
Abstract
Purpose
Evaluate a group-based, trauma-informed health coaching model based on Lifestyle Medicine pillars, delivered by community health coaches, to improve health behaviors and mental well-being for vulnerable populations.
Methods
This program evaluation analyzed quantitative longitudinal data with linear mixed models and qualitative data with reflexive thematic analysis. Participants (n = 720) were low-income adults referred through Federally Qualified Health Centers (FQHCs), who participated in weekly 90-120 minute groups for 3 months. Data were collected via monthly surveys, including the PHQ-9, GAD-7, UCLA 3-item loneliness, exercise as a vital sign, a 2-item dietary screener, and 3 qualitative questions.
Results
Participants saw significant reductions in depression, anxiety, and isolation, and significant increases in daily servings of fruits and vegetables, and weekly minutes of exercise. The qualitative analysis identified 4 themes related to the drivers and reinforcers of positive behavior change and improved mental well-being.
Conclusions
Initial data suggest this model helps reduce depression, anxiety, and isolation, and promotes positive behavior change within populations most impacted by health inequity. Qualitative results identified drivers of positive change, such as creating a sense of belonging and mutual support. Future research should consider how to continue to scale this program to a variety of populations and across different settings.
Keywords
“Our research focused on community-based health coaching utilizing group interventions and led by certified health coaches as opposed to medical professionals or specialists.”
Introduction
As lifestyle-driven chronic conditions eclipse acute illnesses as the leading cause of mortality worldwide, identifying and implementing strategies that promote healthy behaviors has become paramount.1-4 Increasingly, lifestyle medicine is being used to prevent, reduce risk, and treat chronic disease through its emphasis on 6 health behaviors. These behaviors include (1) nutrition (predominantly whole food, plant-based); (2) daily physical activity; (3) sufficient sleep; (4) cultivating stress management techniques and behaviors; (5) avoiding risky substances such as alcohol and tobacco, and (6) social engagement. 5 Beyond physical well-being, lifestyle medicine incorporates psychosocial well-being, due to the bi-directional relationship between mental health and lifestyle.6,7 Research shows that engaging in health-promoting behaviors (e.g., regular physical activity, plant-based diet, social engagement) can mitigate symptoms of anxiety and depression and promote positive mental states which help reinforce these behaviors, creating a virtuous cycle of well-being.6,8-12 Such findings underscore the importance of improving health behaviors to address both physical and psychological dimensions of health.6,13
While the increasing body of evidence related to lifestyle medicine demonstrates its significance in managing chronic disease and its potential to improve mental well-being, simply telling patients to “eat better” or “exercise more” has not produced a healthier population.14,15 Unlike the well-built infrastructure for medications (i.e., medications covered by insurance, an extensive network of pharmacies, and available pharmacists to address questions), there is no comparable infrastructure for “behavioral prescriptions.” They are infrequently covered by insurance, lack a central location to fill them, and have highly variable expertise in a frequently unregulated market. This well-intentioned advice from physicians fails, in part, because of a delivery problem: it lacks the specific details associated with the gold standard for a pharmaceutical prescription, for example, type, dose, frequency, duration, and therapeutic goal. 16 This advice also fails because of an equity problem: under-represented minorities negatively impacted by social determinants of health (SDOH) lack the finances and access to healthy food, safe places for physical activity, external support such as health coaches, and social engagement that are taken for granted by those with privilege.13,17 Campbell and colleagues 18 showed that people with lower incomes were more than 50% less likely to follow the behavioral advice given to them, and more than 70% less likely to follow through on recommended health tests (e.g., cholesterol and blood sugar), citing cost and lack of accessibility as primary reasons. Further, lack of access to nutrient-dense food and opportunities for physical activity creates a self-perpetuating cycle of poor health behaviors and health outcomes across the lifespan.19-22 These social determinants of health, such as income, education, neighborhood conditions, and access to health care, come at a cost. The National Association of Chronic Disease Directors’ 2023 report attributes a third of total annual deaths in the U.S. to SDOH factors and estimates that eliminating racial and ethnic disparities would reduce indirect costs of excess morbidity and mortality by more than $1 trillion over 3 years. 23
While research suggests that lifestyle medicine is one of the most effective ways to address SDOH and achieve health equity24,25 there is concern whether lifestyle medicine can drive the widespread behavior change needed to significantly impact population health, warning that it could also deepen existing health inequities.1,24,26,27 Of particular concern is lifestyle medicine’s focus on individual-level care which insufficiently addresses the upstream social determinants of health (SDoH).13,27 A new, community-engaged model of lifestyle medicine offers promise for extending the benefits of lifestyle interventions to vulnerable populations while mitigating the risk of worsening health inequities. 1 It provides culturally sensitive programming and access to lifestyle medicine interventions through community health workers, freeing the time of health care professionals with limited time to adequately address lifestyle behaviors in their consultations. 24 This paper provides a program evaluation of one such approach, Open Source Wellness’ Community As Medicine model, on patient-reported outcomes related to health behaviors and mental well-being. (Physical health outcomes for a different sample of patients can be found in Rosas et al, 2024. 28 ) This model incorporates a community-delivered and clinically integrated approach to provide accessible, trauma-informed, and culturally relevant lifestyle/behavioral medicine to those who need it most: underserved populations who struggle with poverty, unsafe environments, and upstream drivers of chronic disease.
