
Abstract
Lifestyle medicine (LM) has demonstrated clinical efficacy when utilized within chronic disease guidelines where lifestyle interventions are recommended. Integrating LM content into health professions education, such as doctor of occupational and physical therapy programs, is critically important to empower future clinicians to adequately implement therapeutic lifestyle interventions to improve their patient’s health outcomes. The American College of Lifestyle Medicine Partial Academic Pathway was developed to facilitate the integration of LM content into health professions programs. In this article, we describe the Partial Academic Pathway pilot, which began in the fall of 2022 and concluded in the fall of 2023. In addition, we describe the role of two health professions, occupational therapy and physical therapy, in health promotion and management of lifestyle-related conditions. Finally, we provide an example of how LM competencies were implemented into a doctor of physical therapy curriculum. As the students learning about LM enter the workforce, they have the potential to support their patients’ health through therapeutic lifestyle interventions while reducing healthcare costs and improving patient satisfaction.
Keywords
“Healthcare professionals are experts in restoration and rehabilitation which directly impacts patient’s plan of care.”
Introduction
Research related to the efficacy, safety, and cost-effectiveness of lifestyle medicine (LM) interventions has rapidly expanded over the past decade and has demonstrated enormous opportunities to improve health outcomes while saving healthcare expenditures for these conditions, including cardiovascular disease.1-7 The uptake of LM into health systems has also increased, with over one hundred health systems across the United States actively participating in the American College of Lifestyle Medicine (ACLM) Health Systems Council. 8 LM is a team-based approach, relying on the strengths of multiple disciplines to provide optimal care.
Occupational and physical therapists are impactful team members, utilizing their expertise to empower their patients to optimize their abilities. Currently occupational and physical therapists certified in LM have done so through education post-graduation and conference attendance. The challenge now is to move LM content and competencies into occupational and physical therapy academic programs. This paper will discuss early initiatives to support faculty with the implementation of LM competencies within health professions curricula. This article demonstrates the role of health professionals in the integration of LM in collaborative care. In addition, we aim to provide examples of future opportunities for inter-professional education.
Development of the Academic Pathway
Moving LM content into health professions programs required a multi-faceted approach. One of the first steps was identifying the competencies required for healthcare professionals to utilize LM within their practices. Understanding that there are nuances among all healthcare professions, general competencies were created by a global team of LM experts, which was published in 2022. 9 These competencies were the foundation of the buildout of an incentive program for universities to teach LM content mapped out to the competencies within a health professions course. A certification committee met monthly over the course of a year to determine the criteria for this program. This committee decided that courses that offered content that met at least 25% of the competencies (22 out of 88) through an application process would be designated ACLM Approved Partial Academic Pathway courses. Students who completed the course with a B- or above were offered the opportunity to apply to have one of two prerequisites toward certification eligibility in LM waived. ACLM’s Partial Academic Pathway program removed barriers of time, travel, and cost for an in-person conference while offering the students the opportunity to receive foundational knowledge in LM while still in school.
Faculty support is an ACLM priority. A full-time director was hired to lead the development of the program and meet with faculty to provide guidance. Several resources had been created that were made available to faculty teaching LM within university health professions programs. These included a syllabus and slide deck series, 10 a Taste of Lifestyle Medicine microgrant, 11 a culinary medicine handbook, 12 and a question bank. 13 Faculty were encouraged to utilize resources from the open-access site LMed, which includes slide decks, case studies, recorded webinars, and videos on various topics related to non-communicable chronic diseases and LM interventions. 14 Quarterly meetings were arranged for faculty to share information and resources. An online communication tool was also developed for faculty to have an opportunity to meet, share, and communicate asynchronously (Connect.lifestylemedicine.org). An introductory LM module was created and uploaded to Canvas Commons as an open-access resource. Faculty were encouraged to share their own LM modules to this site in an effort to create multiple faculty resources so those new to teaching LM have additional resources to use when building their own course.
Characteristics of the Programs Participating in the Partial Academic Pathway.
