
Abstract
Acute exercise is linked to memory improvement. Several mediators may influence the effect of exercise such as the type of exercise (aerobic exercise, muscle stretching).
Keywords
“Individuals who were presented with a positive or negative expectation message showed cognitive measures consistent with those messages.”
Introduction
Emerging evidence suggests that a single session of aerobic exercise performed prior to a cognitive assessment improves test performance. For example, among healthy adults, 20 min of moderate-intensity aerobic exercise performed in proximity (before or after exercise) has been shown to improve memory and processing speed compared to rest.1-3 The ability of acute exercise to stimulate immediate improvement in cognitive function is termed “exercise priming.”3-5 In terms of practical implications, an aerobic exercise bout performed prior to psychotherapy (e.g., behavioral or cognitive) may improve retention of skills taught during the therapy session. 6
The mechanisms that explain exercise priming are complex and may be due to increased cerebral blood flow (CBF), the induction of brain-derived neurotrophic factor (BDNF), as well as neural endocrine responses during and post-exercise. 3 CBF has been shown to rise with increased exercise intensity up to 60% and then decreases towards baseline at higher exercise levels. 7 Further, among healthy adults, CBF was shown to be 20% higher (vs resting state) 30 min after completion of a 30-min bout of moderate-intensity aerobic exercise. 8 Therefore, performing a cognitive task within this timeline may take advantage of heightened cerebral activity. For example, 30 min of moderate-intensity exercise increased CBF, which aligned with post-exercise improvement in executive functioning. 9 Acute exercise induction of BDNF has also been linked to cognitive function. 20 min of treadmill running increased circulating levels of BDNF and was associated with improved scores on the Trail-Making Test (measure of processing speed). 10 It’s estimated that 70-80% of circulating BDNF in response to acute exercise is released from the brain via crossing the blood-brain-barrier. 11 The neuroendocrine mediators of post-exercise cognitive improvements have included catecholamines such as norepinephrine and dopamine and has been termed the “catecholamine hypothesis.” 12 Acute exercise release of norepinephrine was responsible for BDNF induction in the prefrontal cortex region. Numerous animal studies have reported a post-exercise dopamine increase in various brain regions (e.g., hippocampus, PFC, midbrain).13-15 Further, circulating dopamine levels in response to 6 min of intense treadmill running was associated with immediate post-exercise learning. 16 Dopamine plays an important role in mood regulation, and therefore, the effect of exercise on mood (via dopamine release) may help to explain the cognitive benefits of acute exercise. 1 Supporting evidence among young adult males suggested a trend in the relationship between mood and memory improvements after acute exercise (P = .06). 16 However, limited data exists on the role of mood in explaining the cognitive benefits of acute exercise.
Another important mediator of acute exercise-related cognitive changes is the expectation effect of the intervention. Evidence suggests that positive expectation can have a large impact on cognitive gains. 17 Only 1 known study evaluated expectation, and the researchers reported an exercise intervention to have the highest level of expectation for memory improvements compared to other interventions (puzzles, videos, and reading). 18 Therefore, the role of expectation on cognitive outcomes after acute exercise needs further exploration.
Aerobic exercise is often used in studies to induce the exercise priming mechanisms. 5 The cardiorespiratory component may be more suitable for promoting the various mechanisms previously discussed (i.e., CBF, BDNF, and neuroendocrine factors). However, it has been reported that acute muscle activation performed as muscle stretching (no cardiorespiratory upregulation) improved cognitive performance and mood state compared to a sedentary control. 19 Further, short-term memory was not different between a single session of high intensity aerobic interval exercise compared to muscle stretching. 20 The lack of difference may be due to the intensity of the aerobic exercise intervention. However, further work is needed to understand whether an aerobic component is important for improving cognitive functioning.
Therefore, the purpose of this study was to compare changes in memory after completion of either moderate-intensity aerobic exercise or muscle stretching. Additional aim was to evaluate the role of mood and expectation on the exercise-induced changes in cognitive function.
