
Abstract
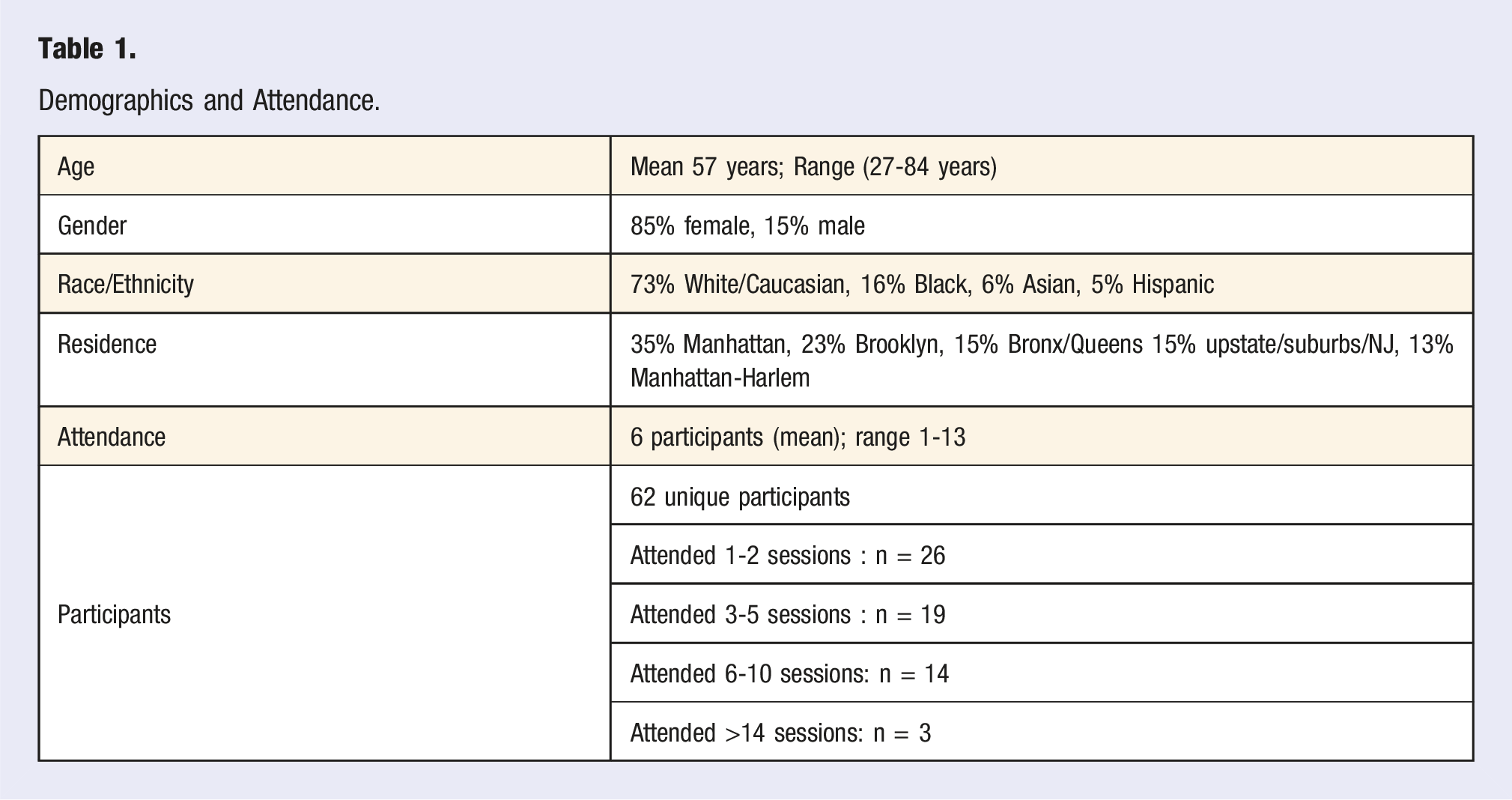
The aim of this pilot was to assess the feasibility and acceptability of virtual Narrative Healing Circles (NHC), a new form of Shared Medical Appointments (SMA) among mixed diagnosis population within an urban tertiary academic medical center. Methods: Multi-method, voluntary recruitment of eligible patients, included referrals, flyers, hospital events page, and patients who participated in an ongoing 7-week integrative oncology SMA series. Two physicians (lifestyle medicine and chaplaincy specialists), both trained in narrative medicine, co-led one-hour long virtual NHC SMAs held every other week for a total of either 4 or 8 sessions. Sessions included a centering meditation, brief check-in, topic introduction, short writing exercise initiated with a written, musical, or visual prompt, followed by time of sharing and listening. Optional electronic pre and post participant surveys were emailed at enrollment (7-questions, response rate 29%) and after 4-8 NHC SMA sessions (12-questions, RR 34%). Results: Virtual NHC SMA were offered from 2/23/22-8/30/23 with 62 unique participants, 266 total visits. Average age: 57 years (range: 27-84 years). Gender: 85% Female, 15% Male; Ethnicity: 73% White, 16% African American, 6% Asian, 5 % Hispanic. About half lived in underserved areas (Harlem, Bronx, Queens, Brooklyn). Payor mix included 40% Medicare, 60% Commercial insurance. Session attendance: 6 participants (mean); 1-13 (range). The number of sessions attended ranged between 1-28 sessions. Anxiety or fear (89%), depression (61%) and pain (67%) were the top 3 symptoms reported in the pre-survey. After 4-8 sessions, participants reported improvements in anxiety/fear (43%), sadness/depression/hopelessness (33%), irritability/stress (33%), isolation/loneliness (33%). They reported several positive changes: restarting yoga or meditation practice, greater focus on awe, journaling, increased mindfulness, and feeling better equipped to manage stress. 94% reported goals met, 95% would recommend the series to others. The 2 clinician leaders reported increased empathy, personal well-being, and work satisfaction. Conclusion: Virtual NHC SMA series among mixed diagnosis population is feasible, positively affects patients’ agency and well-being, and acceptable to patients and providers. A more formal study design with broader representation of diverse population and assessment of causality such as an RCT with longer follow-up is recommended.
