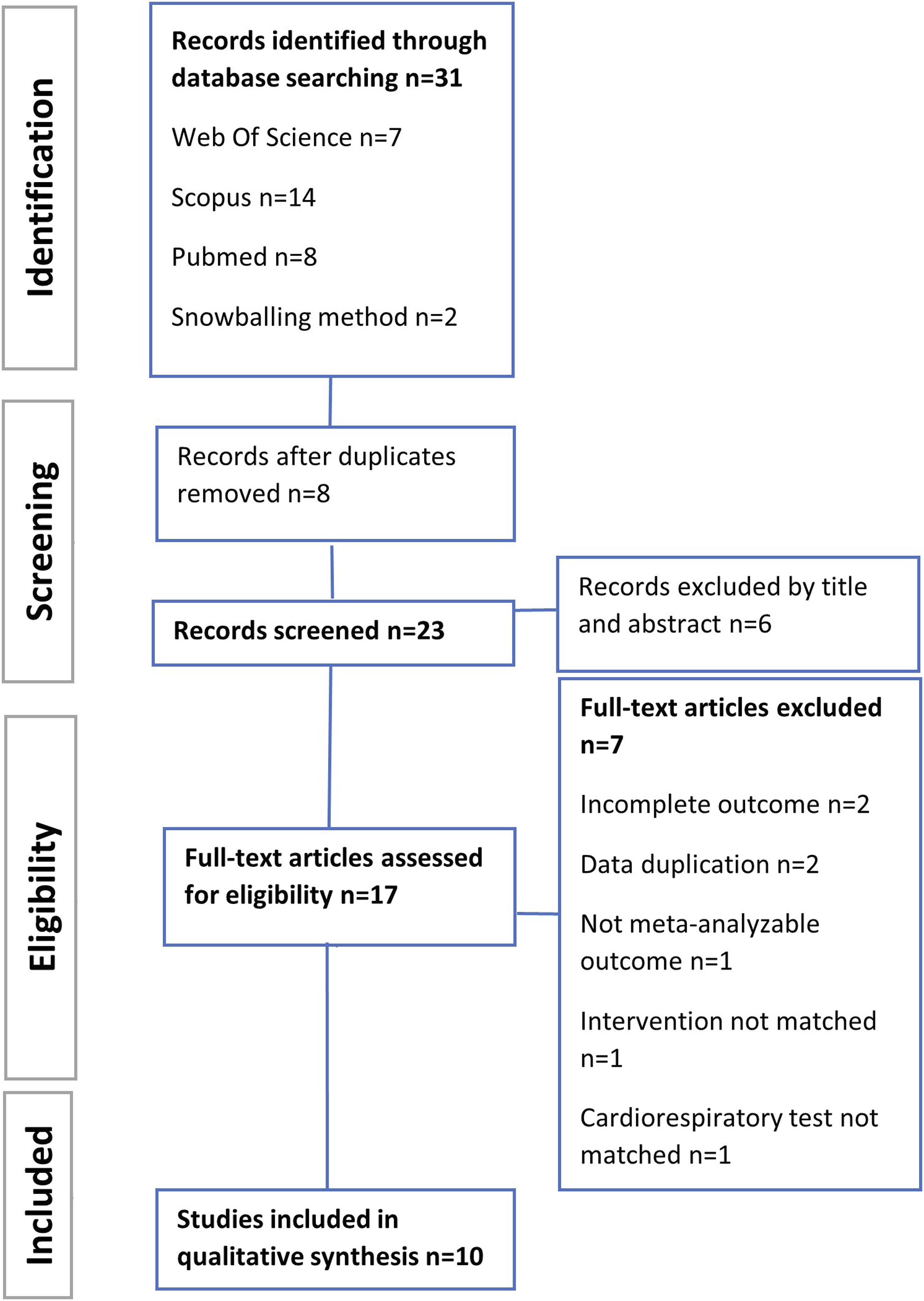
Initial study selection and screening process was completed by 1 reviewer (MFC). After removing duplicate articles, title and abstract were examined to identify the inclusion criteria. Subsequently, 2 authors (MFC and BOR) independently completed full-text screening. Any discrepancies were resolved by consensus or by arbitration from a third reviewer (LGD). The remaining articles were compared and selected based on the population, intervention, comparison, outcome, and type of study (PICOS).
Eligibility Criteria Established by PICO Methodology: Participant, Intervention, Comparison and Outcome.
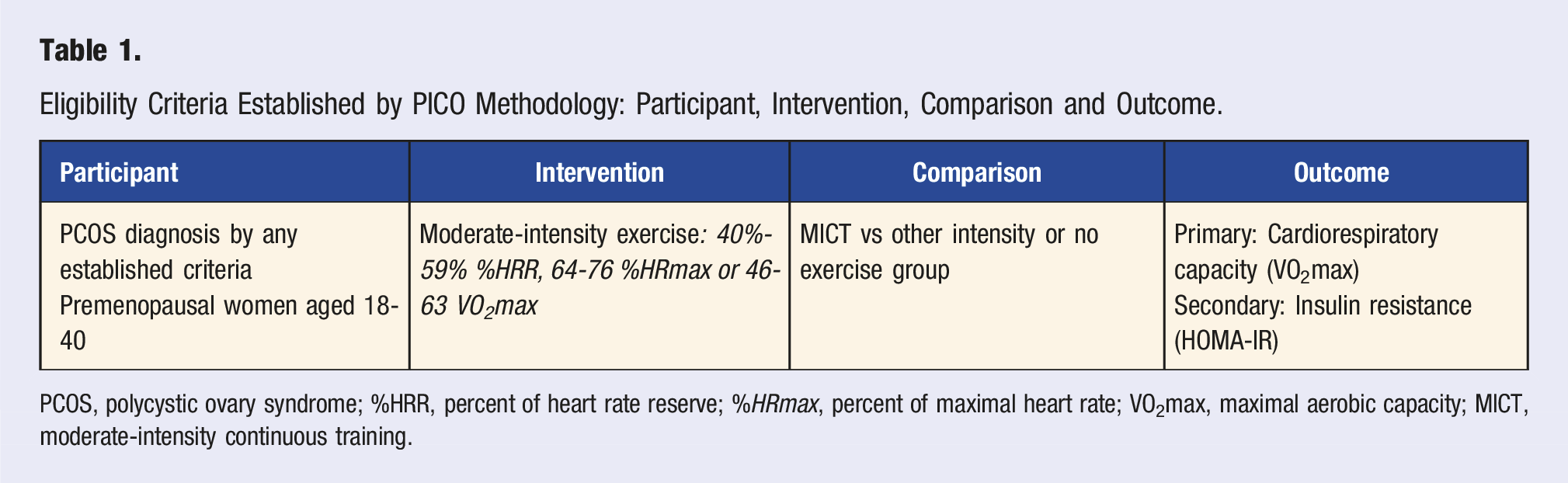
PCOS, polycystic ovary syndrome; %HRR, percent of heart rate reserve; %HRmax, percent of maximal heart rate; VO2max, maximal aerobic capacity; MICT, moderate-intensity continuous training.