The Community as Medicine™ Model
The Open Source Wellness (OSW) Community as Medicine (CAM) model is a group-based health coaching model that is designed as a “behavioral pharmacy,” providing an affordable and accessible delivery system to support health behaviors that drive human health and well-being. 29 The CAM model was created as an effective way to facilitate the adoption of behavioral prescriptions, such as “eat better, exercise more, and reduce your stress” through experiential groups and activities based on the principles of lifestyle medicine.29,30 It includes foundational components of the Social Ecological Model (SEM), which considers the social environment of a person, such as in their relationships with family, friends, or local community groups, and posits that behavior is shaped by social connections, and connection is vital for healthy behaviors and ultimately a person’s health. 31 The CAM model centers on 4 pillars of lifestyle medicine: MOVE (physical activity), NOURISH (healthy meals), CONNECT (social support), and BE (stress reduction) which are guided by health coaches as well as peer leaders. 32 CAM group health coaches are trained in a trauma-informed, culturally humble approach to coaching, to achieve positive health outcomes for a diverse group of individuals facing challenges in physical, mental, or social well-being.33,34 This training helps coaches understand trauma’s impact and how it can manifest in behaviors and health outcomes to minimize the risk of re-traumatization and promote resilience and recovery. This is particularly important as OSW works predominantly in Federally Qualified Health Centers (FQHCs), low-income housing, and in partnership with community-based organizations like YMCAs that may serve adults who have experienced trauma.
OSW works in partnership with clinics and communities to support healthy behaviors in individuals who struggle with behaviorally mediated chronic diseases, such as heart disease, diabetes, depression, and anxiety, as well as food insecurity, social isolation, and other health challenges that are impacted by SDOH. New participants are enrolled into CAM groups monthly on a rolling basis to encourage peer support and positive health behavior influences through social/peer modeling. Participants have the opportunity to learn key skills to improve health behaviors and knowledge, gaining self-efficacy as well as collective-efficacy due to the group design. An emphasis is placed on peer group connection to reinforce healthy behaviors and provide social support and observational learning whereby participants learn from each other’s experiences. 31 During the 12-week in-person or virtual program, CAM groups meet weekly, including both large group time when they engage in physical activity, nutrition education, social support, rest/stress reduction, and small-group health coaching time. Some CAM participants also receive weekly deliveries of locally grown produce during the program as part of a partnership with a local “Food As Medicine” program.
The CAM model also provides a way for clinics to provide supportive behavioral health services that are financially feasible and sustainable. Because health and wellness coaching is not yet typically covered through a reimbursable insurance billing code, novel methods are currently needed to meet the financial requirements of the healthcare provider while simultaneously delivering quality care to those who need them. 35 CAM utilizes a group medical visit (GMV) model recognized for providing improved access to health care and better behavioral outcomes for patients, combined with increased efficiency and reduced burnout for providers because responsibilities are delegated to coaches and the providers’ time is optimized.36-38 The CAM model transfers many of the responsibilities of the physician to the coaches, who are responsible for enrolling and on-boarding patients, engaging them in coaching sessions, maintaining the relationship between sessions, serving as the first level of support if challenges arise, and escalating issues to physicians when necessary. Since coaches are responsible for the majority of the patient relationships, physicians can focus on medical check-ins, allowing them to be far more productive in terms of visits per hour and billing than they otherwise would be. While the CAM model provides benefits to both patients and providers (such as addressing burnout, moral injury, and the monotony of high-volume individual visit schedules), this program evaluation focuses on patient benefits. Specifically, it assesses the effectiveness of the OSW CAM model in reducing depression, anxiety, and social isolation, and increasing minutes of physical activity and the consumption of fruits and vegetables, all of which are associated with better mental and physical health. 30 It also presents qualitative findings describing participants’ insight into the impact the program had on their lives including an increased sense of belonging, meaningful communication, mutual support, and increased self-worth.
