
Abstract
This paper aims to review the current literature on the prevalence of eating disorders (EDs) and their manifestations in individuals with physical disabilities (IWPD). To do this, we performed a comprehensive search of PubMed and identified 631 articles that were potentially relevant to this study. Following a title, abstract, and full-text review, 48 articles were selected. Among the 48 articles included in this review, demographics which were assessed included individuals with spina bifida, cerebral palsy, multiple sclerosis, traumatic brain injury, spinal cord injury, stroke, and athletes with disabilities. These articles were primarily case reports or cross-sectional studies that discussed anorexia nervosa, bulimia, binge eating, food addiction, pica, and sleep-related eating disorders. Upon further analysis of these articles, we conclude eating disorders and disordered eating behaviors are prevalent among individuals with physical disabilities though different disabilities often exhibit different EDs originating from different etiologies.
Keywords
“Individuals with physical disabilities have a higher prevalence of concurrent mental health conditions which may in turn put them at risk of disordered eating.”
Introduction
Among individuals with physical disabilities (IWPD), there exists higher rates of individual-reported poor body image1-9 compared to the general population. The risk of obesity is also a comorbidity highly prevalent in IWPD. 10 Reasons cited for this by the Center for Disease Control and Prevention (CDC) include inaccessible healthy food options, inaccessible exercise modalities, physical limitations due to disability that alter eating habits, medications, increased pain, a lack of resources, and decreased energy levels.11,12 Higher rates of obesity are an area of increasing concern for these individuals and are associated with the development of chronic health conditions such as hypertension, coronary artery disease, cancer, and diabetes.13-15 In addition, IWPD are also at increased risk for other mental health disorders such as anxiety and depression.16-21
Taken together, the prevalence of body image disorders, anxiety, depression, and obesity put IWPD at increased risk for eating disorders or disordered eating behaviors.22-24 These behaviors include, but are not limited to, binge eating, eating non-food substances, excessive calorie/nutrient restriction, or purging of food. While body image, anxiety, depression, and obesity are heavily studied in IWPD, there are limited collated resources available on eating disorders or disordered eating behaviors and how they manifest among IWPD.
The purpose of this narrative review is to appraise the literature focusing on disordered eating among individuals with differing physical disabilities to determine the scope of available literature on this topic. In turn this will allow us to determine gaps within the field and identify potential opportunities for future investigation. A secondary aim of this review is to ascertain what methods are currently utilized to evaluate disordered eating behaviors in individuals with a physical disability.
Methods
