
Abstract
We conducted a clinical trial on nature prescriptions measuring baseline moderate-to-vigorous physical activity (MVPA). 433 children between 6-16 years old completed baseline measures (49.2% female, 50.8% male). Participants self-identified as Latino (88.2%), African-American (9.7%), Asian (0.5%), and other or unknown (1.6%). The mean BMI% was 94.9 (SD 6.2), and mean age is 10.4 years (SD 2.7). The mean MVPA was 16.6 minutes, the mean daily accelerometer wear time was 728.8 minutes (SD 126.6), and the average number of days the participant wore the accelerometer for >8 hours (per day) was 6.8 (SD 3.8). Multivariate regression analysis showed that age was not associated with MVPA. However, boys engaged in 38 more minutes of MVPA per week than girls (P < .0001). Season was associated with MVPA with 5.4 more minutes of MVPA/day in the Fall (P < .01) and 4.8 more minutes in Spring (P < .01) as compared to winter and summer. Participant attitude toward nature was significantly associated with MVPA. One unit of positive increase in individual attitude toward nature was associated with 3 additional minutes of MVPA per day (β = 3.1, P < .001), or 21.7 minutes per week.
Keywords
“As children and adolescents fill their prescriptions, they are exposed to nature more and may develop more positive attitudes toward nature.”
Association Between Nature Attitudes and Physical Activity in Low-Income Youth
Background
For children and adolescents, the benefits of regular physical activity are numerous, and include improved cardiorespiratory fitness, strong bones and muscles, control of weight, and a decrease in anxiety and depression. These aforementioned benefits reduce the risk of developing heart disease, cancer, diabetes, and hypertension, osteoporosis, and obesity. 1 Even though the US Department of Health and Human Services recommends at least 60 minutes of moderate-to-vigorous physical activity per day, 2 76% of children ages 6-17 years do not meet this daily recommendation. 3 Furthermore, children from low-income families have fewer physical activity (PA) opportunities, 4 due to issues of neighborhood safety (levels of crime), including unsafe streets and limited access to safe playgrounds. 5 Children living in poverty are also more likely to suffer from poor health outcomes, such as low birth weight, infant mortality, delayed language development, chronic illness, environmental exposure, poor nutrition, and injury. 6 In addition to the chronic impact of poverty on childhood physical activity, the COVID-19 pandemic introduced an acute impact on PA by further reducing moderate-to-vigorous physical activity (MVPA), when compared to pre-pandemic levels. 7
Spending time outdoors in green space increases the likelihood of physical activity in children.8,9 The ratio between park space and residential area positively correlates with an increase in physical activity of young children. 10 The proximity of density of parks has been shown to increase non-school related physical activity in adolescent females. 11 Many parks include playgrounds, which serve as an important community resource by providing physical activity opportunities. A recent large playground study, comparing traditional vs innovative playgrounds (experimentation in play features and site elements), found that playgrounds with mature trees had twice as many users, and 19% more stay time than playgrounds without trees. 12 Parks, as public spaces, are particularly relevant to low-income and marginalized populations, as parks are often the only accessible areas with natural elements. Acknowledging the contextual settings of low-income children underscores the importance of safe and accessible public spaces and, more specifically the role of parks in promoting physical activity and ameliorating poor health outcomes.
One method of promoting physical activity that has been increasing in popularity is park or nature prescriptions.13,14 Typically, physicians or other health care professionals issue a prescription for the patient to spend time in a nature-rich environment, usually outdoors. 15 The nature prescription is often part of a larger treatment plan to improve 1 or more chronic medical conditions, decrease sedentary behavior, increase physical activity, and promote overall wellness. Nature prescriptions in the clinical setting are typically issued either to address ongoing problems such as overweight/obesity, dyslipidemia, pre-diabetes/diabetes, depression, anxiety, and attention deficit disorders, or as part of the anticipatory guidance for a wellness visit. Because these nature prescriptions are part of a larger treatment plan to address 1 or more medical problems, they are documented in the patient’s medical record, alongside other interventions like medications, diagnostic tests/screens, and referrals to specialists.