Keywords
“The healing circle coordinator has proven to be essential to the seamless execution of the circles.”
Background
The Impact of Isolation and Loneliness on Health
In recent years, we have come to better understand the prevalence and profound health impact of social isolation and loneliness, which can be serious and even life-threatening.
The Surgeon General declared that loneliness is a public health emergency,1,2 and in 2023 he issued an Advisory 3 and a call to action to mobilize communities, private sector, government, and health professionals. 1 The consensus among the public health and clinical experts is that 40% to 80% of health and wellness can be directly or indirectly attributed to social factors, which include social relationships. The prevalence and profound health impact of social isolation and loneliness can be serious and even life-threatening. A 2010 meta-analysis of studies measuring mortality as a function of social relationships found that people with stronger relationships had a 50% higher likelihood of survival than their counterparts with weaker relationships. In terms of mortality, loneliness and social isolation can be as harmful as smoking 15 cigarettes a day.4,5
Social connections are also essential for individual’s assessment of meaning and purpose of life, 6 particularly for people living with acute and chronic disease. Meaning and connection can buffer the effects of stress and facilitate adaptive coping. 7 The large-scale Veterans Health Administration Whole Person/Whole Health evidence-based integrative model of care advocates for a health care paradigm shift from “What’s the matter with you?” to “What matters to you?”8,9 and has outcome data supporting the benefits. One of the nine pillars of the Blue Zone research on longevity, having a sense of purpose, 10 has been associated with health, mortality risk, 11 and well-being outcomes. Research on cancer survivorship has associated illness mindsets with health-related quality of life; leading oncologists suggest we should target not just tumors but also mindsets.12,13 Adaptive mindsets, peer survivor role models, and supportive patient-provider relationships have potential to provide treatments for the psychological and social ramification of illness while simultaneously attacking malignant cells with state-of-the-art cutting-edge treatments.
