
Abstract
‘Improvements in BP responses after 2, 3, or 6 months of CR have been reported in cardiac patients with and without heart failure.’
Introduction
Cardiovascular disease (CVD) represents one of the leading causes of death in men and women, and coronary artery disease (CAD) is the most prevalent etiology (63%). Myocardial infarction (MI) accounts for 38.5% of all CVD deaths and is more prevalent in men (62%) than women (38%). 1 A traditional 12-week exercise-based cardiac rehabilitation (CR) program provides a safe and effective treatment intervention for patients with CVD and has consistently been shown to reduce mortality, blood pressure (BP), CVD risk factors, and associated hospital admissions.2-5 Exercise-based CR also increases functional capacity and walk test performance distance in men and women.6-11 Some studies suggest that the post-CR improvements in functional capacity and walking distance are greater in men than women.7,10 Gee et al 10 evaluated whether the improvement in functional capacity following exercise-based CR varied between men and women with ischemic heart disease and reported that men demonstrated greater increases, expressed as peak metabolic equivalents (METs). Similarly, Gupta et al 7 found that men covered greater distances in walk performance tests than women following CR. In contrast, O’Farrell et al 12 reported no difference in functional capacity improvements between men and women after 3 months of exercise-based CR.
The 6-Minute Walk Test (6MWT) provides a safe and simple field test that is widely used in CR to estimate functional capacity in cardiac patients with and without heart failure.6-8,13 Improvement in timed walking distance following exercise-based CR provides an independent predictor of prognosis after MI in men. 9 Moreover, slower gait and walking speeds are strong predictors of increased mortality in men and women.14,15 Yazdanyar et al 14 evaluated the association between 6MWT performance and all-cause mortality, coronary heart disease (CHD) mortality, and incident CHD in 1665 participants enrolled in the Cardiovascular Health Study. During an 8-year follow-up, there were 305 CHD events, 100 CHD deaths, and 504 all-cause deaths. Participants in the bottom 2 6MWT quintiles (<290 m and 290-338 m) demonstrated an increased all-cause mortality, with hazard ratios of 2.1 and 1.7, respectively.
Improvements in BP responses after 2, 3, or 6 months of CR have been reported in cardiac patients with and without heart failure.8,16-18 Ghashghaei et al 8 evaluated the effectiveness of a CR program on walk test performance and BP responses in patients who had undergone coronary artery bypass graft surgery. After 2 months of CR, the study cohort demonstrated a 19.2% increase in the 6MWT, an 11% reduction in resting systolic BP (SBP), and a 9% decrease in diastolic BP (DBP). Moreover, maximal SBP and DBP were significantly lower following CR. Another randomized controlled study of 118 coronary patients (99 men, 19 women) who were postcoronary angioplasty reported a 4.7% reduction in resting SBP in the training group after 6 months of exercise-based CR. 17 A systematic review and meta-analysis that included 48 studies and 8940 patients revealed that SBP was significantly reduced following CR (weighted mean difference = −3.2 mm Hg; 95% CI: −5.4 to −0.9 mm Hg); however, DBP remained unchanged (weighted mean difference = −1.2 mm Hg; 95% CI: −2.7 to 0.3 mm Hg). 3 A previous report in cardiac patients completing a 3-month CR program found 3.6% and 2.9% reductions in SBP and DBP, respectively, and attenuated exercise heart rate (HR) and SBP responses. 16 HR recovery after a 6MWT serves as a powerful prognostic indicator in heart failure patients with reduced and preserved ejection fraction. 18 Recently, a significant reduction of 6.2 mm Hg in resting SBP was reported in a randomized controlled trial involving 115 cardiac patients who completed 36 and 24 exercise and educational sessions, respectively. 19
An age-related decrease in cardiorespiratory fitness has been reported in the general population.20,21 Therefore, we hypothesized that age would be inversely related to cardiorespiratory fitness as estimated by the 6MWT in CR patients. Because few data are available regarding changes in 6MWT performance and associated BP responses in men and women following exercise-based CR, the present study examined these variables in age-adjusted cardiac patients before and after a 12-week intervention.
