
Abstract
The Complete Health Improvement Program (CHIP) is a premier lifestyle intervention targeting chronic disease that has been offered for more than 25 years. The intervention has been used in clinical, corporate, and community settings, and the short-term and long-term clinical benefits of the intervention, as well as its cost-effectiveness, have been documented in more than 25 peer-reviewed publications. Being an easily administered intervention, CHIP has been presented not only by health professionals but also by non-health-trained volunteers. The benefits of the program have been extensively studied under these 2 delivery channels, consistently demonstrating positive outcomes. This article provides a brief history of CHIP and describes the content and structure of the intervention. The published evaluations and outcomes of the intervention are presented and discussed and future directions are highlighted.
Keywords
‘[The CHIP] has been described by the American College of Lifestyle Medicine as “achieving some of the most impressive clinical outcomes published in the literature.”’
The Complete Health Improvement Program (CHIP) is a comprehensive lifestyle intervention that has been applied in clinical, corporate, and community settings.1-4 Over the past 25 years, an estimated 60 000 individuals have participated in the program worldwide. 5 The CHIP intervention has shown benefits for the management of chronic diseases3,4,6,7 and has been described by the American College of Lifestyle Medicine as “achieving some of the most impressive clinical outcomes published in the literature.” 8 The clinical effectiveness of CHIP has been documented in more than 25 peer-reviewed publications in medical and scientific academic journals. This review provides a brief history of CHIP, the content and structure of the intervention, and details of the published evaluations and outcomes.
A Brief History of CHIP
The CHIP intervention was founded by Dr Hans Diehl in 1986 after working for a period as the director of education and research at the Pritikin Longevity Center. This residential health program offered at the Center achieved significant improvements in chronic diseases and their associated risk factors within weeks. 9 The founder of the Center, Nathan Pritikin, was himself diagnosed with coronary heart disease in his early 40s, but after adopting a largely plant-based, whole food diet, and regular exercise, his autopsy 27 years later showed him to be essentially free of atherosclerosis. 10
Dr Diehl was inspired by the outcomes of the program at the Pritikin Longevity Center but recognized the limitations of residential programs, including their cost, which made it prohibitive for many individuals, and the “artificial” living environment that made sustaining the learned behaviors more difficult for participants when they returned to their home setting. In response, Dr Diehl developed CHIP as an affordable 30-day lifestyle intervention to be delivered to individuals in their community.
The first CHIP was presented in Creston, British Columbia, in 1988, where out of a population of 4000, 400 people enrolled in the 16-session program delivered over 4 weeks. Following the success of this program, CHIP interventions were conducted at numerous other sites, both within and outside of North America. In 1997, Dr Diehl recorded the program before a live audience in Kalamazoo, Michigan. The clinical outcomes of this program conducted at the Borgess Medical Center were published in the American Journal of Cardiology, 6 which was the first CHIP publication to appear in the literature. The presentations were then filmed and, accompanied by a curriculum package, were made available to health professionals and non-health-trained volunteers to facilitate CHIP interventions in their local community after attending a 2-day training workshop. Subsequently, CHIP has been administered and studied through 2 channels: professional delivery (clinical and workplace) and volunteer-facilitated. Interestingly, similarly low dropout rates have been reported when the intervention is delivered by health professionals (93% participant completion) 11 and volunteers (94% participant completion). 12
Through the professional channel, Roger Greenlaw, MD, working with the SwedishAmerican Health System, initiated a project to enroll within a 7-year period 5000 residents of Rockford, Illinois, representing 7% of the targeted population of greater than 40 years of age. 13 As part of the initiative, a series of cohort studies and 2 randomized-controlled trials were conducted that to date have yielded 17 articles in peer-reviewed journals.1-3,7,11,13-22
Through the volunteer channel, volunteers from community-interest groups, mostly members of the Seventh-day Adventist Church, adopted the program. The outcomes of these volunteer-facilitated programs have been studied in the United States,4,23 Canada, 24 and Australasia, 12 with a combined reported sample size of more than 7000 participants (see Table 1). These studies have documented the changes in the selected biometrics, including body weight and blood measures, which are taken as a standard component of the CHIP intervention at program entry and after approximately 4 weeks to increase accountability and engagement with the program.
Overview of the Professionally Delivered and Volunteer-Facilitated Studies of CHIP Showing Percentage Reduction Observed in Chronic Disease Risk Factors Over Approximately 4 Weeks.