Blue Zones research on the areas of the world with the most centenarians 14 has identified 9 lifestyle habits associated with longevity. Four of the nine are related to outlook and connection including purpose (“Ikigai” or “Plan de vida”), belonging (community), loved ones, and right tribe (social circles, “Moais”). There is a body of literature postulating that social support, social networks, and support groups can be protective against mortality15-17 with survival improvements in cancer populations.18-21 Lifestyle Medicine is a medical specialty that uses therapeutic lifestyle interventions as a primary modality to treat chronic conditions including but not limited to cardiovascular diseases, type 2 diabetes, cancer, and obesity. Positive social connections 22 is one of its six pillars. Clearly, optimal patient care, must address multiple dimensions of health including the importance of human connection and purpose. Lifestyle medicine specialists need effective interventions.
Narrative Medicine’s Role Regarding Social Connection and Well-Being
Narrative Medicine 23 is a pedagogical framework that acknowledges and honors individual and collective narratives in the context of clinical practice, research, and education to promote healing. It aims to address the relational and psychological feelings and experiences that occur in tandem with physical illness and caring for the ill. It places emphasis on deep and generous listening24,25 thereby improving patient-physician communication and ultimately patient outcomes. 26 The deepened clinician-patient connection 27 can assuage the isolation that might otherwise amplify a patient’s health concerns, anxiety, suffering, and trauma.
Several studies of narrative medicine interventions have demonstrated improvement in symptoms and/or suffering among patients with asthma, rheumatoid arthritis, heart failure, advanced cancer, diabetes, overweight, pain, and psychogenic non-epileptic seizures. Outcome measures include quality of life, improved medication adherence, decreased emergency room visits, overcoming social withdrawal and fear after a trauma, regaining of meaningful activity, and recovery of lost self-identity during illness and treatment.25,28-40
Emerging data suggest that reflective writing, drawing, speaking, and even singing about meaningful experiences can improve health, reduce unwanted symptoms, ease emotional discomfort, release oxytocin and deepen connections with others, which can ultimately improve quality of life. The stories we tell about ourselves and to ourselves can shift negative narratives through neural re-narrating,41,42 which allows the individual to gain a sense of agency and well-being. Participants who engage with storytelling learn to access deeply held but rarely conscious beliefs and emotions and explore what gives them meaning, joy, and a sense of wholeness.
Narrative medicine and storytelling have been used in the care of underserved populations. They have played a central role in the work of Native American physician Lewis Mehl-Madrona in a study of shared collaborative care and group storytelling in the Native American community. Shared collaborative care refers to a group visit by multiple patients with the same disease, in this case Diabetes Mellitus Type 2, and their families and loved ones. During these encounters, patients and families gave accounts of self, and shared their life stories, hopes, and challenges. This approach to diabetes care was shown to be significantly superior to both group medical care and standard diabetic health education combined with conventional care. 33 It was also linked to improved quality of life in a Canadian indigenous population. 34
Model of Care: Shared Medical Appointments
SMA are a promising, innovative, health-equitable, cost-effective delivery care model found to be feasible and acceptable to patients, clinicians, and institutions.43-49 Various SMAs have been introduced at our integrative health center that operates within an urban tertiary academic medical center. These include sessions on lifestyle change, 50 culinary medicine, 51 women’s health, oncology, 52 yoga, 53 qigong, 54 mental wellness, prenatal health, and meditation. We wondered whether narrative medicine, 53 particularly in group settings 55 could leverage the power of social connection and benefit patients’ health and well-being. To our knowledge, there have not been any reports in the literature for telehealth delivered narrative medicine group visits conducted among mixed diagnosis populations at academic centers.
Our goal was to explore how to bring the benefits of narrative medicine to patients receiving care in an Integrative Health Center within a large urban health system, to foster connections, decrease isolation, and improve symptom severity and well-being.