Material and Methods
Participants
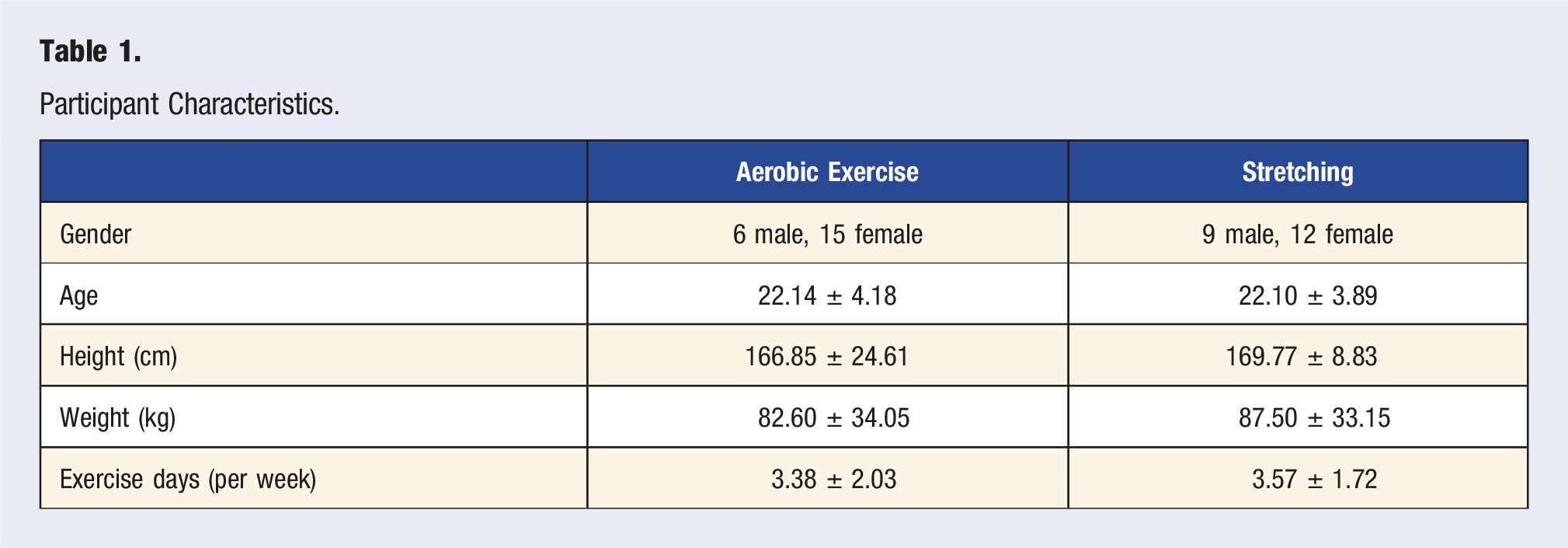
Forty-two young adults (18 to 35 years old) were recruited for this study. Individuals were excluded if they had been diagnosed with cardiovascular, metabolic, renal, pulmonary, bone, or neuromuscular diseases; and women who were currently pregnant or trying to become pregnant. Individuals were recruited from a university setting using flyers and an online sign-up system. All participants provided written informed consent for inclusion prior to participating in the study, and no form of compensation was provided. This study was conducted in accordance with the Declaration of Helsinki, and the protocol was approved by the Ethics Committee of Central Michigan University (protocol # 2021-1624).
Study Design
This study was conducted using a two-group randomized controlled trial comparing 20 min of aerobic exercise (AE) vs 20 min of stretching exercise (SE). The stretching control was used to understand whether muscle contraction/stretch or cardiovascular activation was required for cognitive improvements. Upon arrival, participants were randomized to perform either AE or SE. Upon completion of the intervention (both AE and SE), participants rested for 15 min to allow heart rate to return to baseline, which was followed by the memory assessment and digit span, and lastly rating scales about their mood and expectation. To eliminate experimenter expectation bias, the administration of the tasks, including the consent form, was standardized by pre-recording the instructions.
Moderate-Intensity Aerobic Exercise (AE) Protocol
For this exercise, a three-minute warm-up was followed by 20 min of treadmill exercise. Participants were expected to work at a moderate intensity. The rating of perceived exertion (RPE) scale (6-20 scale with 6 = no exertion and 20 = maximal exertion) was used to monitor intensity with a target value of 12 (i.e., moderate intensity). The treadmill speed and grade gradually increased until the participant reached the moderate-intensity criteria. Participant heart rate and RPE were monitored throughout, and speed and grade were adjusted as needed.
Stretching Exercise (SE) Protocol (Control)
For this exercise, a video recording of a model performing the routine was used to guide the participant. A 20 min full-body, unassisted static stretching routine was performed. 3 upper-body and 3 lower-body stretching exercise were completed. The upper-body stretching techniques consisted of a shoulder stretch, chest stretches, and trunk rotation. The lower-body stretching techniques consisted of the hip stretch, lunge stretch, and hamstring stretch. Each stretching modality were performed on each side of the body 3 times for 30 s each before moving on to the next stretching modality. The participants rested for 10 s between each set and before switching to the next stretching routine.