However, the perceived safety (with regard to crime) of a neighborhood or nearby outdoor space may impact one’s willingness to engage in physical activity, especially for children and youth living in low-income neighborhoods. The results of several studies on this topic are mixed. In 1 study of over 1000 male and female adults using a pedometer-controlled data protocol, adult women were less likely to walk at night when reporting feeling unsafe. 16 In another study of children and adolescents, no association was found between parental perception of neighborhood safety and MVPA. 17 Although not accelerometer-measured physical activity, a cross-sectional study showed that adolescents’ physical activity in parks and neighborhoods was inversely associated with perceived crime safety. 18
The theoretical framework we used for this study is Bronfenbrenner’s ecological systems theory, which consists of 5 environmental systems (microsystem, mesosystem, exosystem, macrosystem, and chronosystem) that co-interact and influence child development. Of these 5 systems, we examined the influence of the individual system and microsystem (child’s immediate environments) on physical activity, including age, gender, and individual attitudes toward nature, and perceived safety of a neighborhood. Given the paucity of published studies on park/nature for prescription programs, and even fewer studies examining the impact of individual attitudes toward nature and perception of safety on the effectiveness of the park/nature prescriptions, our results add to the growing body of literature to help us better understand the role of park/nature prescriptions as an intervention directed at increasing physical activity, and thus contributing to improved health outcomes. Also, considering the popularity of park/nature prescription programs, the disproportionate access to safe and nearby parks for low-income populations, 19 and the impact of poverty on child health outcomes, our study provides novel information to advance what is previously known regarding the relationship among physical activity, safety, and attitudes toward nature, in high-risk children and youth.
Methods
We are currently conducting a randomized controlled trial on nature prescriptions, 20 and this paper analyzes only baseline data. This study is a longitudinal, two-arm, randomized controlled trial, conducted at Unity Health Care, a federally qualified health center based in Washington, DC. Unity includes 9 separate community health centers, with the following demographics: 89.68% black, 24% Hispanic, 2.45% White, 0.84% Asian, 84.95% of patients with incomes below 200% of the federal poverty level, and 60.38% enrolled in Medicaid/CHIP. 21 While all participants were recruited from Unity, the majority were enrolled from the largest site, Upper Cardozo, which comprises the highest percentage of patients who are Hispanic and/or of immigrant parents. An additional 8 clinics also participated.
The intervention arm (250 participants) will be receiving routine medical attention, including a park prescription, at regular intervals (approximately every 3 months). The prescription will be co-produced, between the patient/family and provider. Providers are trained to ask questions regarding place, activity, frequency, and dose, and engage the patient/family in a brief conversation in order to maximize therapeutic potential and safety. Providers will issue park prescriptions, being mindful of accessibility and proximity. Nearby green space, identified by the patient/family, is preferred for practical reasons, given the potential barriers of time and the need for younger children to be chaperoned by an adult or older family member. Providers are trained to recommend 3-month follow-up between visits/prescriptions. All patients at Unity Health Care receive a reminder by text or email. Study research assistants also remind participants of their upcoming appointment and monitor any no–shows, in order to facilitate rescheduling missed appointments.
The control arm (250 participants) will be receiving only routine medical attention. Each enrolled participant completed baseline measurement before any intervention took place. Scheduled follow-up times will be at 3, 6, 12, and 24 months after the baseline.
An eligible individual had to meet all of the following criteria: (1) Informed assent and parental informed consent to participate in the study; (2) Stated willingness to comply with all study procedures and availability for the duration of the study; (3) Pediatric patients ages ≥6 and ≤16 years with 1 or more diagnoses of chronic conditions that usually require 2 or more routine health care provider visits per year; (4) One or more eligible diagnoses (ADHD, overweight or obesity, hypertriglyceridemia or hypercholesterolemia, pre-diabetes and Type 2 diabetes); (5) Having not already received a prior nature prescription; and (6) Likely to live in the Washington DC area in the next 2 years. Exclusion criteria included: (1) Individuals who have previously been given a park/nature prescription; (2) Activity restrictions that limit one’s ability to engage in intense physical activity; (3) Individuals with a sibling already enrolled.
Study participants were asked to complete survey items (without parental assistance) on their demographics, whether they lived with both parents or a guardian, on their attitudes toward nature (9 items),22–24 their perception of neighborhood safety, and their parent’s restriction on being allowed to go outdoors alone. The questions in the Appendix were on a 1-5 Likert scale (1-disagree a lot, 2-disagree a little, 3-neither agree or disagree, 4-agree a little, or 5-agree a lot) for each of the variables. Participants were also asked to wear an accelerometer for 7 days to measure their MVPA. For data analysis, we only used the days where participants wore the Actigraph GT3x for at least 3 days, 8 hours/day. Measures of BMI percentile were also abstracted from their electronic medical records.