A summary of methods for source identification is depicted in Figure 1. Potential sources for inclusion in this narrative review were identified through a search of PubMed. Independent and MESH search terms were utilized with Boolean operators that ensured PubMed results included articles which discussed at minimum one kind of physical disability and one kind of eating disorder or behavior potentially indicative of an eating disorder as depicted in Supplemental Figure 1. Publications from any year were included and a search was conducted in June 2025. A preliminary search identified 631 articles. Inclusion criteria to identify articles required each article to (1) discuss the clinical presentation and/or prevalence of ≥1 type of disordered eating behavior and (2) utilize a sample with ≥1 type of established physical disability. Articles were excluded if inclusion criteria were not met or if articles were systematic or narrative reviews to only include original research articles. However, all narrative and systematic reviews were screened to determine if they utilized any sources which would be relevant to this research, and these sources were included in this review if inclusion criteria were met. There were no restrictions on gender, sex, age, duration of disability, type of disability, or any other demographic marker in the sample when deciding which articles to include as the goal of this review is to determine the scope of all available literature on the topic of disordered eating in individuals with physical disabilities. Article review process. Articles were identified from the PubMed database and narrowed down to a sample of 48 articles determined to be relevant to the narrative review. Articles represented in this review include case reports, retrospective chart reviews, cross-sectional studies consisting of surveys and interviews, and meta-analyses. Narrative reviews and systematic reviews were excluded so singular studies were not overrepresented in this review, but review articles were a key source of other studies which were included in the review. Articles in this review were determined to be relevant if they discussed the manifestation of one or multiple eating disorders or clinically abnormal eating behaviors in individuals with a physical disability.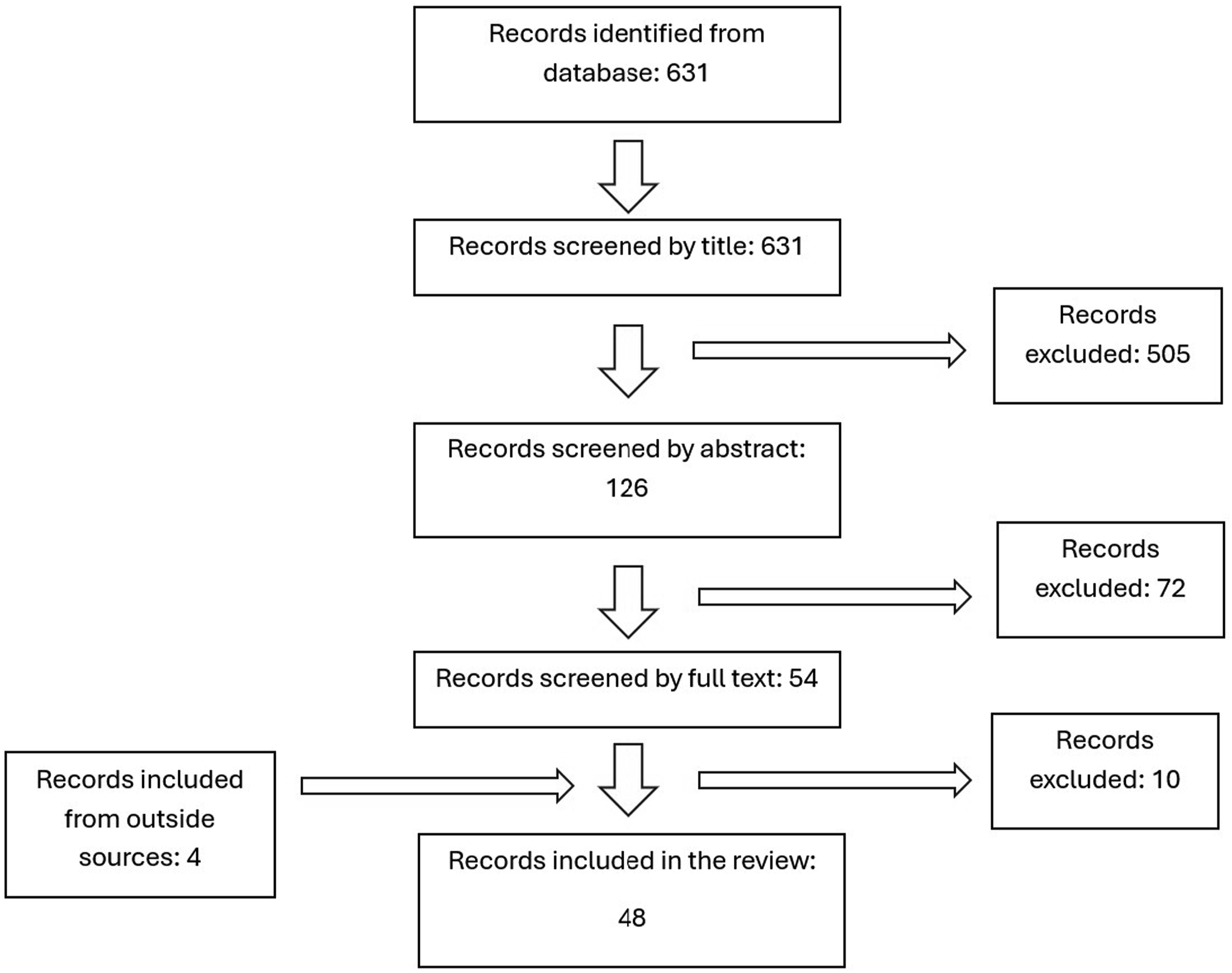
Following title and abstract screening by a single reviewer, the number of articles was narrowed down to 126 and 54, respectively. A full-text review of the 54 articles was conducted including a review of the references list of these 54 articles to identify additional eligible sources from the references lists. Full-text articles were separately screened by two researchers and the articles included in this review were approved by each reviewer. Discrepancies between the two reviewers were resolved through shared discussion of why or why not an article should be included until a unanimous decision could be made. After the full-text review, 10 articles were unincluded from the 54, but 4 additional articles from outside the PubMed database were identified, resulting in a final sample of 48 articles included in this narrative review.
For each of the 48 articles, sample characteristics (sample size, age, gender, race, and type of disability) were recorded in a database. The database also recorded the publication year, study type/methodology, presence of a control group without a disability, the use of validated eating disorder questionnaires, primary study findings, types of disordered eating behaviors discussed.
Results
Summary of Narrative Review Sources.
