
Abstract
Heart failure with reduced ejection fraction (HFrEF) is a major contributor of premature cardiovascular-related deaths. Patients are typically on numerous medications to manage this condition; however, patients continue to experience poor quality of life. Alternative therapeutic approaches are needed to treat HFrEF. The clinical course of seven patients with Stage C and D HFrEF who failed guideline-directed medical therapy were retrospectively analyzed based on medical chart data. All patients consumed a defined, plant-based diet as part of their clinical treatment, and a subset also underwent alternative treatment modalities: External Counterpulsation therapy, BEMER therapy, infrared sauna therapy, ozone therapy, or PlaqueX® therapy. Chart review of these patients indicated improvement in left ventricular ejection fraction (LVEF) and right ventricular systolic pressure (RVSP). All patients also had a significant reduction in medication needs and body weight. Further, all patients reported significant improvements in their quality of life. These data suggest that a defined, plant-based diet combined with other alternative modalities may be efficacious in reducing HFrEF medications and treating Stage C or D HFrEF patients who failed guideline-direct medical therapies. Observations from this case series indicate a need for rigorous prospective studies to confirm these effects.
“Nutrition is the foundation of our integrative heart failure therapy, and therefore, it is the common denominator of treatments.”
Introduction
In the United States, approximately 6.7 million individuals over the age of 20 have a diagnosis of congestive heart failure with reduced ejection fraction (HFrEF); this prevalence is expected to rise to 8.5 million by the year 2030. 1 The lifetime risk factor of heart failure has increased to 24% and if current trends hold 1 in 4 people will develop heart failure in their lifetime. 1 Current treatment guidelines employ various pharmaceutical and non-pharmaceutical therapies to treat HFrEF. 2 Despite the many advances in heart failure therapies, more than 12% of heart failure patients are classified as either stage C or D heart failure.3-5 These individuals can have significant symptoms of heart failure despite optimal medical therapy and require frequent hospitalizations. Patients in these categories typically progress to the point of needing advanced therapies such as left ventricular assist devices (LVADs) and heart transplants. Disease progression in heart failure patients is often accompanied by additional complications, increasing health care costs, and elevated risks for premature mortality.
Data from an earlier case series of three patients with HFrEF indicated a defined plant-based diet (DPBD) was associated with improvements in cardiac function and hemodynamics, in addition to reductions in the need for patient medications. 6 In addition to DPBD, other alternative, nonmedical therapies have emerged in recent years. Beneficial cardiovascular effects have been observed with infrared sauna therapy (IFS),7,8 enhanced external counterpulsation therapy (ECP),9,10 ozone and ultraviolet blood irradiation (UBI),11-13 polyunsaturated phosphatidylcholine (PC) infusion, as well as bio-electro-magnetic-energy regulation (BEMER) therapy.14-19 The current retrospective case series study examines the clinical course of seven acutely ill HFrEF patients (Stage D) who presented to an outpatient integrative cardiac center with worsening symptoms of HFrEF, despite being on optimal guideline-directed medical and nonmedical therapies. These patients consumed a DPBD along with one or more regenerative therapies integrated with limited allopathic heart failure therapies.
Methods
Study Population and Patient Presentations
Baseline Demographics.