Methods
Pilot Intervention
We aimed to examine the feasibility, acceptability, and impact of a new model of SMA (Narrative Healing Circles [NHC]) offered via telehealth. The SMA was developed using narrative medicine and spiritual care principles. Two physicians (lifestyle medicine specialist and chaplaincy specialist), both trained in narrative medicine (through a CME course), developed, and first trialed a mini-pilot of the new NHC as a single session within an integrative oncology shared medical appointment series. Preliminary feedback indicated interest among patients for a biweekly NHC specific SMA program which led to the pilot of the full model.
The 2 clinicians co-led a one-hour long NHC SMA on weekday afternoons via live- internet based videoconferencing. These sessions were held every other week, and depending on the time of year were offered as a series of 4 sessions (summer) or 8 sessions. Sessions included a centering meditation, brief check-in, topic introduction, short writing exercise initiated with a written, musical, or visual prompt, ending with reflection sharing. Participants were invited to share and those who preferred not to, were acknowledged for the gratitude of their presence. Group rules were reviewed at the beginning of each circle, priority given to listening and not trying to fix anyone, trusting that each participant had all they needed within themselves. Over time, participants felt safe to share a brief comment to one another using the chat. At the end of the meeting, the circle’s themes and resources were sent to participants for them to further reflect on in between visits. Documentation of the NHC SMA visit was completed by one of the physicians with billing based on decision making complexity.