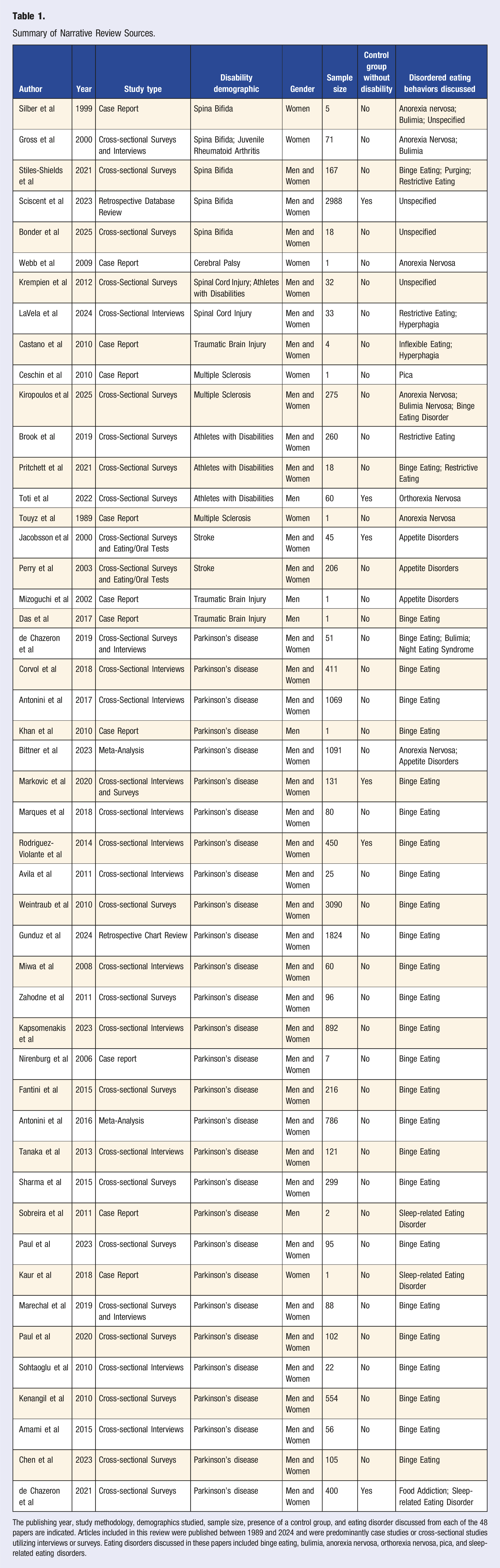
The publishing year, study methodology, demographics studied, sample size, presence of a control group, and eating disorder discussed from each of the 48 papers are indicated. Articles included in this review were published between 1989 and 2024 and were predominantly case studies or cross-sectional studies utilizing interviews or surveys. Eating disorders discussed in these papers included binge eating, bulimia, anorexia nervosa, orthorexia nervosa, pica, and sleep-related eating disorders.
Spina Bifida
Five articles were identified which highlighted disordered eating behaviors in individuals with spina bifida. Three of these articles were cross-sectional studies with surveys and/or interviews, one was a case report, and one a retrospective database review. These studies primarily evaluated the prevalence of anorexia nervosa, bulimia, binge eating, and food restriction.
Anorexia Nervosa, Binge Eating, Bulimia, Unspecified Disordered Eating Behaviors
A recent case report detailed the manifestation of eating disorders among five young women (ages ≤ 24 years) with spina bifida. 25 Two exhibited anorexia nervosa, characterized by rapid weight loss from uncontrolled restrictive dieting with associated feelings of body dissatisfaction and/or depression. One woman also reported a history of bullying and fear of exacerbation of her physical disability if she did not lose weight. Both experiences were contributing factors to the development of her eating disorder. Another case involved a woman exhibiting fasting, binging, and bulimic compensatory behaviors following a series of life stressors and onset of depression. These cases support the notion of an interplay between physical disabilities, mental health disorders, and eating disorders. The last two cases described two women with unspecified eating disorders, mainly characterized by restrictive eating patterns resulting in rapid weight loss for both and dysmenorrhea for one. The woman with dysmenorrhea concurrently had a depressed mood and accepted counseling for treatment. The other woman was admitted to the inpatient psychiatric unit and followed up in outpatient clinic for her eating disorder which resulted in improved symptomology.