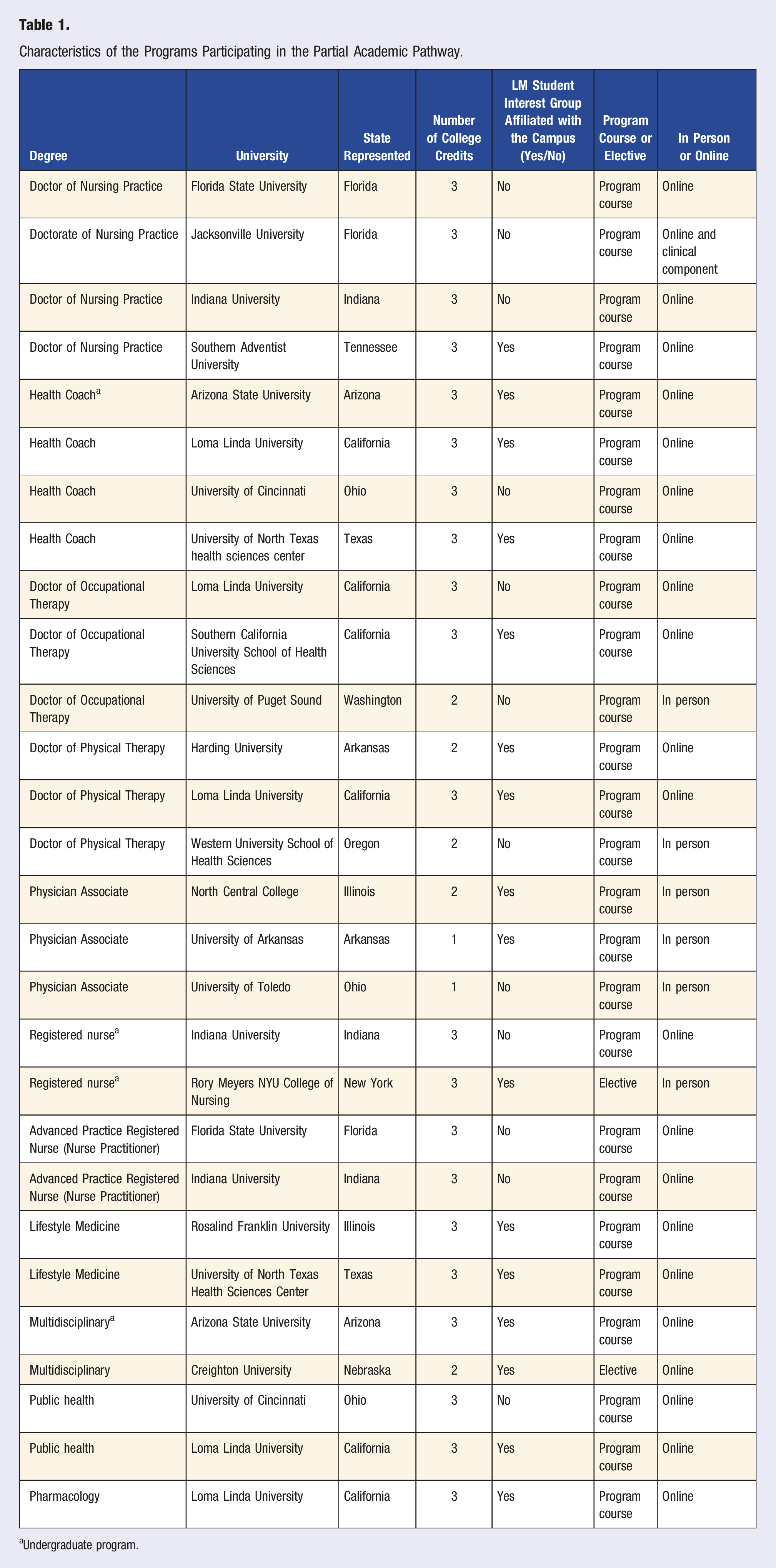
aUndergraduate program.