Statistical Analysis
We first conducted exploratory data analysis at the participant level, including univariate descriptive statistics (mean and standard deviation or percentage) of all study variables and the correlation coefficient matrix among the 3 main study variables of interest. Next, we performed statistical modeling analysis on the participant-day level MVPA data. We applied linear mixed-effect model between the daily MPVA time outcome and the study variables adjusting for other participant level (e.g., gender, age, BMI percentile) and participant-day level covariates (e.g., season of accelerometer measurements, and daily total time of wearing accelerometer). A random effect was used to account for intra-participant correlation among repeated measures. Alternative modeling formulations (i.e., excluding insignificant covariates such as BMI percentiles, using 1 study variable at a time instead of all 3 in the same model) as sensitivity checks for the main model results were also performed.
Results
Univariate Descriptive Statistics of all Study Variables (n = 433).
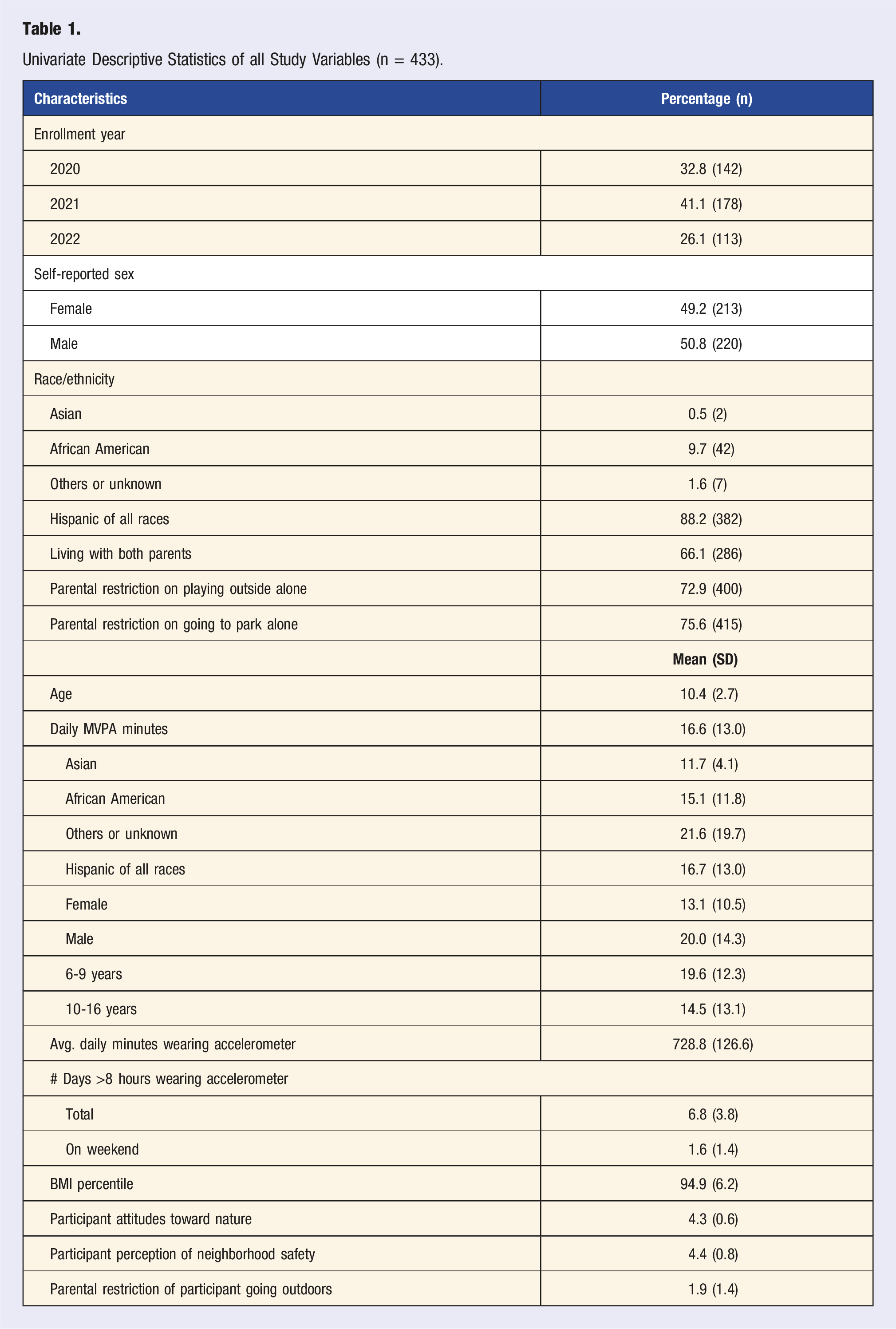
Participants reported an overall highly positive individual attitude toward being outside in nature and perceived their neighborhood as very safe. Based on a Likert scale of 1-5 (1 = least positive attitude toward being outside in nature and 5 = most positive), the mean for individual attitudes toward nature was 4.3 (SD = 0.6). Similarly, for participant perception of neighborhood safety, based on a Likert scale of 1-5 (1 = least safe to 5 = most safe) the mean rating of neighborhood safety was 4.4 (SD = 0.8). Most participants reported their parents did restrict them from going outdoors alone (1.9, SD = 1.4), with 72.9% of participants reported that their parents won’t let them play outside alone, and 75.6% of participants reported that their parents won’t let them go to a park alone. However, there was no significant correlation among these 3 variables. (Table 1)
Model Estimates (units of Minutes per Day) for the Daily MVPA Outcome (n = 433).
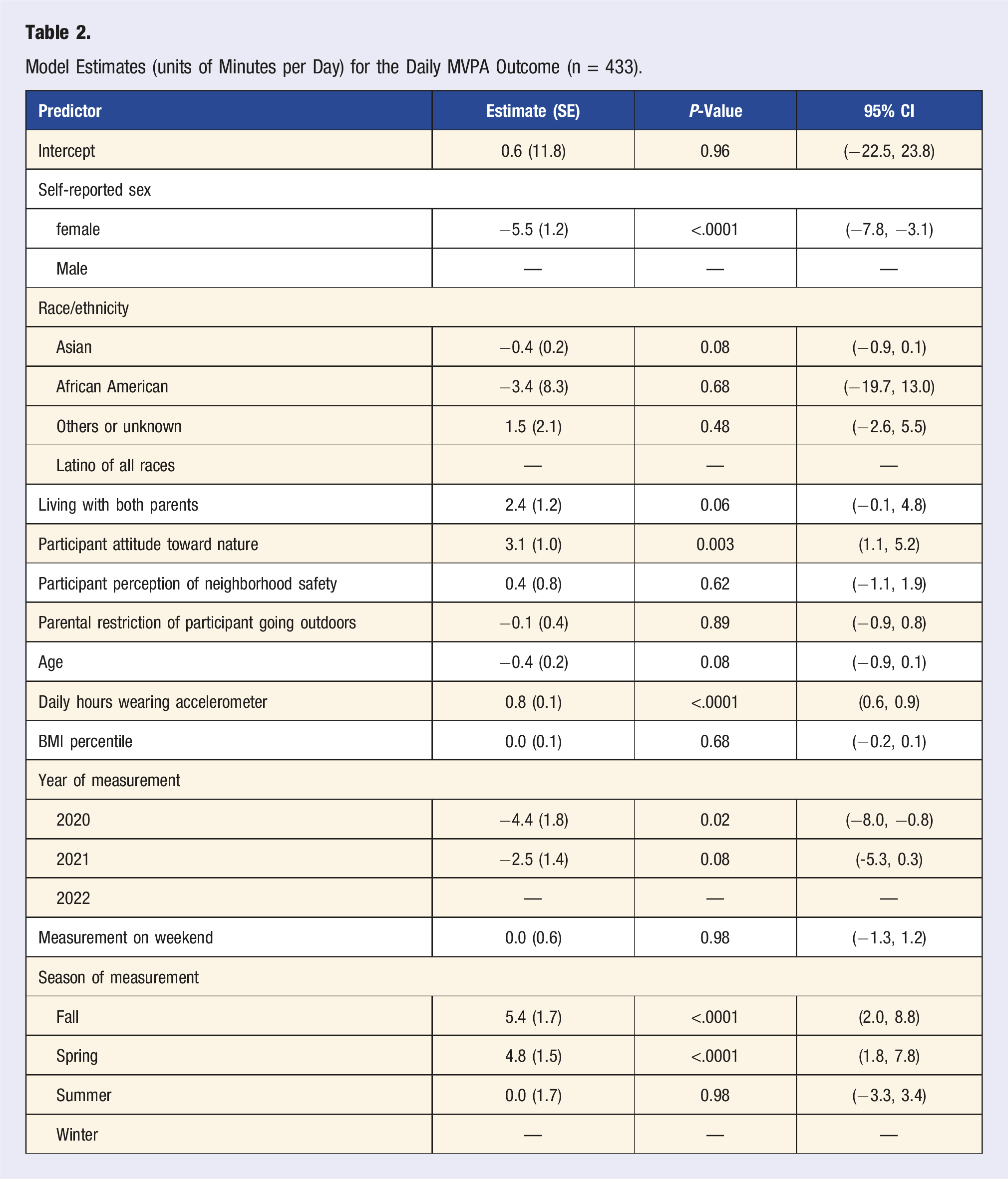