Three cross-sectional studies involving individuals with spina bifida discussed behaviors of binge eating, purging, restrictive eating, excessive exercise, and bulimia. One study by Gross et al investigated solely young women aged 17 to 34 years old who either had spina bifida or juvenile rheumatoid arthritis and evaluated them with the Eating Disorder Inventory Questionnaire and a series of face-to-face interviews. 26 The women in this study (with either spina bifida or rheumatoid arthritis) reported significantly higher degrees of body dissatisfaction in 62% of the participants when compared to past state-wide surveys of body dissatisfaction among adolescent girls. Based on the results of the surveys and interviews, 8% of all participants scored in the eating disorder range for anorexia nervosa or bulimia whereas the prevalence of anorexia and bulimia among all patients presenting to their general practitioner for any reason was reported as only 0.5-2% in a prior study. 27 Further in Gross et al, in the cohort of 48 individuals with spina bifida (excluding the individuals with rheumatoid arthritis), 2% and 12.5% reached the cutoff for clinically significant drive for thinness and bulimia on the EDI respectively. Another cross-sectional study, implemented the Eating Pathology Symptoms Inventory and The Health Questionnaire, in a cohort of females and males aged 15-23 years with spina bifida. 28 This study found these individuals displayed higher levels of body dissatisfaction, purging, and food restriction behaviors compared to similarly aged females and males without spina bifida. 28 Males with spina bifida additionally displayed higher levels of body dissatisfaction. Caucasian participants had significantly higher degrees of binge eating, restricting, and body dissatisfaction compared to other racial groups in the study (African American, Asian, or Hispanic) and individuals with a VP shunt had higher degrees of purging, negative attitudes about obesity, binge eating, restricting, and body dissatisfaction. 28 The final study identified, Bonder et al, administered an online survey containing the Spina Bifida Eating Behaviors Questionnaire, Dutch Eating Behavior Questionnaire for Children (DEBQ-C), Eating Disorder Examination Questionnaire for Adolescents (EDEQ-A), and the Body Esteem Scale for Adolescents and Adults (BESAA) to 18 young adults and adolescents with spina bifida. 29 This study found that 72.2% of the sample reported a desire to change their weight and that 56% of the sample reported that their diagnosis of spina bifida contributed to their body image. The results of the BESAA further indicated the sample had clinically significantly low body self-esteem. For the individuals who reported intentionally decreasing food intake, their reported reasons for doing so were to improve body image as well as spina bifida related symptoms (pressure ulcers, bowel function, etc.). The average scores of the sample’s eating, shape and weight concerns measured by the EDEQ-A were higher compared to past samples of female adolescents/young adults without any type of disability and their degrees of external/emotional eating tendencies, measured by the DEBQ-C was also higher than a past sample of children without disabilities attending a pediatric weight loss program.30,31
No Association With Eating Disorders
A retrospective review compared the 10-year incidence of mental health disorders and substance use disorders in 1494 patients with spina bifida and 1494 matched controls without the condition, aged between 18-25 years. The presence of an eating disorder was also recorded and there was no difference no difference in the 10-year incidence (1.673% spina bifida vs 1.406% in the other group; odds ratio 1.194 with confidence interval of .665-2.142). 17 Although this study was a large cohort, the study was retrospective and the presence of an eating disorder was identified via diagnostic codes only.
Cerebral Palsy
Anorexia Nervosa
One article was identified which highlighted disordered eating behaviors in an individual with cerebral palsy (CP). 32 This article was a case report highlighting a 33-year-old Caucasian woman with CP-related mobility impairments. This individual was diagnosed with anorexia nervosa demonstrated by a fear of weight gain and uncontrolled restrictive dieting. She described her restrictive dieting was due to desires to avoid onset of urinary incontinence and to become “smaller” as means of being less of a burden to others and distance herself from support systems to feel more autonomous. To our knowledge this is the only documented report of an eating disorder in an individual with CP.
Multiple Sclerosis
Anorexia Nervosa
Three articles were identified which highlighted disordered eating behaviors in individuals with multiple sclerosis (MS). Two articles were case report of a single patient, and the manifestation of an eating disorder is different across the two reports. A third article was a cross-sectional survey design.
One of the case reports details the case of a 29-year-old woman with MS and anorexia nervosa. 33 Her body mass index (BMI) was reported as 13.92 and the individual also had emotional dysregulation, denial of her MS diagnosis, obsessive-compulsive thoughts and behaviors, and fear of separation/death. The onset of her eating disorder came after her diagnosis of MS at 21 years old, and the individual reported a lack of appropriate eating due to fear of “feeding and strengthening her MS” and exacerbating her symptoms. Recovery was successful upon admission to an eating disorders unit.
Kiropoulos et al administered the Body Shape Questionnaire and the Eating Attitudes Test-26 as well as the Big Five Inventory (measuring neuroticism) and the Rosenberg Self-Esteem Scale to a sample of 275 individuals diagnosed with multiple sclerosis. 34 The study found that 21% of the sample had a lifetime diagnosis of an eating disorder (specifically 12.4%, 9.5%, and 1.5% diagnosed with anorexia nervosa, bulimia nervosa, and binge eating disorder respectively) and 27.64% of the sample was at risk for an eating disorder. The study also identified strong, statistically significant correlations between neuroticism and poor self-esteem/body dissatisfaction and eating disorder symptoms, indicating a possible interplay and mediating relationship between these variables.