Methods
Participants
We conducted a retrospective chart review of 311 cardiac patients (237 men, 74 women; aged 57.7 ± 13 years), with height 1.67 ± 0.9 m, body weight (BW) 75.3 ± 13.0 kg, and body mass index (BMI) 26.9 ± 3.9 kg/m2, enrolled in a university-based CR program in Costa Rica over 9 years (January 2009 to December 2017). Files were reviewed for demographic information, and patients were assessed before (Pre) and after (Post) the 12-week CR program on the 6MWT, with specific reference to the following variables: resting HR, SBP, resting DBP, post-6MWT HR, post-6MWT recovery HR, and post-6MWT BPs. The study was conducted according to the principles of the Declaration of Helsinki, Fortaleza, 2013. Participation was voluntary, and the experimental procedures, risks, and benefits were explained to each patient. Patients signed an informed consent form before undergoing field testing (6MWT) and the exercise-based CR intervention.
Instruments and Procedures
CR Program Design and Exercise Protocol
All exercise training sessions were conducted in a traditional 12-week outpatient CR program and were monitored with continuous electrocardiographic (ECG) telemetry (Quinton Q-Tel RMS, Cardiac Science, Bothell, WA) and supervised by a family physician and an exercise specialist. The prescribed exercise duration was 20 to 45 minutes per session, with weekly increments of 5 minutes until a total duration of 45 minutes was achieved. The CR program was offered 3 times per week at an intensity of 40% to 80% of VO2 reserve using a treadmill (Quinton Medtrack CR-60, Cardiac Science, Bothell, WA) and a cycle ergometer (Monark 828E, Monark Exercise AB, Vansbro, Sweden). Exercise intensity was adjusted using the HR reserve method, Borg rating of perceived exertion scale (11-13), or the resting HR (+20 to 30 beats per minute) in patients taking β-blockers. In addition, patients participated in a lifestyle management education class once per week. Educational topics included the following: CVD management, medications, a cardioprotective diet, stress management, and recommendations regarding the progression of physical activity.
6MWT and Hemodynamic Responses
Patients performed the 6MWT according to a standardized protocol as previously described. 22 Resting HR, SBP, DBP, and an ECG rhythm strip were obtained before each test at baseline (Pre) and following the 12-week CR program (Post). Accordingly, patients were instructed to remain comfortably seated for 5 minutes before measurements of HR and BP were obtained, without crossing their legs, back fully-supported in the chair and left arm at the heart level. BP was measured using a sphygmomanometer (Welch Allyn, MI) with an appropriate cuff size for each patient. Subsequently, patients walked in a 10-m outdoor hallway for 6 minutes with the goal of covering as much distance as possible. HR, SBP, and DBP responses to exercise were measured immediately after and 5 minutes following completion of the 6MWT.
Statistical Analysis
All data were analyzed using an IBM SPSS statistical package, version 24.0. Descriptive statistics are presented as means and SDs. The 2 by 2 (Gender × Measurement) analysis of covariance (ANCOVA) using age as a covariate was computed to determine differences in selected variables (BW, BMI, resting HR, SBP, DBP, 6MWT distance, and post-6MWT HR, BP, and recovery hemodynamic responses). Pretest to posttest measurement changes (Δ%) and effect sizes (ESs) were also computed. Age quartiles were defined by the following age distribution: Q1 (≤49.9 years), Q2 (50 to 59.9 years), Q3 (60 to 66.9 years), and Q4 (≥67 years). Pearson correlations were computed between the number of sessions completed and changes in hemodynamic variables. Statistical significance was set a priori at P ≤.05.