Methods
Study Intervention
The CAM model is an experiential and accessible health coaching model focused on 4 transdiagnostic behavioral prescriptions: Move, Nourish, Connect, and Be (see Figure 1). CAM groups meet weekly for 60-120 minutes depending on the needs of the clinic and patient population. The groups included in this program evaluation were 90-120 minutes long and consisted of the following structure: 15-20 minutes of socially engaging physical activity accommodating various mobility levels, 5 minutes of mindfulness meditation, a 10-minute interactive lesson on varied health topics, a 5-minute nutrition lesson combined with a plant-based snack (e.g., apple), and 30-45 minutes of small-group health coaching. Participants also received a weekly produce delivery consisting of approximately 10 servings of fruits and vegetables, delivered by Dig Deep Farms, a farm that utilizes regenerative agricultural practices and provides job training to people with barriers to employment. The nutrition lesson during groups would focus on the produce delivered that week to support patients in utilizing it. The partnership between clinics, Open Source Wellness, and Dig Deep Farms was supported by Recipe4Health, an Alameda County Health initiative. Community as medicine (CAM) model.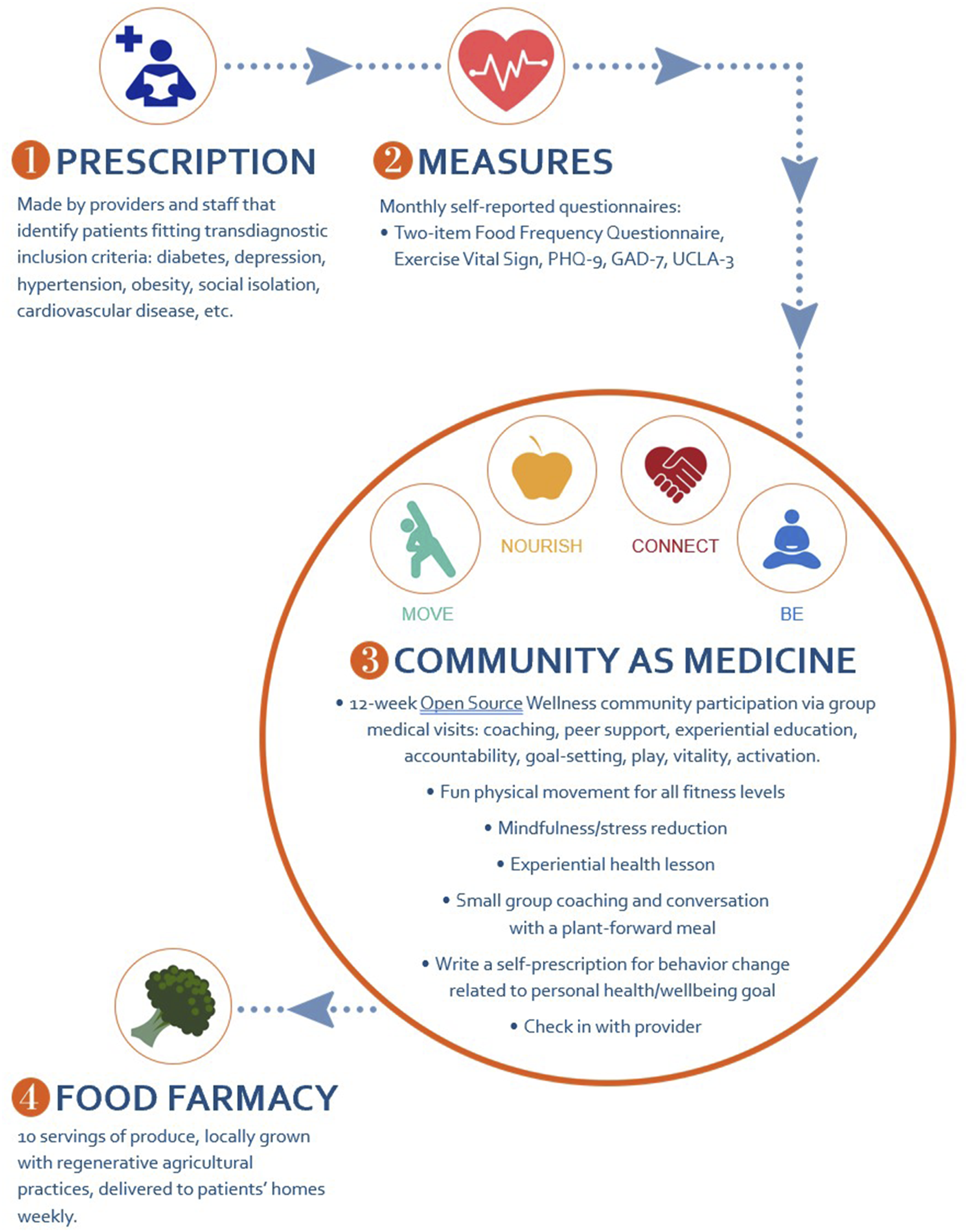
Mindfulness Meditation
The mindfulness meditations were guided and general in nature, and were designed to be accessible to participants with minimal experience with mindfulness. They were led by the health coaches and covered a variety of practices, including focusing on breathing, gratitude, progressive muscle relaxation, and mindful eating.
Healthy Foods and Access
The snacks provided were plant-forward, meaning that they are predominantly but not strictly vegan. This is both because the data demonstrating its health (e.g., plant-based eating led to greater improvements in diabetes than the American Diabetes Association dietary guidelines, 39 and to simplify dietary concerns for participants. Critically, participants were not instructed to follow a specific diet. Instead, general dietary principles (i.e., increasing vegetable consumption, decreasing sugar intake, etc.) were discussed and applied. Coaches focused on each participant’s goals with regard to diet and nutrition, with an eye on their focus on diet and culturally relevant recommendations. For example, 1 participant’s goal was to change from triple cheeseburgers for lunch to double cheeseburgers, a goal which was supported and applauded.
Health Coaches and Peer Leaders
The interactive didactics covered a range of health and well-being topics, such as eating healthy on a budget, increasing physical movement with daily activities, setting interpersonal boundaries to both deepen and limit relationships, and goal setting. Coaches were largely (but not exclusively) trained in National Board for Health and Wellness Coaching (NBHWC) approved programs, 40 and underwent ongoing training and supervision. Coaches were supervised by a senior health coach trainer and 2 clinical psychologists who developed and deliver OSW’s NBHWC approved Community As Medicine Health Coach Training Program.
The small-group health coaching expanded on the didactic topic of the day, and focused on goal setting, motivational interviewing, and social support. Each group was supported by a peer leader who had previously completed a 3-month cohort and subsequently applied for and been accepted to the peer leadership program.
At the close of the small-group coaching, participants wrote personalized “behavioral prescriptions” for their goals that week (e.g., try 1 new vegetable, walk for 15 minutes 3 times this week, replace one can of soda with one glass of water). Each small group also had a group text thread which coaches and group members utilized for group continuity, accountability, and support.