Pica, Binge Eating
The second case report details a 59-year-old woman with MS and pica preceded by a history of binge eating. 35 The woman uncontrollably ingested blackboard chalk and demonstrated a history of ingesting lime and plaster peeled off walls. Life stressors appeared to exacerbate her eating disorder, and she had a history of trauma including sexual abuse, psychological abuse, death of her first husband, and difficulties caring of her daughter, who was born with a disability. It is unclear from the article of any clear connection between the individual’s MS diagnosis and the development of pica, unlike the prior case report where a clear connection was discussed.
Traumatic Brain Injury
Three articles were identified which highlighted disordered eating behaviors in individuals with a history of traumatic brain injury (TBI). All three articles were case reports which detail the onset of an eating disorder in a total of six patients following TBI.36-38 The manifestation of eating disorders among these five patients varied and included (1) food addiction/binging/unrelenting cravings, (2) complete refusal of eating, and (3) obsessive/inflexible eating.
Food Addiction, Binging, and Cravings
The three individuals with food addiction and cravings included a 42-year-old male, a 36-year-old female, and a 22-year-old female.36,38 Das et al reported the male patient had gained 30 kg in the span of a year following an injury to both of his frontal lobes. His eating behaviors were characterized by uncontrollable cravings, excessive snacking in addition to three meals, snatching food from his children, and exhorting strangers for food. 36 The patient also exhibited increased frustration, disinhibition, and aggression following his injury; aggression would occur if his family tried to restrict his food intake. Castano et al reported on a 36-year-old woman who exhibited bilateral temporal lobe lesions, and a 22-year-old-woman had damage to the cisterns at the base of her brain as well as a frontobasal and hypothalamic infarction. 38 The 36-year-old woman exhibited hyperphagia and cravings for sweet foods and reportedly would hide food in her wardrobe. Like the male patient in Das et al, the woman also exhibited aggressive behavior and outbursts when food was not provided. The 22-year-old woman in Castano et al exhibited a “marked increased weight” since her injury and presented with hyperphagia and food cravings which did not remit following treatment with fluoxetine and topiramate. A neuropsychological evaluation found the 22-year-old woman had impaired information processing and mild executive dysfunction alongside her disordered eating behaviors.
Refusal of Eating
The individual who completely refused food included a 66-year-old male who sustained a traumatic brain injury from a motor vehicle accident resulting in a left orbitofrontal lobe contusion and a traumatic subarachnoid hemorrhage. 37 A month after the accident, the individual refused to eat and resisted any medical treatment or rehabilitation resulting in weight loss and undernourishment. After being referred to another hospital two months after the traffic accident, the patient was administered risperidone, resulting in symptom improvement within a week; the patient accepted food without resistance, agreed to participate in physical therapy, and cognitive function appeared to improve.
Obsessive Eating, Inflexible Eating
The two individuals with obsessive/inflexible eating included a 20-year-old-man and a 21-year-old woman. 38 The 20-year-old-man reported a limited appetite but a compulsive ingestion of yogurt. His BMI was 18 and he displayed cognitive inflexibility and obsessive features. His brain injury resulted in a subdural hematoma and contusions in his frontal lobe. The 21-year-old woman had a BMI of 17.5 and reported altered eating habits following her brain injury, most notably abnormal obsession of some foods and rejection of others which often changed with time. Her brain injury caused a subarachnoid hemorrhage and a left frontal acute subdural hematoma with ventricular hemorrhage.
These results also appear consistent with the results of Ciurli et al, which did not investigate explicit disordered eating behaviors, but found that individuals with TBI exhibited a greater prevalence of appetite/eating disturbances (27%) such as altered eating habits or an increased appetite compared to the prevalence of these disturbances in age matched healthy volunteers (2.6%). 39
The onset of eating disorders in individuals with traumatic brain injury is likely due to the location of injury to the temporal or frontal lobes. Uher et al reported that hypothalamic and brain stem lesions associated with appetite changes and right frontal and temporal lobe lesions associated with more complex eating disorders. 40
Spinal Cord Injury
Two articles were identified which highlighted disordered eating behaviors in individuals with a history of spinal cord injury (SCI). Both studies were cross-sectional studies with one evaluating eating disorders in veterans with SCI through semi-structured interviews and the other study evaluating eating disorders in athletes with SCI.
