
Abstract
“Our findings reveal that women can rely on the involvement of close others, regardless of relationship type, in their day-to-day disease management.”
Introduction
Women’s heart health and health care are vital research areas, 1 with growing recognition of distinct health and illness trajectories of female patients. As rates of acute myocardial infarction are increasing in young women, 1 greater attention to women’s cardiovascular health and health care is especially warranted. In this study, we investigate women’s perceptions of involvement of their care partners in their disease management following participation in cardiac rehabilitation.
Following a cardiac event, participation in cardiac rehabilitation can enhance patients’ recovery and promote disease management. 2 Cardiac rehabilitation combines evidence-based health promotion interventions with supervised exercise training. 2 Although cardiac rehabilitation is an effective tool to improve health outcomes following a cardiac event, 3 female patients continue to experience lower quality of life and poorer functional outcomes compared to their male counterparts. 4 It is imperative to illuminate factors that may account for these gender disparities in patients’ health outcomes.
One factor that may account for gender differences in patients’ health outcomes is the availability of a care partner who is actively involved in promoting their heart disease management. Notably, women participating in cardiac rehabilitation are less likely to be married than are men. 5 Prior work has demonstrated health benefits of care partner support for patients’ disease management, particularly involvement of spouses.6-8 Of note however, spousal involvement is not uniformly beneficial, as some well-intentioned but unhelpful behaviors—such as overinvolvement and social control—can negatively affect disease management.7,9 Importantly, far less attention has been given to care partners other than spouses, and particularly, to how they may be involved in health-related activities to promote women’s heart disease management.
In this study of women’s heart health, we first examine differences in participant and care partner characteristics between women who identify a spouse care partner and those who identify another network member (non-spouse care partner). Next, we examine differences in care partners’ (spouse and non-spouse) involvement in women’s health-related activities. Drawing upon the broader literature delineating the health benefits of spouse involvement in disease management, 9 we anticipate that women with a spouse care partner will report more involvement of their care partner than will those with a non-spouse care partner.
Methods
Participants
Women managing heart disease were recruited to participate in one of two pilot studies. Participants from one pilot study (study 1: interview study, n = 32 women; data collected between August 2022 and July 2023) were recruited from hospital-based outpatient cardiac rehabilitation centers in central Indiana. Participants from the second pilot study were recruited through the Prolific platform (study 2: online survey study, n = 22 women; data collected between November and December 2023). The total sample of 54 women included those who (1) had participated in outpatient cardiac rehabilitation; and were (2) 40 years of age or older, (3) residing in the United States, and (4) able to read and respond in English. The University Institutional Review Board approved all study procedures, and all participants provided informed consent before participating in either study.
Measures
Participant Characteristics
Participants were asked to provide their age, race/ethnicity, current employment status, and marital (or partner) status. Participants reported self-rated health on a 5-point scale (1 = “poor” to 5 = “excellent”). Self-rated health was dichotomized to group “excellent” and “very good” together and “good, fair, and poor” together. Functional capacity was assessed with one item to describe participants’ ability to do physical activity (1 = “can perform all activity without getting short of breath, tired or having palpitations”; 4 = “I feel breathless at rest and am mostly housebound”). 10
Care Partner
Participants were first asked to identify individuals close to them who help them with managing their heart disease (care partners). In this investigation, we focus on the care partner who women identified as the person who helps them the most (i.e., primary care partner). Women’s reports of relationship with this care partner (i.e., spouse, adult child, sibling, other) were dichotomized as spouse or non-spouse. Participants reported whether or not they resided with their care partner. Participants also rated the quality of their relationship with the care partner using an adapted version of the 5-item Quality of Marriage Index (1 = strongly disagree; 7 = strongly agree) (α = .88). 11 Example items include, “You have a good relationship” and “You really feel like part of a team with your partner.” Responses to these items were averaged.
Care Partner Involvement
Participants reported whether (yes or no) care partners were involved in aiding them with health-related activities to properly manage their heart disease. These health-related activities included: assistance with maintaining a healthy diet and regular exercise (assessed separately), monitoring blood pressure, and accompanying them to healthcare appointments.
Analytic Strategy
Data were analyzed using SPSS version 28 with statistical significance set at P < .05. To characterize the sample, descriptive statistics (frequencies, means, standard deviations) were calculated for demographic data and survey responses. Chi-square and independent sample t-tests were used to test differences between reports of women with a spouse as their care partner and those with a non-spouse care partner.