Of the 3 study variables (participant attitude toward nature, participant perception of neighborhood safety, parental restriction on child going outdoors alone), only participant attitude toward nature was significantly associated with MVPA. One unit increase in individual attitude toward nature was associated with 3 additional minutes of MVPA per day (β = 3.1, P < .001), or 21.7 minutes per week.
We also saw an association between the time wearing the accelerometer and total MVPA (Figure 1). Printed prescription from ParkRxAmerica.org.
Discussion
Of all of our baseline study results, the most notable is the participant’s attitude toward nature as a strong predictor of MVPA: three-minute per day increase in MVPA with every unit increase in positive attitude toward nature. Our findings are consistent with the results of another study of adults showing a positive correlation between connectedness to nature and physical activity. 26 Given the paucity of studies examining attitude toward nature or connectedness to nature with MVPA, especially in the context of park/nature prescriptions, our results make an important and unique contribution to this area of study.
Although the association between attitude toward nature and MVPA is statistically significant, it is important to note that this finding should not be interpreted to mean that a positive attitude toward nature causes an increase in MVPA. It is equally likely that increases in physical activity outdoors in nature-rich settings influence a young person’s positive attitudes toward nature. Further investigation through an experimental study design would be desirable to examine the possibility of causality between attitude toward nature and physical activity.
Overall, youth participants in our study perceived their neighborhood as relatively safe (paucity or absence of crime); however, our results did not show an association between participant’s perception of neighborhood safety and MVPA. Research on neighborhood safety and physical activity level has been mixed.17,27