Fasting, Calore Restriction, Food Disinhibition, Diet Fixations
Through interviewing thirty-three veterans with SCI, LaVela et al identified five main trends regarding their samples’ eating behaviors; the three main themes pertinent to this review include extreme fasting/calorie restriction, perceived unhealthy eating behaviors, and altered eating behaviors which participants attributed to their injury. 41 The other two themes noted that some individuals still reported healthy eating patterns following SCI and that some individuals noted that their impairment created barriers to their ability to cook for themselves such as inability to grocery shop or inability to safely utilize kitchen utilities. For those who expressed restrictive eating patterns, which represented approximately two-thirds of the sample, the majority indicated a concurrent desire to manage their weight or a loss in appetite following injury. For those who reported unhealthy eating behaviors, they also occasionally indicated feelings of disinhibition around food. Many of the individuals in this group also expressed a fixation with cutting out food groups that they felt would exacerbate their physical disability such as meat, carbohydrates, and desserts. Altered eating behaviors largely involved decreased caloric intake due to their disability restricting their ability to access food and cook or due to a desire to minimize gastrointestinal distress that became more prevalent following their injuries.
Krempien et al, administered the Three Factor Eating Questionnaire to a cohort of athletes with SCI. 42 This 51-item scale assesses three factors: cognitive dietary restraint, disinhibition around food, and hunger and has proven validity in assessing eating behaviors among the general population. 43 From the results of the survey, the sample exhibited high degrees of dietary restraint, especially in men, but low levels of disinhibition around food and decreased hunger cues, indicating a possible intentional minimization of caloric intake. However, reasons for a potential minimization of caloric intake were not elicited.
While both articles discuss behaviors associated with eating disorders (disinhibition, restrictive eating, and fasting), there was no evaluation as to whether individuals were officially diagnosed with an eating disorder.
Parkinson’s Disease
Twenty-nine articles were identified which highlighted disordered eating behaviors in individuals with Parkinson’s disease. Trends identified within these articles include associations of Parkinson’s disease with compulsive eating and sleep-related eating disorders. Additionally, some of the articles discuss mediating variables that may contribute to the onset of eating disorders in individuals with Parkinson’s disease.
Binge Eating
Individuals with Parkinson’s disease are at high risk of a wide range of impulse controls disorders, including gambling, compulsive spending, and for discussion in this article, compulsive eating/binging. Articles discussing Parkinson’s disease and eating disorders which are presented in this review utilized a variety of different surveys, including the QUIP, DSM-5, Questionnaire on Eating and Weight Patterns, and Eating Disorder Examination Questionnaire, and Eating Disorder Diagnostic Scale, as well as semi-structured clinical interviews.44-71 Through these methods, compulsive eating behaviors, diagnoses of binge eating disorder, and diagnoses of food addiction were largely prevalent among the samples analyzed. Kapomensaki et al, details some of the comments made by patients in the sample when interviewed about impulse control disorders. 44 One reported incessant hunger and lack of satiety. Another commented, “I binge eat. I eat a lot of snacks […] I spend a lot of time every day thinking about food […] I can’t control myself when it comes to eating […] I lie when it comes to eating.” Another participant’s wife commented that her husband eats “all day long,” including “every sweet that he can find.”
Sleep-Related Eating Disorders
The manifestation of sleep-related eating disorders in Parkinson’s disease patients were detailed in two case reports and one case-control study. One of these details a 56-year-old woman with a history of pramipexole use. Her husband described her activities as walking into the kitchen unconsciously and eating cereal and chocolate at night. 65 The other report discusses a 28-year-old male with unconscious binge eating at night of “peculiar” food combinations including raw meat or coffee mixed with butter and then anorexia in the morning. 62 He began pramipexole six months prior to the onset of the nighttime eating episodes. The report also discusses a 37-year-old male with a history of pramipexole use who displayed both conscious and unconscious binge eating episodes at night followed by morning anorexia. Conscious binge eating episodes were of sweet foods and the participant’s wife reported unconscious binge episodes were of irregular food combinations. Although the sample size is limited, all three of the patients described in the two case reports of sleep-related eating disorders displayed a history of pramipexole use, suggesting a possible connection. A third study utilized questionnaires to understand eating disorder prevalence in 200 patients with Parkinson’s disease, of which Night Eating Syndrome was observed in 14 patients compared to only 5 patients out of 200 health controls. 71 A fourth article does not specifically describe a sleep-related eating disorder but discusses a possible connection between individuals with probable rapid eye sleep behavior disorder and onset of impulse control disorders including binge eating. 58 These additional findings continue to suggest an interconnected relationship between Parkinson’s disease, sleep, and binge eating, although a model for this relationship is unclear.