Digit Span
Participants rested for 15 min after either AE or SE before beginning the memory assessment. They sat quietly in a windowless room with no access to electronic devices (i.e., cell phone) and no social communication. The forward and backward digit span (DS) memory test was administered via a voice recording on an iPad device. DS is a widely used measure of short-term verbal memory. 21 The forward span asked the participant to repeat the order of numbers read aloud in the exact order beginning with a digit sequence of 2. The backward span required the numbers to recalled in reverse order. Two consecutive trials were administered for each span, and incorrect responses on both trials terminated the test. The maximal number of spans was 8 and scoring was based on the number of completed trials across spans. That is, if 1 successfully completes 2 trials for span 2 and 3 but only 1 trial for span 4, the score is 5. Highest score that could be achieved for both forward and backward DS was 16 (8 spans × 2 trials).
Rey’s Auditory Verbal Learning Task (RAVLT)
After the Digit Span, the RAVLT was administered, which consisted of reading aloud (via an iPad recording), a list of 15 words (List A) across 5 consecutive trials. The participant was asked to recall as many as words as possible in any order. The procedure was repeated for 5 consecutive trials (Trials 1 to 5). Next, a new list of 15 words (Trial 6) was read to the participant (called List B) and immediately recalled. The examiner then asked participant to recall words (Trial 7) from the first list again (List A). After a 10-min delay in which the participant sat quietly in a room (no cell phone or external influences), the participant was asked to recall the words from list A (the first list, termed delayed recall). Lastly, a recognition test was administered where words from lists A and B were read in addition to several phonemically words. The participant was asked to state whether or not each word appeared on list A. 6 outcomes were assessed from the trials: (1) RAVLT immediate learning (sum of scores of Trials 1-5); (2) RAVLT learning (Trial 5 minus Trial 1); (3) RAVLT forgetting (score of Trial 5 minus delayed recall); (4) RAVLT percent forgetting (RAVLT forgetting divided by Trial 5 score); (5) delayed recall; and (6) recognition. 22
Mood and Expectation Ratings
A questionnaire was administered after the memory test that asked about mood state and whether the individual expected AE or SE would improve memory. The expectation question asked, Do you agree with the following statement? “Performing exercise improved my memory?” The mood question asked the participant to, Please rate your current mood. A 5-point Likert scale was used to assess the results.
Statistical Analysis
A priori analysis was used to determine sample size with power set to .80 and alpha level of .05 for memory outcome variables. Criteria for selected studies were acute exercise and cognitive changes.2,23 Estimated effect size for memory outcomes after a single session of acute exercise ranged .18 – .27 (Cohen’s d), which estimated a sample size of 20-44 total participants. The data were analyzed using the Statistical Package for Social Sciences software program (SPSS, version 18.2.1; Chicago, IL, USA). Descriptive statistics are presented as Mean ± Standard Deviation, and a P-value of <.05 indicated statistical significance. A two-way mixed-design analysis of variance (ANOVA) was used to evaluated recalled words across the first 5 RAVLT trials (2 groups × 5 repeated trials). Independent sample t-tests were used to analyze the differences between groups for RAVLT outcomes (immediate learning, learning, forgetting, percent forgetting, delayed recall, and recognition), memory span, along with mood and expectation. Expectation and mood were analyzed as confounding variables using one-way analysis of covariance (ANCOVA). The ANCOVA was used to analyze the covariates for all RAVLT outcomes. Pearson’s correlation coefficient was used to understand the association between the cardiovascular response (i.e., heart rate) and RAVLT outcomes within each group (AE and SE). Heart rate values were analyzed at 10-, 15-, and 20-min timepoints during either AE or SE. This was done to understand the relationships between various exercise timepoints and memory outcomes. This study’s design and analyses were not pre-registered.
Results
Participants
Participant Characteristics.