The clinically integrated groups utilized a group medical visit model, in which a primary care provider would conduct short individual medical visits with participants, improving patient care in several ways. This allowed for much more frequent patient contact, as well as clear longitudinal tracking (i.e., weekly vs annually). It also supported patients seeing the impact of their behavior change on their health outcomes.
Participants and Setting
The sample for this program evaluation consisted of 720 patients who were seen at 2 Open Source Wellness sites, a group medical visit held at Hayward Wellness Center (HWC, n = 437), a Federally Qualified Health Center (FQHC) in Hayward, California that is part of Alameda Health System, and a community site which received referrals from FQHCs from around the broader East Bay, primarily Alameda County, as well as self-referred individuals (n = 283). Participants joined 3-month cohorts, attending weekly 90-120 minute meetings. New participants joined a cohort the first week of each month. This created a constantly rotating group of new participants and experienced participants which facilitated building group culture. Patients were referred to OSW Community As Medicine groups by clinic staff members including their primary care providers, dietitians, clinical pharmacists, social workers, and medical assistants. Participants were English-speaking or Spanish-speaking (separate groups were run for English vs Spanish-speaking participants) adult patients, referred for a wide variety of behaviorally mediated chronic conditions including diabetes, prediabetes, cardiac disease, hypertension, obesity, anxiety, and depression. Patients who screened positive for food insecurity, as assessed by clinic staff, were also referred, due to the broad literature linking food insecurity with chronic disease.41,42 Exclusion criteria included acute suicidality and inability to participate appropriately in a group setting, both determined by the referring provider and secondarily screened by the OSW referral team. There were no other inclusion or exclusion criteria.
The data used in this evaluation were completely de-identified. As such, these data were not considered human subjects research data and were not reviewed by an Institutional Review Board. This decision was made in consultation with the Alameda Health System Institutional Review Board.
Survey Design
Self-report questionnaires were used to assess diet, exercise, and mood on a Likert scale, and 3 open-ended questions were included to collect qualitative data. The questionnaires included these measures:
Two-Item Food Frequency Questionnaire
This questionnaire asks participants how many servings of fruits and vegetables they have eaten in the past week. It has been validated against longer measures of food intake.43,44
Exercise Vital Sign
This two-item questionnaire assesses the number of minutes of moderate or vigorous activity engaged in per week. It has been found to have good face, convergent, and discriminant validity and is more conservative than population-based surveys, potentially reflecting decreased response bias.45,46
Patient Health Questionnaire—9 (PHQ-9)
The PHQ-9 is the most widely used assessment of depression and shows excellent sensitivity and specificity when compared with structured clinical assessments. The PHQ-9 is a reliable and valid measure of both depression and depression severity, demonstrating good internal consistency (α = 0.83 - 0.92), convergent and discriminant validity and responsiveness to change.47,48
General Anxiety Disorder-7 (GAD-7)
The GAD-7 is a 7-item scale, based on Diagnostic and Statistical Manual of Mental Disorders-IV (DSM-IV) criteria, used to identify likely cases of general anxiety disorder. The GAD-7 Scale has undergone validation in extensive patient samples across various nations through multiple studies. It has been found to have excellent psychometric properties and is used extensively in remote health surveys, epidemiologic studies, and primary care settings. 49
UCLA Loneliness Scale (UCLA-3)
The UCLA-3 is a 3-item scale, 50 adapted from the Revised UCLA Loneliness Scale (R-UCLA) 51 that was developed for use as a telephone survey. The UCLA-3 is used to measure 3 dimensions of loneliness: relational connectedness, social connectedness, and self-perceived isolation. The UCLA-3 has been culturally adapted across several countries and societies and has been validated in individuals with physical and mental disabilities in clinical settings. 52
Qualitative Questions
Three questions related to (1) the role of the coach in providing support for behavior change; (2) the perceived impact of the program on the participants’ lives; and (3) suggestions on how to better serve participants.
Data Collection
Questionnaire data were collected monthly (i.e., baseline, after 1 month of group, 2 months of group, and a final measure after the third month of group). Baseline questionnaires were collected before the first group when possible, or within 1 week of the first group. Follow-up questionnaires were collected by secure link texted to patients, with health coaches calling patients to fill them out verbally for patients who struggled with completing the forms themselves. There was no control group for this open evaluation.
Quantitative Data Analysis
Descriptive data were summarized with means and standard deviations, when continuous, and counts and percentages, when categorical. Longitudinal data analysis presents unique opportunities and challenges not found when analyzing cross-sectional data. Additional measurement points offer more nuanced data, allowing for the clear tracking of change over time; however, it also violates the assumptions of independence of errors, requiring specialized analyses.
Linear mixed models (LMM) were used to account for the longitudinal nature of the data as well as to make full use of all available data. This is a particularly strong advantage as listwise deletion of participants’ missing data not only dramatically reduces power, but also biases parameter estimates. 53 Intercepts for subjects were specified as random effects, allowing for the evaluation of the outcome of interest at each assessment point (e.g., depression at baseline, and 1, 2, and 3 months) with participants treated as independent. Time was treated as a fixed effect for each outcome variable of interest (i.e., diet, exercise, depression, anxiety, and loneliness).