Participants were recruited through referrals, flyers, hospital events page, and word-of-mouth from introductory NHC session piloted with an existing 7-week integrative oncology SMA series. Adult patients, English speaking, with internet access and receiving care from the Weill Cornell Integrative Health Center were eligible. The team also included a group visit coordinator to set up telehealth links, organize schedules, troubleshoot technology issues with patients, send weekly reminder emails, and provide online platform instructions to patients. The coordinator also distributed the welcome packet including insurance/billing information.
Data collection included a pre- and post-survey developed using Qualtrics. The SMA coordinator emailed the link to the survey at the time of enrollment and after each 4-8-week series. Responses to the 7-question pre-survey and 12-question post-survey were optional and completely voluntary and anonymous. No incentives were available or offered. Surveys were only available in English. The institutional IRB determined the pilot to be exempt.
Results
Demographics and Attendance.
Patients’ Pre-program Symptoms/Health Concerns, and Whether They Were Addressed and Improved by the Program.
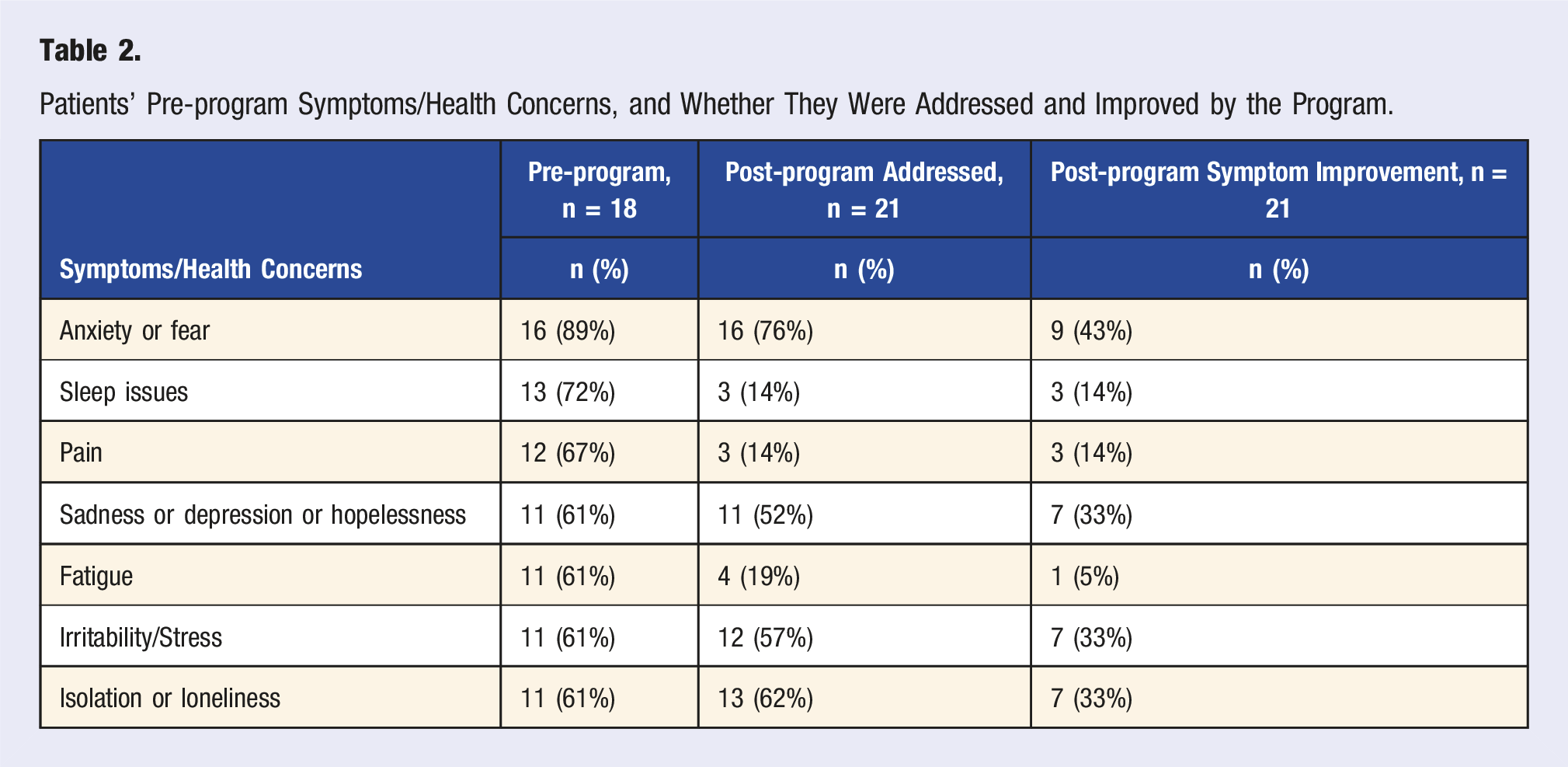
76% of post-series participants reported that the series of narrative healing SMAs addressed their anxiety/fear, 62% reported having addressed their isolation/loneliness and 52% their sadness/depression/hopelessness. Between 33% and 43% reported improvement in anxiety/fear (43%), sadness/depression (33%), irritability/stress (33%), isolation/loneliness (33%).
94% of respondents reported their goals were met and 95% would recommend the program to others. 31% thought that 4-week series were the “perfect length,” 68% preferred more sessions. No one suggested fewer sessions.