RAVLT Outcomes
A main effect of group was statistically significant, F (1, 40) = 4.85, P = .03, ηp2 = .11. A main effect of trial was also significant, F (4, 160) = 159.13, P < .0001, ηp2 = .80. The group × trials interaction was not significant, F (4, 160) = 1.06, P = .37, ηp2 = .03. The main effect of group indicated that recall was higher for AE (10.79 ± 1.69) vs SE (9.66 ± 1.64). The main effect of trials indicated that recall became higher as the trial progressed (Trial 1: 6.07 ± 2.03, Trial 2: 9.38 ± 2.22, Trial 3: 10.98 ± 2.38, Trial 4: 11.93 ± 2.09, and Trial 5: 12.76 ± 1.87), with least significance tests showing that every mean was significantly different from every other mean, P < .05. See Figue 1. Mean RAVLT scores (out of 15 words) during the first 5 trials for aerobic exercise and stretching exercise. RAVLT, Rey auditory verbal learning test.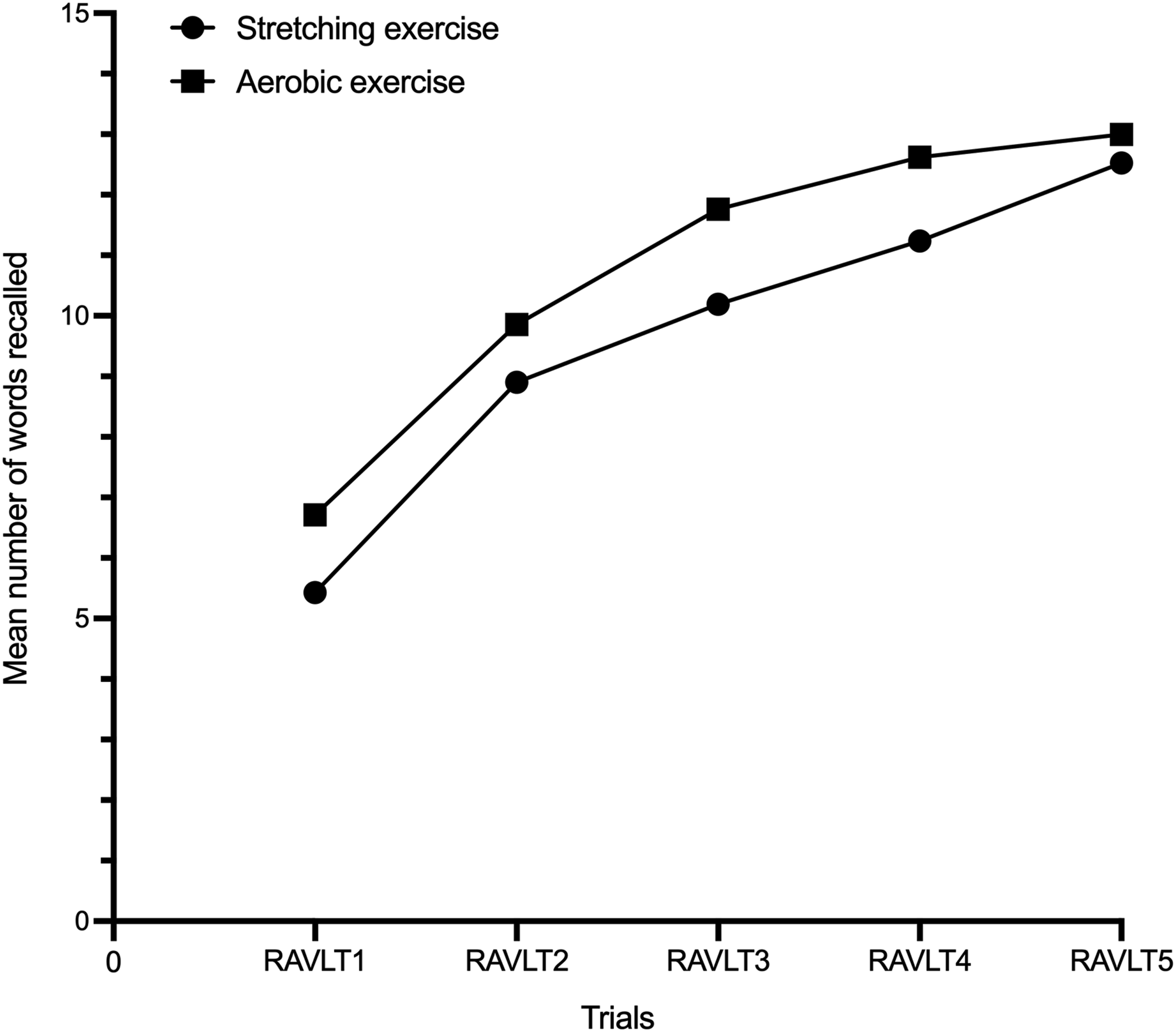
Comparison of Outcomes Between Interventions.
