
Abstract
Most health care professionals can help clients connect with others and expand their support networks, and this is within their professional role. For many professionals, we suggest that being able to size up the available sources of support in patients’ lives is critical to their overall well-being and creating post-treatment conditions that achieve the greatest health outcomes. This may be especially true for adolescents who often turn to peers and adults outside the home for support. However, identifying potential health care allies in a patient’s life can be daunting, and one for which there are few tools or guides. Here we describe several benefits to health care providers from assessing a patient’s web of support and their connectedness. We present 2 assessment strategies that can be used by lifestyle medicine practitioners to both assess and expand their patients’ webs of support and connectedness to others; these small efforts, we argue, can yield major health benefits, in part, by increasing patient compliance with physician directives.
“People connect, behaviorally and emotionally, to those individuals who have provided them needed support in the past.”
Humans are social animals. Healthy and successful human development reflects the dynamic relationship between a person and their context. 1 “Context,” though, is not a monolith. Instead, humans are embedded within a complex, ever-changing, multi-layered system of experiences with people, places, and time; otherwise known as “life.”2–4 The salient experiences in a person’s life are typically mediated by social relationships. We thrive when we are connected to others in meaningful ways and yearn for interaction when we are alone. Decades of research (and millennia of philosophical thought) affirm the essentiality of connectedness to human social, emotional, and physical thriving and influence lifestyle quality.5,6 Relationships are the stuff of life itself. When we are socially connected, we are more likely to have hope for the future, joy in the moment, and purpose beyond ourselves.7,8 This is especially so for youth.
A robust empirical literature has documented the association between social connectedness and the psychological and physical well-being of adolescents and adults.9–12 We know that youth are less depressed and anxious 13 and happier and healthier when they perceive that they are connected to their friends and family through contact, communication, and mutual caring.6,14 Unfortunately, over the past decade, youth have reported substantially more loneliness and less connection to family and friends 15 and higher rates of depression.16,17 While not all researchers agree, 18 a myriad of reasons have been proposed for this reduction in social connection, including a corresponding uptick in social media use and the isolation caused by the COVID-19 pandemic. 16
Systemic issues have contributed to the reduction in relationship quality and quantity reported by youth in recent years. Individual and program-level interventions could offer youth essential opportunities to form and maintain social connections. 19 The outcomes and mechanisms of social connection have been documented in numerous other articles, including articles published in this journal.11,20 For youth, particularly youth who have been historically marginalized in American society, different types of supports from people in a youth’s life can benefit a youth’s mental health, their physical wellness, and their social and emotional competencies.21,22
In this article, instead of focusing on these specific interventions and supports, we propose 2 interrelated organizing frameworks for better understanding contributors to social connection and disconnection. We offer practical assessment tools that professionals can use to improve their health care service delivery by involving the social networks of their patients, clients, and community members.
Why Providers Should Assess Patients’ Webs of Support and Connectedness Profiles
Health care providers provide unique, specialized practices and procedures that improve health or save lives that are not typically provided by anyone else. Providers can also encourage healthy lifestyles that invite greater physical and psychological flourishing that mitigates the impacts of chronic medical conditions. 11 Yet, these positive outcomes from health care services depend greatly on their patients’ abilities to enlist others to support them who reside outside the health care system. Providers can influence the people in the patients’ support network, directly and indirectly, to serve as health care allies and thereby facilitate patient recovery and health promotion.
To aid providers in the identification of health care allies as well as to reveal which patients may need to identify novel allies to fully benefit from provider treatments and services, we describe 2 theoretical frameworks and accompanying assessment tools. We propose that using these assessments can strengthen how lifestyle health care providers can help patients utilize and capitalize on ties in their webs of support to encourage healthy lifestyles and behavior change to facilitate recovery and growth. Both utilize ecomaps, which have been used and described in the health care literature as “graphic illustrations of individuals or family units shown in the center of a circle. Outer circles within concentric circles formed around the center represent the sources of connection to that person or family, reflecting less intimate relationships moving outward.” 22 (p. 2) First, the Web of Support framework is introduced to reveal the extent and types of support in a patient’s life that can be documented through the Web of Support Interview and ecomapping procedure. 23 Second, adolescent connectedness theory (and a corresponding assessment-based Connectedness Ecomap) is used to characterize patients’ common modes of emotional and behavioral engagement with others within and beyond their web of support. 7
We consider the relationships that patients have with those around them in their daily lives—specifically the individuals who could be invited into paraprofessional health promotion and recovery roles—to reflect a system of support that is embedded within their overall ecological system. In terms of their role in a patient’s physical and psychological well-being, the relationships in a patient’s life can be viewed collectively as a social health system. A patient’s existing system of relationships contribute to a healthy lifestyle by providing them the different social supports they need in order to navigate opportunities for and barriers to their social, emotional, and physical health. This relational system develops, becoming larger and stronger, through self-initiated connections to others that are subsequently reciprocated through others’ emotional and behavioral engagement with the patient. Therefore, providers’ efforts to strengthen the linkages between existing relationships in a patients’ lives in service of health care enhancing directives can help patients realize the opportunities afforded by the intersection of available support and patterns of connecting within and beyond a patient’ current network of relationships. In this way, perceived support and an individual’s connecting tendencies are interrelated and function synergistically but have unique qualities. Given this, providers need to understand where social support is available in their patients’ lives and how commonly their patients utilize this support through seeking out and appreciating the range of supports in their lives that might aid in health care service uptake.
The role of social supports, connectedness, and relationship quality in health care, growth, and recovery have been the focus of a multitude of studies; so many, in fact, that many have subsequently been synthesized collectively in systematic reviews and meta-analyses, such as on the effects of social connections on psychological and physical health outcomes.9,11 Among other findings, these reviews and meta-analyses show that youth and adults who perceive support from those around them engage in fewer risky health behaviors (e.g., smoking), have lower rates of cardiovascular disease, and have lower mortality rates than those with less perceived support. These findings are particularly compelling when considered with the recent calls from the United States Surgeon General for a focus on loneliness. 24 For these constructs to be useful in practice, health care providers need clear terminology and specific actions they can take to assess these indicators of social health.
Social Support, Belonging, and Connectedness Among Adolescence: Definitions
Unfortunately, many studies and syntheses have been broad in scope and arguably have used overly broad definitions and operationalizations of social support and connectedness to be helpful. For instance, Wills’ 25 foundational definition of social support focused on one’s perception that others love or care about them, they are valued by these people, and they are part of a mutually beneficial social network.
This definition of social support combines the act of receiving care with the psychological feeling of belonging to a social network. Similarly, research on connectedness has frequently conflated constructs of belonging and behavioral engagement as indicators of connectedness.7,26 This approach runs the risk of the jingle jangle fallacy 27 in which 2 measures with the same name might actually be measuring 2 different underlying constructs (jingle) or 2 measures with different names might actually be measuring the same underlying construct (jangle).
In the following description of the Web of Support framework, our goal is to sufficiently differentiate the people and places where one receives support (and its specific forms) from the patterns of individuals’ connectedness to people, places, and activities in response to perceived support. We try to be as specific as possible about how and why we use particular terminology, such as for types of social support that afford distinct forms of social capital (e.g., bonding vs bridging capital). Our discussion of this framework reveals each of the elements necessary for conducting the Web of Support Interview that can visualize and reveal a person’s “web.”
The Web of Support as an Organizing Framework
An individual’s web of support 23 is the constellation of people and the social supports they provide across the different contexts within a person’s life. These social relationships are infused with the various social supports that an individual needs to thrive. We will describe the structure of the Web of Support framework (WoS), 5 specific types of supports currently provided by individuals in their key social ecologies (e.g., school, home, organized groups), the variety of individuals who could potentially provide additional supports, and the agentic role that the individual plays within their own web. Therefore, a web of support provides a great deal of information, and in particular 3 unique qualities of the individuals social ecology: 1. Specific types of social support they encounter across settings and relationships; 2. The extent to which ties with individuals cross overlapping social networks and core clusters of ties; and 3. The extent to which a given tie offers either bonding and bridging forms of social capital. Knowing these 3 qualities of a person’s web of support can reveal opportunities for practitioners to locate health care allies and solicit their assistance in facilitating growth and recovery.
As previously mentioned, an individual’s system of relationships is embedded within their broader ecological system.
8
A web of support includes all of the people in a person’s life who currently (and sometimes previously, or potentially) provide various types of support and who have a positive psychological, emotional or physical relationship to that individual. These
Ties tend to cluster within the different contexts within which a person lives and goes about their daily business or activities (e.g., such as teacher-student and counselor-student relationships in schools or employee relationships within a workplace). We consider these clusters of ties as comprising
Practitioners often seek to identify the persons a patient considers to be the most important, influential, and supportive people in their lives. Within each core, 1 person typically rises above the others. This is their
A patient’s anchor also may be the person in a patient’s life who a practitioner can enlist to help coordinate the supports that already exist and facilitate connections to those potentially helpful people not already in a person’s web. Importantly, the anchor does not have to provide all of the supports that a person needs. Rather, the anchor is someone seen as available, able to provide at least some types of support, and may be best positioned to be a connector for the patient by bridging the patient to new worlds of resources (information, services, instruction) or someone who can provide access to such resources outside the youth’s existing social network or web of support. In this way, the patient’s anchor may be able to enlist individuals outside or at the periphery of the patient’s existing web of supportive relationships to expand the web (i.e., providing bridging capital).
Other strong ties for a patient are health care practitioners, who regularly provide bridging capital to patients by connecting them with hitherto unknown specialists, health centers, activities, or exercise. These individuals, as well as the supportive experiences with them and the bridging opportunities they can provide would typically be located at the periphery of a patient’s existing web. These weak ties thereby introduce novel insights, knowledge, and motivation about nutrition, exercise, therapies, and psychological wellness. 28 These weak ties can potentially evolve into new cores (i.e., linked ties), providing information about nutritious foods, access to doctors with expertise on a rare cancer, or a link to a group of people who model healthy behaviors.