Health professions represented within the Partial Academic Pathway pilot included occupational therapy, physical therapy, public health, pharmacology, nursing (registered nurses, nurse practitioners, and doctor of nursing practice nurses), health coaching, and physician associates. Two graduate programs offered a specific LM degree. One graduate and one undergraduate program offered a multidisciplinary course as an elective. Most courses approved by ACLM were courses that were part of a university’s health professions program track, not electives. The numbers of programs by the health profession are presented in Figure 1. Courses that were electives tended to be ones offered to a large number of health professions students as opposed to a single health professions track. All but six of the courses were offered online. Three of the in-person courses were in physician associate programs, while one was in each a registered nursing, doctor of occupational therapy, and doctor of physical therapy program. One doctor of nursing practice program offered a course that was online but also had a clinical component. Number of partial academic pathway pilot programs by health profession.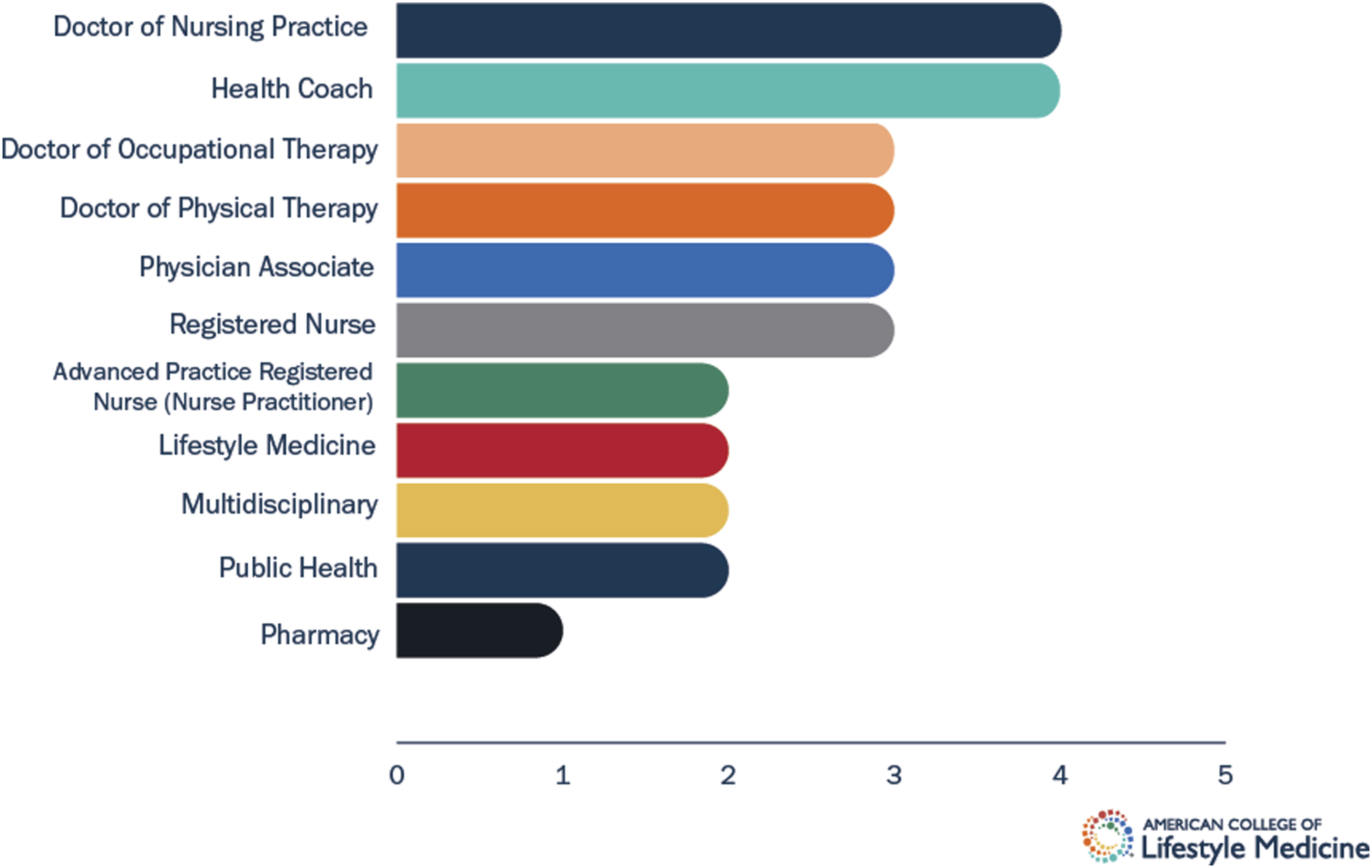
Lifestyle Medicine Competencies in the Curricula
Core competencies in LM were created both to communicate expectations of the LM clinician as well as to have an evidence-based foundation to build certification knowledge. 9 While the original core competencies in LM were developed for physicians,15,16 a global panel developed interdisciplinary core competencies that were published in 2022. 9 These competencies serve as the base for the Academic Pathway toward certification requirements. The competency domains in the 2022 Lifestyle Medicine Competencies include: Introduction to lifestyle medicine, Role of practitioner’s personal health and community advocacy, Nutrition science, assessment, and prescription, Physical activity science, assessment, and prescription, Sleep health science and interventions, Treating tobacco use disorder and managing other toxic exposures, Key clinical processes in lifestyle medicine, Fundamentals of health behavior change, Emotional and mental health assessment and interventions, and The role of connectedness and positive psychology.