Potential Mediating Variables Between Parkinson’s Disease and Binge Eating Disorder
These articles also discuss other variables that associate eating disorder onset with Parkinson’s disease. Particularly, a strong association between dopamine agonists and the onset of impulse control disorders such as compulsive eating was demonstrated.47,49,50,53-55,57,59-62,66,67,70,72 Of these reports, some articles additionally detail a decrease in impulse control disorder following discontinuation of dopamine agonists. Only two articles discussed a lack of an association of dopamine agonists.56,71 The sample analyzed in Miwa et al also found that dopamine agonists were correlated with strong sweet cravings, even in cases without hyperphagia or binging. 72 The relationship between dopamine agonists and the onset of impulse control disorders is partially understood, with dopamine acting on various parts of the limbic system including the prefrontal cortex and amygdala to increase reward seeking behaviors and/or decrease cognitive control. 73
Deep brain stimulation, the female gender, younger age, depression, an earlier Parkinson’s disease onset, greater Parkinson’s disease severity, elevated HbA1c, smoking, restless leg syndrome and unmarried status were other variables correlated to the prevalence of impulse control disorders in Parkinson’s disease, but the degree of evidence for these correlates is much lower than that for dopamine agonists and impulse control disorders.51,56,60,61,63,66,69-71 Kenangil et al and Sohtaoglu et al both provide evidence that associate Parkinson’s disease severity, duration, age, and gender with impulsive eating which is discussed in other articles.67,68
Anorexia Nervosa, Reduced Appetite
Bittner et al was the only paper to discuss anorexia and appetite disorders in Parkinson’s disease patients. 45 The study found the acetylcholinesterase inhibitors, which are occasionally used in Parkinson’s disease treatment, are associated with anorexia and a decreased appetite. The mechanism of this association is unclear upon review of the mechanisms and pathways of which acetylcholinesterase is involved.
Stroke
Appetite Disruption, Food Aversion, Self-Consciousness About Eating
Two articles were identified which highlighted disordered eating behaviors in individuals with a history of stroke. Both studies were cross-sectional studies which included evaluation of stroke patients’ eating and oral functions and interviews. Upon review of the content of the interviews, Jacobssen et al, recognized distinct appetite changes in individuals with a history of stroke 74 with some individuals expressing that certain foods and the smell of them would make them feel nauseous, resulting in aversions to certain foods. This included meat and potatoes and desires to consume “light” foods like soup or fruit compote. Others expressed feelings of embarrassment while eating and desire to hide functional limitations while eating, such as continuously wiping excessive saliva production off their mouths. Similarly, it was difficult for some patients to ask for help to eat due to feelings of humiliation. Those with a nasogastric tube expressed especially strong feelings of humiliation when feeding, describing it as “meaningless.” Unpleasant experiences and fear of eating were also discussed; patients reported a fear of choking or pain, throat narrowing, and dryness of their mouth or throat. Perry et al also used interviews to investigate appetite of stroke patients. 75 Of 40 patients assessed, 20 described their appetite as “good” or “very good,” 3 described it as “not too bad” or “fair,” 4 described it as unchanged from before their stroke, 11 patients said their appetite was changed from before the stroke, 5 individuals reported little to no appetite, and only 1 individual said their appetite improved post-stroke.
The high rates of malnutrition in individuals with stroke, can be largely precipitated by feeding difficulties or lower energy/alertness levels. Further research is necessary to evaluate how appetite is affected following stroke and what are the main insecurities stroke individuals experience while eating.75-78
Athletes With Disabilities
Four articles were identified which highlighted disordered eating behaviors in athletes with physical disabilities. All four articles employed surveys including the Low Energy Availability in Females Questionnaire (LEAF-Q), Eating Disorder Examination Questionnaire (EDE-Q), ORTO-15, and the Three Factor Eating Questionnaire. Three of these articles included athletes with varied types of physical disabilities, including individuals with amputations, spinal cord injury, spina bifida, limb length discrepancy, cerebral palsy, poliomyelitis, and more. One of these three articles evaluated just men. The fourth article, discussed prior, solely surveyed athletes with spinal cord injury.