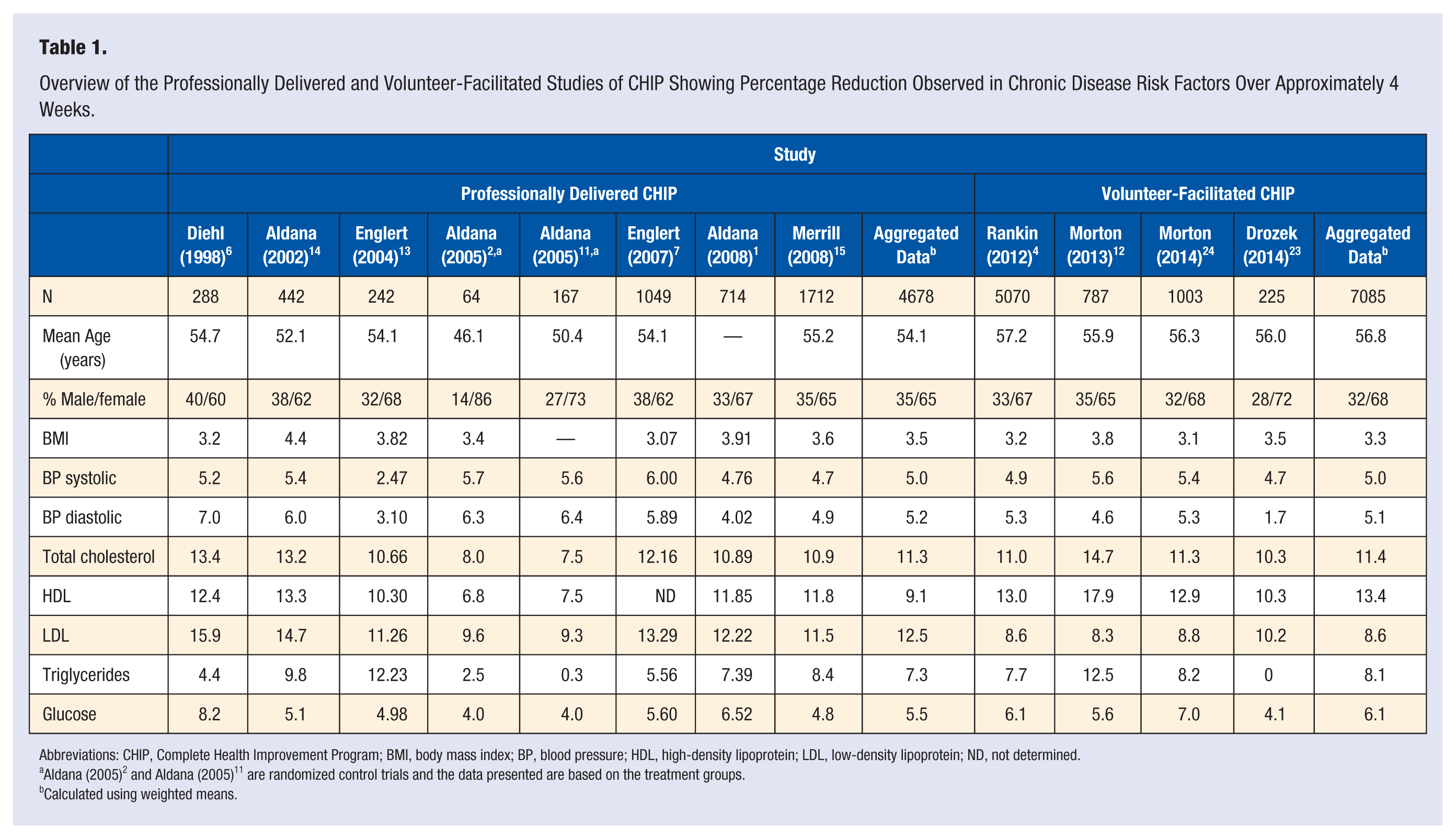
Abbreviations: CHIP, Complete Health Improvement Program; BMI, body mass index; BP, blood pressure; HDL, high-density lipoprotein; LDL, low-density lipoprotein; ND, not determined.
Aldana (2005) 2 and Aldana (2005) 11 are randomized control trials and the data presented are based on the treatment groups.
Calculated using weighted means.
Historically the program was known as the Coronary Health Improvement Project as it targeted cardiovascular disease. However, as studies showed the efficacy of the intervention in addressing other chronic diseases, such as type 2 diabetes mellitus4,14,25,26 and even depression,21,22 it was renamed in 2012 the Complete Health Improvement Program. At that time the program was adapted and expanded (as explained below) with newly recorded video presentations and supporting curricula.