Many frameworks describe social supports, with a cross-cutting view of social supports as relational supplies that are transmitted through a connection between the recipient of the support and one or more people in their social network. For purposes of this article and consistent with how we have previously written about the Webs of Support framework,23,29 we consider 5 types of support: emotional, resources (instrumental/material), informational, appraisal, and companionship (see Figure 1), forming the mnemonic “I CARE.” The first, Informational support (I) is the navigational insights a person needs to confront a challenge or problem, such as knowing how to work through the health care system or how to increase cardiovascular endurance. Companionship support (C) is when a person is available for social activities, providing a sense of belonging to a youth. Examples of companionship support could include accompanying another person to a show, a game, on a walk, or other activity. Appraisal support (A) is when a supporter has expectations for what a person can achieve and praises them upon meeting that expectation. An example would be 2 people who exercise together and hold each other accountable for showing up to a workout and congratulating them when they accomplish a goal (e.g., running a 5k). Resources (R), also known as instrumental or material support, is the tangible support that a person needs to deal with a challenge or problem, such as being given a ride to the doctor’s office or provided a nutritious meal when they have no food. A fifth type of support, Emotional support (E), constitutes the expression of care for someone else, such that the supporter provides the proverbial shoulder to lean on when the person is facing problems in life. A Web of Support, ties, and support types.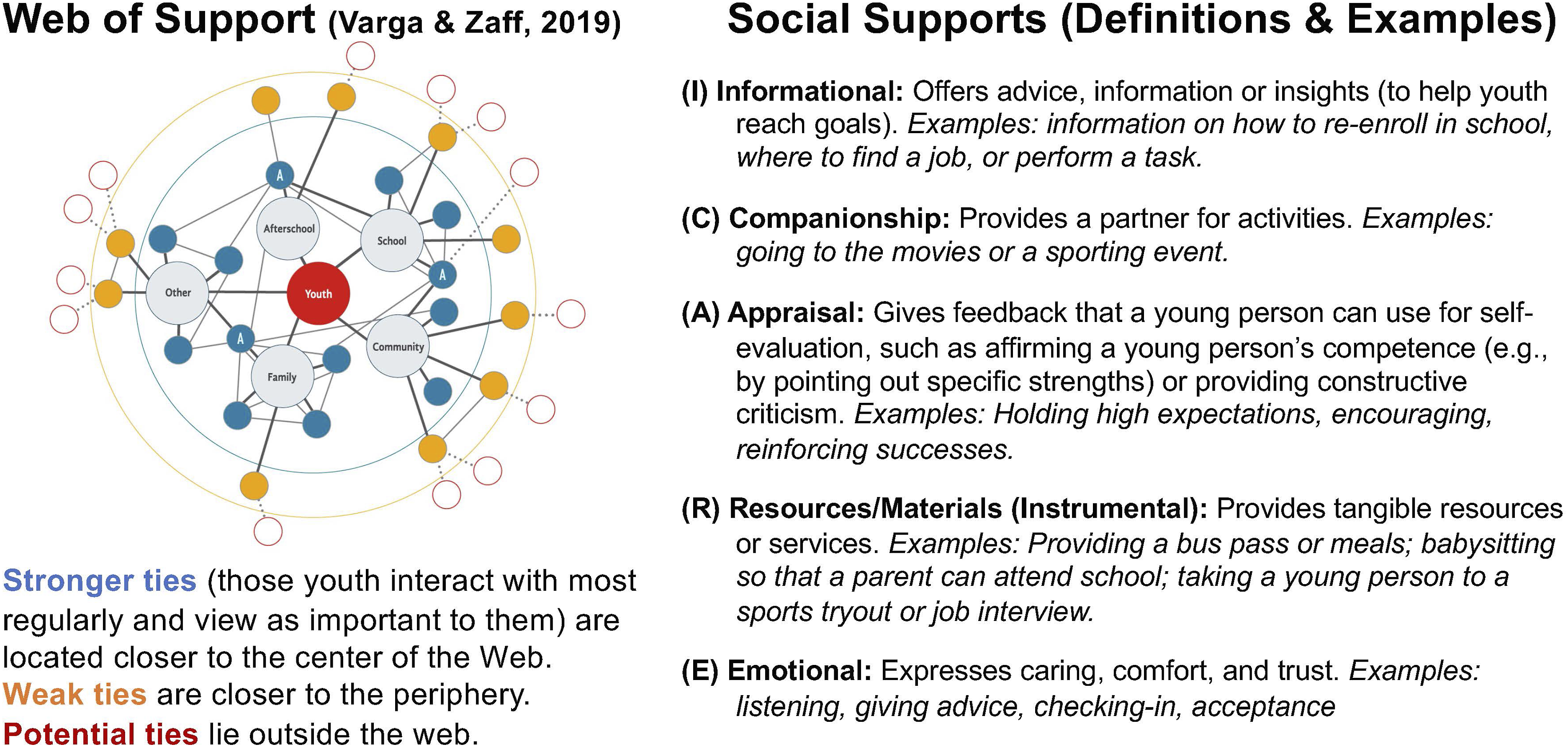
Patients may need help to identify potential health care allies from inside their existing web of support and more peripheral supports that reside outside their web. This constellation of supports could be mobilized around the patient’s current health care needs. A visual depiction of the patient’s web of support, including anchors, various ties (central/strong, peripheral/weak), and designations of the types of support each provides (see Figure 1), can reveal where types of support may be needed, found, or sought either within the web or beyond the current web of support Although not depicted in Figure 1 (to reduce visual complexity), and shown only for Nurse Helen in Jen’s web of support ecomap in Figure 2 are letters indicating the types of support (I, C, A, R, E) provided by the individual just below their name. The total number of each type of support reported in each core is generally written off to the side to provide a tally of the extent of each type of support present in each core. A Web of Support Ecomap with Jen’s constructed Web of Support.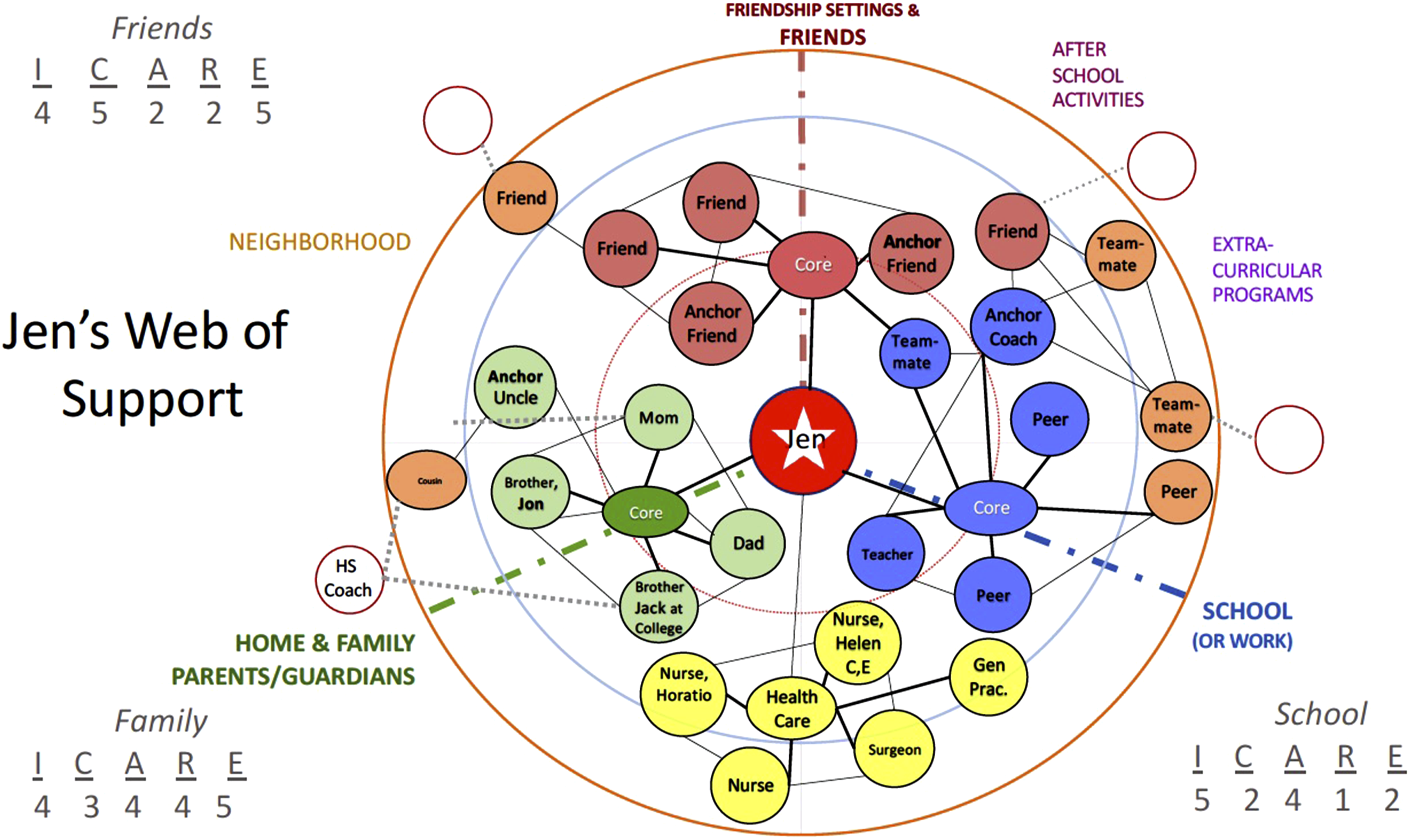
Importantly, health care providers need to consider not who they, as the provider, believes should be a health care ally, but ask the patient who they say they would go to for support (and accept support from). The value of perceived support overrides or supersedes the degree of objective support available to a person. No person is helpful unless the person being helped perceives that person as helpful. Together the Web of Support framework, interview assessment and ecomapping approach provides health care practitioners a patient-centered-view of the perceived support in the patient’s life.