Risk of Bias (Quality) Assessment and Certainty of Evidence
Two authors (MFC and BOR) independently assessed the risk of bias in the trials using guidance outlined in the Cochrane tool for risk of bias assessment with RoB 2. Bias was evaluated as a judgment (high, low or unclear) for 5 domains including selection, performance, attrition, reporting and others. Overall risk-of-bias assessment and categorization were determined and expressed as High risk of bias, Low risk of bias or Some concerns. Same authors assessed the certainty of the evidence using the GRADEpro® framework.
Data Synthesis, Subgroups Analysis and Sensitivity
All outcomes were analyzed using Cochrane’s Review Manager (RevMan Version: 8.18.0). Continuous data were input as means, standard deviation (SD) and sample size. When studies reported standard error of the mean (SEM), SD was calculated according to Cochrane Handbook. 29
Data were excluded from meta-analysis if results were presented only as medians with ranges, or if non-parametric statistical analyses were used. Forest plots of the intervention effect were estimated, and their 95% confidence intervals (CIs) were created for each meta-analysis. Subgroup analyses were conducted to compare the effects of MICT with either no-exercise control groups or with other exercise intensities. Data were pooled using fixed-effect or random-effects models, depending on the level of heterogeneity, which was considered important if I2> 50%. Sensitivity analyses were performed to assess the robustness of the results and the influence of each study on the pooled estimates. Publication bias was assessed visually using a funnel plot graph and statistically using the Egger’s test, performed in RStudio. 30
Results
The systematic search in literature (Figure 1) returned 31 records from the databases and reference lists. After removing duplicates and studies that did not qualify by title/abstract, 17 full-text articles were assessed by eligibility. Of these, 8 records were excluded for different reasons. Finally, a total of 10 articles were included. In line with the specific purpose of this review, we only included MICT and HIIT interventions as pre/post values. A total of 13 interventions were extracted from these 10 studies, where 6 of them applied a MICT protocol with a no-exercise control,31-36 3 compared MICT vs HIIT protocol,37-39 and 1 study evaluated HIIT against both Strength training and a no-exercise group. 40
Participant and Intervention Characteristics
Main Characteristics of Included Studies.
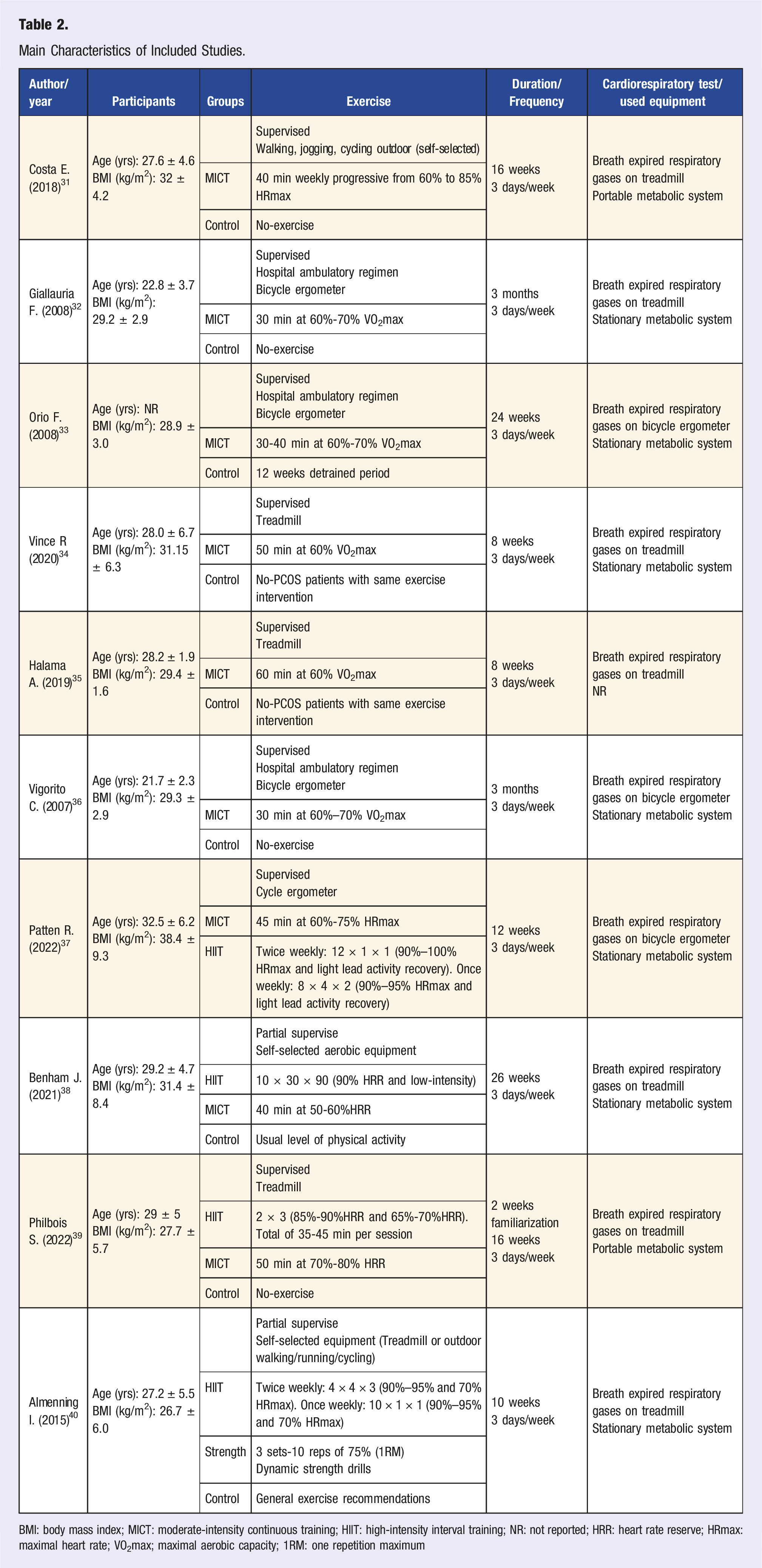
BMI: body mass index; MICT: moderate-intensity continuous training; HIIT: high-intensity interval training; NR: not reported; HRR: heart rate reserve; HRmax: maximal heart rate; VO2max; maximal aerobic capacity; 1RM: one repetition maximum
Interventions extended from 8 to 24 weeks. The 16-week program was most common (n = 3) and exercise frequency was generally 3 sessions per week. MICT protocol fluctuated between 30 and 50 min with intensities prescribed at 60% to 80% prescribed as HRmax,31,37 HRR38,39 or %VO2max.32-36 HIIT sessions ranged between 20 and 50 min involving intensities from 65%-70% up to 90%–100% of HRmax37,40 or HRR.38,39 Exercise modalities included between cycle ergometer, treadmill walking/running and outdoor walking/running. One study allowed for participants to choose their desired aerobic equipment.