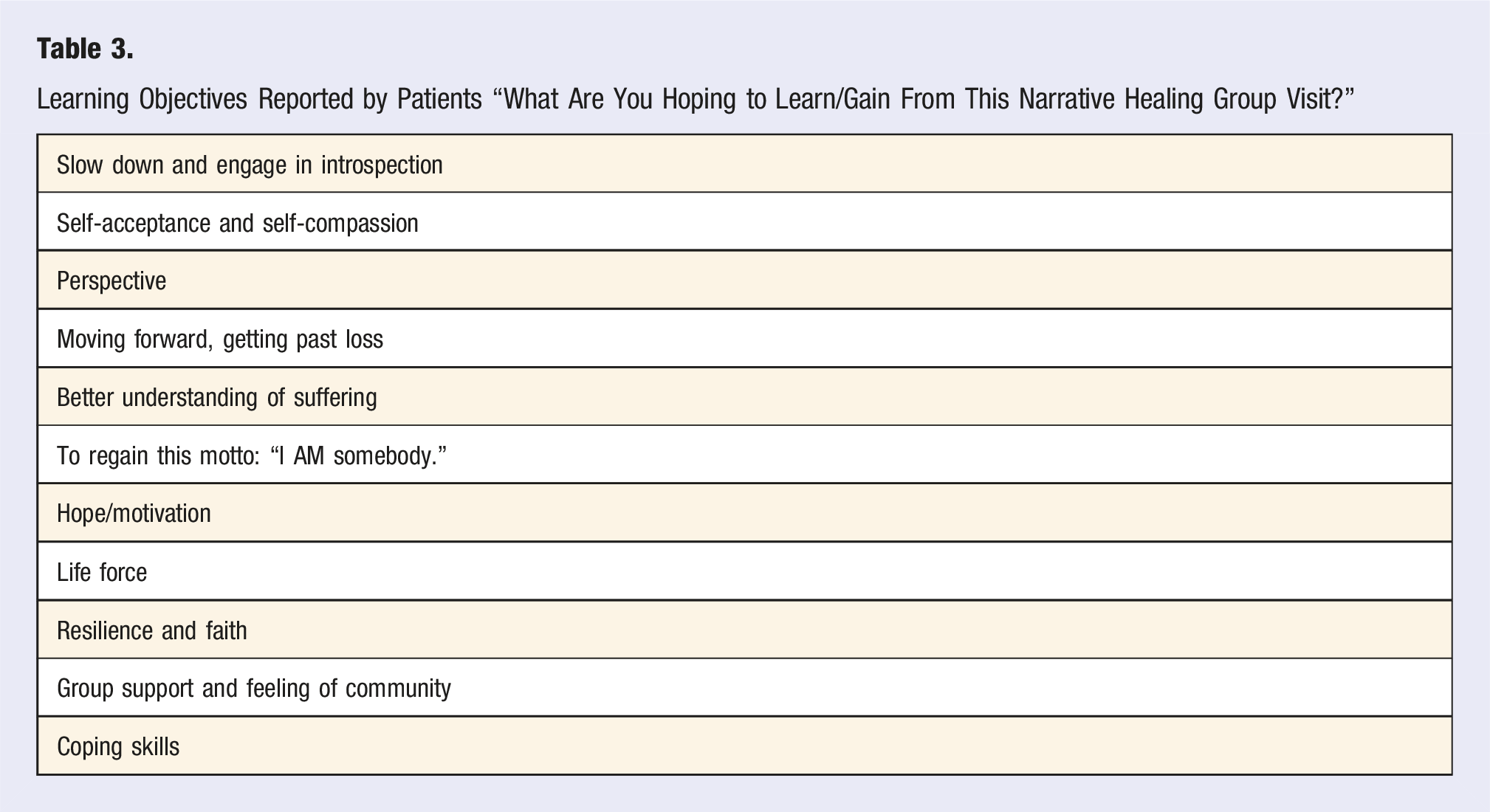
Learning Objectives Reported by Patients “What Are You Hoping to Learn/Gain From This Narrative Healing Group Visit?”