On average, the programs in the Partial Academic Pathway included 44.21 out of the 88 LM competencies in their course. This number ranged from 22 to 76. The LM Core Competencies alongside number and percentage of programs utilizing the competencies can be found in Table 2. There were no competencies that were utilized within 100% of the Partial Academic Pathway programs. Seven competencies were represented in at least 80% of the courses, including: 1) Summarize the scientific evidence that shows health behaviors are associated with key health outcomes 2) Describe the evidence showing that lifestyle interventions effectively impact disease pathophysiology 3) Discuss the prevalence and associated cost burden of lifestyle-related disease, such as hyperlipidemia, cardiovascular disease, prediabetes, diabetes, hypertension, obesity, and cancer 4) Examine the evidence and pathophysiology between physical activity components and health outcomes 5) Describe the benefits of physical activity in preventing or treating disease in special populations, such as healthy older adults, pregnant women, children and adolescents, persons with obesity or disability, cardiovascular disease, diabetes, cancer, disability, and stroke 6) Apply the process of building effective and therapeutic alliances with patients that foster their personal growth 7) Explain how to collaborate with your patients to promote health behavior changes Number of Courses and the Proportion of all Courses in the Partial Academic Pathway Pilot Which Incorporate the Lifestyle Medicine Competency. Italicized Competencies May Not be Applicable to all Health Professions.

Competencies represented in less than 20% of the courses included: 1) Create and utilize data from office systems, such as electronic health records with lifestyle medicine guidance, in clinical decisions and care, including tracking screening frequency, test results, referrals, and recommended follow-up 2) Design a quality improvement project for lifestyle medicine clinical practice, using tools, such as Plan-Do-Study-Act (PDSA) cycles 3) Manage disruptions to the therapeutic alliance 4) Compare and contrast eudaimonia and hedonia, and explain their effect on physical health, including longevity
Occupational Therapy’s Role in Health Promotion and Management of Lifestyle-Related Conditions
Occupational therapy is defined as, “the therapeutic use of everyday occupations with persons, groups, or populations for the purpose of enhancing or enabling participation”; occupations refer to meaningful everyday activities that occupy one’s time. 17 Occupational therapy practitioners facilitate optimal health across the lifespan through looking at all aspects of one’s life, including habits, roles, routines, and rituals that impact the adoption and maintenance of healthy behaviors. 18 The American Occupational Therapy Association (AOTA) holds the position that occupational therapy practitioners are distinctly trained and qualified to address health promotion, including the primary and secondary impacts of chronic conditions across the lifespan. 19 The occupational therapy process begins with an evaluation, which includes a screening, an occupational profile, an analysis of functional performance, and an overall synthesis of the information obtained. 17
Specifically, occupational therapists use a client-centered approach to holistically evaluate a person’s mental and physical health, including their inextricably linked personal and environmental contexts. Following the evaluation components, if appropriate, occupational therapists develop client-centered goals and interventions to address impacted occupations. Interventions for managing chronic conditions can utilize a multi-component approach, incorporating education, goal setting, and problem-solving. These components can be delivered individually or in group settings, with a focus on fostering sustainable behavior change.
Additionally, occupational therapy practitioners are equipped to address complications secondary to primary chronic condition diagnoses, including psychosocial limitations, such as one’s ability to manage stress; physical limitations, such as sensation loss or low vision; impaired personal care occupations, such as bathing or dressing; and impacted instrumental activities of daily living (IADLs), such as meal preparation or home management related tasks.17,19-21
Integrating Lifestyle Medicine Competencies into Occupational Therapy Curricula
Currently, entry into the occupational therapy profession can occur four ways: Associate degree Level Occupational Therapy Assistant; Baccalaureate Degree Level Occupational Therapy Assistant; Masters (of Science) in Occupational Therapy (MOT or MSOT); and Entry-Level Occupational Therapy Doctorate (EL-OTD). The curriculum for these entry points is developed using designated Accreditation Council for Occupational Therapy Education (ACOTE) standards. 22 This section will focus specifically on the two graduate degree entry points, MSOT and EL-OTD.