While full-group outcomes are reported for completeness, mental health outcomes were also examined for a sub-group of patients with elevated levels of depression. Because participant diagnosis varied widely, many participants were not expected to show changes in depression (e.g., a participant with hypertension but non-depressed mood). The depressed subset included participants with a PHQ-9 score of 10 or higher at baseline, indicating clinically concerning levels. 47 This value was prespecified. Data were analyzed with R version 3.3, 54 and R Commander 55 version 2.3. Linear mixed models were estimated using the lme4 package 56 and P-values were estimated using the lmerTest package. 57 Alpha level was set at P < 0.05.
Qualitative Data Analysis
The qualitative analysis utilized reflexive thematic analysis (RTA)58,59 to identify common themes that emerged from this question within the survey data: What has been the biggest impact Open Source Wellness has had in your life? In particular, the research team was interested in identifying the factors that helped drive the quantitative improvement in health behaviors and mental well-being from the unique perspective of the participants. The team selected RTA because it offers a readily accessible and theoretically adaptable interpretative method for qualitative data analysis in which the process of coding and theme development is organic and flexible, evolving throughout the analytical process. 60 The reflexive nature of this process recognizes research subjectivity in the coding and theme development because the researchers are actively involved in the knowledge production. 59 Reflexive thematic analysis is frequently used within empirical health care research.61-64
The analysis began with the survey that participants completed following the first month of the program. From here, researchers S.D. and J.L. followed the Braun and Clark six-phase RTA process. 60 S.D. has a graduate certificate in qualitative research and inquiry methods, and S.D. trained J.L. in the Braun and Clark six-phase RTA process. In Phase 1, Data Familiarization, S.D. and J.L. independently performed “unmotivated looking,” 65 an inductive approach in which the analyst is open to the discovery of patterns or phenomena. In Phase 2, Initial Code Generation, S.D. and J.L. independently reviewed the survey data and assigned preliminary codes by labeling and organizing the data items into meaningful groups. S.D. and J.L. then compared codes, noting similarities and differences and discussing their rationale. Through an iterative process, they agreed upon a preliminary coding framework that included new or changed health behaviors and the participants’ perceived reasons for behavior change, including community support and increased self-worth. In Phase 3, Generating Initial Themes, S.D. and J.L. worked independently to identify common themes by sorting the data into preliminary categories, exploring the meaning and relationships between them, and writing detailed definitions for each theme. Then, through an iterative process that included agreement and disagreement, they refined these themes and the descriptions. In Phase 4, Theme Review, S.D. and J.L. reviewed the entire data set as a whole, applying the themes to ensure there was sufficient data to support a theme then collapsing and modifying themes as needed. In Phase 5, Theme Defining and Naming, S.D. and J.L. continued to cycle between the data and the identified themes; they then reviewed and refined them in collaboration with authors E.M. and B.E.A. to ensure a fit within the broader research. Collectively, the research team elected to focus on the themes related to community engagement and increased self-worth, because these provided the greatest insight about the “why” of behavior change, from the perspective of the participant. The research team acknowledged that the specific behavior changes were already reflected in the quantitative findings. In Phase 6, S.D. and J.L. incorporated the themes and supporting quotations into the qualitative findings. To ensure quality analysis consistent with the Braun & Clark six-phase RTA process, 60 S.D. and J.L. participated in collaborative coding, reflexive discussions, and multiple audits of the data set, all of which were documented in reflexive memos.
Reflexivity / Positionality
S.D. and J.L. approached the qualitative analysis through an interpretive framework, 66 acknowledging that their findings would be influenced by 2 perspectives: (1) the CAM participants’ viewpoint, shaped by their personal interpretations of the CAM experience; and (2) their own perspectives and biases as researchers. To mitigate the impact of personal biases, S.D. and J.L. actively practiced reflexivity through methods such as memoing and debriefing. They also identified instances that deviated from the anticipated themes to highlight discrepancies from their assumptions. 67
Results
Quantitative Results
Participants
The number of participants filling out each measure varied for 2 main reasons. Some measures were added and dropped over time (e.g., the GAD-7 was only given more recently at the community site), and sometimes participants skipped surveys or parts of surveys. Sample sizes for each measure are listed below. The full sample consisted of 720 participants, with 284 participants in the subsample with elevated levels of depression.
Racially and ethnically the sample was diverse: 18.9% African American, 3.7% Native American, 8.8% Asian, 52.5% Hispanic/Latino, 3.3% Pacific Islander, 16.4% non-Hispanic white, 16.3% “Other,” 15.2% prefer not to say. Percentages add up to more than 100% due to the ability to select multiple categories. Gender and age data were not collected. Reasons for participants not beginning or continuing the group included time conflicts with work or childcare, preferences for one-on-one coaching support, and inability to commit to weekly groups.
Full-Group Outcomes
Estimated Marginal Means.