Cardiorespiratory capacity was measured using expired gas analysis performed on a treadmill (n = 7)31,32,34,35,38-40 and on a bicycle ergometer (n = 3).33,36,37 Two of the included studies employed a portable metabolic system.31,39 All results were reported as VO2max in mL/kg/min.
Risk of Bias and Risk of Publication Bias
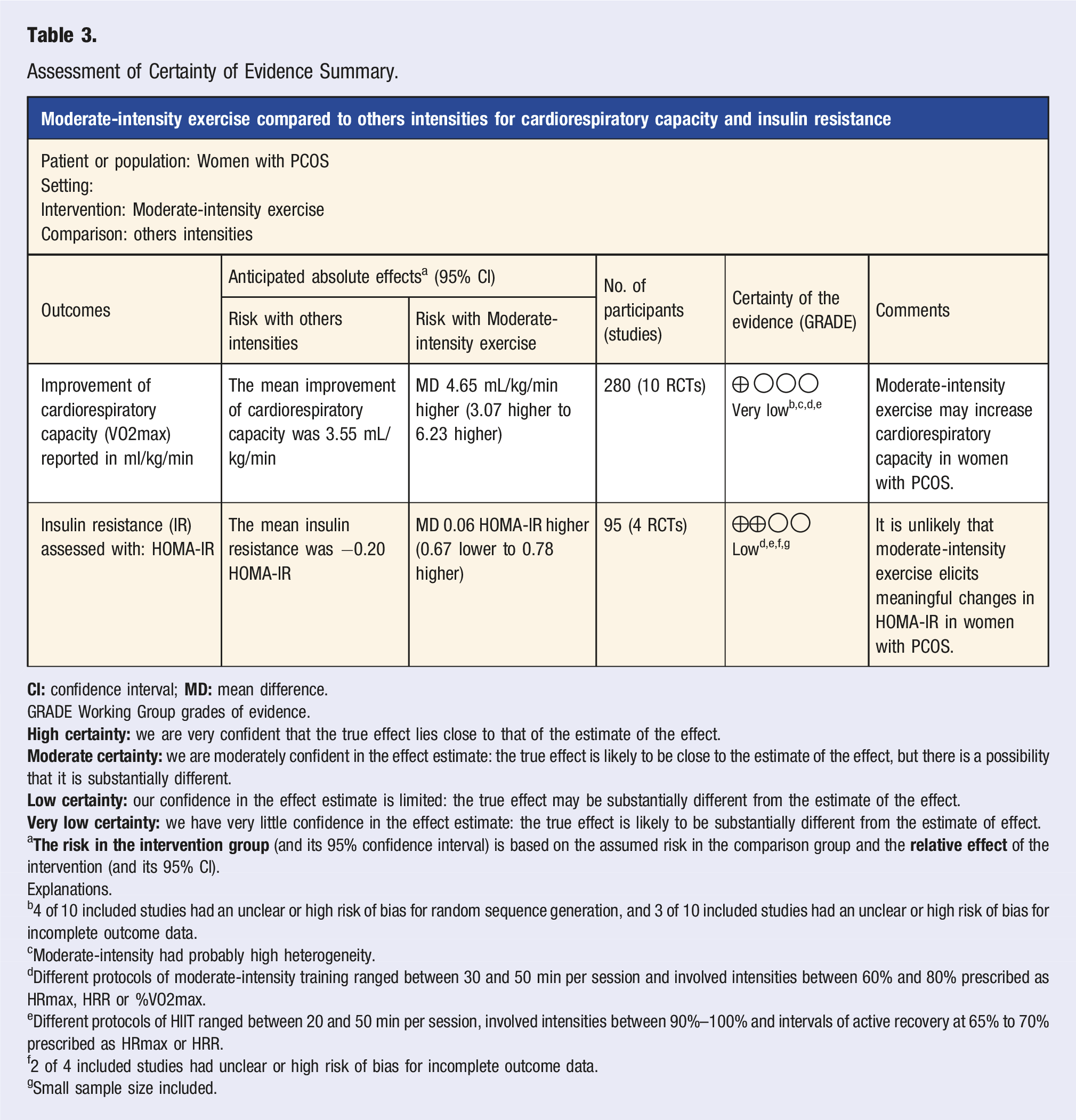
The results of risk of bias assessment by RoB2 are presented in Figure 2 Risk of bias summary by RoB2. Assessment of Certainty of Evidence Summary. GRADE Working Group grades of evidence. a Explanations. b4 of 10 included studies had an unclear or high risk of bias for random sequence generation, and 3 of 10 included studies had an unclear or high risk of bias for incomplete outcome data. cModerate-intensity had probably high heterogeneity. dDifferent protocols of moderate-intensity training ranged between 30 and 50 min per session and involved intensities between 60% and 80% prescribed as HRmax, HRR or %VO2max. eDifferent protocols of HIIT ranged between 20 and 50 min per session, involved intensities between 90%–100% and intervals of active recovery at 65% to 70% prescribed as HRmax or HRR. f2 of 4 included studies had unclear or high risk of bias for incomplete outcome data. gSmall sample size included.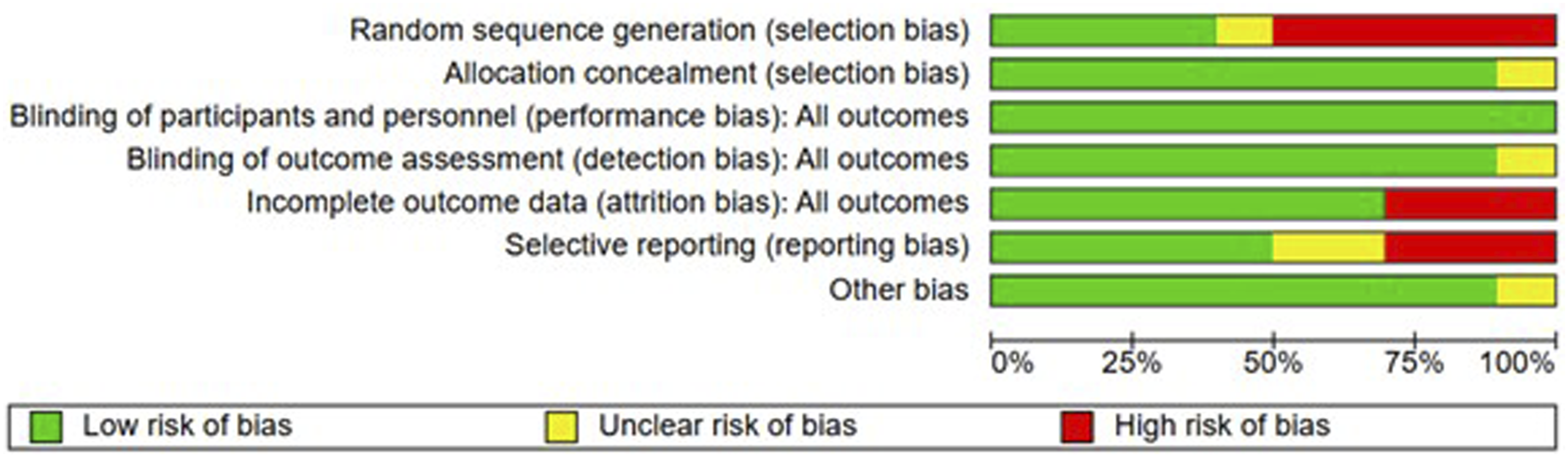