There are specific ACOTE standards that address health promotion, lifestyle choices, and addressing chronic health conditions as foundational components of entry-to-practice education. Broadly, these specific standards reflect that entry-to-practice education should prepare students to analyze factors that contribute to health and the prevention of disease as well as demonstrate knowledge of the impact of social determinants of health for at risk populations; for EL-OTD educational programs, they must also ensure students ability to evaluate these factors along with scientific evidence reflecting the importance of lifestyle balance and health management. 22 Although occupational therapy practitioners are trained to address health promotion and management related to lifestyle-related chronic conditions, the mechanism of content delivery varies widely among occupational therapy educational programs.
At the time of publication, there are three EL-OTD programs approved through the ACLM Partial Academic Pathway, with several additional programs teaching LM content and in the process of pursuing this designation. On average, the currently approved OT educational programs have integrated just over 55% (49 out of 88) of the Lifestyle Medicine Core Competencies. 9 Across these three programs, there are 26 out of 88 competencies that all their courses address using a combination of methods, including assigned readings, lectures, class discussions, group projects, and exams. Two out of these three approved programs have integrated the ACLM Partial Academic Pathway as a part of their core curricula, and one program currently offers this opportunity as an elective.
Occupational therapy educational programs integrating LM competencies into their curricula in alignment with the profession’s accreditation standards illustrates a means to cohesively train students to address epidemiological trends using best health care practices.
The Role of Physical Therapists in the Prevention and Management of Lifestyle-Related Conditions
Physical therapists have a key role in the promotion of health and well-being. The American Physical Therapy Association advocates for the role physical therapists have in the prevention and management of disease and disability as well as in the promotion of health, wellness and fitness. 23 The Standards of Practice for Physical Therapy recognize that physical therapists provide interventions that optimize functional performance and promote a proactive and wellness-oriented lifestyle. 24 The Health-Focused Physical Therapy Model expands beyond the traditional biomedical approach of addressing pathologies and limitations in function. The Health-Focused Physical Therapy Model can be defined as physical therapy practice targeting patient’s overall health and well-being through health promotion and prevention of non-communicable disease. 25 In order to deliver health-focused care, physical therapists are urged to implement routine screening of lifestyle behaviors, such as sleep, diet and nutrition, stress management, substance use and physical activity.23,26-28
Physical therapists are front-line care providers in the prevention and treatment of many non-communicable diseases, such as type 2 diabetes mellitus. 29 It has been reported that up to 80% of patients referred to outpatient physical therapy have either type 2 diabetes, prediabetes or diabetes risk factors. 30 Usually, the referral to physical therapy is related to a musculoskeletal condition, such as pain or limited joint mobility, and not the diabetes diagnosis or risk factors. 30 However, while treating a musculoskeletal condition, it is important that physical therapists screen for diabetes and diabetes risk factors as these could impact the therapeutic exercise prescription. Patient education and exercise prescription are core interventions in physical therapy and provide an excellent opportunity for conversations about the six pillars of LM.
Case Example: Implementing Lifestyle Medicine Competencies in a Doctor of Physical Therapy Curriculum
The Western University of Health Sciences Department of Physical Therapy Education – Oregon was the first physical therapy program to take part in the ACLM Partial Academic Pathway. This process took less than a year from the inception to the first group of students submitting their documentation of course completion to ACLM. The steps of this process are presented in Figure 2. ACLM partial academic pathway Western University of Health Sciences doctor of physical therapy timeline.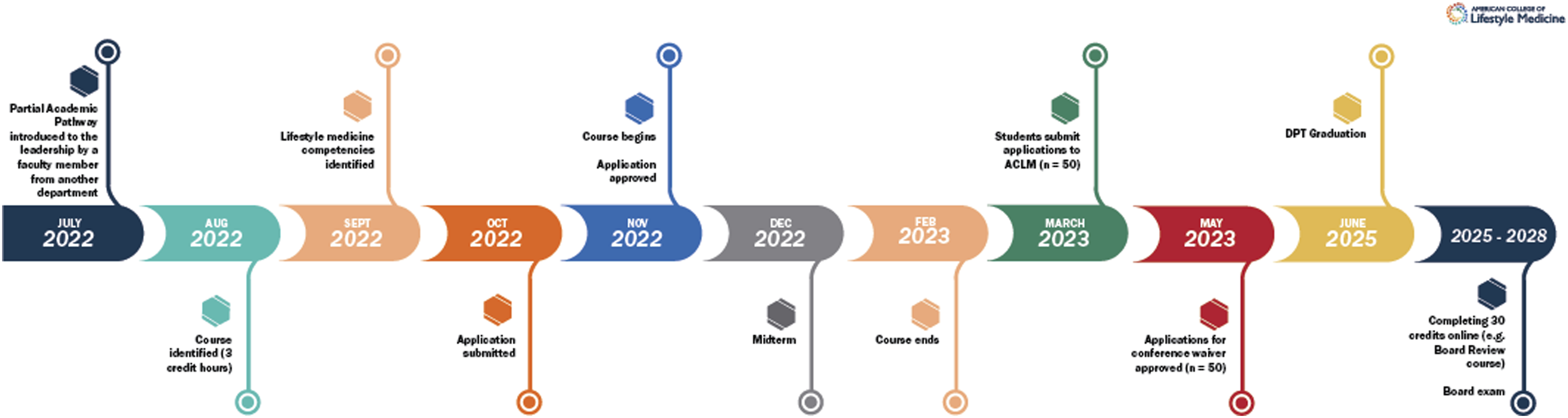