Webs of Support in Lifestyle Medicine Practice: An Illustrative Example
A review of existing literature on available supports, specifically for youth, suggests that the specific forms of social support that may facilitate the adoption of lifestyle changes or post-procedure recovery activities vary widely.12,14,20,30–32 Patients with a vast web of interconnected and supportive individuals tend to face fewer headwinds to their recovery, while those with smaller support systems, or who lack resources (e.g., transportation), or are situated in support systems that are antagonistic to established systems of conventional care or public institutions may encounter numerous challenges to procedural recovery. Assuming individuals have sufficient support across the cores in their lives (e.g., family, employment/school, neighborhood, and friendship groups) can increase the likelihood that both health care provider and patient may be blindsided by unanticipated resistance to pursuing ongoing care or non-compliance with necessary post-procedure recovery activities. This provides 1 important reason why practitioners may benefit from assessing patients’ webs of support.
To illustrate this point, and premised on best practices from previous projects that incorporated ecomapping into a variety of clinical settings,
22
we present a fictional, best-case scenario regarding available supports and how they interact with post-procedure recovery. Imagine that a teen (Jen) with congenital heart issues is preparing to have open-heart surgery to replace a valve. To prepare, Jen and her family decide together that everyone will eat a high-fiber diet low in animal fat so that her body is in good shape for the procedure. As Jen’s parents go to the grocery store, she calls a couple of close friends to see if they will be available to help her get home when she is released from the hospital. These friends surprise Jen with a few visits the week before the surgery to keep her in good spirits and optimistic about the outcome. Her older sibling, Jack comes home early from college so that on the day of the procedure he drives her to the hospital. Upon arrival, Jen is cared for by a group of nurses who, including Horatio and Helen, whom she’s come to know and trust, prepare for surgery and wheel her into the operating room where the surgeon and surgical team are waiting for her. Jen is given full sedation and wakes up a few hours later in her room where a nurse is ready to support her recovery for the next few days until she can go home. While she is in the hospital, a steady stream of close friends come by to socialize, play cards with her, watch a movie, and laugh about fun times they have had together. Before she leaves the hospital, the Surgeon suggests she seek out someone to get her to the school track so she can walk each day at a particular pace. Her General Practitioner suggests, based on her experience with previous patients needing consistent post-surgery exercise, that if Jen can coordinate to meet up with her friends for these walks she’s more likely to follow through on the surgeon’s post-procedure recovery directives. When Jen is ready to go home, Jen’s family packs her up and they drive her home and get her settled back into the house. When Jen can leave her bed independently, upon entering the kitchen, she opens the refrigerator for a snack to find a fridge stocked full of healthy foods and looks on the kitchen counter to find the selection of prescribed medications that her brother picked up. When she wants to start her rehab, she learns Jack is good friends with the high school track coach, whom Jack enlists to drive Jen and her friends to school in the mornings on the coach’s way to work. There, she and her friends walk around the high school track with her and then go to the gym with her afterwards for strength training until one friend’s parent picks them up, as both of Jen’s parents work full time. Because she has so much support, including transportation arranged by Jack, Jen can focus on her recovery, stay positive, and adhere to her post-procedure rehabilitation plan.
In this scenario, the surgeon, surgical team, and nurses (Horatio and Helen) along with other hospital staff are clearly essential to Jen’s care, both treatment and immediate recovery, while she is at the hospital. However, they are not present at her house or in her community to provide direction or other forms of support to facilitate post-discharge recovery. And even while she is in the hospital, the medical team may be informative, caring, and encouraging, they will not bring Jen the same good cheer as her friends and family can (e.g., providing emotional support and companionships). This illustrates that, even while she was in the hospital, the treatment recovery process is buttressed by essential supportive ties outside the medical system. Furthermore, once discharged the surgical team is obviously not going to the grocery store to provide her the “resources” she needs or ensure she has a means of transportation for rehabilitation activities. Because those in the health care system are not at home to help Jen to enlist the various supports that she will need to fully recover, they rely on those in her web of support to serve as paraprofessional health care allies.
We want to highlight 2 key factors in this first example that illustrate how much physical health, and in particular treatment recovery and behavioral change, are inextricably linked with the patient’s social health; that is, on the strength of the ties and range of available supports in one’s web. The first is that much of Jen’s healing and recovery occurs outside health care settings, and thus is beyond the direct influence of health care professionals. Procedure recovery, like lifestyle changes, is greatly dependent on the social supports that are in place outside the health care space, those supportive people who are located wherever the patient heads when released from the hospital or following patient appointments and who provide emotional support, companionship, and encouragement, as well as those who appraise her progress.33,34 There is a recognized disconnection between these 2 worlds of health care providers and informal helpers,30,33 which can undermine treatment efficacy, health care outcomes, and the full implementation of healthy lifestyle changes.35,36
A second factor revealed in the above example is that after their health care procedures and consultations, patients will return to the people and places in their lives and, consequently, will resume their patterned ways of interacting with those potential informal “health care allies.” But in many cases, unless those supportive paraprofessionals health care allies (family, friends, neighbors) self-initiate provision of post-treatment care, as in the example above, or offer specific supports (e.g., ask the patient, “How can I help you do X to aid in your recovery”) the patient will have to solicit these support independently. 36 That is, unless these potential health care allies are provided instructions on how to engage the patient in recovery or lifestyle changes, the likelihood that they will perform these functions is greatly diminished. Patients often need help knowing what help they need to ask for, understanding the nature of the help (e.g., instructions or specific guidance to provide others, like “I need you to drive me to the rehab center 3 times a week.”), and identifying what people in their web of support (including weak ties like Jack’s friend, the coach) could serve as health care allies. Jen needed a way to get herself and her friends to the high school to walk the track, and her brother Jack enlisted his friend the coach to provide that support, thereby pulling the coach more proximately into her web of support. In addition, those in a patient’s web need to have an understanding about what the patient (and their friend or family member) might need so that the burden to ask is not placed on the patient’s shoulders; with a particularly unhelpful question to ask a patient being, “what can I do to help?” This point speaks to relationships being two-way streets, with each person having roles and responsibilities as part of their preexisting relationships that may not directly align with needed support for needed rehabilitation or lifestyle changes. It is a challenge for health care and public health systems to determine how providers can equip people in patients’ support networks with the knowledge and skills to act as health care allies and take on new supportive roles.35–37
Specifics of Creating a Web of Support Map
The web of support is typically constructed collaboratively through asking the youth to identified helpful, supportive and important people in their lives and then to place each on the Web of Support Ecomap (see Appendix). Opening questions include the following: “We are going to spend some time now talking about some of the people you know. I would like to get an idea of which family and friends and other people you feel have been most important to you and most helpful. To begin with, I am going to ask who you spend time with, are important to you, and who you turn to for different kinds of help.” The assessment, conducted via an interview in person, may take a half hour to 45 minutes if done fully. Some information might be able to be gathered more efficiently using other methods, but typically someone in the health care setting would conduct it in person.
After identifying individuals at home, school, and other settings, the youth is asked to describe how each person has been helpful. Each of the descriptive sentences in the following script describe 1 of the 5 types of support described earlier using the I CARE mnemonic (Informational, Companionship, Appraisal, Resources [Instrumental], and Emotional Support): “Think about the people who support you in life. They may help you to figure out how to do something like completing your homework or filling out a college applications (I); spend time with you like by playing basketball, just hanging out or going with you on job interview or to visit a college (C); give you feedback on how you are doing or cheer you on in whatever you do in life (A); give or lend you things you need like food, clothes, or money (R); or give you a shoulder to lean on when you are feeling down (E).” Once the youth has identified individuals in each of the primary Cores of Home, School, and Friends (and usually no more than 6 are needed to assess the range of available support in each core), they are asked about other settings or contexts that may be important sources of support like a workplace, after school program, youth group etc. For each person, ask what their primary role is (how they are related to or know that person), such as being a friend, relative, teacher etc. and how long they have known that person-enduring relationships often are important ties, even if they have not provided specific support or interacted with this person recently. Such people as teachers from years back or a caring aunt who is rarely seen nowadays, may prove to be anchors in waiting or may serve as peripheral ties that allow access to unique and important forms of support beyond their current web of support. The names or initials of individuals are written on sticky notes placed on the Ecomap.
Instructions are provided on placement of names so that those who they view as most important and who they see most frequently are placed closer to the person in the center. Once all individuals are placed, the youth is encouraged to move the “most important” individuals closer to the center. For example, Jen moved her Surgeon closer to center because of her importance to Jen, which moved the Surgeon from the outer ring closer to the center ring. Information regarding the frequency of contact and importance (i.e., the proximity of the supportive person to the youth at center) can be very helpful in determining who is available to serve as a health care implementation ally. The individuals in the outer ring, with whom the youth is not close and sees rarely, are called peripheral ties. Often being embedded in other social networks than the youth’s, these peripheral ties provide links that bridge new people (or potential ties) outside the youth’s web (shown in red circles in Figures 1 and 2) into their web of support. For example, Jen’s brother Jack was able to recruit his friend, the high school coach to help by driving Jen and her friends to the high school track several days each week. This bridging capital thereby expanded Jen’s web.