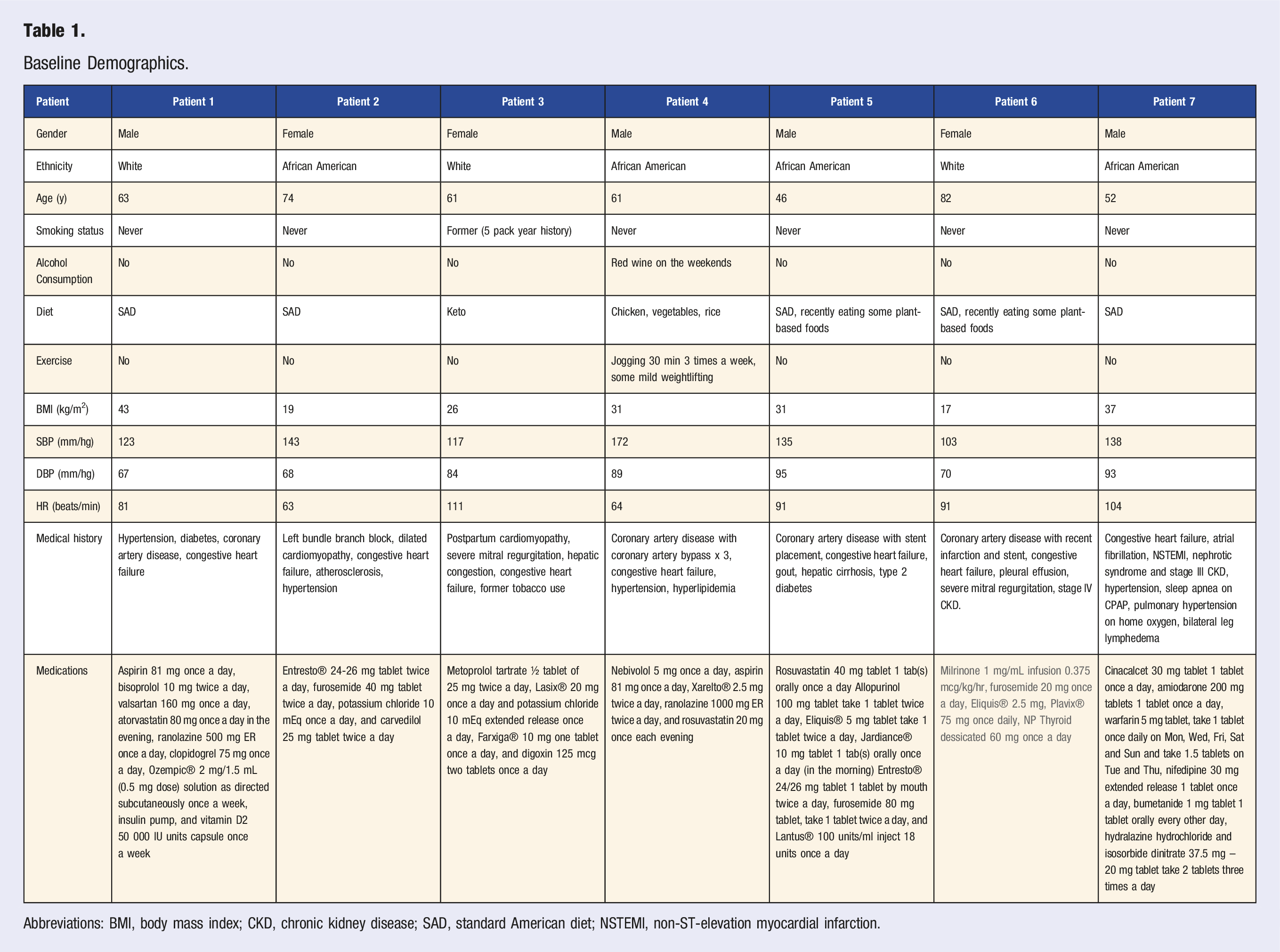
Abbreviations: BMI, body mass index; CKD, chronic kidney disease; SAD, standard American diet; NSTEMI, non-ST-elevation myocardial infarction.