Course Content
A total of 32 out of the 88 Lifestyle Medicine Core Competencies 9 were covered in the first-year course in the Doctor of Physical Therapy program. This 2-credit hour course included at least one competency from each of the ten domains. The domain with most competencies covered was the “Physical Activity Science, Assessment, and Prescription” domain: all nine core competencies were covered. This is expected, considering that Doctor of Physical Therapy students are studying to be experts of human movement and exercise is one of the most common interventions utilized in physical therapy. However, it is important that physical therapists are familiar with all pillars of LM in order to support their patients in disease prevention, management and reversal. Therefore, all pillars of LM were introduced.
Future Implications
While the original LM competencies targeted physicians, the updated competencies fit the practice of many health professions. There are multiple opportunities to connect LM core competencies within a health professions curriculum that expands beyond what was discussed in this paper. While the end goal of LM interventions is improved patient outcomes, it also appears that healthcare clinicians who learn about lifestyle interventions utilize them in their own lives as well as with their patients. Inter-professional education may be a conduit to link this content with students of many health professions to allow them the opportunity to work together and learn about LM interventions. A culinary medicine experience, where health professions students are working together in a kitchen to make healthy meals, is one example. Another is a simulated patient experience where the patient has multiple chronic diseases, polypharmacy, poor lifestyle behaviors, alongside the opportunity to complete a thorough lifestyle assessment and apply therapeutic lifestyle interventions.
The ACLM Partial Academic Pathways provides a practical way to integrate LM competencies into health professions curricula. There has been rapid growth of the Academic Pathway program participation across disciplines, including occupational therapy and physical therapy graduate programs. As students enter the workforce, they will be equipped with knowledge, tools, and resources that can empower them to be the healthiest version of themselves while optimizing the health of their patients. While this paper describes a pilot program, future research could examine more closely the growth of lifestyle medicine content within health professions programs as more programs begin to implement the Partial Academic Pathways.
Conclusions
The integration of lifestyle medicine competencies into health professions programs through the ACLM Partial Academic Pathways helps support what students need to learn to address chronic disease through therapeutic lifestyle interventions. Better health outcomes can be achieved through consistently training providers to deliver lifestyle interventions. Healthcare professionals are experts in restoration and rehabilitation which directly impacts patient’s plan of care. This expertise can support patients in addressing lifestyle-related health issues and potentially reduce clinician burnout as well.
In this review, we have described some of the current education that allied health professionals are receiving in LM as well as provided examples of how occupational therapists and physical therapists can contribute to the prevention, management and reversal of lifestyle-related non-communicable disease as members of a multidisciplinary team. The implementation of LM core competencies in health professions curricula via the Academic Pathways program is essential in ensuring a consistent and evidence-based delivery of care. This approach has the power to optimize patient health through aligned therapeutic lifestyle interventions.
Footnotes
Acknowledgments
The authors would like to thank Kathy Pollard, MS, Research Projects Manager at American College of Lifestyle Medicine for citation support as well as Capt. Morgan Snyder, USAF Skillbridge intern and Ayesha Tyagi, for table and figure support. Additionally, Kelly Freeman would like to thank Ardmore Institute of Health for grant funding that helped to support the development and piloting of the Partial Academic Pathways.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: ZB and AR received no financial support for this article’s research, authorship, and publication. KF has received grant funding through the Ardmore Institute of Health.