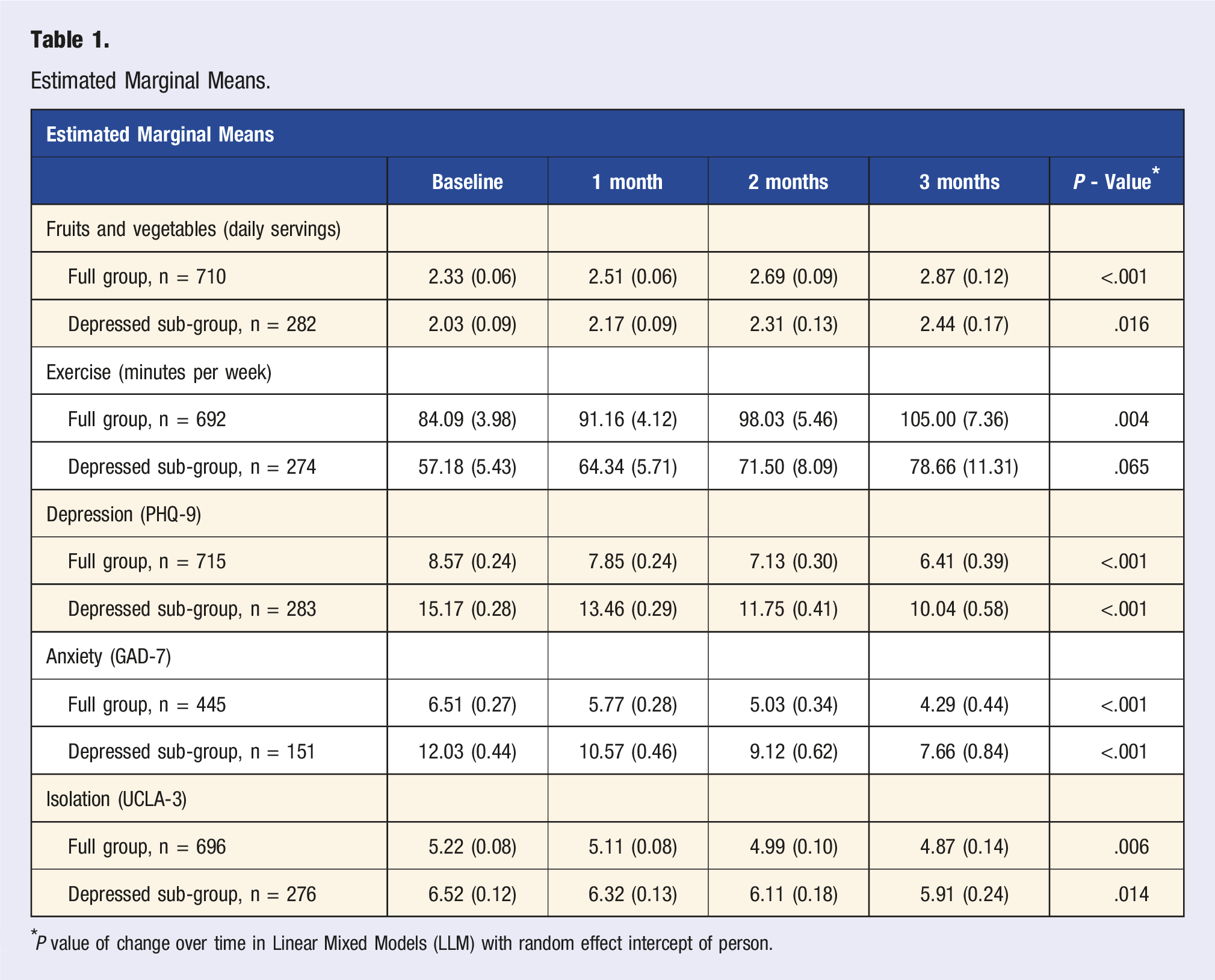
*P value of change over time in Linear Mixed Models (LLM) with random effect intercept of person.
Depressed Sub-group
When examining our depressed sub-group, participants showed a significant decrease in depression, b = −1.71, P < .001, n = 283, anxiety, b = −1.46, P < .001, n = 151, and isolation, b = −0.21, P = .014, n = 276.
Qualitative Results
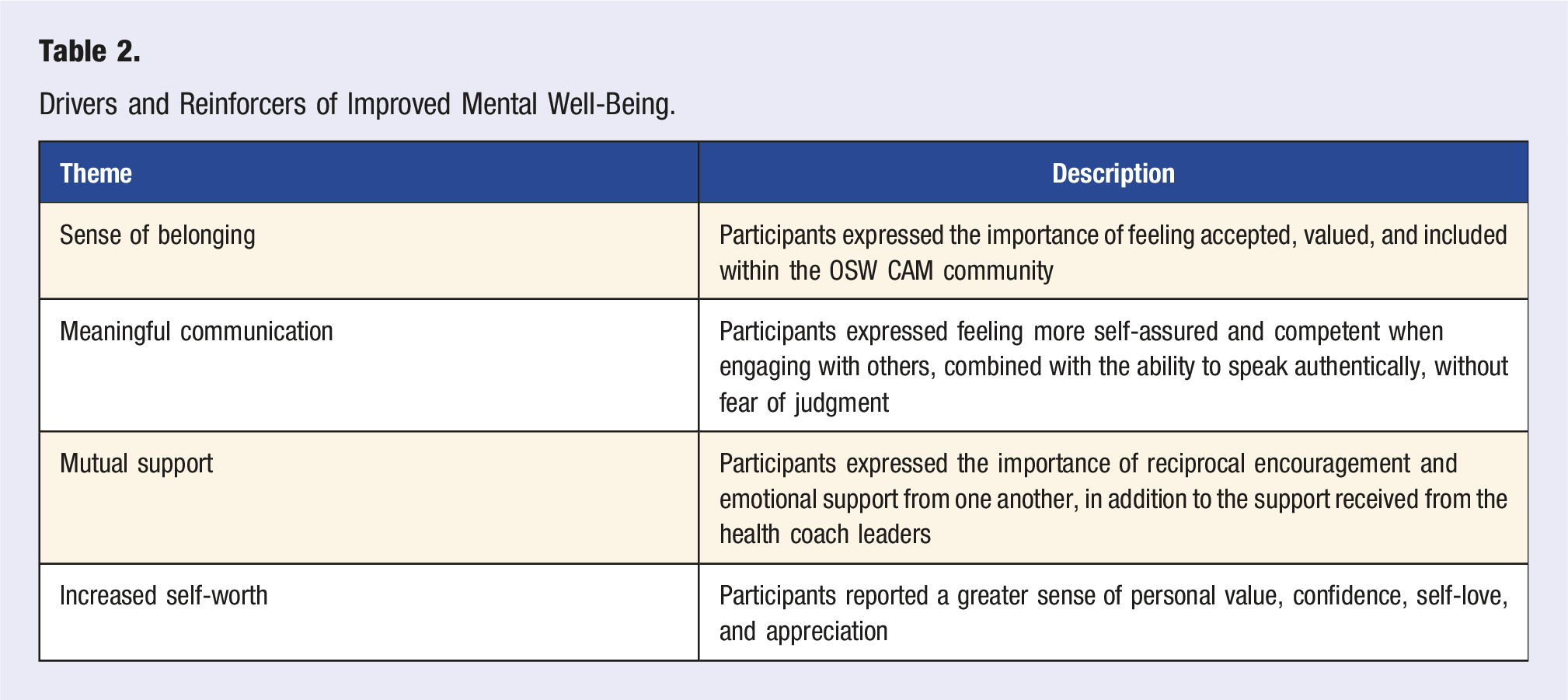
Drivers and Reinforcers of Improved Mental Well-Being.
Sense of Belonging
Looking at the CAM experience from the perspective of the participants, a sense of belonging emerged as the first key theme to drive and reinforce positive change. Participants wrote about the importance of being accepted and valued for who they were, and no longer feeling alone or abnormal. They also identified the significance of being part of a community of individuals who were facing the same struggles as they were. The following quotes were taken from verbatim participant comments. Some words were entered [in brackets] for clarity. “They make me feel welcome. Also they make me not to feel stupid or not normal.” “The group helped me to realize that I am normal.” “Feeling that I am not alone, and that it is hard sometimes to take care of yourself.” “Connection, knowing I can find friends and invest in myself.” “Seeing the different perspectives and lives of other people who want to better themselves in terms of health.”
Meaningful Communication
A second theme that emerged was meaningful communications, for example, the ability to share one’s true thoughts and feelings with honesty and vulnerability, and without fear of judgment. Participants described the positive impact of communicating their feelings in a safe environment and being able to express thoughts that they couldn’t share with others outside this community. “Helped me to understand my feelings and communicate them better. Gave me great tools like meditation and social skills to improve my mental [health] and sense of community.” “You [tell them] the stuff you don't tell your family for not making them worried, you can share your