Content and Structure of the CHIP intervention
The original CHIP involved 16 group sessions over approximately 30 days. Subsequently, the program has been expanded to 18 group sessions delivered over 6 to 12 weeks. The core elements of the intervention, however, have remained the same. Each of the group sessions is 1 to 1.5 hours in duration in which approximately half of the session involves viewing a prerecorded educational video with the other half constituting group activities, such as cooking demonstrations, physical exercises, and discussion. The sessions are structured around a model of learn, experience, reflect. 27
In the first part of the program (sessions 1 to 11), participants are educated on the etiology of chronic disease and the benefits of positive lifestyle choices, with particular attention given to diet and physical activity. The program advocates a predominately whole-food, plant-based diet. As this eating pattern tends to be high in nutrient density and fiber yet low in energy density, the program does not restrict the volume of food that participants may consume. The consumption of whole-grains, legumes, fresh fruits, and vegetables is recommended, whereas cholesterol, fats, refined sugars, and salt is discouraged. 6 Participants are also encouraged to consume liberal amounts of water daily and to become more physically active by performing moderate intensity physical activities—walking is especially encouraged through the use of pedometers—and resistance exercises. The first few weeks of the intervention are intentionally designed to be intensive in order to disrupt the participants’ present lifestyle patterns and to provide them with measurable health improvements within a relatively short period of time.
The second section of the CHIP intervention (sessions 12-18) concentrates on overcoming barriers and providing participants with strategies for behavior change maintenance. A qualitative appraisal of the CHIP intervention from the perspective of the participants found that while they reported improved diet, enhanced exercise, and weight loss, some encountered resistance from within themselves or from family and friends. 28 Consequentially, self-monitoring, goal setting, and problem solving are encouraged, 29 and an awareness of environmental (social and physical) influences on lifestyle practices is developed and strategies for negotiating them are covered.
Other lifestyle-related determinants of disease are also addressed in this second section of the intervention, including substance use, sleep, stress, and mental and emotional health. The program concludes by exploring themes from the positive psychology literature relating to self-worth and personal flourishing. 30
Behavior Change Theory Underpinning CHIP
The CHIP intervention incorporates elements from several behavior change theories including the Health Belief Model, 31 the Social Cognitive Theory, 32 and the Transtheoretical Model. 33 Underpinning the intervention, however, is the Theory of Planned Behavior. 34 The Theory of Planned Behavior asserts that behavior is driven by intention, which is formed from attitudes, social norms, and perceived control. 35 CHIP has a strong educative component to change the participants’ attitudes toward healthy living, and health literacy around nutrition and health behaviors has been shown to significantly improve as a result of the program. 2 CHIP occurs in a group setting to foster new social norms and accountability. Noteworthy, group programs have been shown to be more effective for achieving weight loss than individual programs, even for those who claim to prefer individual programs. 36 Finally, the intensive nature of CHIP, coupled with regular health risk assessments, are designed to increase the participants’ health related self-efficacy and perceived control.
A criticism of the Theory of Planned Behavior is that not all behavior is mediated by intention. 37 For example, emotions can override intentions and hijack behavior. Also, unsupportive environments can prevent intentions translating to the intended behavior. For this reason, CHIP includes sessions relating to the development of emotional intelligence and adopts a social-ecological framework that provides strategies for managing and reengineering unsupportive environments.
Effectiveness of Professionally Delivered CHIP
The first study of the CHIP intervention was conducted on 288 participants (123 men, 165 women) who completed a hospital-based professionally delivered program, presented “live” by the program founder, Dr Hans Diehl. 6 The primary goal of the intervention was to improve participants’ blood lipid and sugar levels and to decrease blood pressure. Secondary goals were to decrease participant’s body weight and medication usage for hypercholesterolemia, hypertension, and diabetes. 6
At 30 days, significant reductions were observed in all biometrics (Table 1). Two themes emerged from the data: participants at greatest risk experienced the greatest changes, and males tended to experience the greatest improvements. 6 On average, males with the highest levels of total cholesterol at program entry (ie, 240-279 mg/dL) experienced a 22% reduction in 30 days. Comparatively, females with the highest levels of total cholesterol experienced a mean decrease of 11%. Noteworthy, in the same year that these data were published, a systematic review of the effectiveness of dietary interventions for lowering total cholesterol in free-living subjects, published in the British Medical Journal, concluded that improvements of only 3% to 6% could be expected. 38
Diehl also reported large changes in low-density lipoprotein (LDL) levels (males = −22%, females = −14%) and triglycerides (males = −39%, females = −20%) for those participants who had the highest classifications of these biometrics at program entry. All of the 9 insulin-injecting participants had their insulin dose lowered, some by as much as 30%, and some participants were able to decrease or discontinue medications for diabetes, high blood pressure, or hypercholesterolemia. This study demonstrated that measurable clinical improvements could occur within 30 days through a community-based lifestyle intervention, at a relatively low cost compared to residential programs.