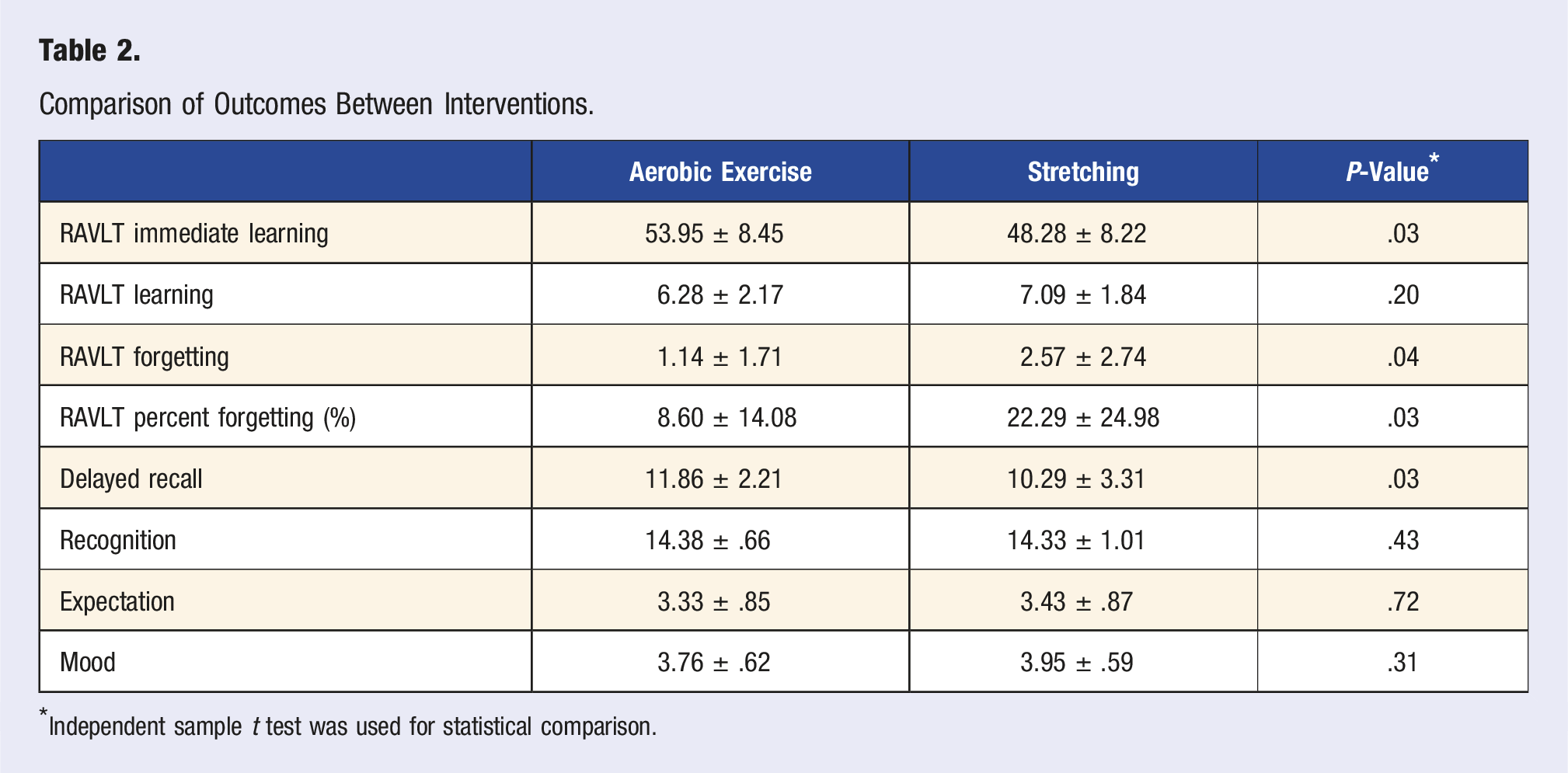
*Independent sample t test was used for statistical comparison.
Memory Span Outcomes
Forward span did not show a difference between AE (10.00 ± 2.10) and SE (10.38 ± 1.71), t (39) = .64, P = .40, Cohen’s d = 1.64. Likewise, backward span did not show a difference between AE (7.14 ± 2.41) and SE (6.90 ± 1.84), t (40) = .36, P = .13, Cohen’s d = 2.15.
Expectation and Mood Relationship With RAVLT Outcomes
No differences were detected between AE and SE for both expectation and mood (Table 2). Expectation did not significantly influence the group differences for RAVLT immediate learning (F (1, 39) = 2.85, P = .09), RAVLT learning (F (1, 39) = 1.61, P = .21), RAVLT forgetting (F (1, 39) = .09, P = .76), and RAVLT percent forgetting (F (1, 39) = .31, P = .57). Similarly, mood did not significantly influence changes in RAVLT immediate learning (F (1, 39) = .81, P = .37), RAVLT learning (F (1, 39) = .495, P = .48), RAVLT forgetting (F (1, 39) = .28, P = .59) and RAVLT percent forgetting (F (1, 39) = .006, P = .93).
The Relationship Between Cardiovascular Response and Memory
Physiological Response to Interventions.