thoughts with the group (that is how much you get close and comfortable with them).” “Made me at ease to talk to people, trust them to share my thoughts and feelings, make me motivated to do something good, and try to find time for myself without the guilt.” “It made me so comfortable that I can openly talk about my feelings in front of everyone (for someone that was shy and not easy to talk with anyone).”
Mutual Support
A third theme related to positive change was support, specifically mutual support, which included both receiving and providing support. Participants noted the value of support from professionals (e.g., health coaches and nurses), but also expressed the role that other group members played and the desire to help them in return. “The biggest impact is [that] everyone in our group and other groups/coaches are giving us suggestions and support.” “Hearing the advice from the nurse and hearing from others.” “The ability to share and converse with other members both in our weekly meetings and privately by phone.” “The compassion and respect everyone shows for one another is amazing to witness. In turn, that has encouraged me to come out of my shell a bit more. I’m still kind of shy, but knowing everyone is SO NICE and understanding makes me feel so much more comfortable.” “Slowly get rid of my shyness [to] give me confidence to speak out in front of everyone in the group [and] try to answer questions or help out.”
Increased Self-Worth
A fourth theme that emerged was increased self-worth, described as a greater sense of value, confidence, and appreciation for oneself. Participants acknowledged learning self-love along with health behaviors, and having increased confidence to sustain positive change. “OSW has given me a whole new perspective on the Whole Me, and recognizing when and what to zero in on myself.” “They make [me] feel good about myself.” “Help me recognize my worth as a person!” “Reminded me of what I am capable of doing.” “OSW has helped me open up, taught me about self love, nutrition & meditation.” “I've learned about eating healthy, setting goals, meditation & self love.”