The encouraging outcomes of this pilot study resulted in an ambitious project to enroll 7% of the targeted population of Rockford, Illinois, to CHIP interventions delivered in clinical, corporate, and community settings. 13 The project used a video-based version of CHIP for the educational lecture component of the intervention and was accompanied by a series of pretest/posttest cohort studies and 2 randomized controlled trials.
Rockford Pretest/Posttest Cohort Studies
The first Rockford study, 13 initiated as a pilot, involved 242 participants. The observed biometric improvements were similar to those reported by Diehl 6 (see Table 1). This study also documented the nutritional profile typical of participants during the CHIP intervention, which was necessary as the program did not prescribe a dietary dogma but instead encouraged participants to move along the spectrum toward the ad libitum consumption of vegetables, fruits, whole grains, and legumes. Three-day food logs indicated that the participants dramatically reduced their total calories from fat from 39% to 20%, and cholesterol intake decreased on average by 77% (see Table 2). Carbohydrate consumption increased from 46% to 64%, primarily from unrefined sources, which also corresponded to a significant increase of 19 g (160%) in fiber consumption. Although the volume of food was not restricted, the increased emphasis on foods of high nutritional value but low energy density resulted in a significant decreased calorie intake of approximately 800 to 1000 kcal/day. These results indicated that participants were achieving the nutritional goals set by the program.
Mean Changes in Diet Composition of Participants in the CHIP (Adapted from Englert et al 11 ).
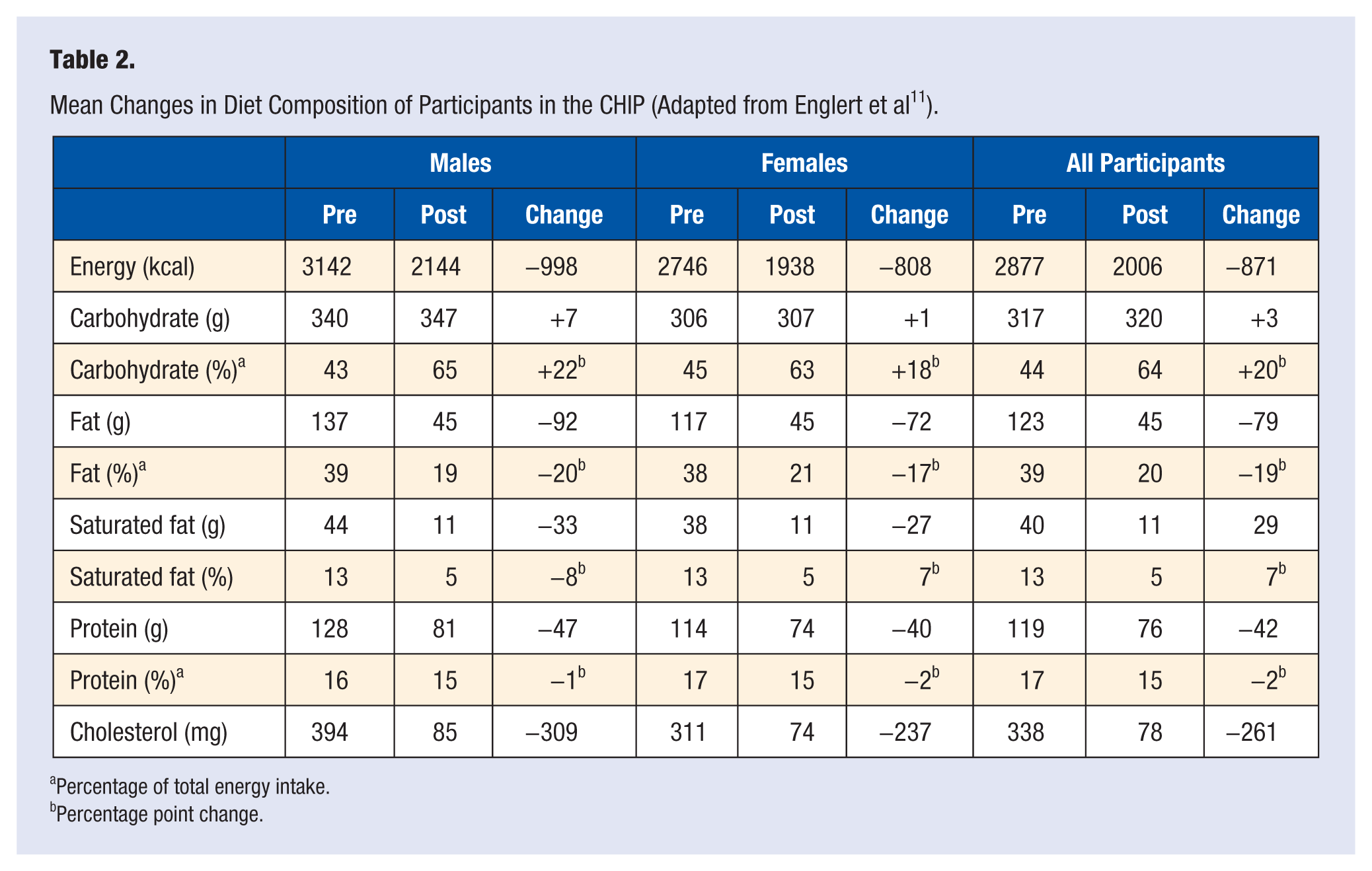
Percentage of total energy intake.