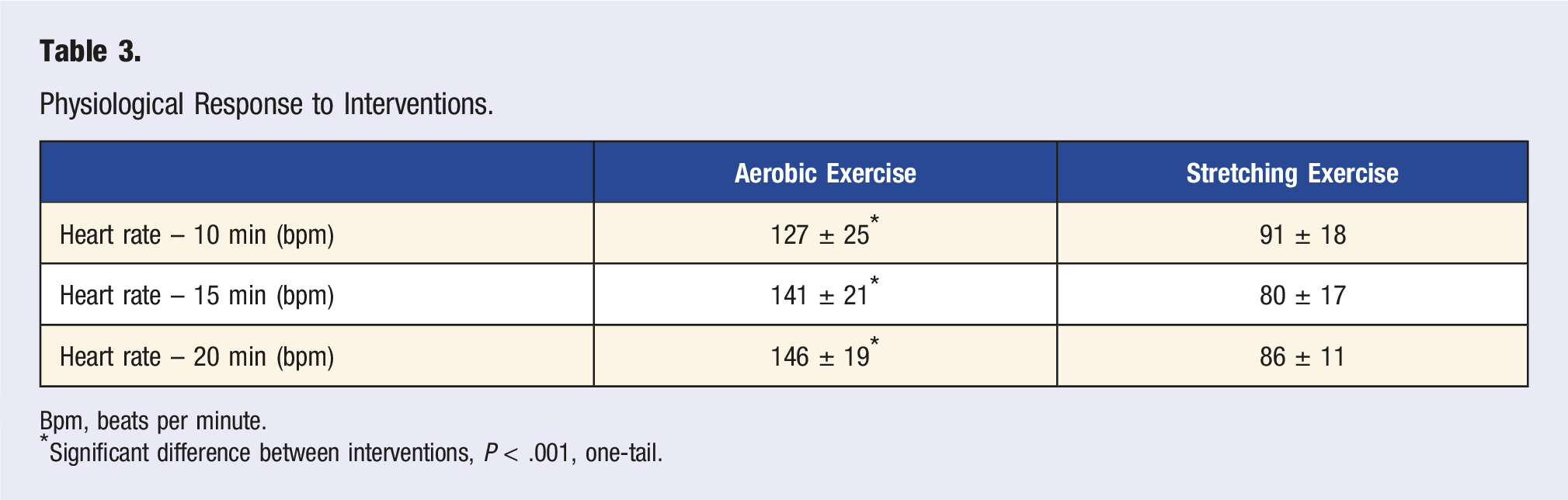
Bpm, beats per minute.
*Significant difference between interventions, P < .001, one-tail.
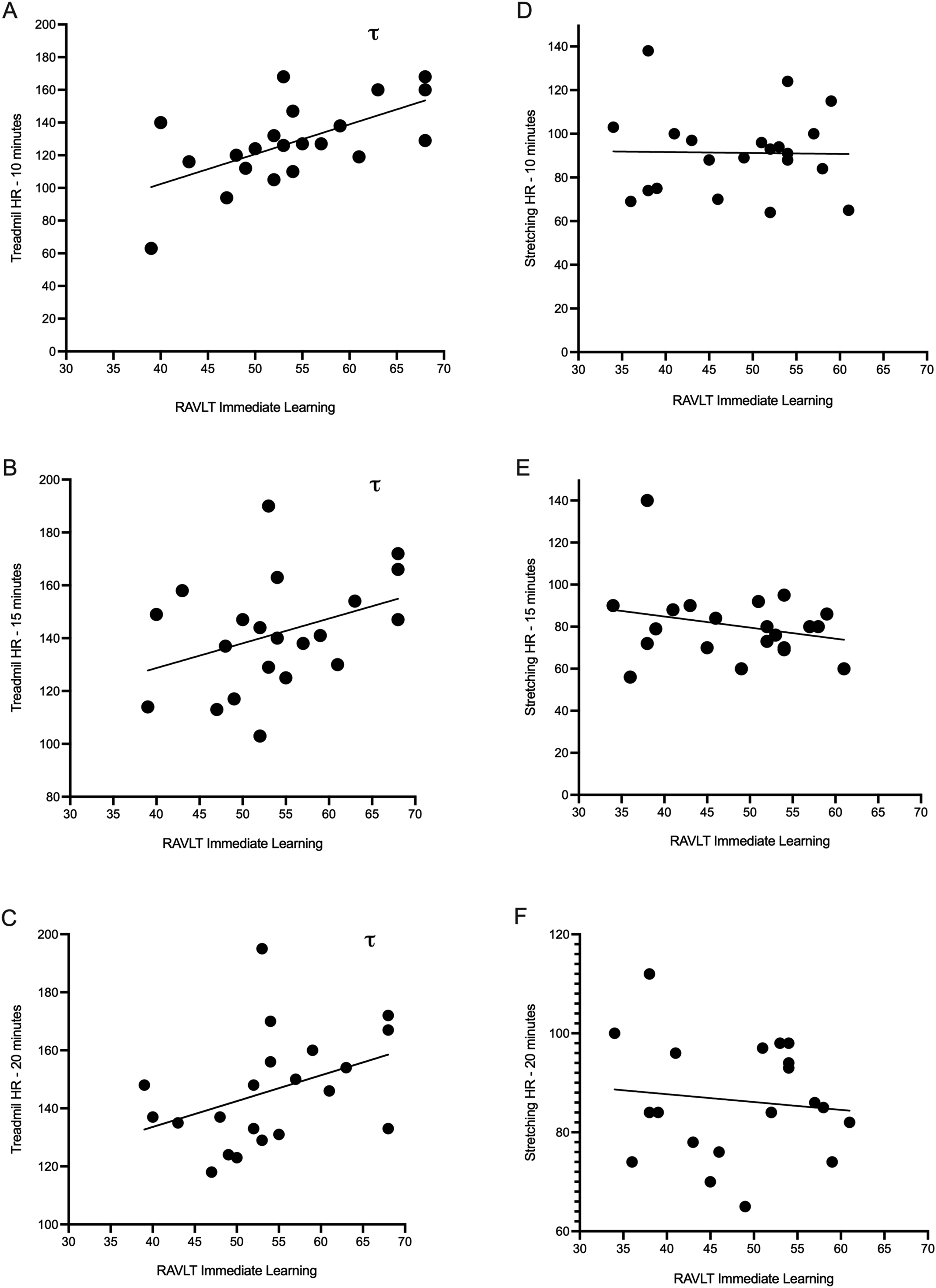
Association between heart rate at various time points and RAVLT immediate learning. The aerobic exercise (A-C) and stretching (D-F) are displayed separately. τ significant relationship between heart rate and RAVLT immediate learning, P < .05, one-tail. RAVLT, Rey’s auditory verbal learning task; HR, heart rate.
Discussion
The key finding of this study was that verbal memory outcomes of RAVLT showed higher immediate learning and retention over time after completion of moderate-intensity aerobic exercise (AE) compared to muscle stretching exercise (SE). RAVLT learning as well as recognition did not show a group difference. The former finding indicates that the intervention did not affect the learning rate. The latter finding was likely due to a ceiling effect. Overall, these results indicate that aerobic exercise created an increase, albeit modest, in memory encoding capacity. Further, memory span did not show a difference between AE and SE groups, indicating that the benefit of aerobic exercise was specific to long-term memory and does not extend to short-term/working memory. Further, both mood and expectation did not influence with exercise-related changes in cognitive measures.