Weekly Visits
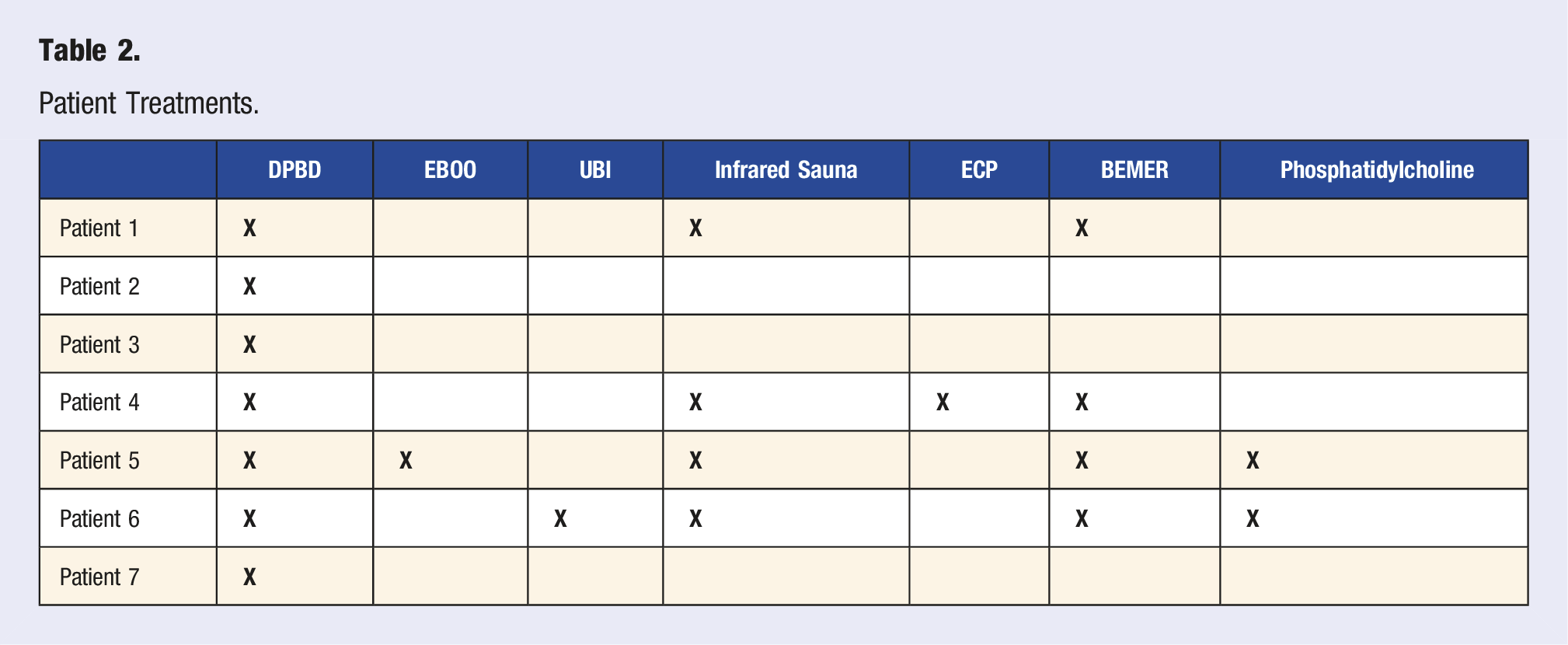
Patient Treatments.