Results
In our investigation of care partner involvement in women’s heart disease management, data from participants in two pilot studies comprise the current analytic sample. Participants in our two pilot studies (i.e., interview study and online study) differed in several ways. Women who participated in our interview study were significantly older (M = 70.6, SD = 9.2 vs M = 54.8, SD = 8.2; t(52) = 6.5, P < .001), fewer were currently employed (40.6% vs 59.1%; X 2 (1) = 16.3, P < .001), and more reported living with their care partner (56.3% vs 40.6%; X 2 (1) = 9.05, P < .01) compared with those from the online study.
Participant and Care Partner Characteristics (Participant Reports).
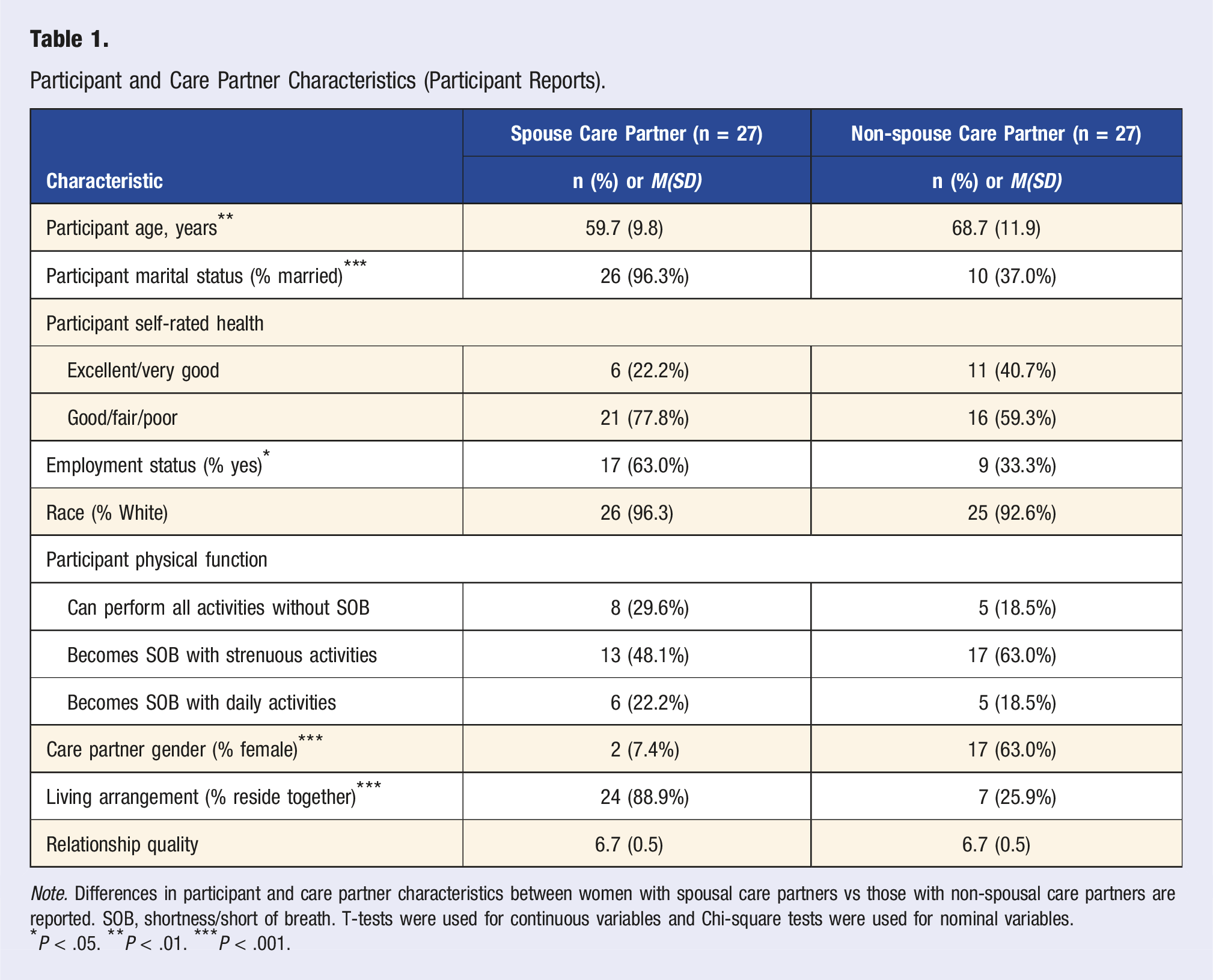
Note. Differences in participant and care partner characteristics between women with spousal care partners vs those with non-spousal care partners are reported. SOB, shortness/short of breath. T-tests were used for continuous variables and Chi-square tests were used for nominal variables.