Compared to the SE group, young healthy participants who completed a single 20-min bout of moderate-intensity aerobic exercise showed higher immediate learning (Trial 1 to 5) and retention over time (i.e., delayed recall was higher in the AE group and forgetting and percent forgetting were lower in the AE group). Similarly, meta-analytical results of previous studies showed a small but significant effect of acute aerobic exercise on cognitive function. 2 20 min may be the ideal duration threshold to maximize the cognitive benefits of exercise with shorter durations (between 11-20 min) and longer (more than 30 min) having a negative effect. 2 Furthermore, McMorris and Hale reported moderate-intensity exercise to be optimal for promoting improvements in processing speed. 24 However, the influence of intensity may be predicated on the amount of time between the end of exercise and the cognitive test. For example, light intensity exercise was more impactful when testing was performed immediately after exercise, but when delayed by more than 1 min, the effect was lost. Higher intensity was necessary when post-exercise testing was performed after an 11-20 min delay, but beyond 20 min, the effect of intensity on cognitive function was lost. 2 The mechanisms that explain the cognitive benefits of exercise such as the catecholamine response, enhanced hemodynamics, neurotrophic, and neurotransmitter factors may require higher intensity for induction when there is a substantial delay between exercise and cognitive testing. 2 A 15 min delay between exercise and cognitive testing was used in the current study, which fits within the ideal time range (11-20 min).