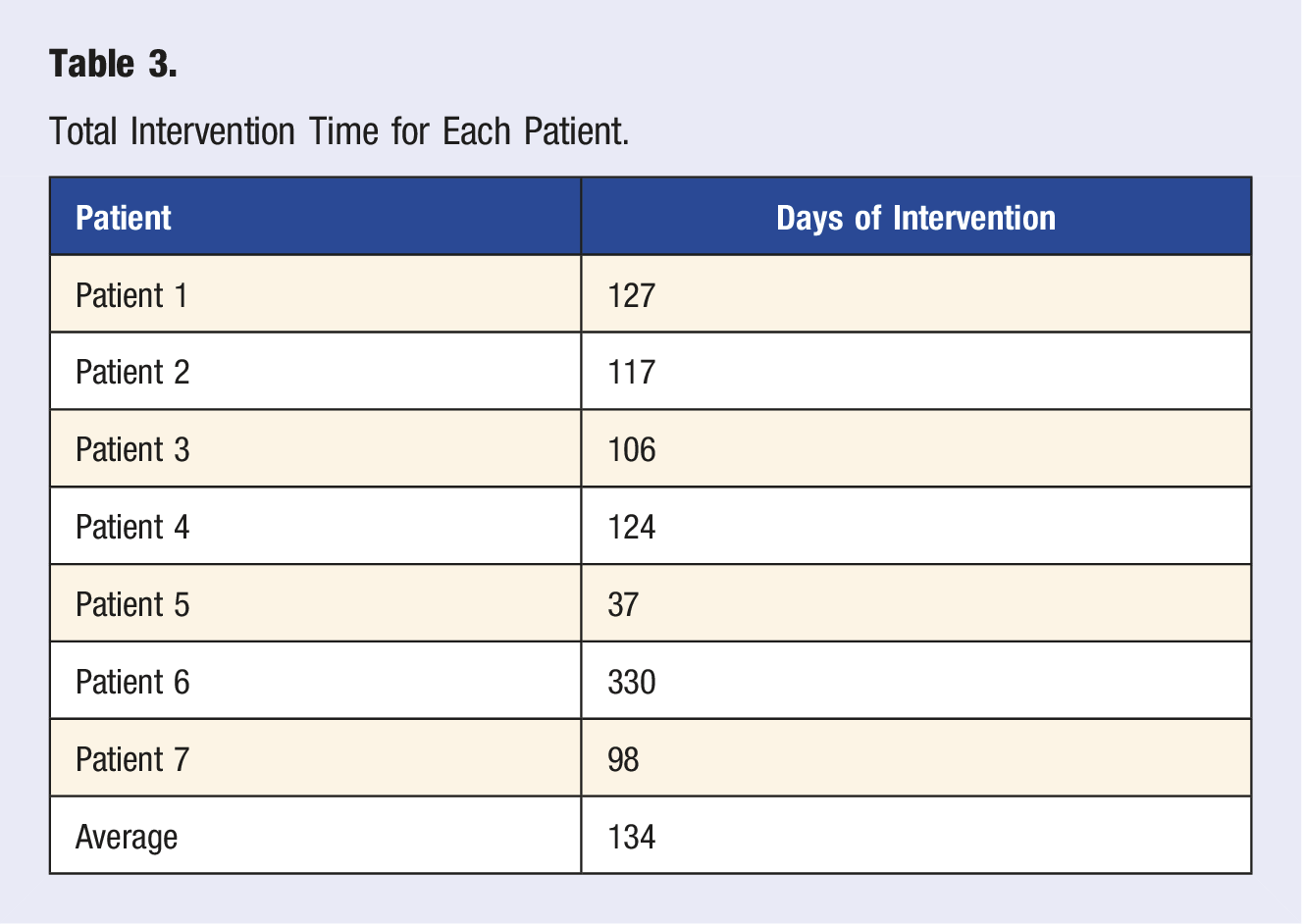
Total Intervention Time for Each Patient.
Results
Patient Clinical Course
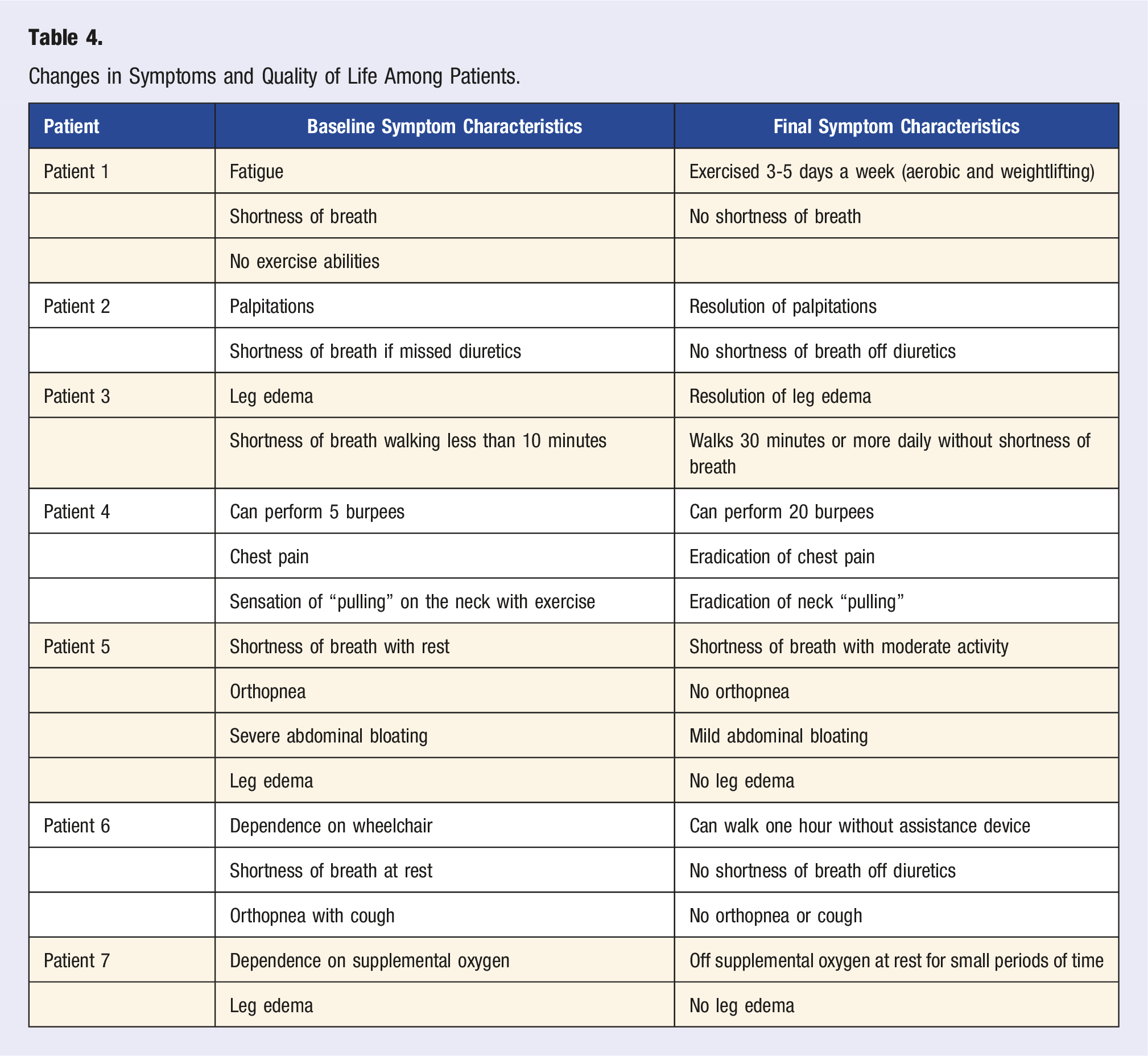
Overall, LVEF trended towards an increase from baseline (Figure 1), although statistical significance was not reached (P = 0.08). Due to Patient 6’s worsening condition, the removal of milrinone was required which resulted in LVEF reduction Figue S1. As such, a separate analysis of LVEF without patient 6 was conducted (Figure 1B); this analysis resulted in a significant increase in overall LVEF (+37%, P = 0.0071). In addition, RVSP trended towards a 21% reduction (P = 0.0548) following the intervention (Figure 1C). There was also a significant reduction in body weight (−12%, Figure 1D) following the intervention (P = 0.034), and a significant reduction in medication usage (Table S2, Figure 1E; −55%, P = 0.0004). No significant changes were observed in other clinical parameters (Figure 1(F)–(K)). In