Patients may also need help identifying who in their life could provide them a specific kind of support that is not commonly part of their usual interactions. Someone who typically provides emotional support through caring conversations, like Jens friends, may need to be relied upon to provide material support, like transportation or to get medications. Someone who usually provides companionship (a neighbor) or informational support (a colleague at work), may need to provide appraisal support by helping to assess the quality of the patients’ efforts to perform rehabilitation exercises or to comply with dietary or exercise habit changes. In short, it may not be clear to patients who in their social network could best perform what functions; so health care providers who want to maximize uptake of patient directives need a way to survey their patients’ support landscape. With this information, providers can tailor their recommended post-op activities or behavioral health recommended practices in ways that leverage assistance from the individuals in their webs of support in the delivery of supportive accountability. 37
Connecting in a Disconnected World
A web of support ecomap, however, may not provide all the information a provider needs to identify whom the patient should seek out to provide specific types of health care support. To know who an adolescent patient seeks out most for various forms of support, we must study their everyday mode of engaging or connecting to other people, places, and activities. The people, places, and activities a person values and engages with often align with their Web of Support, but not always or exactly. When they do not align, opportunities to enlist the best “paraprofessional” helpers or allies in a patient’s growth or recovery may be missed.
In a way, health care providers are trying to direct their patients to new destinations. Getting their patients into these new lifestyle destinations may require incorporating new ties or reorganizing existing support networks in ways that involve the existing supporters as health care allies (e.g., partners, family, friends, neighbors, coworkers) in new and needed roles to provide specific forms of support, sort of like health care paraprofessional mentors,35,37 who provide a form of supportive accountability the providers cannot. Another target or destination providers may want to direct their patients to, is a set of healthier lifestyle practices or behaviors. Effectively engaging patients in rehab activities or positive lifestyle changes often requires diverting them from their old, typical patterns of engaging in health-compromising activities. Knowing their patients’ typical patterns of connecting with others can make more evident how drastically different specific lifestyle changes or post-procedure recovery activities are from the patients’ normal mode of connecting with others.
Health care providers need to know “in what direction was the patient already headed?” to effectively provide them with new directions (or “directives”) to healthier lifestyle destinations. Beyond knowing what types and the extent of support existing into which the patient will return we also need to know how they tend to engage with others. This is the “direction” the patient is already headed and the trajectory of ways in which the patient is already emotionally and behaviorally directed or “connected.” Assessing adolescent patients’ connectedness, therefore, reveals toward what people and places they currently and regularly direct themselves. We learn what gets them moving, day after day, and to whom they are naturally drawn. This answers questions like, “Do they commit time and attention to school, family, or friend cores similarly?” And “Are some relational worlds prioritized over others?”
Profiling Adolescent Patient’s Connectedness to School, Friends, and Family
People connect, behaviorally and emotionally, to those individuals who have provided them needed support in the past. Townsend and McWhirter described connectedness as: “when a person is actively involved with another person, object, group, or environment, and that involvement promotes a sense of comfort, well-being, and anxiety reduction.” 38 (p. 193) We concur with this definition and further assert that connectedness is not belonging—it is not the feeling that I am supported, included, or part of a given system or “core.” The jangle problem of calling connectedness all things relational (from belongingness to engagement and even social network size) has thwarted the effective use of connectedness as a reliable indicator,27,39 especially when used in research syntheses.26,40 Instead, we rely on adolescent connectedness theory7,41 and present the tripolar adolescent connectedness theory (TACT) assessment tool 7 here as a complement to the web of support assessment, suggesting they are both useful in different ways.
Connectedness is the degree to which individuals engage behaviorally and emotionally in the various social worlds, relationships, and activities that are developmentally relevant to them. For adolescents, worlds of connectedness—like connectedness to friends, classmates, teachers, parents, siblings—cluster in core regions of worlds with family, school, friend connectedness typically being the most significant core regions.
41
Within each of these 3 core worlds of connectedness regions are specific relationships (see Figure 3). The family connectedness region includes the patterns of connectedness to siblings and parents or caregivers, generally, recognizing that varying degrees of connectedness are often reported for each parent or caregiver. In the school region, youth connect to multiple people, both adults (teachers, coaches) and youth (classmates, culturally different peers). Thus, one can look at patterns of connectedness across a wide range of worlds or can focus in on specific regions, such as overall connectedness to school, family and friends. Health care providers may benefit most by considering the configurations of connectedness their patients report across the regions of family, school, and friendships. This is because differences in the frequency of behavioral contact and the degree of positive affect expressed toward these people (i.e., connectedness to others) tells a great deal about the youth’s openness to the directives of adults. For example, youth whose connectedness to both parents and teachers is low but their connectedness to friends is high are less likely to utilize their parents and teachers as supports as they are to turn to friends. Just knowing patients’ connectedness levels in these 2 region scores (school and friends) can provide practitioners a lot of useful information to guide their efforts to create post-op care directives and identify possible health care allies to assist in their implementation; this is because the similarity and differences across these 2 regions of connecting often indicates whether the youth’s general pattern of engagement is conventional or unconventional. Items on the 3 Connectedness Compass subscales.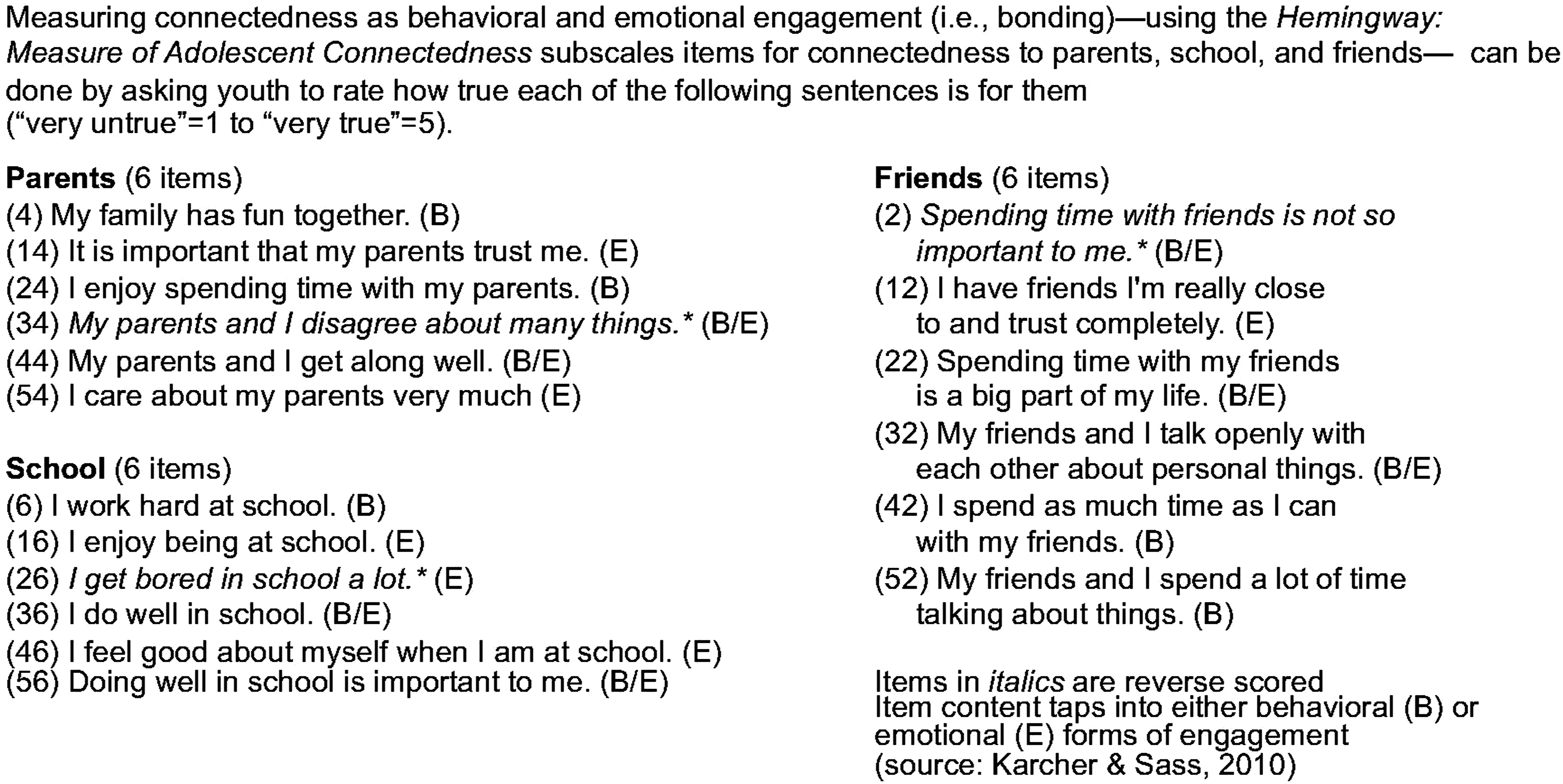
Adolescent connectedness can be characterized along a continuum from conventional to unconventional. The term “conventional” comes from the work of Jessor and Jessor 42 who revealed the role of conventional bonds to societal institutions and its representatives (parents, teachers, police, employers, and, perhaps, health care providers) in preventing or promoting delinquency. In short, when children do not receive consistent, reliable, and sufficiently caring support from parents and other adults, they become teens who do not trust adults to uphold their role as protectors and providers. (Notice, here, how the presence or nature of support one receives leads to their subsequent patterns of connecting and bonding with others.) They come to reject adults, and all that they (adults) stand for; instead, such youth regularly turn to those who do support them and embrace the values, goals, and activities of youth, specifically their friends.
Youth who reject the conventions of adults often come to reject their classmates or peers, too. While sometimes such youth are disconnected from peers because they are temperamentally shy or have been socially rejected, in many cases they view classmates as stooges for the conventional systems of adults and reject them as a result. When youth report being highly connected to friends and to their neighborhood but disconnected from classmates, parents and school, there is ample evidence of an unconventional style of connectedness. Unconventionally connected youth are less likely to effectively seek support from adults than conventionally connected youth, whether the adults are parents or their mentors, teachers, coaches, doctors or therapists. This can hamper their own growth or recovery. Therefore, health care providers may find behavioral change and rehabilitation directives that depend on their patients partnering with adults as health care allies result in non-compliance.