The linkage between exercise heart rate and learning outcomes were evaluated to better understand whether a cardiorespiratory component or muscle activation alone (i.e., stretching) was required to promote exercise-related cognitive gains. McMorris proposed the catecholamine hypothesis for the acute exercise-cognition interaction, which highlighted the importance of aerobic exercise for promoting mechanisms linked to exercise and cognition. 12 This model ascertains that exercise facilitation of cognition is mediated via moderate-intensity aerobic exercise stimulation of the brain stem via catecholamines. However, McMorris also highlighted that the muscle stretch reflex may play a role, which motivated the current study to compare aerobic exercise and muscle stretching. As expected, in the current study, heart rate was higher at all time points during the aerobic session than during the stretching session, and for the AE group only, a significant relationship was observed between immediate learning and heart rate at the 10, 15, and 20 min time points. This indicates that the hemodynamic response to exercise may play some role in mediating the post-exercise cognitive response; however, cause and effect cannot be determined. One additional study compared aerobic exercise to a stretching control. Alves et al, evaluated memory and selective attention after either high intensity interval exercise (10, 1 min efforts at 80% heart rate max) vs low intensity active stretching. 20 Selective attention was higher after interval exercise, but no difference in memory was detected after the interval exercise compared to stretching, and no evaluation of the heart rate response was performed. The difference in memory outcomes between Alves et al and the current study may be attributed to the differing intensities studied and/or the type of memory test administered.
We also attempted to evaluate the relationship between self-perceived expectation and memory outcomes. Expectation was evaluated after both interventions (AE and SE) using 5-point Likert-type scale. Mean expectation was not different between groups, and did not influence memory outcomes in either group. The effect of expectation on memory outcomes is complex and not well understood. Positive expectation has been linked to higher cognitive gains in comparison to negative expectations. 17 In addition, individuals who were presented with a positive or negative expectation message showed cognitive measures consistent with those messages. 17 Recent work also showed expectation to be the highest after physical exercise when compared to various other tasks such as video games, puzzles, and TV watching. 18 Specifically, participants generally expected to have greater cognitive performance after completing acute moderate-intensity exercise compared to the other conditions. 18 Despite higher expectation after exercise, no increase in memory was detected, which is in opposition to the findings in the current study (i.e., no expectation effect but improved memory). These results further complicate the role of expectation, and additional research is needed to evaluate the expectation effect.
Similarly, self-reported mood state did not influence memory outcomes in both the AE and SE groups. It is well studied that aerobic exercise has a positive relationship with mood state, but the effect of mood on cognition is less clear. Martin and Kerns reported worse short-term memory in response to a positive mood state. 25 The explanation was that mood increases the activation of working memory, which then decreases the ability to store information during focused attention. Conversely, Kiefer et al, proposed that good mood state supports superior memory performance for word generation. 26 Therefore, evaluating the role of mood was of importance in the current study. No difference in mood was detected between groups; however, pre- and post-mood measures were not performed so the change in mood state could not be evaluated. Future work should evaluate the change in mood and its relationship with exercise-related memory changes.
One limitation of this study is baseline maximal cardiopulmonary testing was not completed to verify accurate intensity targets for each participant. Self-perceived exertion was used to guide exercise intensity, which has been shown to accurately target appropriate intensity among young adults. 27 A second limitation is the study was completed among young (college-aged) adults, which limits the generalizability of the results. Thirdly, the lack of the research team being blinded to the intervention may have introduced some bias. A fourth limitation is using a between group study design. This decision was made to prevent a learning effect for the RAVLT that may have occurred using a within design. Lastly, the inability to measure mechanistic outcomes (e.g., BDNF, brain blood flow) limits the ability to explain the findings.
Conclusions
Our research findings add to a growing body of research suggesting that an acute bout of moderate-intensity exercise is effective in contributing to higher cognitive function, as compared to a muscle activating control (i.e., stretching exercise). Increased cardiovascular activation could be important to these cognitive improvements, though more specific research is needed to understand the causation. Further, both mood and expectation did not influence the memory outcomes. In the future, these findings may be helpful to apply to clinical settings: For example, using a single bout of moderate-intensity exercise prior to a psychotherapy session to help patients retain information. The field may benefit from focusing on molecular changes in cardiovascular components during acute exercise, acute exercise types and intensities, and findings in different age groups across a lifespan.
Supplemental Material
Supplemental Material - Verbal Memory is Higher After Aerobic Exercise When Compared to Muscle Stretching
Supplemental Material for Verbal Memory is Higher After Aerobic Exercise When Compared to Muscle Stretching by Abigail Doku, Gavin T. Roupe, Emma Rankine, Isabel Flemming, Jacob A. Provost, Micah Zuhl, and Hajime Otani in American Journal of Lifestyle Medicine.
Footnotes
Author Contributions
Abigail Doku: investigation, resources, data curation, writing—review and editing; Gavin T. Roupe: Conceptualization, investigation, methodology, resources; Emma Rankine: investigation, writing—original draft; Isabel Flemming: investigation, resources, data curation; Jacob Provost: data curation, investigation, methodology, resources; Micah Zuhl: Conceptualization, methodology, formal analysis, writing—review and editing, supervision, project administration; Hajime Otani: Conceptualization, methodology, formal analysis, writing—review and editing.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Statement
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.