Percentage point change.
Several other larger Rockford-based pretest/posttest cohort studies1,3,7,11,14 consistently demonstrated significant reductions in body weight and associated body mass index (BMI), blood pressure, blood lipid profile, and blood glucose levels (Table 1). The magnitude of improvements was strikingly similar to those observed by Diehl. 6 It also confirmed the observation that participants at highest risk at program entry experienced the greatest benefits. In one of these cohort studies, 44% of the 114 participants taking oral medication for diabetes and 42% of the 59 participants taking insulin were advised by their personal physician to reduce their daily medication dosage during the trial. 39 The overall clinical changes were among the largest reported in the literature for a community-based lifestyle program and were approaching those outcomes achieved in residential lifestyle programs. 13 The average reductions in blood pressure were greater than those reported in the DASH study and comparable with the results of the PREMIER clinical trial. 3 As also observed by Diehl, 6 males experienced better outcomes than females.1,14
One cohort study involving 2624 CHIP participants found that in addition to improving biometric markers, sleep hygiene improved and stress indices decreased. 18 For example, the number of participants who self-reported to suffer insomnia after the 4-week intervention decreased by 64%. The observed improvements in sleep quality were related to increases in physical activity and decreased body weight. 18
In a 12-month follow-up of 1712 CHIP participants who participated in 1 of 6 programs in the Rockford area, significant improvements in all cardiovascular risk factors measured were recorded, including BMI, resting heart rate, systolic and diastolic blood pressure, total cholesterol, LDL cholesterol, triglycerides, and glucose. 15 Compared to measures taken at 4 weeks after program entry, some regression was observed at 12 months for blood pressure (systolic and diastolic), total cholesterol, LDL cholesterol, and triglycerides, but BMI showed continued improvement at 12 months (−4.0% at 4 weeks vs −5.1% at 12 months). Nutrition quality, physical activity patterns, and smoking levels remained improved through 12 months.
An 18-month follow-up of 211 CHIP participants from an original cohort of 348 individuals who had completed the 4-week CHIP intervention examined behavioral recidivism. 19 While no biometrics were collected in this study, the participants maintained significant improvements after 18 months in each of the 21 nutrition variables examined, except calories from protein, alcohol consumption, and whole grain servings, which were not different to program entry. Physical activity improved significantly through 18 months only for participants in the lowest 2 quartiles of physical activity at baseline. It was concluded that even though behavioral recidivism occurred, most healthy behaviors did not return to baseline levels after 18 months. Noteworthy, only 45% of the participants self-reported attending monthly support meetings offered after the CHIP intervention. These changes were therefore maintained even in the absence of attending ongoing support sessions.
While the pretest/posttest cohort studies showed promising outcomes, it was acknowledged that a randomized controlled trial was needed to eliminate confounders including regression to the mean and the Hawthorne effect.6,7 Hence, 2 Rockford-based randomized control trials were initiated.
Rockford Randomized Controlled Trials
The first trial recruited 348 participants who were randomly assigned to a CHIP intervention or a delay-control group that was stalled 6 months before receiving the CHIP intervention.3,11,15-17,19-22 The intervention used the video-based version of the CHIP intervention but was facilitated by health professionals in a clinical setting. After completing the intervention the participants were encouraged to attend monthly group support meetings. Data were collected at 6 weeks and 6 months after program entry.