With an understanding of the extent to which their adolescent patients tend to seek out and feel positively towards adults, including both parents and the health care practitioners themselves, relative to their connectedness to friends, romantic partners, or others in locations outside of the home, school, or workplace (like the youth’s connectedness to neighborhood), some IF-THEN decisions can be made about to whom the youth is most likely to turn for (or be willing to receive from) the support they need to implement provider recommended lifestyle changes (described later). Specifically, patients who are disconnected from parents and teachers likely need to become involved in youth-based activities that correspond with the patient directives (e.g., for better eating, exercise, or avoidance of illegal substances). Obviously, knowing a patient is highly disconnected from her parents should lead providers to seek other supportive health care allies, such as the patient’s friends, or perhaps nurse or coach at school if school connectedness is relatively high.
But how can providers know for sure the extent of positive, healthy connectedness their patients have established with various adults and peers in order to guide their selection of health care allies, especially given youth don’t always reveal their disdain for their parents in office visits? In the remainder of this section we describe a second tool, which provides an easily administered, self-report assessment of youth’s connectedness across a range of specific connectedness worlds, and which uses a definition of connectedness that is active, affective, and reflects the kind of directive beliefs about self-and-others that is essential for identifying allies.
The Hemingway: Measure of Adolescent Connectedness7,41 is a publicly available self-report assessment of youth’s emotional and behavioral engagement (i.e., “connectedness”) to fifteen people, places, and activities central to their growth and development. Its can be completed by youth online in advance of a doctor-patient meeting, on paper, using a digital device while in the waiting room, or administered verbally directly with the youth (See Appendix). There also is a parent and teacher report format. To score it, the pool of survey items in the subscale for each of the worlds of connectedness are averaged. These mean subscale scores can be compared with age- and gender-specific normative data (e.g., see Karcher et al.
7
) or transformed to create a z-score (or standardized score) for each individual’s subscale to more easily determine how typical their degree of connectedness is relative to some sample, whether that is the pool of one’s own patients who have completed the survey for the provider previously or some published normative data. For instance, using z-scores we can consider a z-score of 0 as average, 1.0 or larger as “high” and −1.0 or larger as “low” (see Figure 4). Here, high and low indicate the youth’s response is higher or lower than two-thirds (68% or 1 standard deviation) of his or her peers. Similarly, z-scores of 2.0 (that is, 2 standard deviations above the mean of kids their age) reflect scores higher (or lower if larger than −2.0) than 95% of their peers. Studies with large samples, using the scale translated into multiple languages, have provided evidence that the subscales are relatively invariant across boys and girls and most American ethnic group adolescents.41,43 By comparing the level of connectedness in terms of emotional and behavioral engagement with parents, school, and friends, patterns or profiles emerge that may reveal health care allies. Patterns of connectedness don’t reveal from whom the youth receive support, but rather with whom they associate, spend time, and care most about. Connectedness Ecomap with Compass plotted.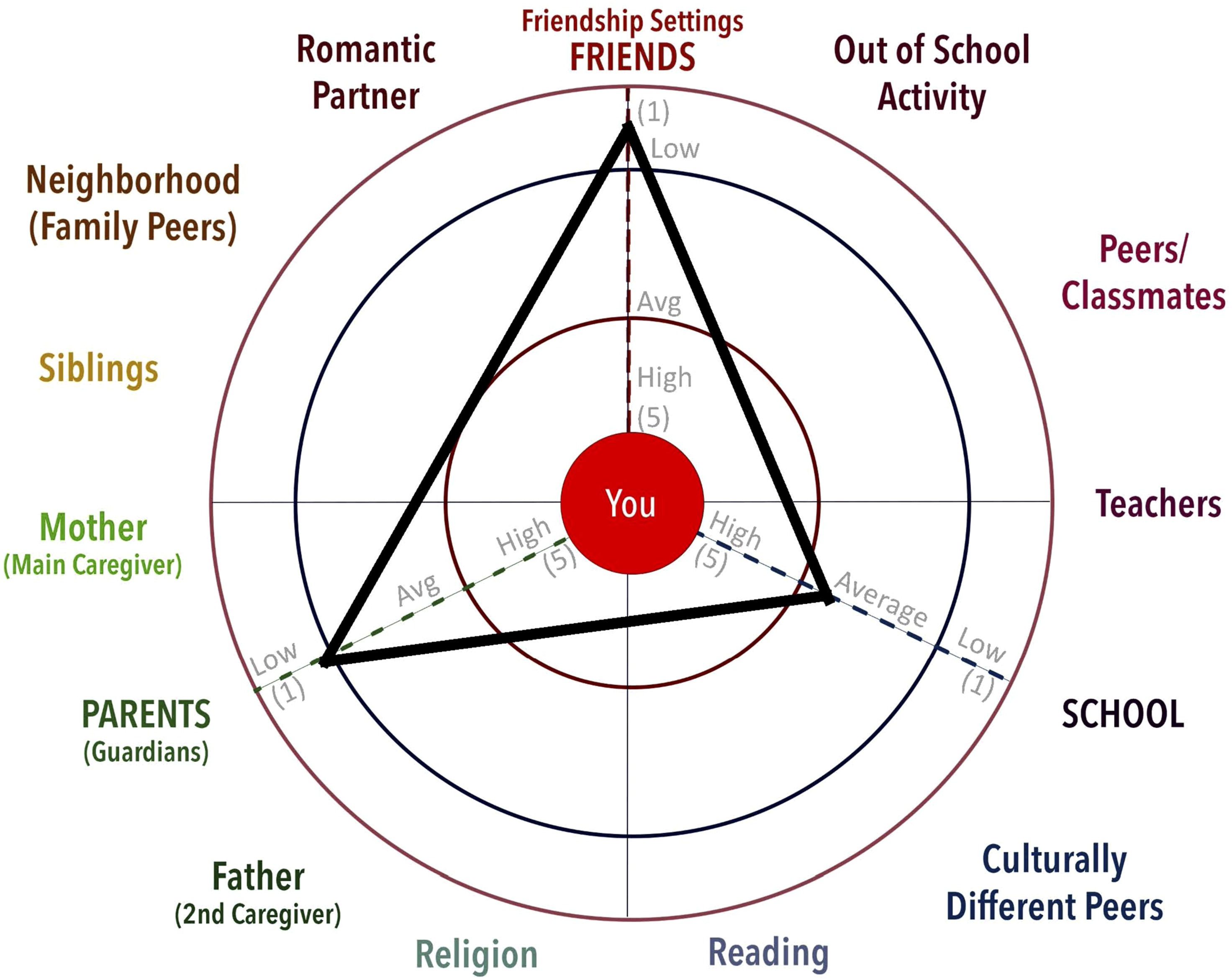
The Correspondence of Webs of Support and Connectedness Ecomaps
Although the web of support and connectedness ecomap profiles tend to correspond, they communicate different information. The web of support reveals typical, current and available sources of support for the youth, while the connectedness Ecomap indicates where youth direct their energy, attention, care and concern. The connectedness Ecomap provides a different view on whom a youth may be most open to listening to and be most influenced by, such that when a health care provider wants to enlist someone in a youth’s life to communicate about and advocate for important behavioral changes it may be helpful to enlist someone to whom the youth naturally turns for information and advice. Sometimes, youth will identify parents, family, or school adults as available and potentially supportive people in their web of support. However, those may not be the people whose opinions the youth value most.
A key factor revealed in patterns of connectedness is what Jessor and Jessor referred to as conventional or unconventional orientation toward others. A conventional orientation reflects an openness by the youth to “conforming to traditional and established networks of the larger society” 41 (p. 36) and acceptance of adults’ values, beliefs and agendas. When youth are low in connectedness to parents, and particularly to school, and high in connectedness to friends, they tend to have an unconventional or “anti-conventional” orientation. For such youth, even if adults are listed in their web as available and helpful, those adults may not be whose opinion the youth values most. Thus, for an unconventionally connected youth, it may be less successful when a health care professional proposes an adult as a possible ally (i.e., “paraprofessional”) to assist the youth in implementing the recommended behavioral changes or post-operative directives than if a peer, friend, or a specific adult to whom the youth reports being connected is the proposed ally.
Plotting a youth’s connectedness to parents, school and friends on the Connectedness Ecomap (Figure 4) can give a quick assessment of whether the youth generally engages in a conventional or unconventional pattern of engagement. This quick three-world screening requires asking just 18 items for the connectedness to parents, school, and friends (see Figure 3), computing these 3 mean scores, and plotting them on the Connectedness Ecomap to form a Compass (Figure 2). Surveying youth, computing the 3 scores, and plotting them on the Ecomap may seem complex, but likely takes less time than some other screeners proposed for use in lifestyle medicine (e.g., Borillo et al 44 ), particularly when the surveying and scoring is automated. As shown in Figure 4, if one plots the youth’s scores for connectedness to parents, school, and friends on the Ecomap and connects those points on the 3 lines, we generate a triangle within the larger circular ecology depicted in the background. The longest legs of the triangle point to where the youth “needs to go” or grow in order to strengthen connectedness.
The longest side of the triangle (its hypotenuse) points to the worlds to which the youth is least connected. With 3 or more scale scores computed and plotted on the Connectedness Ecomap it serves as a Connectedness Compass that points to areas of needed growth in terms of establishing more balanced behavioral and emotional engagement. Additionally, it reveals where in the adolescent’s web of support there may be insufficient support at present (or in the past), because youth tend to connect to those people, places, and activities in their social ecology where they experience the greatest support.