A previous study on park use and neighborhood crime statistics, has shown that only murders and violent crime make a difference in park use rather than robberies or lower levels of crime. 28 As such, 1 limitation is that we did not ask more questions about neighborhood safety in the participant survey, and did not interview the parent on this issue of neighborhood safety, which would have provided a different point of view with which to compare to that of the participant.
With regard to child/adolescent independent mobility, most parents did restrict participants from going outdoors alone, with 72.9% of participants reported that their parents won’t let them play outside alone, and 75.6% of participants reported that their parents won’t let them go to a park alone. Although several other studies have previously shown a positive correlation between independent mobility and physical activity,29–31 our results did not show an association between participant’s report of their parental restriction of going outdoors and MVPA. The way we asked this question is itself a limitation, in that it did not ask the parent directly, but rather indirectly from the point of view of the participant. Although we do not know the reasons for this parental restriction on child/adolescent independent mobility, we posit that it could be related to the children’s age and issues like traffic and possibly distance to park settings, rather than fear of violence or crime.
It is important to point out that the commencement of our study coincided with the advent of the COVID-19 pandemic, followed by civil unrest and an insurrection in our nation’s capital, all of which resulted in decreased access to public space and an increase in police presence. Our study participant recruitment effort began in March 2020, and continued through the end of May 2022. Given the demographic context of our participants (low-income, largely immigrant, black, indigenous, people of color), and the overlapping in time and place between our study recruitment and these major events in the national capital region, it is reasonable to consider how these events may have influenced participant perception of neighborhood safety (low crime) and parental restriction on independent mobility of their child/adolescent.