addition, quality of life drastically improved for all patients (Table 4). Patient-specific outcomes and additional results can be found in the supplementary materials. Clinical changes in subjects from baseline (pre) to final (post). (A–C) LVEF and RVSP were quantified via echocardiogram. LVEF data is presented with (A) and without (B) patient 6. (F–H) SBP, DBP, and HR were determined with an automated sphygmomanometer. (I–K) was measured by external laboratory analysis. Changes in Symptoms and Quality of Life Among Patients.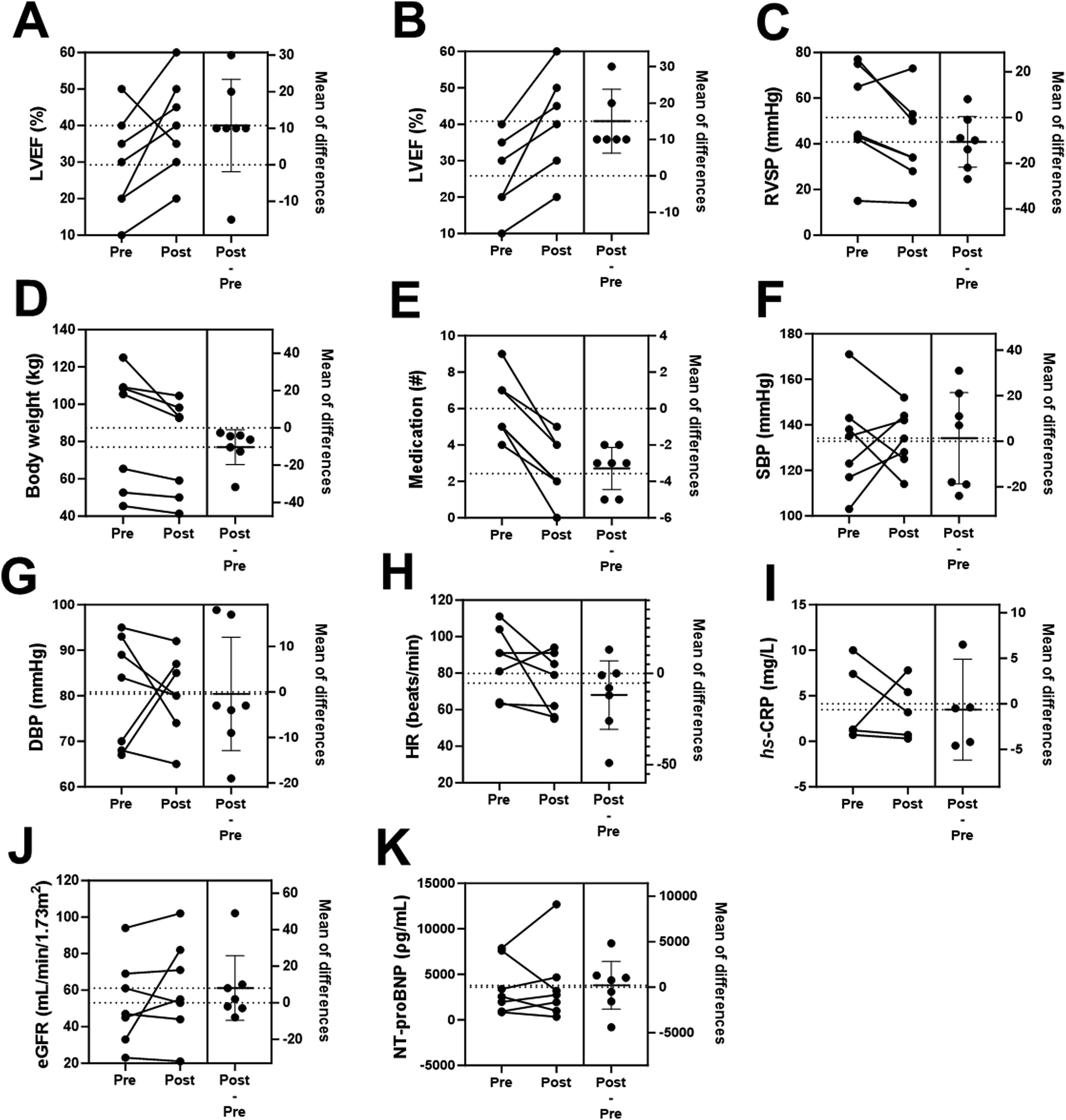
Discussion
We illustrate in this small, retrospective case series that a DPBD along with other integrative therapies was effective in improving heart failure while simultaneously reducing heart failure-managing medications. Considering the dramatic improvement in the quality of life of these patients (Table 4), these findings are noteworthy. Although the sample size and treatment duration limit the conduct of formal outcome analyses, this patient group experienced a positive clinical course consisting of overall clinical improvement. Despite a reduction of body weight in patients 2 and 6 who were already of low body mass index (BMI), they improved both from a clinical perspective and quality of life perspective. Patient 6, for example, was wheelchair-bound prior to the intervention and was able to walk and hike following the intervention. All seven patients had improvement in their functional status with increased exercise tolerance and an overall improved quality of life. The universal clinical improvement of this patient group strongly supports the likelihood that the nutritional and regenerative intervention had a positive clinical impact. Furthermore, the relatively short average treatment duration of 134 days in this cohort supports the likelihood that this intervention had a relatively immediate effect in this acutely ill population.