By juxtaposing the youth patient’s connectedness compass against the patient’s corresponding web of support ecomap the practitioner can see the extent to which the patient tends to utilize the supportive people in their lives (e.g., Figure 5). The Web reveals who are the supportive people in each primary context or core, identify the types of support the youth is currently provided in each of these ecological settings, and determine whether there is an anchor to whom the provider might direct the patient to utilize as a health care ally. But the youth’s compass reveals their readiness to utilize this support and also other potential “paraprofessionals” who might lie in waiting, ready to be of use in implementing patient directives for recovery or lifestyle changes.
Most critical as an aid to practitioners is how the Compass may reveal a youth’s general tendency to reject conventional adults that might not be apparent in regular patient visits or even in the Web of Support. The Compass or triangle created in the Connectedness Ecomap can reveal this pattern of connectedness. Unconventional connectedness, which suggests a tendency to turn to peers over adults for support, is present when legs of the triangle or Compass pointing to parents and school connectedness scores are longest and legs to the friends’ connectedness score are much shorter. When this is the case, a practitioner knows this youth may prove difficult to engage in typical post-operative care practices or behavioral lifestyle changes that are dependent on the youth working with adults, such as to coordinate trips to the rehabilitation center, to receive appraisal of the fidelity of their home exercise activities, or to engage in behavioral or lifestyle changes that adults have previously advocated for (and which may have become parent-child battlegrounds between them in the past).
The same pattern of unconventional bonding may appear in a web where the core for friends is closer to the center than the cores for family and school, but the Compass and the Web ecomap can differ, making the use of the Web of Support alone insufficient for such youth. The better assessment of prior supportiveness and current availability of individuals for providing support, such as by parents, teachers, and others, clearly, is the Web of Support. But the web does not reveal the tendency for the youth to take advantage of the range of support available to them. This is why they complement each other as tools a provider can use to identify health care allies.
In summary, not all patients (perhaps not even most) will return from a procedure to an integrated web of supportive family, friends, neighbors and coworker “paraprofessionals,” who are ready to assume supportive functions as health care allies,35,37 as did Jen in the opening example. Jen had a network of supportive individuals who stepped up to ensure that, following the health care procedure, Jen the patient would find post-operative conditions that would ensure optimal healing and procedure efficacy. For many other patients, especially for teenagers perhaps, optimal healing, recovery, and growth requires coordinated supports outside the health care setting; for them, there may need to be strategic efforts made by the health care team to compensate for absent supports in the patient’s life by identifying and enlisting other health care allies. This may require health care providers to assess the patients’ existing web of supportive relationships in order to determine where social supports are readily or potentially available. Yet, sometimes there are supportive, potential health care allies in patient’s lives who are in effect hidden, waiting in the wings to be identified, called into action, and empowered to provide necessary recovery supportive functions. We believe many patients need guidance in identifying and enlisting health care allies who can help them achieve their health care or lifestyle goals.
Using the Connectedness Compass and Webs of Support in Practice: An Illustrative Example
To illustrate our main point that health care practitioners can easily overestimate the adolescent patient’s receptivity to seemingly available health care allies in the youth’s family, we provide a second fictional adolescent case. Figure 5 presents Jon’s Connectedness Compass and his corresponding web of support ecomap. It appears quite different from the web of support profile of Jen that we presented earlier (Figure 2). Recall that those with whom Jen had strong ties were mostly located in cores equally close to her (close to the center of her web); as Jen had a family who rallied around her and friends who made considerable efforts to support her in preparation for surgery and in her post-op recovery. They provided a range of supportive functions and even were able to enlist a potential tie (the coach) by her older brother exercising bridging social capital to facilitate the supportive functions (bonding capital) of her friends. Support Ecomap with Jon’s Web of Support and overlayed Connectedness Compass.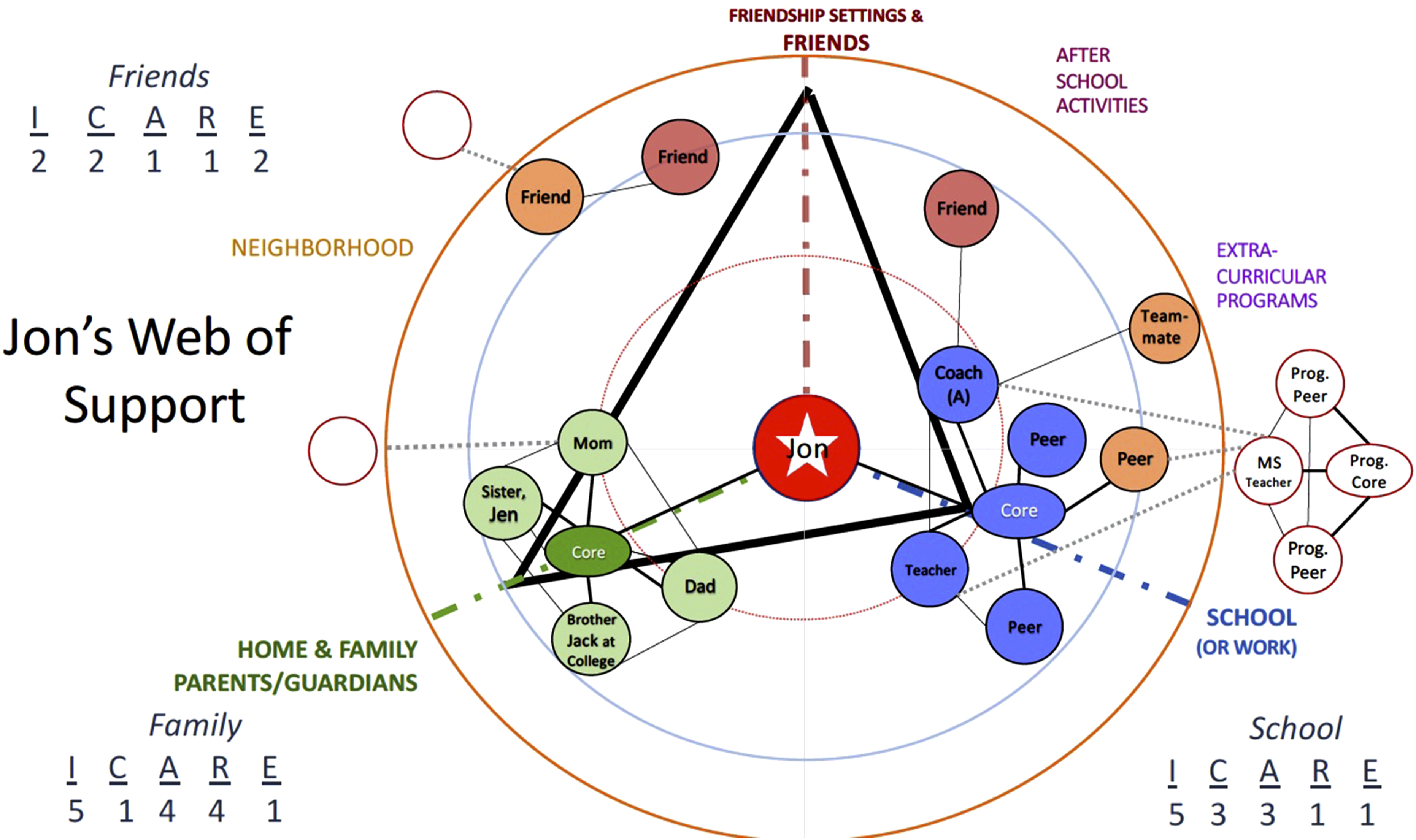
Jon, the adolescent whose Web of Support Ecomap and Connectedness Compass are shown in Figure 5, reveals a quite different pattern of perceived support in his web, and correspondingly, his connectedness profile differs from Jen’s in ways that suggest the same ties or sources of support will be similarly useful health care allies for him. Although Jon, like Jen, reports being most highly connected to school (so his pattern of connectedness is not unconventional), he reports being disconnected from parents and friends. We would assume he comes from a very different family than Jen’s. He doesn’t. This scenario is not uncommon; Jon is Jen’s other brother; they live in the same house with the same parents.
The family’s General Practitioner (GP), having observed how Jen’s family rallied to support her, could easily assume those family would rally similarly for Jon, were he to need support. They might. The GP, having previously observed no antagonism between Jon and his parents at appointments, might assume that Jon would just as readily accept their informational, material, emotional, and feedback support as did Jen. But he didn’t.
A critical point we want to bring home in this paper is that people are as supportive as they are perceived to be by the individual receiving their support; in other words, their support efforts will only be experienced as such when the person being helped is willing to receive their support. The GP who has worked with Jen and Jon’s family for years likely thinks she knows this family, their interpersonal dynamics, and their patterns of intrafamilial support. This is an assumption most GPs should not make blindly; assuming that Jon experiences his parents to be just as supportive as Jen perceived them, could be a mistake with serious medical implications.
Notice that Jon and Jen have some similar elements in their webs of support. Namely, they have the same family members, who tend to provide similar types of support to both Jen and Jon. The main difference is Jen and Jon’s patterns of engagement or styles of connecting (their compass). Jen seeks out and feels emotionally engaged with her parents (high parent connectedness), while Jon interacts less frequently and feels less positively toward them than Jen does. His parents are not placed on his web of support as close to the center as they are in Jen’s web; but their location in the 2 webs is not so different as to reveal their parents are not ideal health care allies for Jon. They provide similar types of support; it’s just that Jon does not utilize their support or seek it usually. Despite their apparent readiness to support Jon, his lack of engagement with them (i.e., his low scores on his connectedness to parents) reveals they are not people who he tends to seek out, spend time with, and care about; Jon does not perceive them as helpful supporters. Jon also reports few supportive friends and no friend as an anchor. Therefore, the GP should not expect Jon to receive the same level of support from his family and friends as Jen did. Jon’s connectedness style is neither conventional (prioritizing adult influences) nor unconventional (relying on peer over adult support), and neither the family nor friend cores include an anchor.