Discussion
This paper evaluated the effectiveness of CAM, a group-based, trauma-informed health coaching model, on patient-reported outcomes. Participants, low-income adults with chronic disease, significantly increased their fruit and vegetable consumption and weekly minutes of exercise, as well as significantly decreased their reported anxiety, depression, and loneliness symptoms. These mental health results were observed within the full population of participants, with larger improvements found within participants with elevated levels of depression at baseline. Similar results have been demonstrated in Group Medical Visits (GMVs) which improve patient health by combining clinical care from physicians with health education and peer support,68-70 as well as lifestyle medicine interventions led by specialists. 71 In contrast, our research focused on community-based health coaching utilizing group interventions and led by certified health coaches as opposed to medical professionals or specialists. There are fewer studies on community-based health coaching that meet this description, and none that we were able to find that incorporate this design and population. Community-based health coaching studies that were similar support our findings of increased physical activity,72-74 increased fruit and vegetable consumption, 74 and healthier eating habits. 73 Similar findings related to changes in mental health have been found in other community-based coaching programs, including reductions in perceived stress, anxiety, and depression.72,73 However, these community-based coaching studies were done with different populations, including adults aged 65 and older 72 and cancer survivors 73 and with small populations under 50 participants.74,75 Our study demonstrated statistically significant improvements in health behaviors and mental health within a large population (N = 720) of low-income adults with a wide-range of chronic health issues, overcoming substantial SDOH barriers to see significant improvements in health.
While other community-based health research studies provided quantitative data related to health behaviors and mental well-being, this paper examines the role of community-based, clinically integrated health coaching from the viewpoint of the participants themselves. These qualitative findings identified 4 key themes related to potential reasons for these improvements including: (1) Sense of Belonging: (2) Meaningful Communication; (3) Mutual Support; and (4) Increased Self-Worth. These interrelated and mutually reinforcing themes 75 are consistent with the social ecological model (SEM) which suggests that many factors, beyond personal characteristics or willpower, influence individuals’ behavior and health outcomes, including the dynamic interaction between peers and mentors; shared experiences as part of a community; and the larger social, cultural and environmental contexts, such as access to healthy food and safe recreation spaces. 31
These findings are supported by Berkman’s85 research on the role of social relations in health promotion, which describes the interrelatedness of belonging and self-esteem, noting that, to be effective, community-based social support “must provide both a sense of belonging and intimacy and must help people to be more competent and self-efficacious.”85(P.245) Participants also identified the importance of self-love, which has been linked to better functional health 76 and reduced depression, anxiety, and stress.77-79
Connected with a sense of belonging was a theme we identified as “meaningful communication”—the opportunity for participants to share their true thoughts and feelings with honesty and vulnerability and without fear of being judged. A qualitative study of participants with pre-existing mental health challenges found that sharing experiences with peers helped participants overcome social isolation and build trust, increasing their capacity to understand and self-manage their mental health issues. 80
While numerous studies have demonstrated the critical role that social support plays in promoting physical health and mental well-being,81-83 an interesting finding in our study was related to mutual support, specifically the value participants place on giving as well as receiving support. A small 2016 study by Inagaki and colleagues 84 found that giving support, not just receiving it, had positive effects on areas of the brain associated with stress and reward responses. Jiang et al 85 found that the willingness to give social support, not just receive it, improved 1 key measure of health, chronic inflammation, in a 2-year observational study of 1054 participants. While more studies are needed, emerging literature suggests that providing support is an often overlooked factor in how social support can benefit health. Overall, these findings indicate that the CAM program met significant psychosocial needs of participants, potentially impacting shared health determinants like attitudes and beliefs, subsequently improving health behaviors.6,9,11,76,77,86
Limitations and Strengths
This program evaluation has several limitations, primarily related to its design. It utilized a non-randomized, uncontrolled single-arm approach. The absence of a control group means that changes in participant health could be attributed to factors other than the intervention, such as external social support, cohort effects, etc. A second limitation is that the qualitative data were generated from a single survey question and researchers were not able to perform member-checking (e.g., verification with participants) to clarify responses. Because these data were collected as part of program evaluation rather than a formal, funded evaluation process, demographic data are limited. A final limitation is the unmeasured impact of the COVID global pandemic during the 2020-2023 time period when these data were collected. Further research, ideally a randomized design combined with semi-structured interviews, is necessary to identify other potential effects of the model, delve deeper into participants’ insights, and assess the ability to produce sustained changes after program completion. A strength of this program evaluation is its setting in an FQHC, a safety-net system serving primarily Medicaid patients and the uninsured, who often bear the heaviest disease burden and face numerous challenging social determinants of health. With minimal exclusion criteria, the study leans heavily towards the effectiveness side of the effectiveness/efficacy continuum, enhancing its external validity and generalizability. Further research is needed to incorporate multiple perspectives (patient, provider, and health care system) when evaluating how this multi-level intervention can broadly influence chronic disease care and potentially lead to improved outcomes. This includes examining the effects of the CAM model on time efficiency, productivity, billing, morale, and burnout among health care providers within FQHC systems.
Conclusions
This program evaluation of the Community as Medicine model contributes to the literature by demonstrating statistically significant improvements in health behaviors and mental well-being through a community-based health coaching model for diverse low-income populations. This model addresses both the physical and mental well-being of underserved populations who struggle with poverty, unsafe environments, and upstream drivers of chronic disease. Future research should be directed to incorporating this model into other community-based programs that serve this population and measuring its effectiveness both for patients and the providers.
Footnotes
Author Contributions
Conceptualization, B.E.A. and S.C.D.; methodology, B.E.A. and S.C.D.; validation, B.E.A. and E.A.M.; formal analysis, B.E.A., S.C.D., J.L..; writing—original draft preparation, S.C.D., B.E.A., and J.L; writing—review and editing, E.A.M.; supervision, B.E.A. All authors have read and agreed to the published version of the manuscript.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr Emmert-Aronson and Dr Markle are the co-founders of Open Source Wellness.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.