A contributing factor to these patients’ underlying illness is the fact that they were on an average of 6 medications each. While they were all on some form of guideline-directed medical therapy for heart failure, the underlying complex drug-to-drug interactions could contribute to adverse biochemical and or physiological effects. 20 Indeed, simply reducing one medication in the setting of polypharmacy reduces CVD mortality by 17%. 21 Illustrating this further, frequent and regular diuretic use can lead to intravascular volume depletion and electrolyte deficiencies, resulting in compromised overall cardiac output due to impaired filling pressures, myocardial dysfunction, and cardiac arrhythmias. The use of statin drugs in patients with underlying coronary disease and hyperlipidemia may result in impaired mitochondrial function,22,23 possibly worsening overall LV function. Therefore, medication reduction was an important part of the intervention. We also found that the DPBD could act as an alternative to statins by reducing LDL-C by 24.6 mg/dL (∼17%) and hs-CRP by 2.4 mg/L (∼32%). 24
We are unable to determine the relative efficacy of the various treatment modalities in the present case series due to the small sample size. However, evidence suggests that these alternative modalities are all effective in treating CVD and HFrEF, hence, our use of these modalities.7-14,17-19 Nonetheless, nutrition is the foundation of our integrative heart failure therapy, and therefore, it is the common denominator of treatments. These clinical observations raise important questions about the potential benefits of these integrative therapies in the HFrEF population. Future, well-planned, prospective studies could evaluate these questions and add to this area of medicine.
Conclusion
This case series demonstrates that a DPBD and regenerative therapy integrated with limited and targeted allopathic drugs can result in clinical improvements in stage C and D heart failure patients who remained symptomatic while on guideline-directed medical and surgical therapies. The potential safety and efficacy of this intervention for this critically ill population is an important observation and needs further evaluation in a randomized prospective study. Such a study is needed to elucidate the mechanisms and relative importance of the various interventions used in this case series.
Supplemental Material
Supplemental Material - A Defined, Plant-Based Diet and Other Integrative Therapies Improve Functional Status and Ejection Fraction while Reducing Medications in Patients With Heart Failure: A Case Series
Supplemental Material for A Defined, Plant-Based Diet and Other Integrative Therapies Improve Functional Status and Ejection Fraction while Reducing Medications in Patients With Heart Failure: A Case Series by Camille V. Owens, Rami S. Najjar, Marino A. Bruce, Bettina M. Beech and Baxter D. Montgomery in American Journal of Lifestyle Medicine
Footnotes
Acknowledgments
We would like to thank the support of key personnel in facilitating the care of these patients: Baxter D. Montgomery, Jr, and Manuel Hinojo. We would also like to thank the culinary team of the Garden Kitchen for preparing foods for these patients.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: BDM is the Medical Director of Montgomery Heart and Wellness Center and is the founder of the Garden Kitchen.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded, in part, by a grant from the National Heart, Lung, and Blood Institute (NHLBI) R25HL126145 to M.A.B., and B.M.B.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.