*P < .05. **P < .01. ***P < .001.
Care Partner Involvement in Health-Related Activities (Participant Reports).
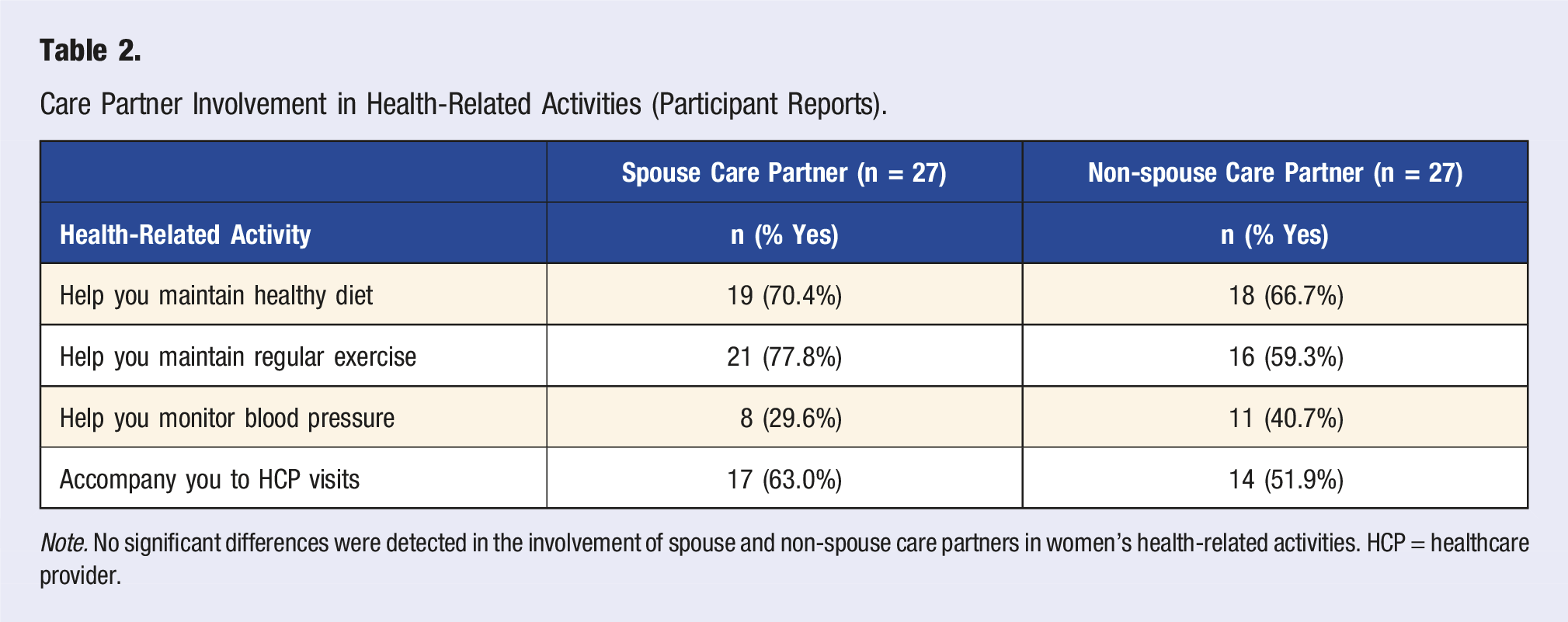
Note. No significant differences were detected in the involvement of spouse and non-spouse care partners in women’s health-related activities. HCP = healthcare provider.