Results
Baseline characteristics of the cardiac patient population (n = 311) are presented in Table 1. Overall, patients improved their 6MWT distance by 29.8% (P < .001; ES = 1.25), reduced their resting SBP by 3.6% (P < .001; ES = 0.23), and decreased the corresponding DBP by 3.0% (P < .001; ES = 0.20) following the 12-week CR program. No significant changes were observed for BW, BMI, and resting HR. Significant between-gender changes were observed only for SBP following the 6MWT. Significant within-gender changes were observed on the 6MWT, post-6MWT HR, SBP, and DBP in both men and women, and post-6MWT SBP and recovery HR only in men (Table 2 and Figure 1).
Baseline Characteristics of the Cardiac Patients, by Gender. a
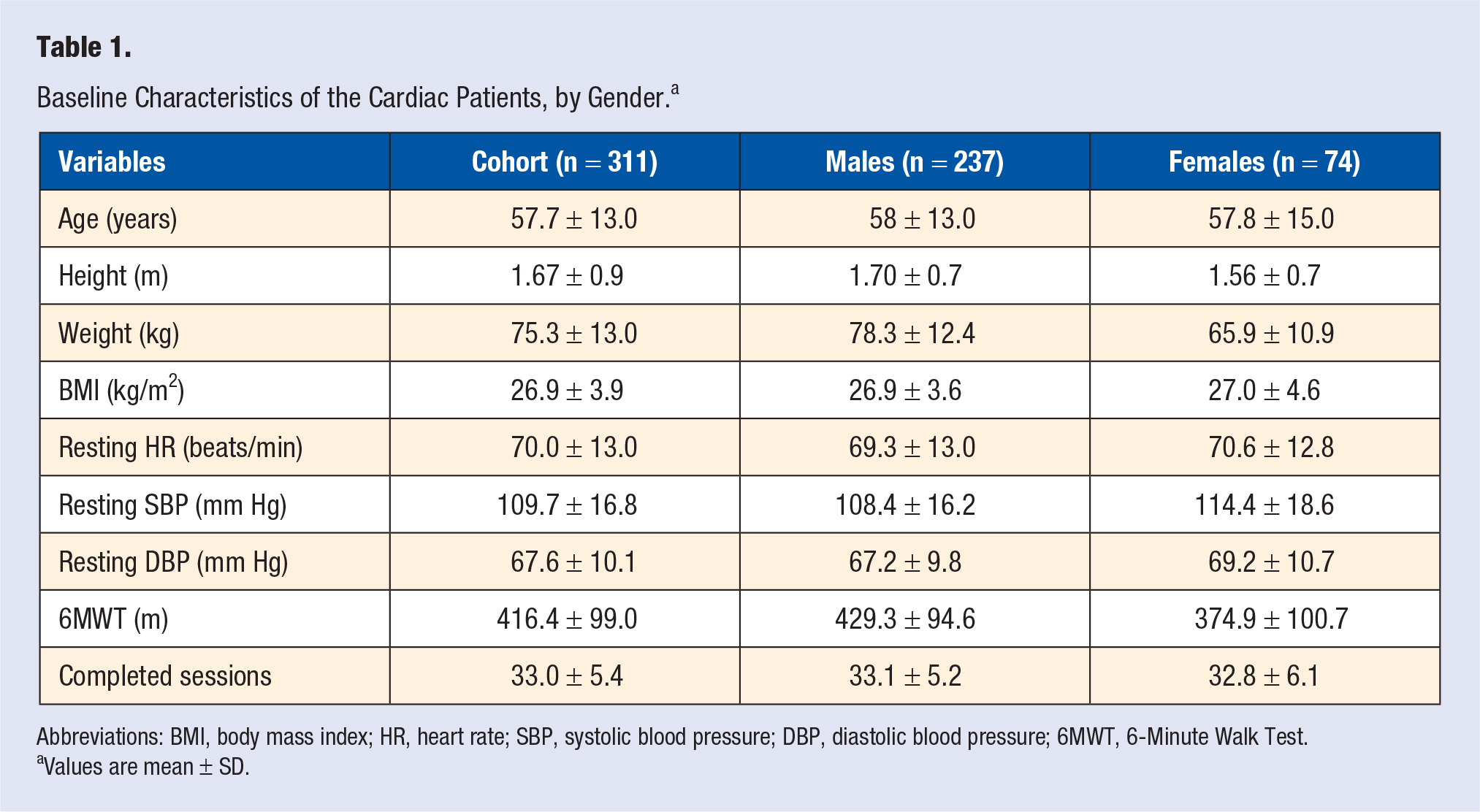
Abbreviations: BMI, body mass index; HR, heart rate; SBP, systolic blood pressure; DBP, diastolic blood pressure; 6MWT, 6-Minute Walk Test.