At 6 weeks, significant improvements in all biometric risk factors were observed among the intervention group, similar in magnitude to those reported in the previous cohort studies of CHIP.1,11,13,14 While significant improvements were also seen in some biometrics among the control group, the intervention group showed significantly greater improvements for almost all the chronic disease risk factors measured. 11 Of special interest was the finding that those in the intervention group were 63% (P < .0001) more likely to report a decrease in depressive symptoms after 6 weeks, measured using the Beck Depression Inventory, compared with those in the control group. 21 This finding was partially mediated by the decrease in body weight experienced by the participants. 22 Other factors identified as potentially contributing to the improved mental health of the participants included the social connectedness inherently gained through the program, the mood-enhancing qualities of the physical activity promoted in the intervention, an improvement in self empowerment and efficacy, and a sense of new hope. 22
At 6 months, health behaviors remained improved in the intervention group with participants in this group taking on average 12 000 more steps each week compared to program entry. 3 All nutrition markers, determined using the Block 98 questionnaire, were significantly improved in the intervention group only, except for serves of whole grains, which increased in the intervention group by 0.7 serves/day but did not reach significance. 3
Changes in overall health status were assessed at 6 months using the SF-36v2. Participants in the intervention group showed significantly greater increases in scores for physical functioning, general health perceptions, vitality, social functioning, role-physical, role-emotional, and mental health. 16 Those in the intervention group were 34% (P < .0001) more likely to experience a decrease in the Beck Depression Inventory score at 6 months compared with those in the control group. 21 Depressive scores were related to sleep hygiene, which also showed significant improvements at 6 weeks and 6 months. 17
With regard to the biometric assessments at 6 months, participants in the intervention group showed significant reductions in BMI, body fat, systolic and diastolic blood pressure, and resting heart rate. 3 Stratified analyses showed those in the intervention group with the highest classifications at baseline of triglycerides and fasting plasma glucose had significantly lowered levels of these risk factors at 6 months. Reductions in total cholesterol and LDL cholesterol were not significantly different to baseline at 6 months in the intervention group, although stratified analyses showed that they approached significance for the participants who entered the program with elevated levels of these measures. Six-month changes in the control group were generally not statistically significant or were of a smaller magnitude than the intervention group. Interestingly, the study did not indicate that the intervention had any significant impact on C-reactive protein levels, which is inexplicable given the significant loss in body weight. 20 Further study of the impact of the intervention on inflammatory markers such as interlukin-6 and TNF-α is needed.
A second randomized controlled trial, similar in design to the previously described trial, involved 145 employees in a workplace setting. This study assessed clinical and behavioral changes at 6 weeks and 6 months, and changes in health literacy. 2 The intervention group had significantly improved BMI, body fat, and total cholesterol at both 6 weeks and 6 months. Improvements in LDL cholesterol were significantly greater in the intervention group than in the control group at 6 weeks but not at 6 months. There was no difference between the intervention and control groups in triglycerides, plasma glucose, or C-reactive protein levels at either measurement point. Consistent with other studies discussed, body weight continued to decrease in the intervention group from 6 weeks (−6.4 lb) to 6 months (−9.7 lb).
Health behaviors were significantly improved in the treatment group at 6 weeks and 6 months; however, there was some evidence of recidivism. For example, the average number of steps measured by a pedometer peaked at 6 weeks, with a 25% increase over baseline, but by 6 months this had dropped to a 16% increase above baseline. Consumption of vegetable servings per day increased from 3.2 servings at baseline to 4.8 servings at 6 weeks and 4.7 servings at 6 months. The control group recorded no change in these measures throughout the duration of the study. Cognitive understanding of the requirements for a healthy lifestyle increased in the intervention group with participants increasing their average test scores on a validated health knowledge test from 64% at program entry to 95% at 6 weeks.
It could be concluded from the professionally delivered Rockford CHIP studies that the intervention, when delivered by health professionals, can effectively reduce selected risk factors for chronic disease and improve health literacy and quality of life measures. Furthermore, benefits of the intervention may persist for 18 months after program entry and be comparable to residential programs, suggesting a cost-effective mode of administering lifestyle medicine.
Effectiveness of Volunteer-Delivered CHIP
In addition to being facilitated by health professionals, CHIP has been extensively offered in community settings by volunteer facilitators interested in making a positive contribution to the health and well-being of their local communities.4,12,24,40 Annually, some 200 CHIP interventions are facilitated in community settings worldwide through this volunteer channel. Most of these volunteers are sourced from the Seventh-day Adventist church, which in North America was coordinated through the Adventist CHIP Association.