Funnel plot graph showed there was probably a high risk of publication bias in the overall report for VO2max, Figure 3A. After Egger’s test, low risk of publication bias was obtained (P = 0.238), see Figure 3B. Funnel plot symmetry showed probably risk of publication bias in HOMA-IR (Figure 3C), but Egger’s test indicated low risk (P = 0.5352; Figure 3D). Risk of publication for: (A) cardiorespiratory capacity; (B) Egger’s test for: cardiorespiratory capacity (P = 0.238); Risk of publication for: (C) HOMA-IR; Egger’s test for: (D) HOMA-IR (P = 0.5352).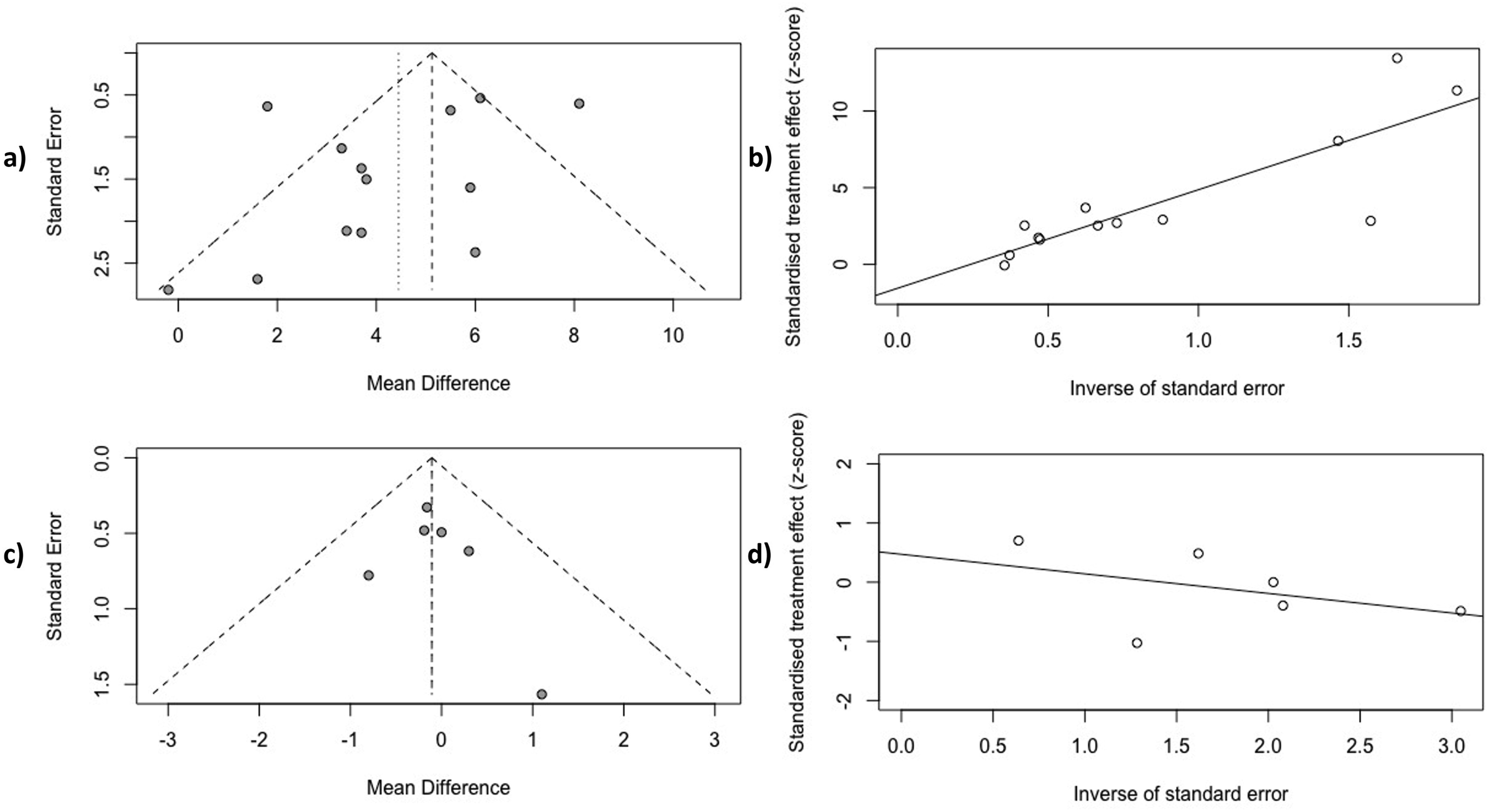
Meta-Analysis
A total of 13 interventions were included in the meta-analysis. All studies reported pre and post values for cardiorespiratory capacity (VO2max) and only 6 interventions reported additional changes on IR assessed by HOMA-IR.31,38-40
When compared with baseline, exercise significantly improved VO2max (4.45 mL/kg/min, 95% CI: 3.17-5.73, P < 0.001, I2 = 77%), see Figure 4A. After sensitivity analyses, 2 studies were removed.33,35 Nonetheless the effect size remained significant (4.61 mL/kg/min, 95% CI: 3.61-5.62, P < 0.001, I2 = 37%) Effect of exercise (pre/post) for change in: (A) cardiorespiratory capacity (mL/kg/min) n = 13; (B) insulin resistance (HOMA-IR) n = 6.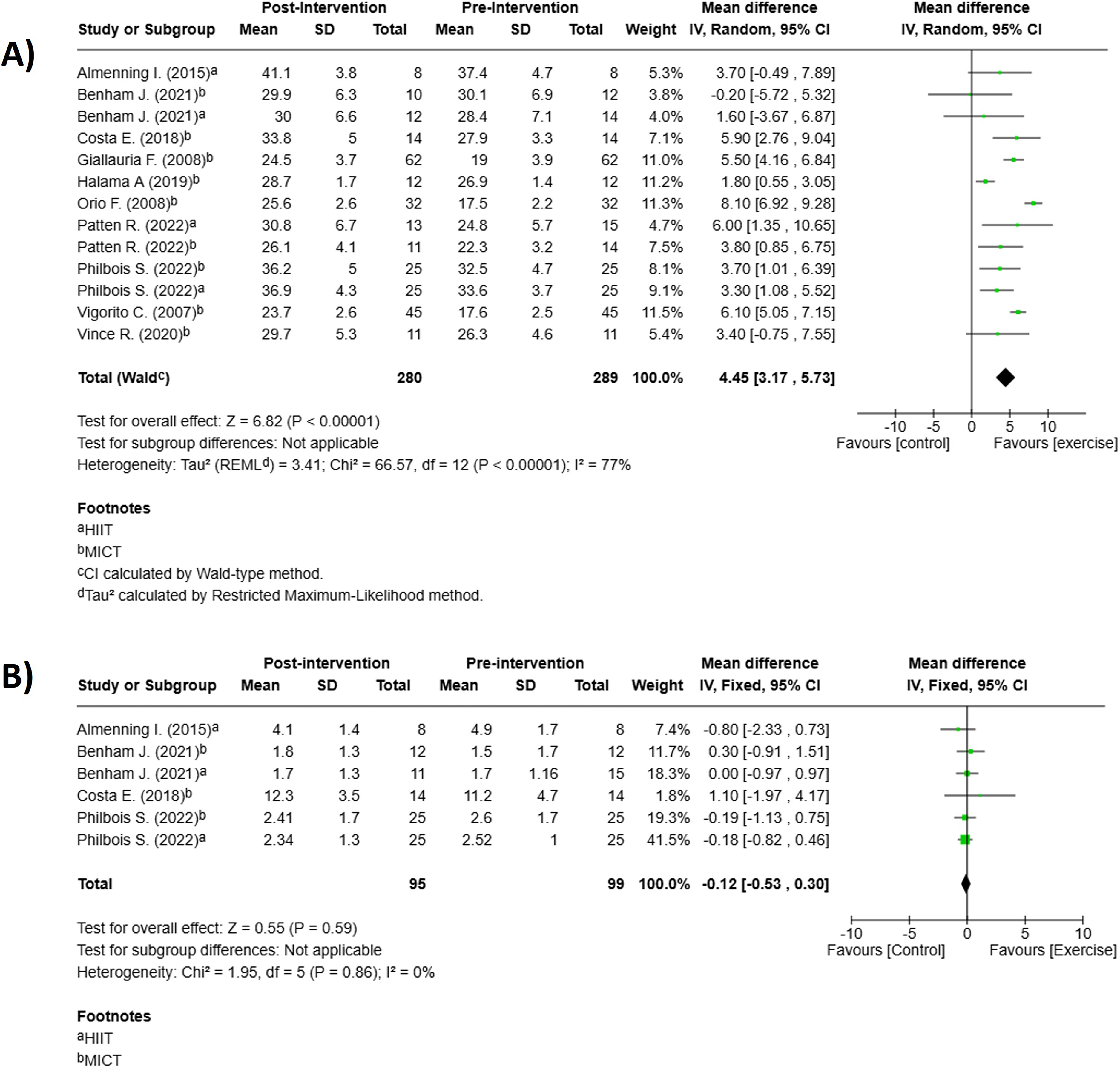
Sub-Analyses
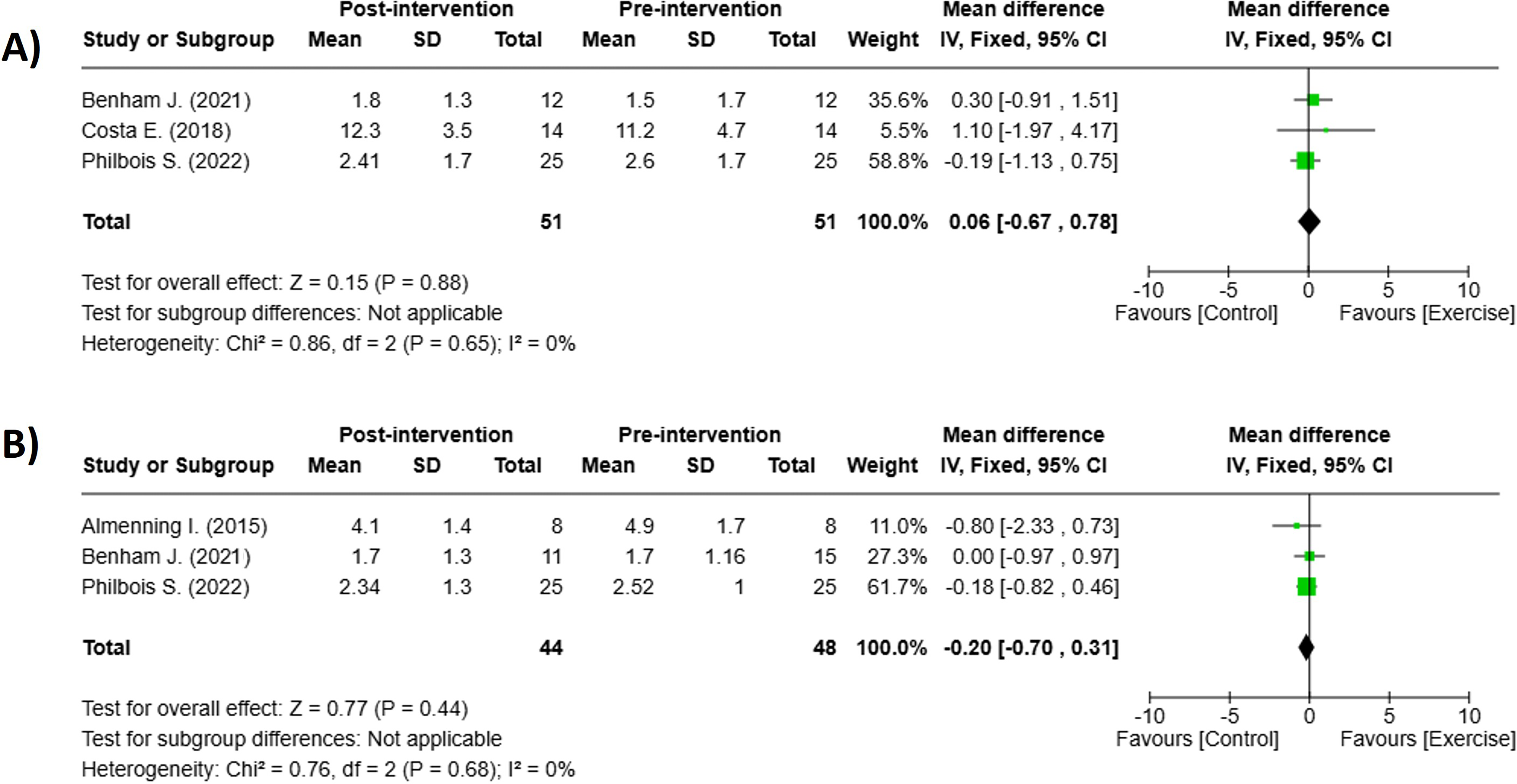
For primary outcome, 3 studies provided sufficient data to compare the effect of MICT vs HIIT on cardiorespiratory capacity.37-39 Both protocols resulted in insignificant improvements in VO2max (Figure 5). MICT: 4.65 mL/kg/min, 95% CI: 3.07-6.23 P < 0.001, I2 = 84% n = 9 Figure 5A, HIIT: 3.55 mL/kg/min, 95% CI: 1.84-5.26, P < 0.001, I2 = 0% n = 4 Figure 5B. However, neither MICT nor HIIT produced statistically significant change in HOMA-IR when compared with baseline (Figure 6). MICT: 0.06, 95% CI: −0.67-0.78 P < 0.88, I2 = 0% n = 3 Figure 6A, HIIT: −0.20, 95% CI: −0.70-0.31, P < 0.44, I2 = 0% n = 3 Figure 6B Sub-Analyses: Effect of (A) MICT (pre/post) n = 9, and (B) HIIT (pre/post) n = 4, for change in cardiorespiratory capacity. Sub-Analyses: Effect of (A) MICT (pre/post) n = 3, and (B) HIIT (pre/post) n = 3, for change in insulin resistance (HOMA-IR).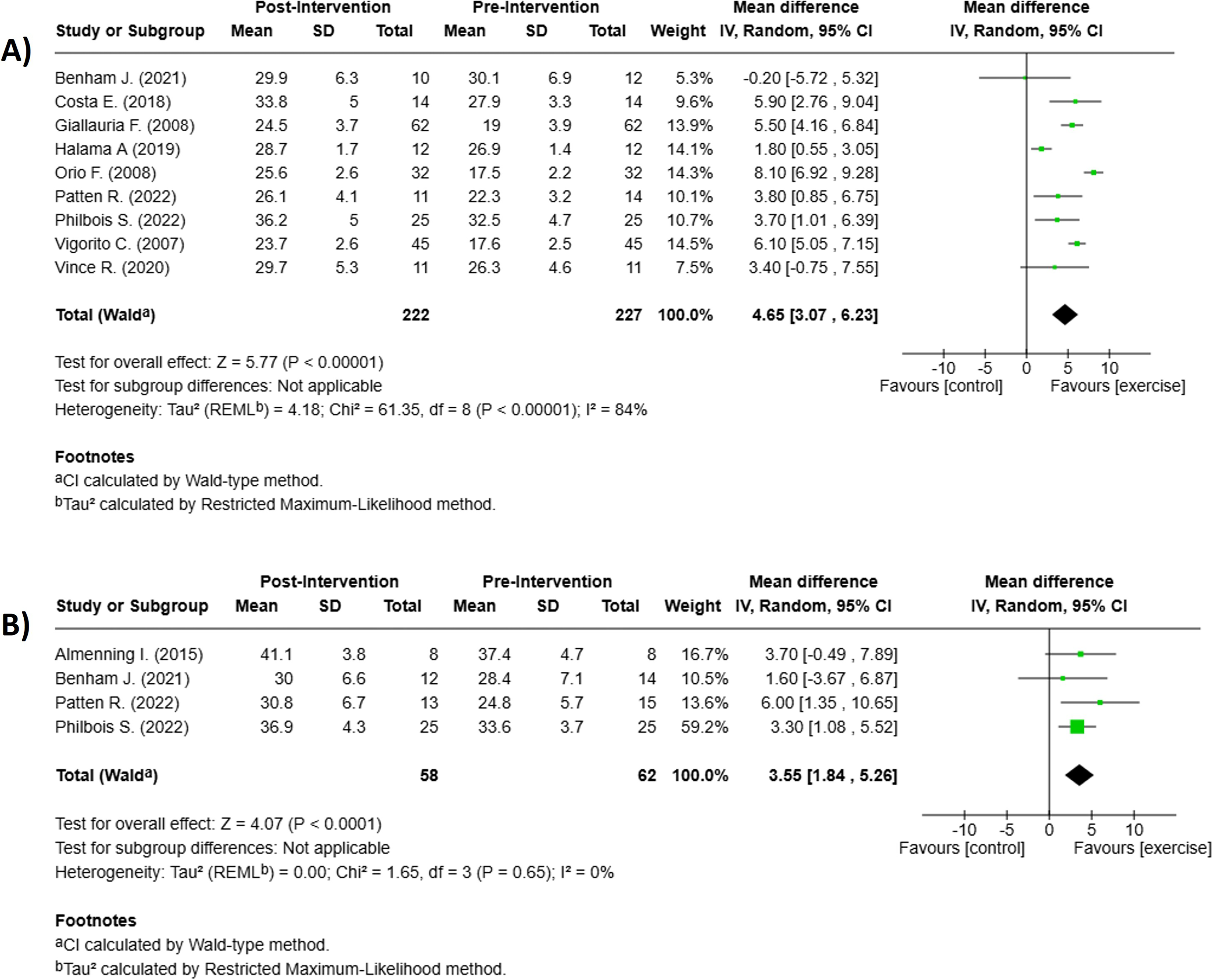
Discussion
We evaluated the effect of MICT on VO2max and HOMA-IR in comparison with different exercise protocols or no-exercise in women with PCOS. 13 protocols involving a total of 289 participants were included in the meta-analyses. When compared with baseline, results showed that exercise significantly improves VO2max. Along with other studies, this improvement may contribute to reducing cardiovascular risk 41 and risk of mortality 42 on PCOS patients. The overall results were not affected by the study of Benham et al 38 even though their 24-week intervention did not significantly change VO2max neither by MICT nor by HIIT. These results may be attributed to the reduce adherence reported in the last 3 months of the intervention (64% and 44% median exercise adherence for MICT and HIIT respectively). Despite this, most studies included in this review provide up-to-date evidence that exercise had a beneficial influence on enhancing cardiorespiratory capacity in women with PCOS.