Values are mean ± SD.
Outcome Differences Between the Patients by Gender Before and After the CR Program (n = 311). a
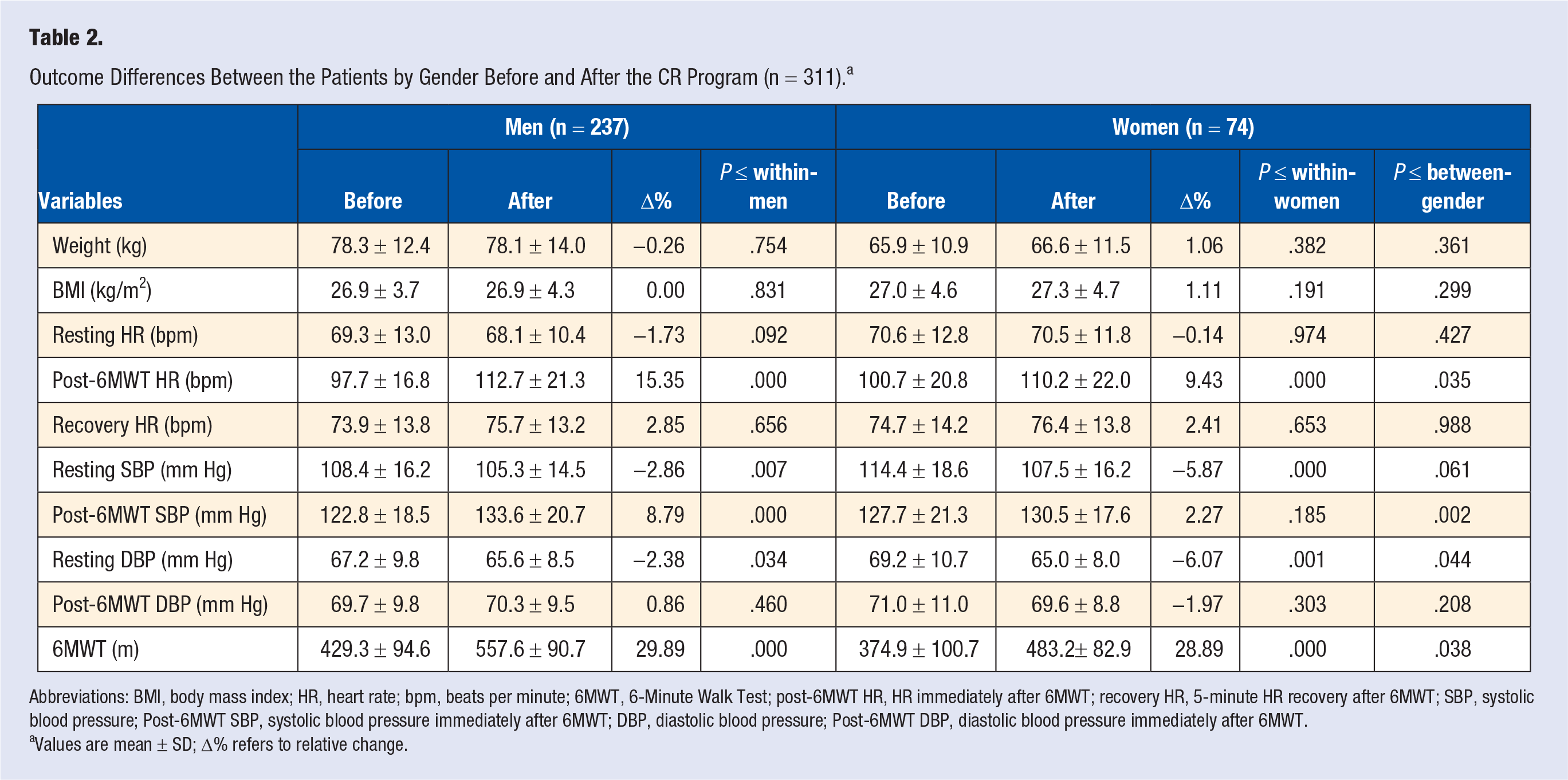
Abbreviations: BMI, body mass index; HR, heart rate; bpm, beats per minute; 6MWT, 6-Minute Walk Test; post-6MWT HR, HR immediately after 6MWT; recovery HR, 5-minute HR recovery after 6MWT; SBP, systolic blood pressure; Post-6MWT SBP, systolic blood pressure immediately after 6MWT; DBP, diastolic blood pressure; Post-6MWT DBP, diastolic blood pressure immediately after 6MWT.
Values are mean ± SD; Δ% refers to relative change.
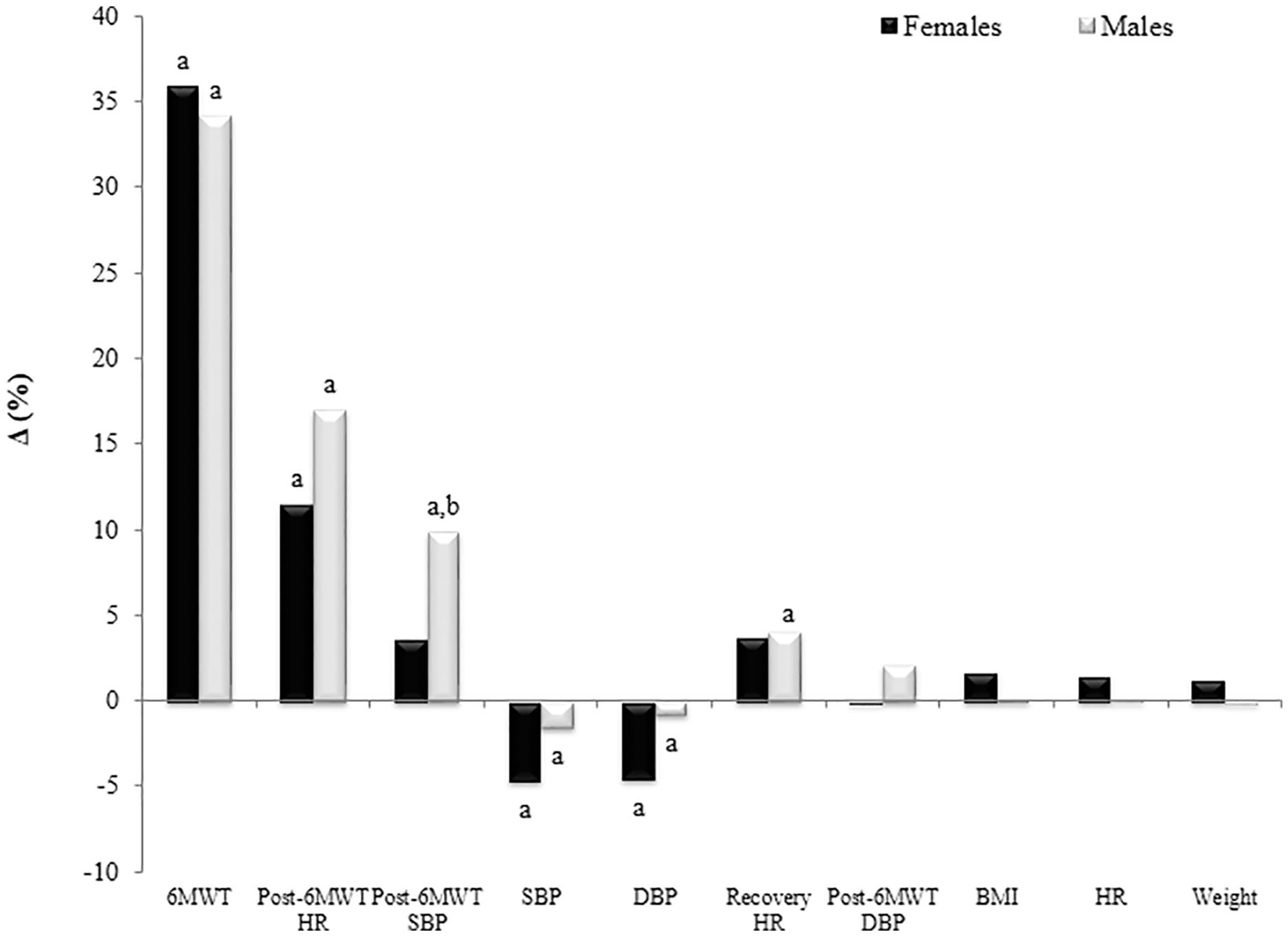
Relative change (Δ%) in physical and outcome variables following a cardiac rehabilitation program.
Significant correlations were found in the youngest male cohort (Q1) between CR sessions completed and ΔDBP (r = −0.33; P = .013), in Q2 for Δpost-6MWT HR (r = 0.41; P = .001) and Δ recovery HR (r = 0.29; P = .030), and in Q4 for Δrecovery HR (r = −0.31; P = .016) but not for men in Q3. For women in Q4, significant correlations were found between CR sessions and ΔDBP (r = 0.47; P = .040) and Δpost-6MWT SBP (r = 0.51; P = .022). No significant correlations were found between CR sessions on Q1, Q2, and Q3 for 6MWT on any hemodynamic variable.
Discussion
The present study examined changes in 6MWT distance and associated resting and exercise BP responses following a 12-week exercise-based CR program in men and women. These findings are consistent with previous reports relative to improvements in standardized walk performance testing after CR.6-8 Ghashghaei et al 8 reported a 19.0% increase in walking distance in patients after coronary artery bypass graft surgery following 2 months of CR. Similarly, Gupta et al 7 reported a 19.1% improvement in walking distance in cardiac patients after 24 to 36 CR sessions. Other studies have found that cardiac patients improve their walking distance by 21.6% and 31% following CR.6,16 In the present study, cardiac patients improved their walking distance by 29.8% after 33.0 ± 5.1 CR sessions. Men and women improved their walking distance by 29.9% and 28.9% after CR, respectively. The relative improvements between genders were not statistically significant, substantiating a previous report. 