The volunteer facilitators are not required to be health professionals, although some are, but undergo 2 days of training to learn about the CHIP intervention and develop group facilitation skills. The facilitators are then provided with a comprehensive CHIP resource package that includes a curriculum guide for program delivery, the prerecorded educational presentations, a plant-based eating cookbook, 41 a participant textbook, 42 and a journal. 27 The role of the volunteer is to organize and facilitate the proceedings of the group sessions; it is not to educate, as this occurs through the video presentations.
The first study of the effectiveness of volunteer-facilitated CHIP interventions involved the aggregated data from 5070 participants involved in 176 programs conducted at 136 sites throughout North America between 2006 and 2009. 4 Subsequent to this study, multisite studies in Australasia 12 and Canada have been conducted, 24 involving 836 and 1003 participants, respectively. Recently, another North American–based study concentrated on the low socioeconomic and disadvantaged region of Appalachia in Ohio. 23 The limitations of these studies included the following: the subjects were self-selected and hence probably had a high readiness for change, the lack of a control group, the short duration of the intervention (4 weeks), and behavioral measures were not collected and so changes in diet and activity levels during the program could not be determined. Notwithstanding these imitations, these studies recorded significant improvements with large effect sizes in all chronic disease risk factors measured, especially among those participants who entered the program with the highest risk.
Similar results were observed in the various international settings. 24 Participants who entered the program with the highest classifications of total cholesterol, LDL cholesterol, triglycerides, and fasting plasma glucose typically experienced 20% or greater reductions in these measures in 30 days.4,12,24 Of those participants with baseline plasma glucose levels >125 mg/dL indicative of diabetes, approximately 40% reduced their levels below 125 mg/dL in 30 days without the addition of medicaiton.4,12,24 In the study of 5070 participants from North America, an algorithm derived from the Framingham study 43 forecast that the improved risk factor profile of the participants would avert over 70 cardiac events among this cohort in the following decade. 4 Most notably, as shown in Table 1, the reductions in risk factors observed in these studies were similar in magnitude to those reported in the professionally delivered CHIP interventions. 40
A recent study examined the long-term effectiveness of volunteer-facilitated CHIP interventions for reducing chronic disease risk factors. 44 The study targeted a rural town, Hawera, in New Zealand, where a team of volunteers, including a local physician, had conducted CHIP in their community for over 5 years. All participants who completed the intervention 3 to 5 years previously (N = 284) were invited back for a free health assessment of which 106 (37%) returned (mean duration to follow-up = 49 months). Of these participants, those who had elevated biometrics at program entry maintained significantly (P < .001) lowered BMI (−3.2%), diastolic blood pressure (−9.4%), total cholesterol (−5.5%), and triglycerides (−27.5%). Further reductions in BMI (−4.2%), diastolic blood pressure (−13.3%), and blood glucose levels (−10.4%) were found among the 67% of participants who returned for follow-up and reported being compliant to most or all of the lifestyle principles promoted in the program. While the results of the study were subject to selection bias and the study did not include a control group, it is encouraging that the participants had significantly lowered chronic disease risk factors some 4 years after completing the CHIP intervention.
The sustained reduction in body weight is especially noteworthy given that most people regain all weight lost within 5 years of participating in a 20- to 30-week weight loss interventon. 45 The authors suggested one factor that may have contributed to the sustained weight loss observed in the Hawera study was the satiety-promoting ad libitum plant-based, whole-food dietary approach of the CHIP intervention. 44 Many weight loss programs restrict energy intake by limiting portion sizes, which often results in hunger and dissatisfaction with the eating regime, thus contributing to low compliance and weight regain. 46
The large number of participants in the volunteer-facilitated CHIP interventions, in particular the North American cohort (N = 5070), 4 has provided a useful data set to explore other questions relating to lifestyle interventions that promote a plant-based, whole-food eating pattern.