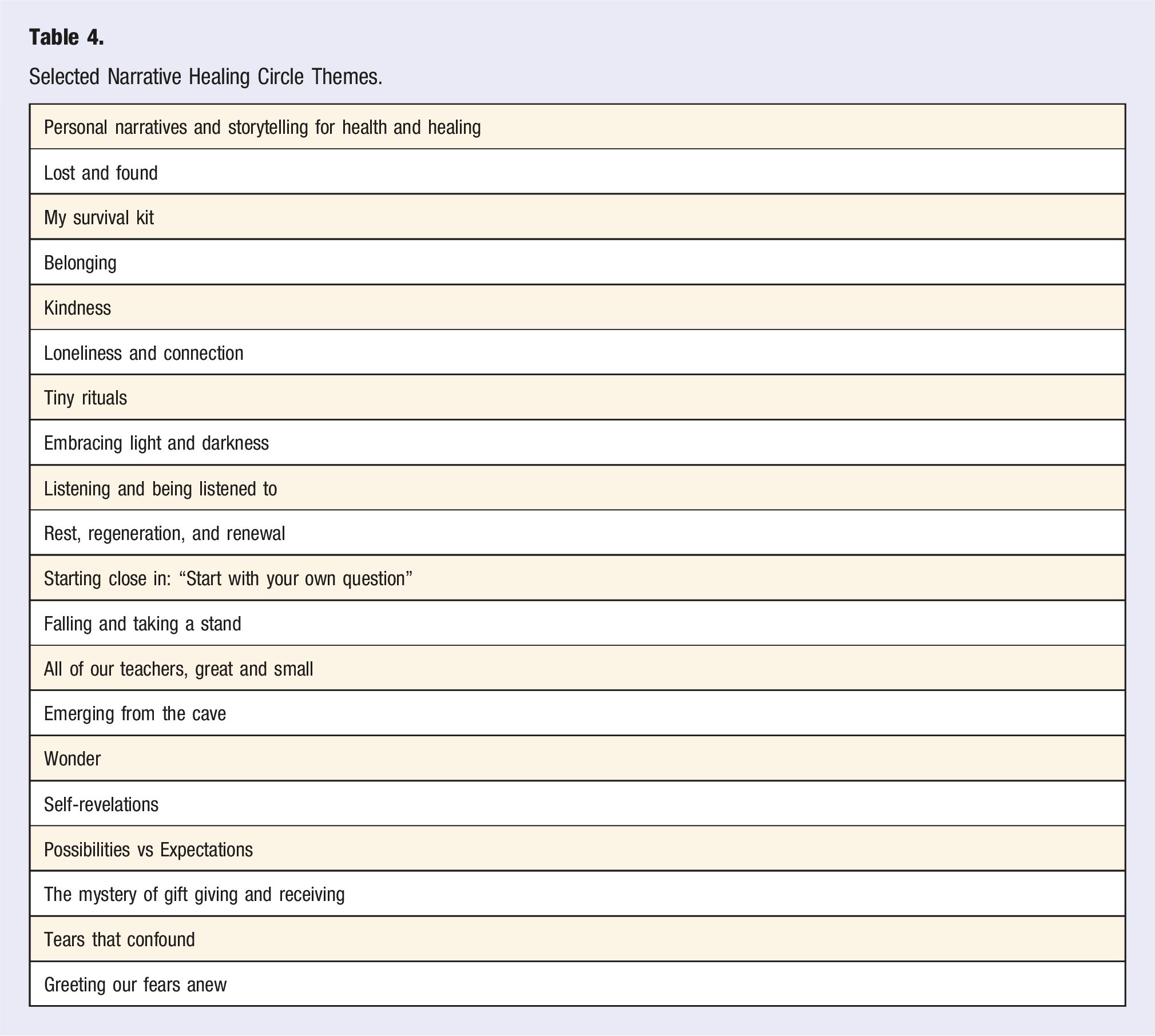
Selected Narrative Healing Circle Themes.
Discussion
Current societal factors are contributing to the significant increase in the prevalence of loneliness and lack of social connections. There is demonstrated negative impacts on health. Over 52% of Americans live with at least one chronic condition and 27.2% have more than one. 56 Mental health issues such as depression, anxiety have also skyrocketed, and so has the incidence of suicides. Life expectancy, quality of life and overall wellness are also significantly affected. The situation led the Surgeon General to declare a public health crisis and to issue a call to action to address rampant isolation.
Fortunately, effective resources and interventions are available to health professionals.57,58 Specialists trained in lifestyle medicine have an important role to play in supporting patients with serious illnesses and complementing care offered by physicians in other specialties. These services are now reimbursed by payers,59-61 who recognize the practice standards for the specialty established in 2016 by the American Board of Lifestyle Medicine. 62
Our goal was to explore whether social isolation and a sense of loneliness could be improved using a group visit that would engage participants in self-reflection and safe conversations and aimed to foster community and sense of agency and resilience. We also wanted to test whether our new model of SMA that integrated narrative medicine and spiritual care principles (Narrative Healing Circles) could be feasibly implemented within an Integrative Health Center. The group visit was developed by two specialists, one with Lifestyle Medicine training and the other with Spiritual Care training, and both with continuing education training in narrative medicine.