The decline in MVPA during childhood and adolescence has been well documented, and is more prominent in girls than boys. 32 Our baseline data analysis is consistent with previous literature in that being female was associated with a lower level of MVPA in comparison to boys (β = −5.5, P < .0001). This equates to more than 38 minutes per week difference between genders. Given that 88.2% of our participants identified as Latino, and recognizing the paucity of data regarding gender differences in Latino childhood and adolescent MVPA, 33 our results further the evidence for this gender difference, specifically among Latino youth. These gender differences persist despite policy and advocacy efforts to narrow the gap, which underscores the importance of ongoing efforts to address this physical activity gender disparity.
Season was also associated with MVPA with considerably higher levels of MVPA in the Fall (β = 5.4, P < .01) and Spring (β = 4.8, P < .01) as compared to winter and summer. On a weekly basis that translates to 37.8 more minutes per week in fall and 33.6 more minutes per week in the Spring. Within Unity Health Care, the majority of our participants were recruited from Upper Cardozo Community Health Center, which provides health care to a large immigrant population, whose geographic area of origin is predominantly Mexico, Central America, and the Caribbean. When compared to the more tropical climate of these aforementioned regions, the climate of the National Capital Region experiences a greater variation in temperature between summer and winter. The more moderate temperatures in the National Capital Region coincide with spring and fall, the 2 seasons where we observed a significant increase MVPA. Future research on the impact of climate change (extreme weather and temperature) on the seasonal differences in physical activity in youth may help to inform future interventions and programming to increase physical activity outdoors.
In conclusion, we analyzed baseline data, within a larger randomized trial on the effectiveness of park/nature prescriptions, to explore potential predictors (i.e., participant attitude toward nature, participant perception of neighborhood safety, parental restriction of independent mobility) of MVPA, and to report on age, gender, and seasonality differences on MVPA. With regard to individual factors, it is possible that children and adolescents who have more positive attitudes toward nature would benefit more from a park/nature prescription because they already enjoy going outside and are more likely to fill a prescription. Alternatively, as children and adolescents fill their prescriptions, they are exposed to nature more and may develop more positive attitudes toward nature. Given the diversity of clinical settings and patient populations where park/nature prescriptions are issued, the gaining popularity of this kind of social prescription, and the paucity of studies examining the effectiveness of park/nature prescriptions, further research on the roles of these individual factors may help us to understand how best to optimize the effectiveness of park/nature prescriptions.
Footnotes
Acknowledgments
Claudia Amaya, research assistant. Jeimy Castillo, research assistant. Mari Crespo, research assistant. Andrea Rendon, research assistant. Allison C Voorhees, research associate. Kayode Abrahms, driver to drop off and pick up accelerometers. Haoyuan Zhong, data manager
Author Contributions
Robert Zarr, MD, MPH, Wing Yi Chan, PhD Deborah Cohen, MD MPH conceptualized the study, coordinated and supervised the data collection, drafted the initial manuscript, and approved the final manuscript as submitted. Erika L. Estrada, MPP, developed and maintained data collection systems, prepared data for analysis. Haoyuan Zhong and Bing Han performed the statistical analysis, interpreted the results, and contributed to writing the first draft. All authors approved the final manuscript as submitted and agree to be accountable for all aspects of the work.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Institutes of Health National Heart Lung and Blood Institute.
Clinical Trial Registry Name and Registration Number
Park Rx and Physical Activity Among Low-income Children (ParkRx), NCT04114734. Registered on October 3, 2019.
Appendix
Questions regarding participant attitude toward nature.
1. I think that spending time in nature is a waste of time. 2. There is nothing fun or entertaining for me to do outside. 3. I prefer staying inside to going outdoors. 4. I enjoy being outside in nature. 5. My favorite places are outside in nature. 6. I know a place in my neighborhood where I can go to play outside in nature. 7. I need time in nature to be happy. 8. Sometimes when I am unhappy, I find comfort in nature. 9. Being out in nature is a great stress reducer for me.
Questions regarding participant perception of neighborhood safety
1. It is safe to walk or jog in my neighborhood. 2. There is a lot of crime in my neighborhood. 3. The parks that are nearby are safe to play in.
Questions regarding parental restriction of participant going outdoors
1. My parent(s) won’t let me play outside alone. 2. My parent(s) won’t let me go to the park alone.