Rather, Jon connects most with people at school, and the GP’s awareness of this, gained through assessing Jon’s web of support and connectedness profile, provides her with 2 rewards. First, it raises a red flag and reveals the GP cannot assume Jon will seek social support from family and friends as Jen did. Second, Jon’s web provides the GP additional information that allows her to think creatively either about how to buttress any behavioral lifestyle changes Jon might need to make or how to locate needed support for Jon were any major medical procedure recovery required.
This GP is familiar with the role of connectedness and social support in health and recovery. She knows, for example, that youth with insufficient connectedness to friends often fare worse following surgery.11,30 She also is aware that for youth who are connected to school, support from a teacher or coach can play a vital role in their mental and behavioral health.10,13 As a result, this GP was ready to enlist adults from the school setting when there was need for a support system to assist in the implementation of lifestyle behavioral health changes beyond the health care setting. She saw from his web of support that Jon felt supported by his coach and health careers class instructor. This helped clarify to whom at school he was most connected. Because Jon already moved relationally toward these people at school, it was those adults who might most realistically be enlisted as allies to provide support to Jon, rather than his family or friends.
This opportunity for enlisting support for Jon outside the health care system arose a year after Jen’s surgery, when Jon’s annual bloodwork panel revealed elevated liver and kidney functioning. Specifically elevated were the AST enzyme and the urea. The GP spotted these abnormalities and a specialist later conferred the significance of these problems. But the cause was indeterminate. The only possible causes that either doctor could surmise for these problems were all lifestyle related, not any underlying physiological issue to be treated with medicine or a medical procedure. The elevated AST and urea needed immediate behavioral lifestyle changes. When the GP reported to Jon and his family the abnormal liver and kidney functioning, she subsequently discovered 1 possible cause for the enzyme elevations could be excessive dietary supplement intake by the youth. Daily, Jon took a number of dietary supplements to increase his muscle building efforts at the gym, including creatine, pre-workout energy powder, whey protein powder, and sought additional protein supplementation through a diet high in meat. All of these, individually and collectively, have been implicated in liver and kidney functioning.45–48 How did the GP advise the teen to manage this in a way that capitalized on what she had learned from Jon’s Connectedness Compass and his web of support ecomap?
Understanding Jon’s perspective on the supportiveness of his family, and specifically Jon’s tendency to seek out (i.e., connect to) and feel supported by, adults at school and specifically those supporting his body-building efforts, the GP was able to see that Jon’s parents would be only minimally helpful in helping Jon reduce his excessive protein intake. That is, his parents might not be effective in changing Jon’s attitudes about the safety and necessity of the dietary supplements that could be responsible for his health issues. Therefore, in order to capitalize on the direction Jon was already moving toward school-related adults and those he felt supported by, this GP thought outside the box to create an innovative intervention in which Jon might be helped by helping others with the encouragement and direction of the adults at school to whom he was most connected, namely, his coach whom he listed as his only anchor.
Jon’s GP synthesized 3 sources of information to develop her proposed behavioral lifestyle intervention. First, she realized Jon needed a shift in his beliefs about the necessity and safety of dietary supplementation for teens and could see from Jon’s web of support that his family was not going to be a trusted source of information and emotional support for such a change. Having seen the location of his parents so far from him in the web of support and seeing how Jon and his family discussed the possible problems these dietary supplements might be causing him left him feeling shamed and criticized by his parents, the GP surmised adults at school might perform this informational and appraisal or feedback support role better.
Second, the GP was aware that Jon’s deficits in connectedness to friends was a problem needing to be addressed and which could complicate subsequent health care intervention effectiveness.11,20 Recognizing his disconnection from peers was a problem, the GP understood she could help boost his connectedness, thus improving his health10,49 She saw the need to help boost Jon’s connectedness to peers, that might also foster friendship formation, by increasing the time he spends with peers and in activities that allowed him to express his caring for them (to elicit their reciprocated support) and strengthen ties with them.
Third, this GP was aware of both the literature on ways to enlist teachers, peers and paraprofessionals in promoting connectedness,19,35 and research suggesting that learning and attitudinal changes through service might provide a unique means of leveraging attitudinal and behavioral change for Jon regarding the need for supplements. Teens and adults often experience changes in beliefs and attitudes through their service to others as coaches, mentors, and peer-teachers related to lifestyle behaviors.20,31,32,50,51 With the parents’ permission, as well as Jon’s assent, the GP contacted both Jon’s coach and the health class instructor at Jon’s school. Learning that a group of high school students regularly worked with younger children as health-related peer mentors and class topic speakers, 52 she suggested Jon might be a valued guest speaker at their partnering middle school on the topic of the good and bad of protein supplementation for body building 53 and dietary supplementation in general. 46 She suggested this could be done in person as well as virtually and thus his talks and peer coaching could supplement the existing virtual delivery of health information. 54 Both adults also saw the need for Jon to find ways to make more friends, and agreed with the doctor to encourage Jon to take a lead in informing peers about the consequences of excessively high protein consumption. They agreed this might both provide him a peer context in which to engage in prosocial peer interactions and indirectly influence his own beliefs and behaviors related to his own dietary supplementation practices. 11
But this creative health care and lifestyle-change intervention would not have become apparent had the GP not been able to access information on Jon’s web of support and his connectedness profile. More specifically, the GP doctor learned from the Web of Support interview, which was completed by her office staff before annual visits, that Jon prefers to work with adults by assuming leadership roles at school, as this was revealed by multiple examples Jon gave about teachers support (positive appraisal) and that Jon feels affirmed and supported when teachers see him as helpful, committed, and having leadership potential. The GP was able to identify and reach out to the coach at the school who Jon had identified as his only anchor. This gave the GP a point of contact at the school, Jon’s coach, to share what she’d learned about Jon’s positive interest in body building but perhaps unwise use of extreme protein diets and supplements, and subsequently to seek the anchor’s ideas about how to help others.
One year later, Jon had become part of a peer mentoring outreach program at this school, 55 where he could discuss the harms of protein powder with middle schoolers in a structured setting (after school) that also offered opportunities to build friendships with other peers his age by engaging in conventional, prosocial activities of leadership, play, and instructional guidance to younger teens. The doctor thought that the lifestyle-change directive (less protein and supplement use) would be more likely to take hold if it could capitalize on the youth’s tailwind toward school engagement. Simultaneously this could address the headwinds Jon faced to finding new friends. This approach to lifestyle changes was considerably more effective than just telling Jon and his family to stop protein supplementation. These ideas for how to take charge of change behaviors would not have emerged without learning about Jon through the web of support interview and ecomap construction activity as well as the connectedness survey, mapping, and compass use.
Integrating Psychosocial Assessment Tool Data to Improve Health Care Service Outcomes
Our premise is that doctors (with office staff), health care providers, and even counselors and therapists can use assessments of Webs of Support and Connectedness and mapping activities to guide their efforts to develop beyond-the-office prescriptions for lifestyle changes or post-procedure care or intervention directives. We think doing so might radically improve the outcomes of their treatment efforts but also expand the benefits of their doctor-patient care regime by thinking outside the box.
We assume that following the use of these assessments and efforts to provide feedback and explain profiles to patients in the service of helping patients build their webs of support in ways that foster healthy lifestyle changes health care providers would generate new ideas about how to help structure patients’ out of the office activities and thereby have a double-impact from their interventions or procedures. First, the uptake or implementation of their post-care directives by patients would lead to higher treatment success rates (e.g., from greater adherence to post-surgery physical therapy). Second, they might effect changes in their adolescent patients' webs of support and the strength of their conventional connectedness to adults and peers that influence additional benefits for patients. A third benefit might be that providers develop a new set of questions to ask the child/youth patient and parents that allow a range of new post-care prescriptions or doctors directives, allowing the incorporation of health care goals and recommended activities beyond what they did previously, and that could leverage greater recovery and health promotion through a wider range of prescriptions for physical activity, eating, and goal-setting (related to engagement and support) in ways that previously seems not the purview of their traditional role.