The model for the narrative healing circles proved to be feasible; the pilot started in February 2022 and ended in August 2023, yet the circles have continued uninterrupted beyond the pilot and are scheduled until October 2024 and beyond. Financially, SMAs have been reimbursed by Medicare and private health plans. Future plans are to negotiate Medicaid reimbursement to strengthen the financial sustainability of the SMAs. More detailed financial data on the return on investment of our various types of SMAs have been published.52,63
The staffing model has also proved to be efficient, 2 clinicians’ time, 1 hour every other week and prep time. Besides the hour for the session, 1 additional hour was blocked for documentation and program development, as well as 2 hours for preparation of the session materials (selected poems, music, art; and questions to guide reflection on the topic of the session (e.g., hope, loneliness, stages in one’s life).
The healing circle coordinator has proven to be essential to the seamless execution of the circles. Logistics have been simple, given that meetings occur on Zoom and not in-person. In fact, as in-person option was explored post-COVID restrictions, the virtual option remained the preferred one, as inclusive of all patients regardless of disabilities or other health restrictions.
SMA patients reported benefits that are supported by the literature, such as stronger social bonds,64,65 self-efficacy and self-agency, 66 reduction in isolation, and improved depression, hopelessness. Given the current crisis affecting the mental health workforce, our SMA model can provide interim support to patients with limited access to mental health services.
During the question/discussion time, mutual sharing about disease self-management, behavior change tools, lifestyle interventions resulted in patients being inspired by peer adaptive coping strategies, and development of patient/provider equitable and trusting relationships. 67 They also noted how this form of appointment was unique and atypical of usual medical encounters.
The limited number of participants and the voluntary sampling are perhaps the most important limitations to the interpretation of the results. Another major limitation of interpreting the data in this pilot is that we are not comparing the same patients pre/post survey. We acknowledge the lack of generalizability—participants were all English speaking and we lacked information to fully evaluate the effect of social determinants of health. The responses to the pre-post series surveys were anonymous, and do not allow us to track changes over time at the individual level, but only at the group level. A large number of patients (41%) only attended 1-2 SMA sessions and we cannot assess the reasons for this. Time concerns such as competing medical appointments, caretaking or work schedules, or preferences for 1:1 therapy over group visit are possible explanatory factors. The study design is inappropriate to allow any assessment of possible causality.
Conclusion
The pilot represents a proof of concept and results do support broader spreading of the model and a more formal evaluation that follows a cohort and reduces bias, such as a randomized clinical trial. Further work should ensure the adequate diversity of participants, a focus on the benefits of the model on underserved populations, and its effect in mitigating clinician burnout.
Footnotes
Acknowledgments
We wish to recognize all the patients who participated in the narrative healing circle SMAs and provided feedback. We also wish to acknowledge Mary Acosta for her administrative support and Chiti Parikh MD for her leadership support.
Author Contributions
Dr. Loy conceptualized and designed the study, coordinated, and supervised data collection, collected data, conducted the initial analysis, drafted the initial manuscript, reviewed, and revised the manuscript. Dr Audet designed the intervention, that is, the content and delivery of the narrative healing circle SMA, reviewed, and revised the manuscript. All authors approve the abstract as submitted and agree to be accountable for all aspects of the work.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Institutional Review Board Statement
The WCM Institutional Review Board (IRB) determined on 31 January 2023 (#23-01025565) that this activity is not considered research involving human subjects due to its anonymous, retrospective, program evaluation nature and that further IRB review and approval is not required.
Data Availability Statement
Data used in this program evaluation will be made available upon request.