12 In contrast, after adjusting for potential confounders, including age, race, and baseline demographic data, Gupta et al 7 found that men demonstrated significantly greater relative improvements in walk performance testing than women (20.7% vs 16.8%, respectively) following CR. Gender differences in walk performance testing following CR in previous studies may be explained, at least in part, by the total number of exercise sessions performed by the patients. Gee et al 10 reported that women had a lower CR completion rate than men: 73% versus 65.6% for men and women, respectively. In the present study, men and women completed a comparable number of sessions (n = 33). Another possible explanation regarding the gender differences in physiological outcomes is that for several reasons, including lower education level, multiple comorbid conditions, non-English native language, lack of social support, and a higher burden of family responsibilities, women are less likely to enroll in and complete CR than men.23-26
In the present study, although the post-CR increment in walking speed—1.3 km/h (0.8 mph) for men versus 1.1 km/h (0.7 mph) for women—did not reach statistical significance, it may have clinical significance. Kavanagh et al 9 found that a 1.6 km/h (1-mph) increase in walking speed was associated with a 20% decrease in cardiovascular mortality in men with coronary disease. Each 1-MET increase in functional capacity in men appears to confer a 12% improvement in survival 27 and a 17% decrease in mortality in women. 28 Although the present study did not estimate or directly measure functional capacity, expressed as METs, based on mathematical calculations of walking speed, men walked at 4.3 km/h (2.7 mph) and women at 3.7 km/h (2.3 mph) on initiating CR, which approximated 2.8 to 3.2 METs. Following the CR program, men walked at 5.6 km/h (3.5 mph) and women walked at 4.8 km/h (3.0 mph), corresponding to energy expenditures of 3.3 to 3.7 METs, representing increases of 0.6 and 0.5 METs for men and women, respectively. Middle-aged and older adults who are able to achieve these post-CR walking paces, that is, 3.3 to 3.7 METs, likely have a functional capacity >5 METs, a fitness level compatible with a lower-risk patient subset. 15
In the present study, 3.6% and 3.0% decreases were observed in resting SBP and DBP, respectively. This finding is consistent with previous studies reporting reductions between 2.9% and 11% following CR.6-8,16,17 A previous report found that cardiac patients reduced resting SBP by 3.6% and DBP by between 2.9% and 5.6% following 3 months of CR. 16 A randomized controlled trial of 118 patients who underwent coronary angioplasty reported average relative reductions in resting SBP of 4.7% after 6 months of CR. 17 Another study found even larger reductions in resting SBP and DBP—11% and 9%, respectively—in patients who had undergone coronary artery bypass graft surgery followed by 2 months of CR. 8 Reductions in resting SBP and DBP in cardiac patients after exercise training may be a result of reduced total peripheral resistance, increased vasodilation mediated by enhanced endothelial nitric oxide production, or both. 29
Recovery HRs after the 6MWT in men and women completing the CR program were 37 and 34 beats/min lower than those obtained following the initial evaluation, consistent with previous reports in cardiac and heart failure patients. 18 Importantly, an impaired recovery HR after a 6MWT is a strong prognostic indicator of future cardiac events and heightened cardiovascular mortality in heart failure patients. 18 Exercise training has been shown to improve cardiovascular responses via adaptations to the autonoemic nervous system, specifically decreased sympathetic and increased parasympathetic activity, likely reducing recovery HR.4,30 In the present study, only SBP following the 6MWT was significantly different between men and women.