Previous systematic reviews have shown the efficacy of exercise for improving an array of cardiorespiratory fitness outcomes. This review and meta-analysis goes beyond by providing VO2max values exclusively measured by breath-by-breath respiratory gas analysis. This direct method provides more certainty in the results to be analyzed than when indirect methods are included such as Multistage fitness test or the 6-min walking test. In the current study, changes in VO2max varied between intensities and training periods. MICT showed modest improvement in VO2max (1.80 mL/kg/min) after 8 weeks of training at 60% VO2max. 35 Greater values (8.10 mL/kg/min) were obtained after 24 weeks of a supervised aerobic exercise at similar intensities (60%-70% VO2max). 33 In that study, authors also evaluated the effects of a training program after its cessation, showing that 12 weeks of detraining resulted in a complete loss of all favorable adaptations obtained from exercise. This suggests that not only increasing training period could improve cardiorespiratory fitness but also exercise might be maintained through life for its benefits to be preserved.
Although both MICT and HIIT protocols were effective in increasing VO2max, the role of duration, intensity and frequency in mediating the favorable impact of exercise has been explored in women with PCOS. Cardiorespiratory sub-analyses suggest that greater mean difference values are obtained by MICT protocols rather than HIIT. These findings are supported by previous meta-analyses reporting larger VO2max increases with MICT (5.33 mL/kg/min, P < 0.001) than with HIIT (2.87 mL/kg/min, P < 0.001). 43
HIIT has been increasingly studied as an emerged alternative. It has been recognized as a time-efficient additional exercise to traditional endurance training by the exercise-based international guidelines for managing type 2 diabetes. 44 The current review supports its effectiveness in improving VO2max especially in protocols that involved short periods of exercise above 85% HRmax with intervals of light activity recovery. The efficacy of HIIT on cardiorespiratory capacity has been related to the improving pulmonary ability to take in oxygen for distribution to working skeletal muscle during exercise. 45 Other colleagues have proved that even in healthy sedentary subjects, a low volume of HIIT is enough to increase mitochondrial respiratory capacity in skeletal muscle with comparable adaptations to endurance training. 46 It is important to say that variability in HIIT protocols (intensity, duration, frequency, and the type of exercises employed) makes it challenging to standardize its effects on VO2max. Nonetheless, our findings suggest that HIIT is a viable strategy for improving cardiorespiratory function in women with PCOS.