Restrictive Eating, Binge Eating
The articles discussing eating disorders in athletes with disabilities follows a theme of athletes partaking in excessive dieting, restrictive eating, and occasional episodes of binge eating. Toti et al specifically researched orthorexia nervosa in a sample of male wheelchair basketball athletes. 79 While no statistically significant difference was elicited in this sample vs a sample of controls without a physical disability, the study found that in the wheelchair athletes who did exhibit orthorexia tendencies, these tendencies were more associated with physical factors, such as severity of gastrointestinal esophageal reflux and hunger severity, as opposed to psychological factors, suggesting orthorexia in this demographic manifests from a desire to minimize gastrointestinal and starvation symptoms rather than from desires to alter their body appearance. Brooke et al and Pritchett et al conducted questionnaires on athletes with disabilities and came to similar conclusions surrounding unhealthy eating behaviors in their samples.80,81 In Pritchett et al, 54 participants were administered the Eating Disorder Examination Questionnaire which indicated only one female participant was “at risk” of an eating disorder. 81 However, one participant described feeling a compulsive desire to burn calories to alter their body composition and another described a desire to cut calories to fit into their wheelchair. Four athletes described eating unusually large quantities of food on occasion within the prior month and one patient described a discrete binge eating episode lasting four days. The Low Energy Availability in Females Questionnaire administered to the female participants in the sample found that 78% of them were at risk of low energy availability based on their menstrual history and physiological symptoms. Brook et al administered surveys to 260 athletes with disabilities. 80 Of this sample, 32.4% had elevated Eating Disorder Examination Questionnaire (EDE-Q) pathologic behavior subscale scores although only 3.1% had officially reported a prior eating disorder, indicating improved eating disorder screening is necessary in this population. Athletes indicated a desire to alter their weight and body composition to improve at their sport. Forty-four percent of premenopausal females had oligomenorrhea/amenorrhea. Weight concerns were especially present in the sample, with at least one-third of all individuals with a physical disability (spinal cord injury, cerebral palsy, acquired central neurological injury, lower extremity amputation, and upper extremity amputation) reporting a pressure to maintain a specific body weight. Demographics that were disproportionately affected by this pressure included females with cerebral palsy (71.4%) and males (66.7%) and females (57.1%) with acquired central neurologic injury. Bone stress injuries, a possible result of malnutrition, were especially prevalent in those with spinal cord injuries; individuals with spinal cord injuries accounted for 20% of all bone stress injuries recorded in the sample.
Discussion
This is the first narrative review to our knowledge providing an overview of eating disorders in IWPD. From this review, it is clear there are associations between the presence of a physical disability and disordered eating behaviors. However, there is a need for larger scale studies that examine the presence of eating disorders and the potential reasons for their increased prevalence in certain individuals with physical disabilities. This is especially true for individuals with a history of stroke, SCI, MS, CP, and athletes with disabilities. A possible interplay between having a physical disability, impact on mental health, body dysmorphia, and onset of an eating disorder may exist for many individuals irrelevant of disability type.
This relationship may be facilitated by a variety of factors. For one, individuals with disabilities often exhibit mobility limitations, chronic pain and fatigue resulting in an impaired ability to exercise and modify body composition through physical activity.82-86 As such, individuals with physical disabilities may focus more on diet rather than physical activity to improve their body image. Individuals with physical disabilities also may have an impaired ability to access, prepare, or physically chew or swallow food which possibly results in various pathologies such as malnutrition, food restriction due to distaste for available food, or binge eating when desirable food becomes available.87,88 Lastly, individuals with physical disabilities have a higher prevalence of concurrent mental health conditions which may in turn put them at risk of disordered eating.89-93
The second aim of this study was to identify the ways in which eating disorders are quantified and characterized in individuals with disabilities. We found that no standard methodology is employed, with a wide variety of surveys and interview techniques being used in clinical practice. Further research should investigate the accuracy and validity of these questionnaires in measuring disordered eating behaviors in this demographic.
There are several limitations to this research. First, most articles included in this review are case studies or cross-sectional studies with limited sample sizes. These articles are also heterogenous, evaluating a wide range of ages, genders, and disability types and utilizing a wide range of study methods, resulting in a difficulty to synthesize findings and identify trends within the data. The lack of consistency in measurement tools used to assess disordered eating and consistent validated assessment tools makes assessing the true prevalence of this issue challenging.
The present review provides a foundation that investigators can use to identify future areas of need in this realm to promote earlier identification, prevention, and successful treatment of eating disorders in individuals with physical disabilities.
Supplemental Material
Supplemental Material - Disordered Eating Behaviors in Individuals With Physical Disabilities: A Narrative Review
Supplemental Material for Disordered Eating Behaviors in Individuals With Physical Disabilities: A Narrative Review by Emma Raffman and Prakash Jayabalan in American Journal of Lifestyle Medicine
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Dr. Jayabalan receives support from the National Institute of Aging, Claude Pepper Center 1P30AG059988-01A1.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.