One of these questions relates to the effect of a shift toward a plant-based eating pattern on high-density lipoprotein (HDL) cholesterol levels. 47 Epidemiological studies have indicated that low HDL levels are an important risk factor for cardiovascular disease. 48 As such, they have become 1 of the 5 criteria for the diagnosis of the metabolic syndrome (MetS). 49 However, lifestyle interventions that promote a low-fat, plant-based eating pattern have paradoxically been shown to reduce cardiovascular risk and even promote coronary plaque regression, while lowering HDL levels.50,51 A study of the North American volunteer-facilitated CHIP cohort showed that while all other chronic disease risk factors measured significantly improved, HDL levels decreased on average 8.7% (P < .001), which had implications for the diagnosis of MetS. 47 This study showed that through the program significant numbers of participants no longer met the MetS criteria for high BMI (277 participants), raised blood pressure (767 participants), elevated fasting plasma glucose (472 participants), or elevated triglycerides (180 participants); however, 610 participants newly met the MetS criteria for low HDL levels. Applying the convention of MetS being defined as meeting 3 of the 5 criteria listed above, 112 participants acquired the MetS classification during the 30-day CHIP intervention as a result of a reduction in their HDL levels. 47 This study raised questions regarding the value of using HDL levels as a predictor of cardiovascular risk in populations who follow a plant-based eating pattern, especially given that in populations such as the Tarahumara Indians in Mexico who consume a largely plant-based diet, HDL levels are very low but there is virtually no cardiovascular disease. 52 As the functions of HDL are becoming more clearly elucidated,53,54 there is growing sentiment that HDL function might be more important than HDL level. 55
A second question that has been more comprehensively explored using the large data set derived from the volunteer-facilitated North American CHIP cohort relates to the differential responsiveness of males and females to the intervention. As observed in several of the professionally delivered studies of CHIP,1,6,14 males achieved better outcomes than the females. 56 This trend has also been observed with the residential Pritikin Program that also prescribes a whole food, plant-based eating pattern. 9 While the underlying factors responsible for men being more responsive than females to the CHIP intervention remain to be elucidated, it has been suggested that they may involve physiological or behavioral factors. 56 From a physiological perspective: men and women clearly have different hormonal profiles; men tend to have a propensity to store fat in the abdominal region which is more metabolically active and therefore easier to remove; 57 and men tend to have greater muscle mass and therefore a higher metabolic rate. 58 From a behavioral viewpoint, men may engage better with a lifestyle program once committed, 59 although getting them to initially commit might be more challenging. In the Western world, men access and use health services less often than women, even though their health tends to be poorer and mortality rates are higher. 60 It is noteworthy that in all the volunteer-facilitated, community-based CHIP interventions that involve self-selected participants, two thirds are consistently female.4,12,24 The influence of gender on the uptake and responsiveness to the CHIP intervention needs further investigation.
In conclusion, evidence from the volunteer-facilitated CHIP interventions indicates that this model of delivering Lifestyle Medicine may present a cost-effective mode for combating the widespread rise of chronic disease, as an adjunct to professionally delivered health care.
Cost-Effectiveness of CHIP
For Lifestyle Medicine to become more widely accepted in clinical practice, the cost-effectiveness of lifestyle interventions needs to be demonstrated. The Diabetes Prevention Program61,62 has been shown to be cost-effective in the United States63,64 and other countries; 65 however, more work needs to be done.
Recently, Shurney and colleagues 25 reported the cost-effectiveness of the CHIP intervention at Vanderbilt University and Medical Center. The study enrolled 28 employees with diagnosed type 2 diabetes and compared their health care claim data for the 6 months after program entry to 6 months prior to commencing the intervention, as well as against other employees with type 2 diabetes. The CHIP participants reduced their medical service utilization costs by 43% and medication usage costs by 14% compared with control individuals who recorded service utilization cost increases of 13% and medication cost increases of 10%. Almost 1 in 4 participants who completed the CHIP intervention eliminated one or more medications within 6 months. The return on investment after 6 months was 1.4:1.
A similar unpublished trial has been conducted at Lee Memorial Hospital in Florida, showing potential cost savings when using the CHIP intervention in the workplace setting, mediated through improved employee health status. A multisite study is currently in progress to determine the cost-effectiveness of the CHIP intervention on a wider scale.
Future Directions
CHIP continues to be delivered in clinical, corporate, and community settings and is presently offered in numerous countries including the United States, Canada, Australia, New Zealand, the United Kingdom, several islands of the South Pacific, the Philippines, Bahamas, and Mexico. In the future, data collected on CHIP participants globally will allow a robust investigation of how lifestyle interventions can be used most efficaciously to combat the global burgeoning rise of chronic disease. Specifically, questions relating to the influence of participant characteristics on the responsiveness to lifestyle interventions, the impact of facilitation factors, and the relative merits of lifestyle changes in different populations, will be considered.
Conclusions
The CHIP intervention has a long history as an evidence-based Lifestyle Medicine program. The CHIP formula of intensive, group-centered, evidence-based health behavior change provided in a community setting that supports participants in their usual living environments has a significant track record of success. The numerous studies of CHIP to date have resulted in it being the most well-published community-based lifestyle interventions in the literature. As CHIP continues to expand in its offering globally, the research effort surrounding it will help inform best practice in the delivery of lifestyle medicine interventions. Effective, acceptable, and low-cost health behavior change resources, such as CHIP, must continue to be developed and implemented if the worldwide chronic disease epidemic is to be reversed.