Regarding the secondary outcome, we evaluated the effect of exercise on IR. Recent data has found that cardiorespiratory fitness may be strikingly impaired in women with PCOS and this may be linked to insulin resistance in overweight and obese women with PCOS. 47 Some studies have found a relationship between VO2max and HOMA-IR or some other IR markers (glucose to insulin ratio, glucose or insulin area under curve, etc.).32,33 Also, an inverse association between VO2max and HOMA index was described by using univariate and multiple regression analyses. 48 In contrast to that, the present meta-analysis showed that exercise did not significantly reduce HOMA-IR. Previous analysis 49 had also found no significant effect of exercise in the post intervention group (−0.22 mL/kg/min, 95% CI: −0.80.0.36, P < 0.004). These results may be attributed due to possible changes in the patient’s diet which were not assessed in studies and could influence the results. In managing PCOS, lifestyle modifications, involving dietary are recommended to ameliorate metabolic perturbation. When combining exercise and diet, it has proved to be more effective than exercise alone for reduction of IR. 50
Searches in overweight/obesity subjects without PCOS have found HIIT to be as effective as MICT in improving most glucose and insulin resistance markers,51,52 others have revealed a more robust increase of proteins activity related to glycolytic metabolism by HIIT when compared to continuous medium- to low-intensity exercise. 53 In accordance with that, our sub-analyses showed that women with PCOS had greater reductions in HOMA-IR after HIIT compared to MICT. The positive effect of HIIT on blood glucose has been reported in adults with IR or type 2 diabetes54,55 but also has proved its efficacy on aerobic performance, anthropometric indices and insulin sensitivity in PCOS patients. 56 On the other hand, the intensity and volume of exercise may provide distinct health benefits in women with PCOS 57 and some authors also observed improvements in insulin sensitivity parameters by MICT with enough sensitivity. In their study, 58 8-weeks exercise showed a significant improvement of VO2max in PCOS patients while healthy control did not. Yet, HOMA index did not difert between groups.
Some authors support the hypothesis that PCOS patients exhibit an abnormal mitochondrial function involved in the occurrence and development of IR and hyperandrogenism. 59 By contrast, studies examining mitochondrial changes with exercise in women with PCOS are limited and have not been able to demonstrate an improvement in mitochondrial characteristics. 60
To date, there is a gap in the knowledge about the underlying exercise response mechanisms associated with improvements in IR. Yet, the impact of either MICT or HIIT in IR suggest not to be unique in women with PCOS. Current data suggest that this response to exercise could be possibly linked to increased fat oxidation and a reduction in intramyocellular fat metabolites which would improve IR. 57 Further evidence is needed to elucidate the physiological mechanisms linked to exercise response.
Limitations
We believe this study has some limitations worth mentioning. First, the certainty of evidence for primary and secondary outcomes was very low and low respectively, limiting the strength of confidence in the recommendations that can be drawn from these studies. The quality of evidence was downgraded due to the majority of studies demonstrating unclear or high risk of bias on domains like random sequence generation and selective reporting data. Second, few studies have evaluated the effect of exercise on VO2max by direct method. Further research based on breath expired gases analysis is needed to determine exercise-induced improvements in cardiorespiratory capacity and IR in women with PCOS. Third, the included studies varied in duration, ranging from 8 to 26 weeks, and showed differences in session duration, intensity and equipment used to conduct the exercise protocols. This was particularly evident in HIIT protocols where there is considerable heterogeneity among protocols which can influence the results.
Despite these limitations, it is important to highlight that the present review incorporated a comprehensive search strategy based on international publication guidelines. Also, we included only RTCs which are considered the gold-standard design for determining causality and performed sensitivity analyses to explore heterogeneity and publication bias. Our findings provided an up-to-date synthesis of current evidence regarding the effects of MICT and HIIT interventions in women with PCOS.
Conclusions
PCOS is a common endocrine disorder affecting young women. In addition to the androgen excess, the high prevalence of IR and its association with cardiopulmonary impairment could increase the risk for cardiometabolic disease. This meta-analysis demonstrates that exercise, whether at moderate or high intensity, plays a beneficial role in cardiorespiratory capacity. In particular, MICT appears to promote greater changes of VO2max than HIIT. Such benefits may ultimately contribute to improving the metabolic and reproductive health of women with PCOS. However, HIIT also appears to be a viable alternative to MICT due to its impact on cardiorespiratory fitness. Despite the time-efficient characteristics, further evidence is needed to determine which specific HIIT protocol provides the most benefit for the PCOS population.
In addition to the fact that current studies are limited in providing a definitive intensity for exercise prescription in women with PCOS, it would also be of great interest to include studies that report diet as a relevant variable for IR.
Thought the growing interest for determining the best exercise prescriptions for women with PCOS, we consider that it’s important to not only increase their physical activity but promote adherence to lifestyle changes. Otherwise deconditioning would lead to the loss of all the beneficial effects of exercise and the clinical characteristics of PCOS could return.
Supplemental Material
Supplemental Material - Physical Exercise on Aerobic Capacity in Women With Polycystic Ovary Syndrome: A Systematic Review and Meta-Analysis
Supplemental Material for Physical Exercise on Aerobic Capacity in Women With Polycystic Ovary Syndrome: A Systematic Review and Meta-Analysis by María F. Chávez-Díaz, Briseidy Ortiz-Rodríguez, Lidia G. De León, Ramón Candia-Lujan, and Claudia E. Carrasco-Legleu in American Journal of Lifestyle Medicine.
Footnotes
Author’s Note
The corresponding author, on behalf of all co-signatories, affirms the accuracy, transparency, and integrity of the data and information presented in the study; confirms that no relevant information has been omitted; and certifies that any disagreements among the authors have been appropriately addressed and thoroughly documented.
Author Contributions
María F. Chávez-Díaz: Idea conception, data acquisition, analysis and data interpretation. Draft writing, review and editing. Final approval of the version submitted.
Briseidy Ortiz-Rodríguez: Idea conception, analysis and data interpretation, draft review and editing. Final approval of the version submitted.
Lidia G. De León: analysis and data interpretation, draft review and editing. Final approval of the version submitted.
Claudia E. Carrasco-Legleu: analysis and data interpretation, draft review and editing. Final approval of the version submitted.
Ramón Candia-Luján: analysis and data interpretation, draft review and editing. Final approval of the version submitted.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
ORCID iDs
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.