Discussion
We examined care partner characteristics and involvement in health-related activities as reported by women managing heart disease. Consistent with previous research, our findings highlight the role of spousal support in the context of illness management, 9 and also reveal the role of non-spouse care partners in the management of heart disease among female patients. These findings illuminate active care partners from women’s broader social network and underscore the importance of considering their involvement in research and interventions to promote women’s health. 12
Findings revealed that women with non-spouse care partners are generally older and more likely to live apart from their care partner compared to those with spouse care partners. This demographic insight is crucial for understanding the context in which non-spouse care partners operate and underscores the need for tailored support strategies that address the specific challenges faced by older women and their care partners. Notably, women participating in cardiac rehabilitation are less likely to be married than are men, 5 and women managing heart disease often report challenges with prioritizing self-care and management among other responsibilities (i.e., those pertaining to family and household roles). 13 In addition to these factors, delineating who is involved in women’s heart disease management and what these care partners do to facilitate vital health-related activities is essential to inform high-quality social network interventions that enhance the quality and quantity of life of women with heart disease. 14
Our findings align with prior work12,14 in recognizing the involvement of spouse and non-spouse care partners to older adults managing chronic illness. It merits mention that non-spouse care partners (i.e., adult children, siblings, and friends) were more often women than men, consistent with the larger caregiving literature. 15 Women who provide care are more likely than men to prioritize this role over other demands (e.g., work) and to engage in direct, hands-on care. This difference in care partner gender may explain, in part, the finding of no significant difference in involvement of spouse and non-spouse care partners in women’s health-related activities. Importantly, our findings reveal that women can rely on the involvement of close others, regardless of relationship type, in their day-to-day disease management.
Recognizing the role of care partners in women’s disease management activities not only benefits women’s health, but it also can bolster the capability of care partners. For some care partners, their involvement in disease management marks the start of a caregiving journey that gradually involves more frequent, and more personal, care tasks. 15 As described in the chronic disease care trajectory, 15 care responsibilities may advance from sporadic disease management activities to tasks that require regular involvement, and eventually, to intensive, long-term caregiving demands. For instance, care partners may offer to assist to a family member or friend who requires frequent medical visits. Attendance at these medical visits may lead to their discovery of other needs for assistance, such as aiding their family member in preparing healthier meals or monitoring their blood pressure, which then prompts an increase in their involvement in chronic disease management. Acknowledging care partners who are engaged in assisting family members with routine disease management tasks can be an opportune time to provide early support and tailored interventions to help them prepare them for potential increases in care provision.
Involvement of spouses in their partners’ disease management is well-recognized, and several couple-level interventions have been developed to capitalize on spouses’ involvement.9,16 Less attention has been paid to other family members or friends (non-spouse care partners) who assist an older adult with disease management. Of note, one investigation identified non-spouse companions who accompanied older adults to medical visits. 17 Companions at medical visits most often were adult children, but siblings and grandchildren also accompanied older adults to medical visits. Importantly, many of these companions reported additional care responsibilities prior to and following the medical visit. Probing companions’ current levels of involvement provides an opening for healthcare providers to share resources that can boost their efficacy and help them prepare for expanded responsibilities for care, if circumstances require. Such opportunities to educate and prepare potential caregivers aligns with a recent recommendation to prepare all adults for caregiving, including information about caregiver roles and responsibilities and basic caregiving skills. 15 In particular, training and resources designed specifically for non-spouse care partners could help prepare both caregiver and care-recipient for what may be an unexpected shift in their established relationship.
Findings of this study should be considered in the context of notable limitations. First, the limited diversity of this sample (predominantly White women) may affect the generalizability of the findings. Future studies should include a more diverse sample to determine whether the involvement of non-spouse care partners varies across demographic groups. This consideration will provide a more comprehensive understanding of care partner involvement in disease management and related health outcomes. This study is also limited by reliance on brief self-report measures, given the pilot nature of our studies. Specifically, the use of dichotomous response options (yes or no) for care partner involvement for health-related activities limits the ability to capture the frequency and quality of involvement. This limitation could explain the unexpected finding that care partner involvement did not differ by care partner role. In future work, researchers should consider assessing how often or how much care partners are involved in women’s health-related activities. In addition, this study used self-report measures only from the perspective of the women managing heart disease, which can have inherent biases. Reports from care partners also are needed to better understand how they view their involvement in women’s heart disease management.
Despite noted limitations, our investigation contributes to understanding women’s perspectives of care partner involvement in health-related activities essential to managing heart disease. Our findings suggest an opportunity to more fully acknowledge and engage network members who are involved in promoting women’s health and recovery in future research, clinical practice, and public health interventions. Implications for cardiac rehabilitation and intervention include expanding efforts to recognize and engage non-spousal care partners in supporting women’s heart health. Programs should consider flexible strategies that account for varied living arrangements and relationship dynamics, particularly for older women who may rely on adult children, siblings, or friends for disease management support. Leveraging the involvement of members of women’s broader social network can galvanize available support for disease management, ultimately improving health outcomes and quality of life for female patients with heart disease.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was funded with support from the Indiana Clinical and Translational Sciences Institute, which is funded in part by Award Number UM1TR004402 from the National Institutes of Health, National Center for Advancing Translational Sciences, Clinical and Translational Sciences Award. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Ethical Statement
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.