Limitations
We acknowledge some methodological study limitations. First, we reviewed data retrospectively from a single CR program in a university-based setting in Costa Rica. Second, we assessed exercise performance based on the 6MWT and did not estimate or directly measure cardiorespiratory fitness or aerobic capacity, specifically the VO2max, expressed as METs. Third, we only included participants with 6MWT and hemodynamic evaluations at baseline and following the 12-week CR program. Fourth, it is possible that changes in cardiac medications during CR may have influenced hemodynamic responses in a small number of patients. Finally, the follow-up was limited to 12 weeks. Despite these limitations, the present results, based on one of the largest populations of cardiac patients reported to date (n = 311), have significant clinical implications regarding the benefits of exercise-based CR.
Conclusion
In outpatients with stable CAD, the 6MWT provides independent and additive information beyond traditional risk factors and a prognostic ability similar to treadmill exercise capacity, expressed as peak METs, for predicting future cardiovascular events, including heart failure, MI, and death. 31 The present findings confirm and extend previous studies, highlighting the relative improvement in 6MWT performance following CR, demonstrating comparable exercise trainability in adherent men and women, and uniquely providing comparative resting and exercise hemodynamic responses to the 6MWT before and after CR. The only gender difference observed was the SBP response following the 6MWT, where men showed greater relative increases than women.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
The study was conducted according to the principles of the Declaration of Helsinki, Fortaleza, 2013.
Informed Consent
Patients signed an informed consent form before undergoing field testing and the exercise-based CR intervention.
Trial Registration
Not applicable, because this article does not contain any clinical trials.