Were providers to conduct these assessments at least annually and have visual and statistical comparisons reviewed and discussed annually with patients, this could help the providers get to know their adolescent patients differently and come to see a wider picture of what’s changed in their patients’ lives in the past year. By reviewing patients’ connectedness and social support levels over time, providers may discover new strategies to promote health (such as obesity prevention), help patients set future goals, and identify new relationships that could be sought by patients and their families to leverage improvements in health. For example, a child who is isolated at home and from peers may engage in excessive hours of video game playing to avoid family and in the absence of peers or ways to see friends in an isolated neighborhood, leading to obesity. But this youth, whose connectedness compass looks like that shown in Figures 4 and 5, is highly connected to school. This is the direction the child is already moving (school connectedness); so might there be ways to capitalize on this tailwind to counter the headwinds posed by low parent and friend connectedness? Could engaging the child with peers at school in a manner that also created a second home for the child serve to offset or address the absence of caregiving and lack of information communicated at home by parents that might correct poor eating habits (low parent connectedness) and address the absence of friends outside of school (low friend connectedness). Seeing this connectedness profile, a doctor might, for example, encourage the child to engage in peer mentoring program for obesity at the school, either as mentee or mentor, as a way of influencing beliefs and boosting social connection.52,55
The diagnostic decision-making flowchart shown in Figure 6 starts (at left) with the question, “Is patient change highly influenced by compliance or support from others?” If patient change is not heavily dependent on support from others (see “No” arrow), then there is only 1 situation in which a modification of the standard behavioral change procedure is warranted. That’s when change is context specific and the youth is not connected to others in that context. In such a case, one should look to the patient’s Web of Support Ecomap to see if there are Anchors (adult or peer) who may be helpful to enlist in supporting the patient’s behavioral change. A decision-making flowchart for using ecomapping and connectedness assessments.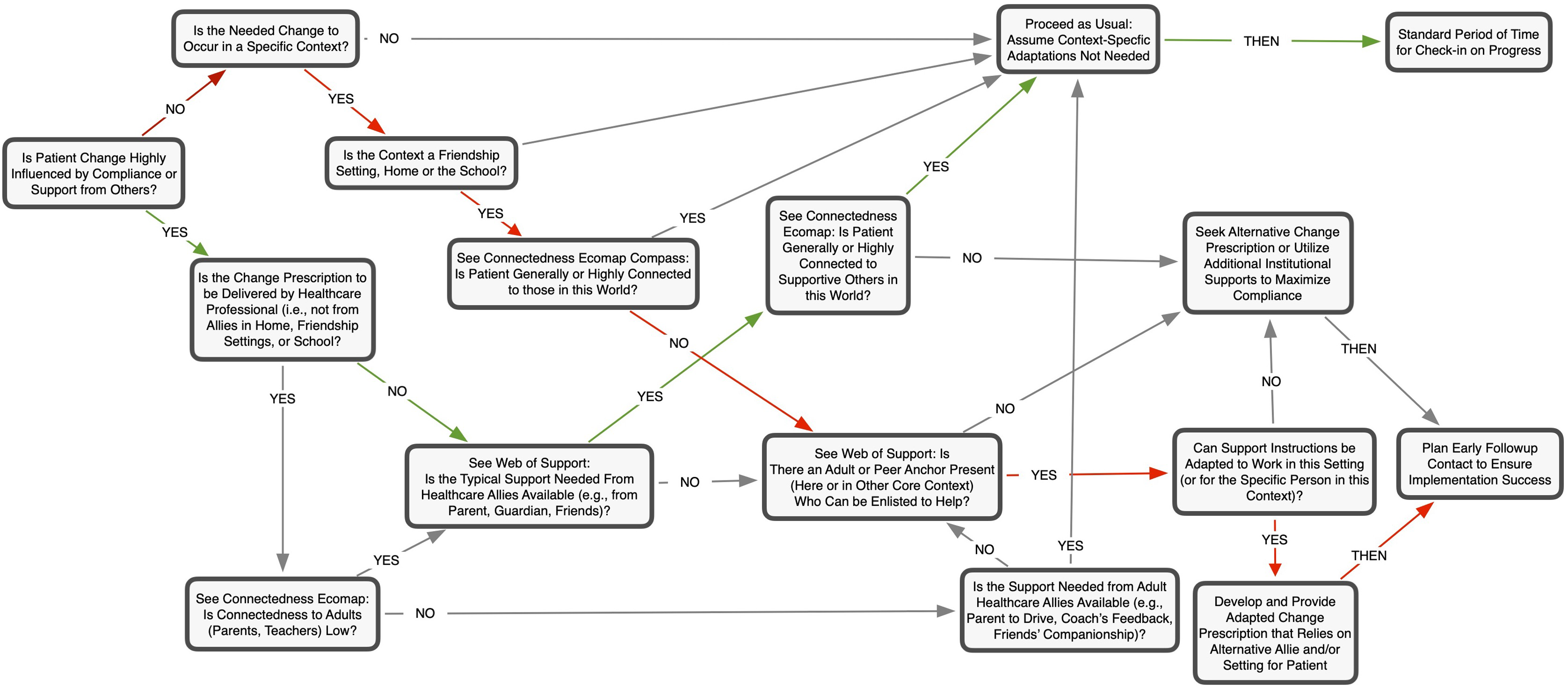
When the success of the behavioral change prescription (i.e., successful compliance with post-op or rehabilitative procedures) is highly dependent on others (either health care professionals or non-professional allies or both) then a series of binary questions can be useful. Answering these questions, using data from the Connectedness and Web of Support Ecomaps can help determine when a health care provider should consider making modifications to the change prescription for the patient or those helping her (bottom right textbox), when to secure additional professional supports to facilitate the original change prescription, or when to seek an alternative change procedure altogether. These decisions help identify 2 situations. The first is when working with a patient who has an unconventional form of connectedness (i.e., is a youth likely to reject adults’ help) that is likely to result in their rejecting needed support and assistance from adults. The second case that the question reveals is when there is either an absence of needed support in a specific core context in a youth’s life or when the more effective ally for the patient’s behavior change is someone other than who the provider might typically assume would provide the needed help.
Identifying a youth’s world of greatest disconnection—viz the world to which the longest legs of their connectedness compass point—can reveal whether the youth’s current pattern of connecting to the world will present tailwinds to the health care directives (assisting their implementation) or pose headwinds that push against effective implementation of prescribed lifestyle-change directives. Lifestyle medicine practitioners efforts to uncover patterns of connectedness can reveal these tailwinds and headwinds that then can be factored into treatment plans and specific health care directives. These winds can reveal likely on-the-ground barriers and uncover hidden allies that may buttress a health care provider’s prescriptive.
Limitations, Constraints & Considerations
All health care data collected on minor patients is subject to HIPPA regulations related to releasing information to parents of minors upon request, and these data on perceived social support and forms of connectedness would be subject to such regulations; but especially when treating adolescents whose situations are like Jon’s it might be more concerning to such youth were their perceptions of who are supportive, caring, and available individuals in their lives to be shared with their parents, specifically, but also with individuals the practitioner might seek out directly to enlist as a health care ally. This means that youth should be informed that this information is, under certain circumstances, accessible to their parents. More importantly, however, is the need to communicate to the youth that any information the practitioner might want to share with parents in an effort to work with them to solicit supports in and beyond the family would, in most cases, be discussed with the youth prior to disclosure to parents. Conversely, at the conclusion of the web of support interview, it may be useful to inquire directly as to whether there is information on their web of support ecomap that they would prefer not be included in discussions with parents or others.
Time constraints may dictate the extent of the interview that is conducted as well as the manner of collecting the data. To fully complete the web of support interview in person, for instance, can take upwards of 45 minutes; whereas, to collect just the basic information on who are the supportive people in their lives can take less than 10. A fully detailed web of support ecomap—one that includes the designation of anchors, lines drawn between those supportive individuals who know each other, and careful placement of such individuals according to the frequency of contact and importance—can provide information to practitioners that is very useful to identifying possible supportive allies. But in some cases, time constraints may make this unfeasible. Therefore, virtual or online delivery of these assessment tools outside the health care office, as well as the use of automated scoring tools, may be a more efficient option for some providers. However, in-person questions or surveys may be required for youth with auditory, visual, or language processing limitations, thereby eliminating an online data collection option.
It may be necessary to start small, so to speak, by selectively using these tools in order to both see their value and work out the kinks in data collection, retention, and interpretation. Some practitioners may choose to use the tools selectively, such as when evidence of absent support is present for a given youth. For example, when a pattern of disconnection from family is revealed in the connectedness Ecomap, practitioners may see this as an obvious situation in which a web of support map is needed to know who to enlist in post-procedure directives. Alternatively, some providers may want to see evidence of the value of using these tools before deploying them routinely to all patients. However, we believe it is in the best interest of most providers (and their patients) to collect the data regularly, systematically and universally so that a normative database can be developed. Developing this local, normative database will help practitioners compare patients’ data to the typical levels of support and connection reported by their adolescent patients, revealing how much any given youth presents a unique pattern of support and connectedness relative to others.
Conclusion
The call for health care practitioners to use screeners for lifestyle factors at annual visits and for screener data to be factored into a wider view of the general practitioner’s approach has grown in recent years, with many such tools appearing in this journal.43,56–58 The importance of screening to assess for the quality of social relationships, engagement and support also has established its importance as a predictor of mortality risk, general health, and procedure recovery.9,11,20,30 The tools and methods introduced in this article add to the set of tools that may assist health care practitioners in the use of social relationship quality screeners not only to estimate presenting risks for patients, and for children and adolescents specifically, but also may provide a wider array of options for prescribing support, interventions, and healthy lifestyle changes beyond the health care setting.
The screening approach introduced here may provide a unique set of tools to add to those that comport with the “connection prescription” proposed by Martino et al 11 who argue that “counseling patients on increasing social connections, prescribing connection, and inquiring about quantity and quality of social interactions at routine visits are ways that lifestyle medicine specialists can use connection to help patients to add not only years to their life but also health and well-being to those years.” 11 (p. 466). They propose a number of specific metrics to be gathered, many of which are captured in the web of support and connectedness assessment profile described here, such as the frequency and the quality of these social interactions.
Martino et al 11 acknowledge that incorporating the connection prescription approach fully in one’s practice may present some challenges, such as the additional time needed to undertake this approach, but suggest the benefits may outweigh the costs. As we and they note, simply asking about social relationships and their accompanying supports could facilitate a huge step in a positive, healthy direction. 59 We fully concur with this assessment, but add that once this additional information is considered—namely, the awareness of the importance of connection, the knowledge of the degree of support in their patients’ lives, and their patients’ tendencies to engage in some ecological settings and relationships more than others—many lifestyle medicine practitioners may soon imagine a wider range of viable and compelling prescriptions for connection. Collaboratively generating this understanding with patients can yield measurable benefits to treatment satisfaction, health outcomes, and patient retention.
Footnotes
Acknowledgments
The authors acknowledge the invaluable contributions that Dr Shannon Varga made in developing the original Webs of Support theoretical framework.
Author Contributions
Both authors made equal contributions to the conceptualizing and writing of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Statement
Data Availability Statement
There are no data to share from this paper, but the materials associated with these assessment tools, including blank and editable versions of the Ecomap sheets, Web of Support Data Collection Form, and Connectedness Survey, as well as Excel based data scoring file and manual for the Hemingway measure are all available free of charge from the first author and online at websofsupport.com and ![]()